www.elsevier.com/locate/cuor
MINI-SYMPOSIUM: THE PAEDIATRIC HIP
(iv) Legg Calv
!e Perthes’ disease
James B. Hunter*
Consultant Paediatric Orthopaedic Surgeon, Queen’s Medical Centre, Nottingham NG7 2GZ, UK
Summary Many controversies remain in Perthes’. These algorithms are presented as
a way through the maze of contradictory and incomplete evidence. Catterall has
emphasised the importance of clinical examination in the assessment of cases of
Perthes’ and this is particularly important in the younger group, many of whose hips
heal very round, despite rather adverse-looking X-rays early on, because they have
maintained an excellent, almost normal, range of movements. The older child or
early adolescent with Perthes’ requires urgent attention, as the femoral head lacks
the regenerative capacity of the younger child. Before any operation in Perthes’,
action must be taken to unstiffen the hip. Containment procedures will fail if
performed on a stiff hip and even salvage procedures are best performed on a hip
that has been loosened as much as possible. Surgeons need to recall that most
untreated Perthes’ do not require intervention until the age of 40. If our
interventions on the child result in hip replacement being required in the 20’s,
then we have not done that patient a service.
&
2004 Elsevier Ltd. All rights reserved.
Introduction
Perthes’ disease is idiopathic avascular necrosis of
the femoral head in childhood. It was described
independently by Legg in the USA, by Jacques Calv
!e
in France and by Georg Perthes’ in Austria during
the first decade of the 20th century. The descrip-
tion of Perthes’ disease followed rapidly after the
intervention of the radiograph. Prior to that, it had
been thought to be a self-limiting infection,
possibly tuberculosis. In many countries the disease
is known as Legg-Calv
!e-Perthes’ disease, or LCP. In
Britain the condition is generally referred to as
Perthes’ because he had recognised the fact that
this was a form of avascular necrosis.
Despite the fact that 2004 is the centenary of
Legg’s lecture at Hartford describing the condition,
there is more that is not known about Perthes’ than
is known. We do not know what causes Perthes’. We
certainly do not know what is the best way to treat
it. We are unsure of the outcome. These factors
have led to a heterogeneity of different treatment
modalities, ranging from the highly invasive to the
fully nihilistic. Very few studies are available that
give any insight into the long-term effects of the
condition.
Epidemiology
Even the incidence of Perthes’ disease is contro-
versial. Incidences are quoted per 100,000 of the
ARTICLE IN PRESS
KEYWORDS
Perthes’ disease;
Clinical features;
Investigation;
Treatment
*Tel.: þ 44-115-924-9924.
0268-0890/$ - see front matter & 2004 Elsevier Ltd. All rights reserved.
doi:10.1016/j.cuor.2004.06.001
Current Orthopaedics (2004) 18, 273–283

population but also per 100,000 children.
It is
probably 1.5 to 4 cases per 100,000 of the popula-
tion, leading to a prevalence of between 6 and 12
per 100,000 of the child population. Higher inci-
dences of Perthes’ disease outside this range are
quoted, particularly for some urban areas.
The male
to female ratio is 6:1. The incidence of bilateral
Perthes’ disease is approximately 25% and in the
majority of these cases the disease does not occur
synchronously in each hip. If it does, alternative
causes should be considered, the most common of
which would be multiple epiphyseal dysplasia.
Aetiology
Theories on the aetiology of Perthes’ are multiple
and difficult to disentangle.
Growth patterns
A constant feature in papers that describe the
epidemiology and aetiology of Perthes’ is that
patients are relatively immature in that they have
delayed bone age. This was noted particularly by
Wynne-Davis and Gormley in Scotland, but also in
Birmingham and more recently in Coventry.
The
delayed bone age has been reflected in the short
stature of patients and some have found evidence
of reduced growth factors, such as somatomedins,
in patients with Perthes’ disease. Although true
bilaterality only occurs in 25%, some investigators
have found abnormalities of the contra-lateral hip,
which they believe represent the growth abnorm-
alities that cause the condition.
Genetic factors
The role of genetic factors is controversial. Wynne-
Davis originally felt that the factors affecting the
incidence of Perthes’ disease were environmental
rather than genetic. Clustering in families has,
however, been described on several occasions. It is
clear, however, that Perthes’ is not a straightfor-
ward genetic condition with a predictable mode of
inheritance.
Environment
A number of different environmental influences
have been suggested. In both Scotland and Liver-
pool, poverty has been suggested as an aetiological
factor and this came to be associated with an urban
environment.
More recently, it has been suggested
that a rural environment might be associated more
with poverty and Perthes’ disease.
Add to this that
there are several studies suggesting that there is no
relationship between the environment and Perthes’
disease and the situation is even more confusing. It
does seem to be true that the urban clustering
previously described is in fact a feature of popula-
tion density rather than true effect and this has
been most satisfactorily demonstrated in Northern
Ireland, where population mobility is more limited
and therefore long-term follow-up for epidemiol-
ogy more easy to achieve.
Trauma
The onset of symptoms is frequently associated in
the mind of patient and parent with a traumatic
episode. Until the 1950’s most aetiological theories
centred around trauma or repetitive trauma.
However, at the peak ages of Perthes’ there is no
difference in the amount and type of physical
activity taken by boys and girls, so other factors
would have to explain the discrepancy of inci-
dence.
Thrombosis and fibrinolysis
Over the last decade, interest has been focused on
abnormalities of thrombosis and fibrinolysis in the
genesis of Perthes’. Glueck originally described a
16-fold incidence of Protein C and S deficiency
(causes of thrombophilia) in patients with Perthes’
disease in Ohio, compared to controls.
Other
investigators, attempting to repeat this work,
found different abnormalities of clotting, not all
of which might be associated with a thrombotic
tendency.
Several groups have described an
association between Perthes’ and passive smoking.
Smoking has an effect on tissue plasminogen
activator levels supporting the thrombotic theory,
but is also potentially a cause of small stature and
delayed bone age. Perthes’-like changes can be
produced in the femoral head by vascular experi-
ments involving interruption of the blood supply,
particularly if this was done twice, the so-called
second infarction theory. Other investigators have
demonstrated increased blood viscosity in patients
with Perthes’ and also intra-osseous venous hyper-
tension.
Against this, a series of investigators have found
no abnormalities of the measurable parameters of
thrombosis and fibrinolysis and others have pointed
out that in the few histological specimens of
Perthes’ available, thrombosis was not a feature.
The current concept of clotting and fibrinolysis is
extremely complex. The clotting cascade is a
ARTICLE IN PRESS
274
J.B. Hunter

concept of the past and factors interact with each
other in a far from straightforward manner. Added
to this, are the considerable difficulties of perform-
ing investigations on clotting factors. Although the
jury remains out on the relationship between
thrombosis and fibrinolysis with Perthes’, further
study is definitely still merited.
Irritable hip
Episodes of transient synovitis were thought to be
associated with an increased incidence of Perthes’
disease. In fact, the relationship is the other way
round. The initial presentation of Perthes’ is that of
an irritable hip, sometimes with synovitis and
effusion. The synovitis is triggered by the subchon-
dral fracture and the initial collapse. It is certainly
not worthwhile following up all cases of transient
synovitis to see if they were early Perthes’ disease.
Natural history
The natural history of Perthes’ is normally de-
scribed in terms of the progression of the radi-
ological appearances. The clinical course of the
disease is very unpredictable. Some cases do not
present until they are well into the healing phase
and some restriction of movement or an awkward
gait has been noted, whereas others present with
pain and stiffness before any but the most subtle
radiological signs are visible.
The natural history was originally described by
Waldenstrom, whose classification is interesting, in
that the active stages of the disease were all
crammed into what he described as the evolu-
tionary stage of the disease. He felt that the
disease was prolonged in extent and this certainly
can be the case. More recently, Joseph’s group from
India have popularised the use of a classification
modified from the Elizabethtown classification,
which divides the condition into four stages;
sclerotic,
fragmentation,
healing
and
healed
(
and
This natural history study
also records the median duration of each stage and
the morphological changes as they occur, recording
the timing of epiphyseal extrusion, metaphyseal
widening and the appearance of adverse changes,
suggesting that deformation of the epiphysis occurs
during the late stage of fragmentation or in the
early stage of revascularisation. This has led to
their recommendation that any containment sur-
gery be performed before the late stage of
fragmentation. This is an important study and
together with its companion piece on the timing
of intervention for Perthes’ represents a major
contribution to the understanding of Perthes’.
Pathology
The information on the pathology of Perthes’ is
poor because it is a non-lethal condition with active
stages during childhood. Few full pathological
specimens are available and much of the informa-
tion comes from small biopsies and curettings.
It
was fairly well established that there is thickening
of the articular epiphyseal cartilage. The bony
epiphysis and the deep layers of epiphyseal
cartilage are affected by the ischaemic process
and infarct, whilst the superficial layers of the
articular cartilage continue to gain nourishment
from the joint and synovial fluid. In severe
Perthes’, the physis itself is disrupted with distor-
tion of the physeal columns and the formation of
irregular cell columns and cartilage. The physeal
distortion is seen radiologically as the metaphyseal
cysts and Gage sign. Both of these ‘‘cysts’’ in fact
contain unossified columns of cells from the
distortion of the physis. The fragmentation of the
bony epiphysis is the beginning of the repair
process, with infarcted and damaged structures
being removed prior to reossification.
Prognosis
The long-term complication for patients with
Perthes’ disease is osteoarthritis. The long-term
follow-up from Iowa shows that at 40 years of
follow-up (i.e. patients in their late 40’s and 50’s),
40% had had a joint replacement, 10% had disabling
arthritis that warranted a joint replacement and a
further 10% had Iowa hip scores less than 80.
Groups of patients followed up for less than 40
years appear to be functioning well. Between 20
and 40 years of follow-up, the majority of patients
ARTICLE IN PRESS
Table 1
Modified Elizabethtown classification of
disease natural history and median duration of
each stage.
Modified Elizabethtown classification
Days
I Sclerotic
220
A no loss height B height loss
II Fragmentation
240
A early B late
III Healing
550
A peripheral B41/3 epiphysis
IV Healed
Legg Calve
´ Perthes’ disease
275
ARTICLE IN PRESS
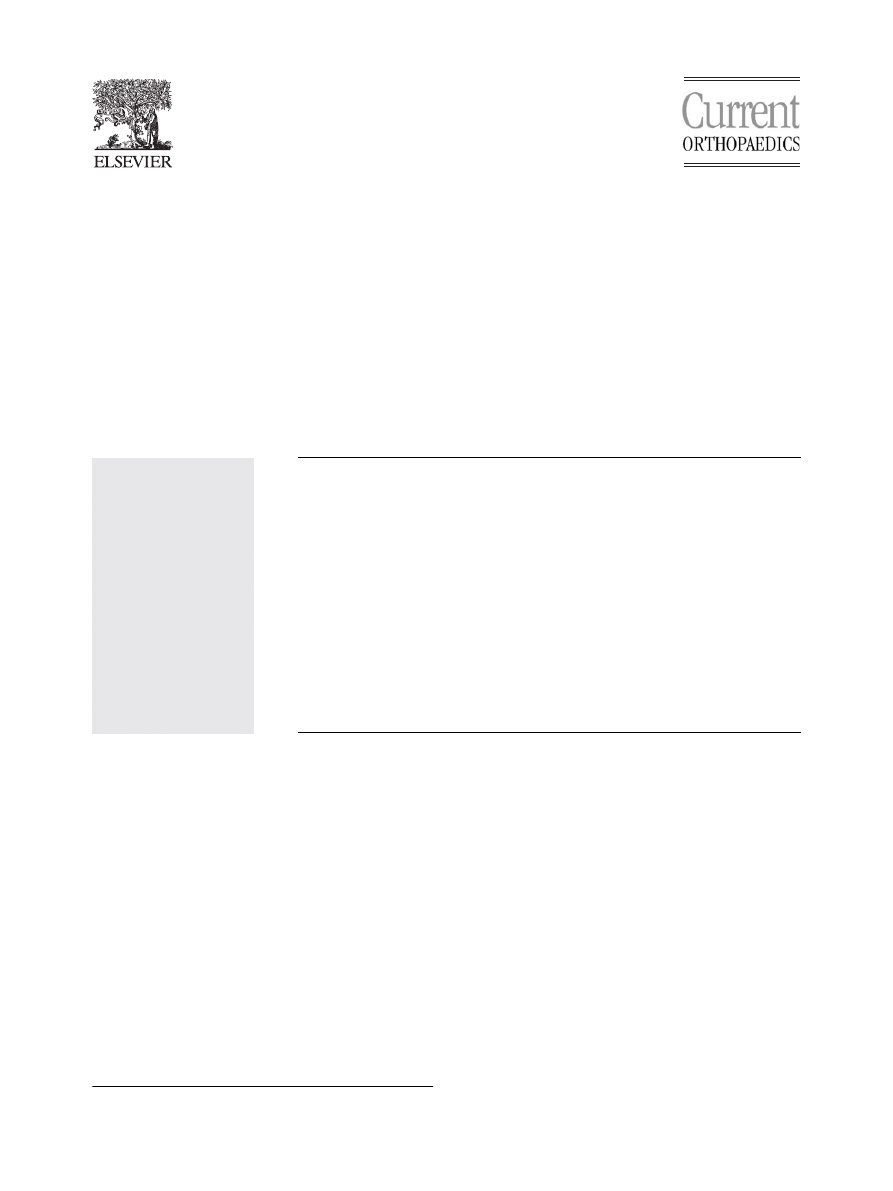
Figure 1 The stages of Perthes’ (a) Sclerotic with a sub-chondral fracture, (b) early fragmentation (femoral osteotomy
performed), (c) early healing, peripheral only, (d) late healing, (e) head healed, result is Stulberg 1, Mose good.
276
J.B. Hunter
(70–90% depending on the series) are functioning
well with little pain, despite abnormal X-rays.
The factors affecting the prognosis have histori-
cally been given as the age at onset and the shape
of the femoral head at maturity. Female gender
was thought to be a poor prognostic fracture, but
the evidence for this is limited and if the ages of
girls with Perthes’ are corrected for skeletal
maturity, their prognosis appears to be much the
same as boys. An onset of Perthes’ before the age
of 5 appears to have a good prognosis with an onset
after the age of 8 carrying a poor prognosis. This
leaves a considerable indeterminate area and
Snyder and others have reported poor results even
in very young patients with Perthes’.
Much effort has focused on judging the shape of
the femoral head at maturity. Two methods are
commonly used, the classification of Stulberg et al
and the concentric ring method of Mose
). Neither is completely reliable.
Doubts have been cast on the intra- and inter-
observer reliability of the Stulberg classification
and in the Iowa series, even completely round
femoral heads, as judged by Mose, had severe
arthritis by the middle of their seventh decade,
although no arthritis in their 30’s.
The classic results of Catterall suggested that
less severe disease carried a better prognosis.
Follow-up was to six years (so not extensive) and
the outcome grade was that devised by Sundt,
which has not been widely used. The results suggest
that 50% or more of patients with Perthes’ do
extremely well with no intervention and this has
led to the development of severity gradings to be
applied during the course of the disease to select
appropriate patients for intervention.
ARTICLE IN PRESS
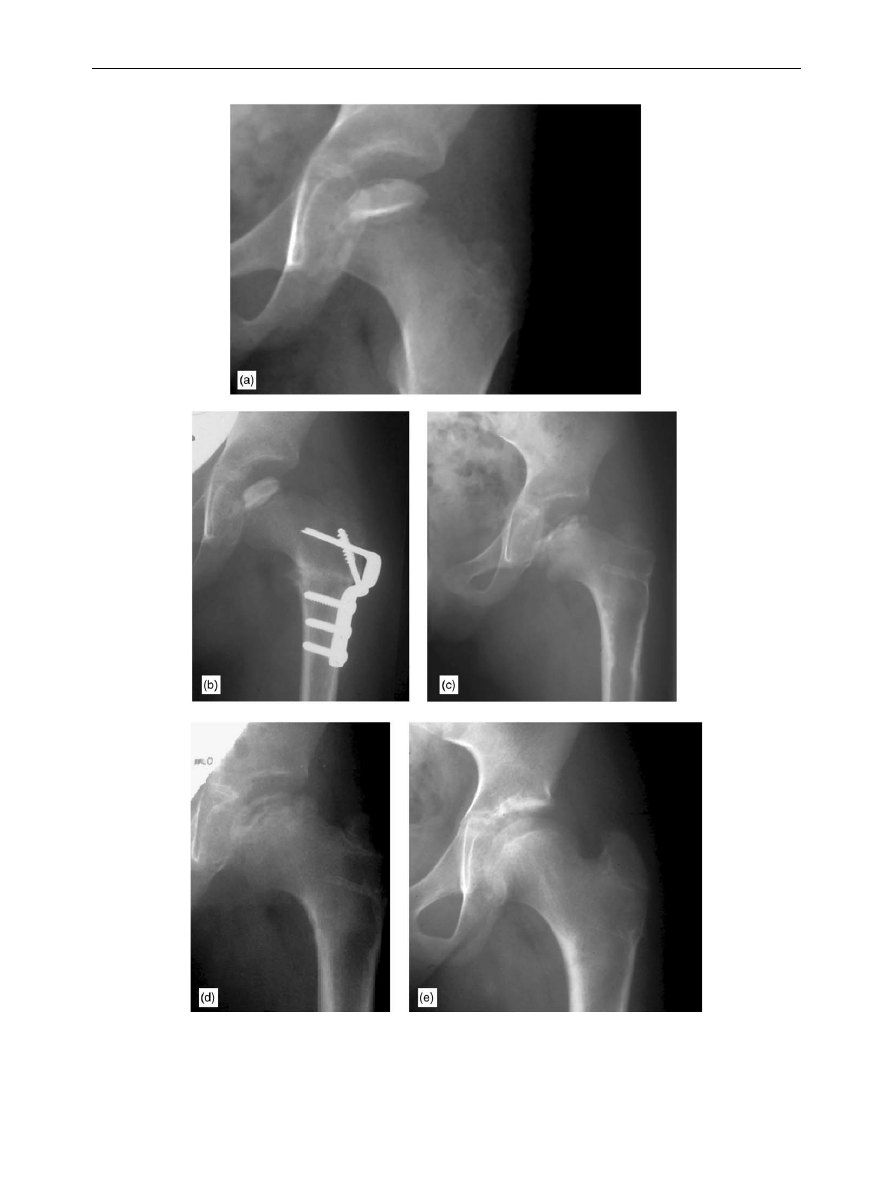
Figure 2 Example Stulberg outcome grades. (a) Grade 2, (b) Grade 3, (c) Grade 4, and (d) Grade 5.
Legg Calve
´ Perthes’ disease
277
Severity gradings in Perthes’ disease
Although the form and duration of interventions is
unclear, there is merit in trying to judge the
severity of the disease early in its natural history,
in order to spare those patients, for whom the
prognosis is good, the inconvenience of any inter-
vention whatsoever. There are three classification
systems in current use, all with their own advan-
tages and disadvantages. It is useful to determine
early in the disease whether more or less than 50%
of the femoral head is involved and especially to
determine whether a very large proportion is
involved. When less than 50% of the head is
involved the intact portion of head acts as
scaffolding for the repair process, maintaining
femoral head height and shape. This is not the
case when a larger proportion of the head is
involved
Fsevere collapse, extrusion and defor-
mity follow. A working knowledge of each of the
classification systems is useful because at different
times in the evolution of the disease each of the
systems is more applicable.
Early in the disease the most useful classification
is that of Salter and Thompson (
). This is
based on the extent of the subchondral fracture
that occurs in the sclerotic phase of the disease.
If the subchondral fracture indicates that more
than 50% of the head is going to be involved, then
early action may be indicated. The subchondral
fracture, however, is only seen in about 40% of
cases with Perthes’ and frequent X-rays may need
to be taken at the commencement of the condition
in order to visualise it at its fullest extent. My
personal practice, as regards the subchondral
fracture, is to take X-rays at six-week intervals in
the early stages of Perthes’ in order to obtain early
guidance as to the extent of the disease.
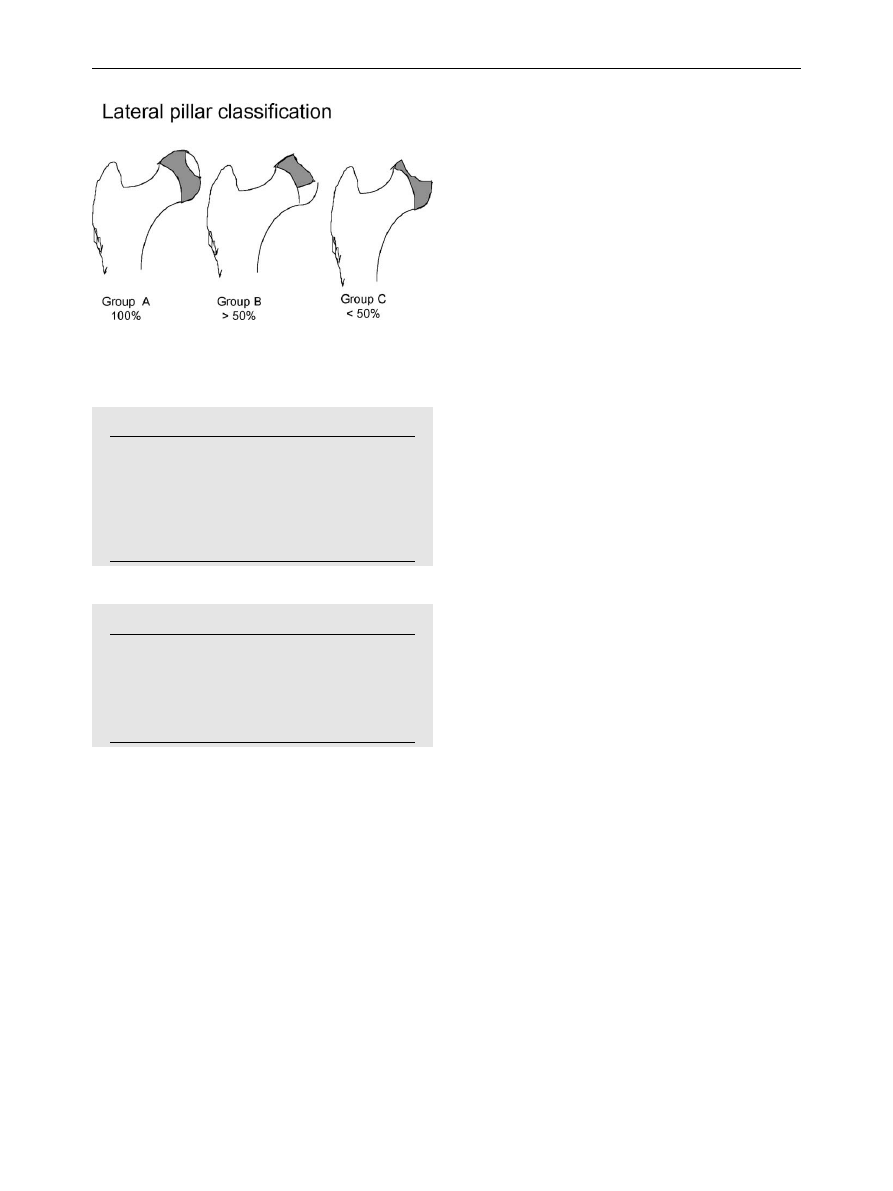
The lateral pillar classification of Herring was
published in 1992.
Femoral heads are classified
into three groups, depending on the maintenance
of height of the lateral pillar of the femoral head,
compared to the height of the lateral pillar on the
opposite normal side (
). Many investigators
have demonstrated that maintenance of lateral
femoral head height is associated with a reduction
in deformity and prevention of extrusion. The
advantages of the lateral pillar classification is that
it requires only an AP radiograph and the measure-
ments are easy to perform and to understand. The
disadvantages are that the definitive measurement
must be made at the fullest extent of fragmenta-
tion (i.e. well into the course of the disease and
therefore after the most suitable time for inter-
vention), that it is not suitable for bilateral
disease, and that femoral heads may progress from
one category to the other. Added to this, Herring
has recently presented work which has blurred the
edges of his categories making the classification
less easy to understand and to apply.
The Catterall classification was introduced in his
paper of 1971. Femoral heads are classified into
four groups and this classification too must be done
ARTICLE IN PRESS
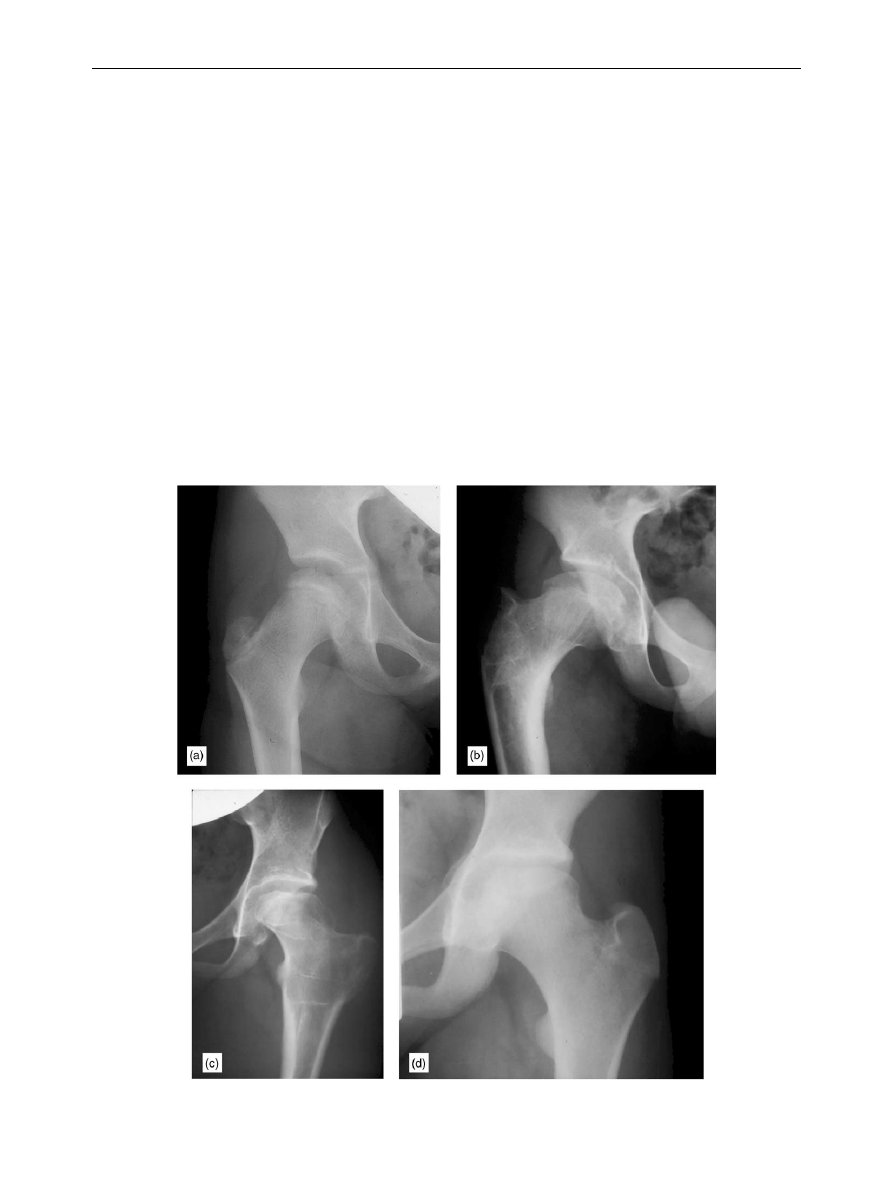
Figure 3
Mose’s method of grading result with con-
centric circles.
Table 2
Stulberg outcome grades. There is an
increased tendency to premature osteoarthritis
with increasing grade.
Stulberg outcome grades.
I Completely normal
II Spherical with coxa magna/short neck/steep
acetabulum
III Not spherical but not flat ie umbrella or
mushroom shaped
IV Flat head with abnormal head/neck/acetabulum
V Flat head with normal head/neck/acetabulum
Figure 4
The sub-chondral fracture line which is the
basis of the Salter Thompson classification of severity.
This is Grade B, the more severe, as more than 50% of the
head is fractured.
278
J.B. Hunter
during the fragmentation stage, when the fullest
extent of epiphyseal involvement has been estab-
lished. Essentially, groups 1 and 2 have less than
50% head involvement and groups 3 and 4 greater
than 50% head involvement and thus the classifica-
tion can be used if no subchondral fracture line has
been visualised. Paediatric orthopaedic surgeons
have not universally found this an easy classifica-
tion to use and there have been some doubts cast
on its intra- and inter-observer reliability. The
classification puts considerable emphasis on meta-
physeal involvement and this certainly seems
appropriate as metaphyseal involvement is asso-
ciated with premature growth plate fusion and the
presence of final deformity.
In addition to the basic classification, Catterall
has introduced the clinical and radiological signs of
the head at risk (
). The clinical signs
of the head at risk are extremely important,
because although research papers on Perthes’ focus
considerably on radiological appearances, the
management of the child with Perthes’ needs to
be guided, particularly in the younger age group, by
the clinical state. Of the radiological signs, it was
originally stated that the presence of two or more
of these signs was an indicator of a poor prognosis
and therefore, since the signs appeared to be
reversible, an indication for intervention.
Investigations
Plain X-rays
AP and lateral X-rays of the hips are the mainstay of
investigation for Perthes’. Perthes’ is a protracted
disease and the repeatability of plain X-rays
enables the course of the disease to be charted.
MRI
Several classifications of Perthes’ disease based on
MRI appearances have been proposed. At this stage,
none has gained acceptance, because they have not
proved definitively prognostic and the necessity for
repeated imaging studies in Perthes’ is inconveni-
ent and expensive in the context of Perthes’.
Bone Scan
Many groups have described the benefits of using
isotope bone scanning in Perthes’. The groups in
Montpelier and Chicago suggest that pinhole colli-
mation (which provides a far more detailed picture)
is useful in recording the viability of the lateral
column of the epiphysis. This in turn may predict
deformity. Conventional bone scanning without
collimation would appear to have no role.
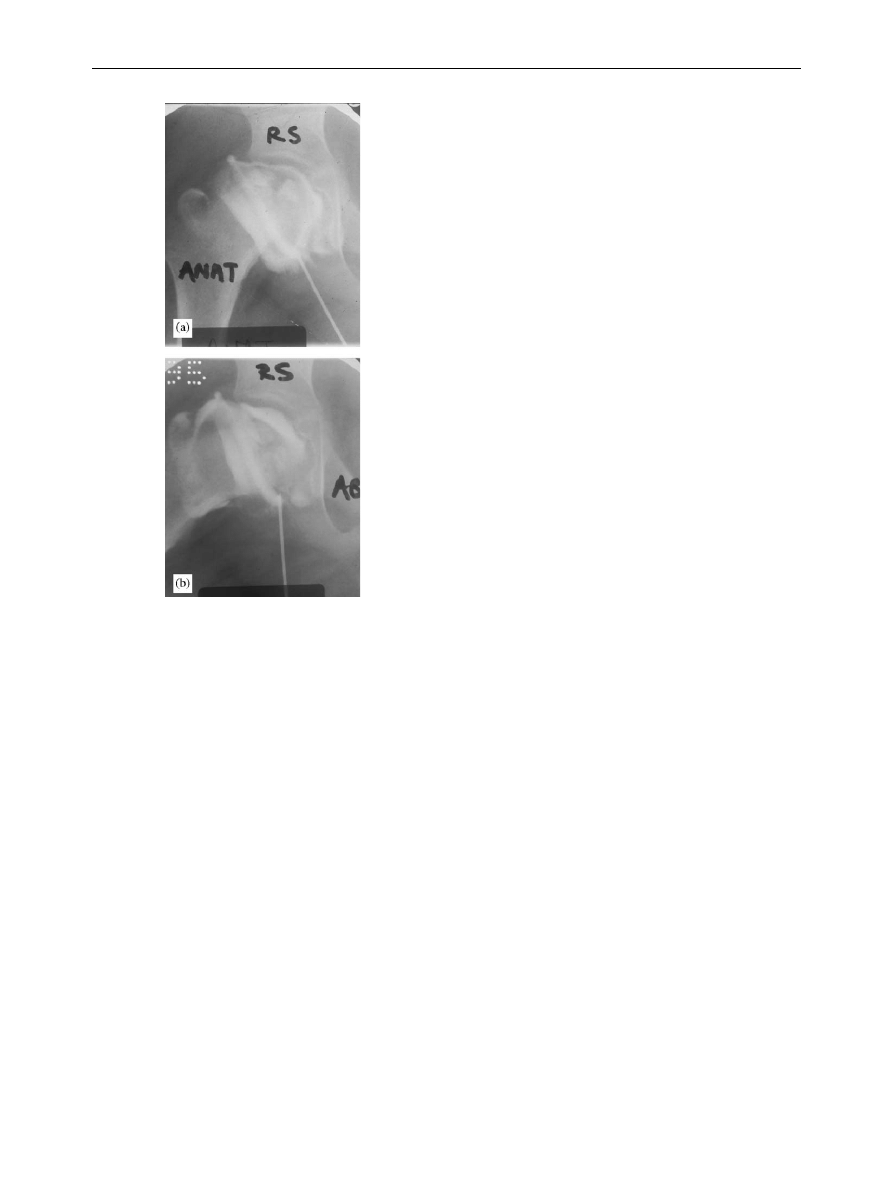
Arthrography
The arthrogram is an important investigation of the
child for whom intervention is being considered.
Catterall emphasises the importance of the arthro-
gram being dynamic. The surgeon must certainly
view how the hip moves, as medial pooling occurs
both with a flattened head that moves congruently
and with hinge abduction (
). An arthrogram
may demonstrate whether the hip is containable
(i.e. the area of disease can be located satisfacto-
rily within the acetabulum) or in non-containable
hips may demonstrate the position of best fit prior
to valgus or valgus extension osteotomy.
ARTICLE IN PRESS
Table 4
The signs of the head at risk, clinical.
Clinical ‘‘At risk’’ signs
Older child
Heavy child
Progressive loss of movement
Adduction contracture
Flexion with adduction
Table 3
The signs of the head at risk, radiological.
‘‘At risk’’ signs
Radiological
Gage sign
Calcification lateral to the epiphysis
Subluxation
Epiphyseal angle
Diffuse metaphyseal reaction
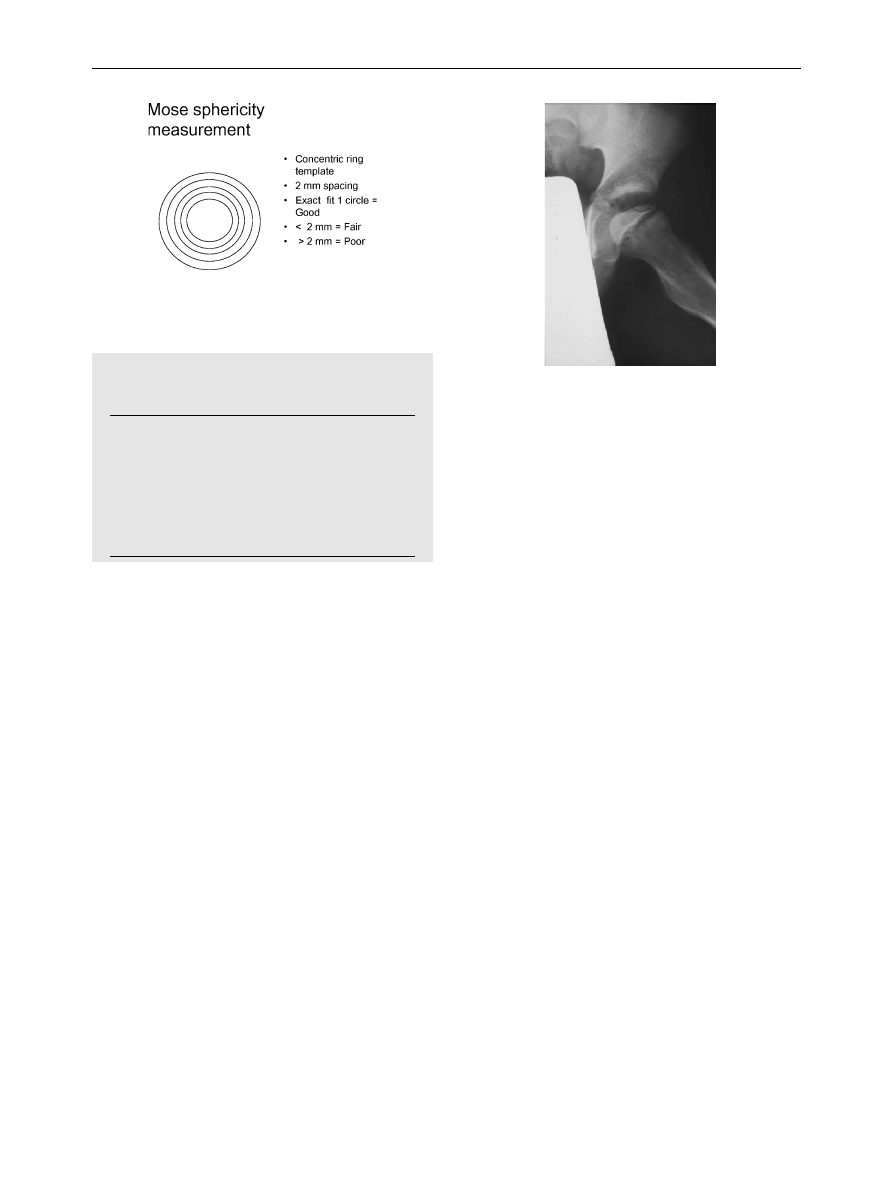
Figure 5
The lateral pillar classification. Children in
Group A and younger children in Group C had a good
result.
Legg Calve
´ Perthes’ disease
279
Theories of treatment
Relief from weight-bearing
Because the natural history of the condition
indicates collapse and extrusion to be associated
with femoral head deformity and therefore it is
assumed a poor result, the earliest treatments
available involved prolonged relief of weight-
bearing whilst healing was allowed to progress. In
some cases this resulted in many years of bed rest
with or without an abduction frame.
Other
methods of relief of weight-bearing involved trac-
tion and the use of the Snyder sling, which kept the
affected leg in the Long John Silver position.
Containment
The main theory proposed for the treatment of
Perthes’ disease is that of containment. Essentially,
the injured femoral head is secured within the
socket and kept moving in order that after
regeneration it should be round and fully mobile.
The methods used to achieve this have varied from
plaster casts, various forms of orthotic braces to
operations. The theoretical basis of containment
was supported by animal experiments performed
on pigs.
Femoral heads subjected to an ischaemic
insult but then contained within the acetabulum of
the pig reformed a satisfactory shape, whilst those
that were not contained did not. There are some
important differences between the hips of pigs and
men; most notably the pig’s acetabulum is suffi-
ciently large to contain the entire femoral head,
which is not possible in the human. However, it is
probably
that
effective
containment
can
be
achieved if redirection into the socket is combined
with effective movement.
Containment can be achieved by orthotics or
plasters that go below the knee to effectively
control both abduction and rotation of the femur.
There is plenty of evidence to show that orthotics
that remain above the knee do not effectively
contain the hip. The use of above knee braces has
been demonstrated to be ineffective.
The
prolonged use of below knee plasters does not
allow free movement of the hip and may be
instrumental in promoting uniplanar movement of
the joint. Given the psychological problems asso-
ciated with prolonged wearing of a brace and the
dangers of missing the opportunity of surgical
intervention in the older age group, surgery seems
to be the best way to obtain containment in the
21st century. Surgical containment can be achieved
by operating either on the proximal femur or the
pelvis or indeed both.
Proximal femoral osteot-
omy is a simple and effective procedure, but in
older children may result in some shortening and an
overriding trochanter.
More and more involved
acetabular surgery has been proposed for Perthes’
over the years and provided these procedures can
be done effectively and without complication, they
are more or less equally effective
(
).
Surgical methods that do not require extensive
and prolonged immobilisation are to be preferred
because a stiff hip is never a good result. The
timing of surgery may be crucial. Certainly, opera-
tions should be done as soon as possible after it is
decided they are required. In the older child or
early adolescent this should be before there is
significant collapse of the femoral head. Early
surgery may accelerate the natural history and
indeed the fragmentation stage may be avoided
altogether after appropriate early surgery.
Although this is the centenary of Perthes’, there
are no good quality comparative studies of treat-
ment modalities. The older studies contained very
little information on the severity of the Perthes’
that was being treated and there are no modern
ARTICLE IN PRESS
Figure 6 Hinge abduction of the femoral head demon-
strated on arthrogram.
280
J.B. Hunter

randomised studies. Over the last decade an
American multi-centre study, which is essentially
a set of synchronous case series, has been
conducted under the auspices of Dr Herring.
Publication is awaited. The initial presentation
suggested that all conservative methods performed
the same as each other, as did all operative
methods.
In the age group 8 and over, there
appeared to be clear benefit from being treated by
surgery. Surgery reduces the duration of the disease
and results in rounder femoral heads.
Salvage procedures
Children who have had Perthes’ and present with
deformed femoral heads, difficulties walking, stiff-
ness and pain, require treatment, even if that
treatment cannot be with the objective of creating
a round femoral head at maturity. The most
frequent cause of pain and stiffness is hinge
abduction, when the extruded lateral segment of
epiphysis impinges on the lateral border of the
acetabulum.
Abduction osteotomy
This osteotomy is designed to remove the impinging
segment of epiphysis from the lateral wall, allowing
the foot to be placed comfortably underneath the
pelvis and a more normal gait. It is effective at
reducing pain. In the best circumstances, because
of the restoration of movement, remodelling of the
femoral head occurs and very good results have
been reported for this procedure from Catterall. It
is important that this procedure not be performed
too early. Healing needs to have started before
abduction osteotomy is performed. There is a
conflict in the literature as to whether the
abduction should be combined with flexion or
extension. The former would better remove the
affected segment from the acetabulum, the latter
deal better with any fixed flexion.
Cheilectomy/recreation of offset
An alternative approach to the extruded fragment
is to remove it surgically. As originally proposed this
operation was done through an anterolateral
approach with simple excision of the fragment.
Many orthopaedic surgeons have had poor experi-
ences with this procedure. Stiffness of the hip joint
has been a frequent sequela and more seriously,
removal of the perichondral ring, together with the
fragment, has resulted in slipped upper femoral
epiphysis of the remaining epiphysis. This operation
had fallen into disuse until repopularised by the
Bern group, who have performed it in association
with trochanteric distalisation and surgical disloca-
tion of the hip.
When performed on a hip with an
open physis they have always stabilised the
epiphysis to prevent slipped upper femoral epiphy-
sis. Reshaping of the femoral head and recreating
the femoral offset in the manner they describe is
certainly a more thorough approach than ‘‘bum-
pectomy’’ and the long-term results of this are
awaited.
Hip Arthroscopy
Occasionally in Perthes’, healing of the epiphysis is
incomplete and patients complain of symptoms
suggestive of a loose body. If this is truly the case,
then hip arthroscopy can be very useful. It should
be noted that sometimes the ‘‘loose body’’ is not
loose at all and detaching it from the femoral head
arthroscopically can be extremely difficult.
Conclusion
Many controversies remain in Perthes’. These
algorithms are presented as a way through the
maze of contradictory and incomplete evidence
(
). Catterall has emphasised the
importance of clinical examination in the assess-
ment of cases of Perthes’ and this is particularly
important in the younger group, many of whose
hips heal very round, despite rather adverse-
looking X-rays early on, because they have main-
tained an excellent, almost normal, range of
movements. The older child or early adolescent
with Perthes’ requires urgent attention, as the
ARTICLE IN PRESS
Figure 7
Lateral augmentation acetabuloplasty for
severe Perthes’.
Legg Calve
´ Perthes’ disease
281
femoral head lacks the regenerative capacity of the
younger child. Before any operation in Perthes’,
action must be taken to unstiffen the hip. Contain-
ment procedures will fail if performed on a stiff hip
and even salvage procedures are best performed on
a hip that has been loosened as much as possible.
Surgeons need to recall that most untreated
Perthes’ do not require intervention until the age
of 40. If our interventions on the child result in hip
replacement being required in the 20’s, then we
have not done that patient a service.
References
1. Kealey WD, Moore AJ, Cook S, Cosgrove AP. Deprivation,
urbanisation and Perthes’ disease in Northern Ireland. J
Bone Joint Surg Br 2000;82(2):167–71.
2. Hall AJ, Barker DJ, Dangerfield PH, Taylor JF. Perthes’
disease of the hip in Liverpool. Br Med J Clin Res
1983;287(6407):1757–9.
3. Wynne-Davies R, Gormley J. The aetiology of Perthes’
disease. Genetic, epidemiological and growth factors in
310 Edinburgh and Glasgow patients. J Bone Joint Surg Br
1978;60(1):6–14.
4. Harrison MH, Turner MH, Jacobs P. Skeletal immaturity in
Perthes’ disease. J Bone Jt Surg Br 1976;58(1):37–40.
5. Barker DJ, Hall AJ. The epidemiology of Perthes’ disease.
Clin Orthopaed Relat Res 1986;209:89–94.
6. Glueck CJ, Glueck HI, Greenfield D, et al. Protein C and S
deficiency, thrombophilia, and hypofibrinolysis: pathophy-
siologic
causes
of
Legg-Perthes
disease.
Pediat
Res
1994;35(4 Pt 1):383–8.
7. Glueck CJ, Crawford A, Roy D, Freiberg R, Glueck H, Stroop
D. Association of antithrombotic factor deficiencies and
hypofibrinolysis with Legg-Perthes disease. J Bone Jt Surg
Am 1996;78(1):3–13.
8. Kealey WD, Mayne EE, McDonald W, Murray P, Cosgrove AP.
The role of coagulation abnormalities in the development of
Perthes’ disease. J Bone Jt Surg Br 2000;82(5):744–6.
9. Glueck CJ, Freiberg RA, Crawford A, et al., Secondhand
smoke, hypofibrinolysis, and Legg-Perthes disease. Clin
Orthop 1998;352:159–167.
10. Hresko MT, McDougall PA, Gorlin JB, Vamvakas EC, Kasser JR,
Neufeld EJ. Prospective reevaluation of the association
between thrombotic diathesis and Legg-Perthes disease.
J Bone Jt Surg Am 2002;84-A(9):1613–8.
11. Joseph B, Varghese G, Mulpuri K, Narasimha Rao KL, Nair NS.
Natural evolution of Perthes disease: a study of 610 children
under 12 years of age at disease onset. J Pediatr Orthop
2003;23(5):590–600.
12. Joseph B, Nair NS, Narasimha Rao KL, Mulpuri K, Varghese G.
Optimal timing for containment surgery for Perthes disease.
J Pediatr Orthop 2003;23(5):601–6.
13. Catterall A, Pringle J, Byers PD, et al. A review of the
morphology of Perthes’ disease. J Bone Jt Surg Br 1982;
64(3):269–75.
14. McAndrew MP, Weinstein SL. A long-term follow-up of
Legg-Calv
!e-Perthes disease. J Bone Jt Surg Am 1984;
66(6):860–9.
15. Snyder C. Legg-Perthes disease in the young hip: does it
necessarily do well? J Bone Jt Surg 1975;57-A:751–9.
16. Fabry K, Fabry G, Moens P. Legg-Calv
!e-Perthes disease in
patients under 5 years of age does not always result in a
good outcome. Personal experience and meta-analysis of
the literature. J Pediatr Orthop B 2003;12(3):222–7.
17. Stulberg SD, Cooperman DR, Wallensten R. The natural
history of Legg-Calv
!e-Perthes disease. J Bone Jt Surg Am
1981;63(7):1095–108.
18. Mose K. Methods of measuring in Legg-Calv
!e-Perthes disease
with special regard to the prognosis. Clin Orthop Relat Res
1980;150:103–9.
19. Neyt JG, Weinstein SL, Spratt KF, et al. Stulberg classifica-
tion system for evaluation of Legg-Calv
!e-Perthes disease:
intra-rater and inter-rater reliability. J Bone Jt Surg Am
1999;81(9):1209–16.
20. Weinstein SL. Natural history, treatment outcomes of child-
hood hip disorders. Clin Orthop 1997(344):227–42.
21. Catterall A. The Natural History of Perthes’ Disease. J Bone
Jt Surg 1971;53-B(1):37–53.
22. Salter RB, Thompson GH. Legg-Calv
!e-Perthes disease. The
prognostic significance of the subchondral fracture and a
two-group classification of the femoral head involvement.
J Bone Jt Surg Am 1984;66(4):479–89.
23. Herring JA, Neustadt JB, Williams JJ, Early JS, Browne RH.
The lateral pillar classification of Legg-Calv
!e-Perthes dis-
ease. J Pediat Orthop 1992;12(2):143–50.
24. Herring JA, Kim HK, Browne R. Legg-Calv
!e-Perthes disease: a
multicenter trial of five treatment methods. In: POSNA;
2003; Amelia Island, Florida: Paediatric Orthopaedic Society
of North America. Rosemont, Illinois; 2003. p. 26.
25. Catterall A. Legg-Calv
!e-Perthes syndrome. Clin Orthop
1981(158):41–52.
ARTICLE IN PRESS
Table 6
Algorithm for management of younger
child with Perthes.
Algorithm: Age 7 and below
Stage and percentage involvement
Clinically good
Fconservative with regular
review
Clinically bad/head at risk: arthrogram
If containable operation
If not
Make containable and operate
Conservative and salvage
Table 5
Algorithm for management of older child
with Perthes’. Operation should be performed early
before any fragmentation and collapse.
Algorithm: Age 8 and above
Assess Elizabethtown stage and degree of
involvement (50%)
If healing; conservative Rx or salvage
If sclerotic or fragmented; arthrogram
If containable operation
If not
Make containable (soft tissue releases) and
operate
Conservative and salvage
282
J.B. Hunter
26. Comte F, De Rosa V, Zekri H, et al. Confirmation of the early
prognostic value of bone scanning and pinhole imaging of
the hip in Legg-Calv
!e-Perthes disease. J Nucl Med 2003;
44(11):1761–6.
27. Tsao AK, Dias LS, Conway JJ, Straka P. The prognostic value
and significance of serial bone scintigraphy in Legg-Calv
!e-
Perthes disease. J Pediatr Orthop 1997;17(2):230–9.
28. Brotherton BJ, McKibbin B. Perthes’ disease treated by
prolonged recumbency and femoral head containment: a
long-term appraisal. J Bone Jt Surg Br 1977;59(1):8–14.
29. Salter RB, Bell M. The pathogenesis of deformity in
Legg-Perthes’
disease:
an
experimental
investigation.
J Bone Jt Surg 1968;50B:436.
30. Martinez AG, Weinstein SL, Dietz FR. The weight-bearing
abduction brace for the treatment of Legg-Perthes disease.
J Bone Jt Surg Am 1992;74(1):12–21.
31. Meehan PL, Angel D, Nelson JM. The Scottish Rite abduction
orthosis for the treatment of Legg-Perthes disease. A
radiographic analysis. J Bone Jt Surg Am 1992;74(1):2–12.
32. Olney BW, Asher MA. Combined innominate and femoral
osteotomy for the treatment of severe Legg-Calv
!e-Perthes
disease. J Pediatr Orthop 1985;5(6):645–51.
33. Axer A, Gershuni DH, Hendel D, Mirovski Y. Indications for
femoral osteotomy in Legg-Calv
!e-Perthes disease. Clin
Orthop 1980(150):78–87.
34. Kumar D, Bache CE, O’Hara JN. Interlocking triple pelvic
osteotomy in severe Legg-Calv
!e-Perthes disease. J Pediatr
Orthop 2002;22(4):464–70.
35. Kim HT, Wenger DR. Surgical correction of ‘‘functional
retroversion’’ and ‘‘functional coxa vara’’ in late Legg-
Calv
!e-Perthes disease and epiphyseal dysplasia: correction
of deformity defined by new imaging modalities. J Pediatr
Orthop 1997;17(2):247–54.
36. Quain S, Catterall A. Hinge abduction of the hip. Diagnosis
and treatment. J Bone Jt Surg Br 1986;68(1):61–4.
37. Garceau G. Surgical treatment of coxa plana. J. Bone Jt Surg
1964;46-B(4):779–80.
38. Ganz R, Gill TJ, Gautier E, Ganz K, Krugel N, Berlemann U.
Surgical dislocation of the adult hip a technique with full
access to the femoral head and acetabulum without the risk
of avascular necrosis. J Bone Jt Surg Br 2001;83(8):1119–24.
39. Bowen JR, Kumar VP, Joyce JJ, 3rd, Bowen JC. Osteochon-
dritis dissecans following Perthes’ disease. Arthroscopic-
operative treatment. Clin Orthop 1986(209):49–56.
ARTICLE IN PRESS
Legg Calve
´ Perthes’ disease
283
Document Outline
- (iv) Legg CalvÕ Perthes’ disease
Wyszukiwarka
Podobne podstrony:
Osteochondritis dissecans in association with legg calve perthes disease
Interruption of the blood supply of femoral head an experimental study on the pathogenesis of Legg C
Modified epiphyseal index for MRI in Legg Calve Perthes disease (LCPD)
Hip Arthroscopy in Legg Calve Perthes Disease
Legg Calve Perthes’ disease
Legg Calve Perthes disease The prognostic significance of the subchondral fracture and a two group c
Computerized gait analysis in Legg Calve´ Perthes disease—Analysis of the frontal plane
Coxa magna quantification using MRI in Legg Calve Perthes disease
Osteochondritis dissecans in association with legg calve perthes disease
Interruption of the blood supply of femoral head an experimental study on the pathogenesis of Legg C
Intertrochanteric osteotomy in young adults for sequelae of Legg Calvé Perthes’ disease—a long term
Legg Calvé Perthes Disease in Czech Archaeological Material
Legg Calvé Perthes disease multipositional power Doppler sonography of the proximal femoral vascular
Multicenter study for Legg Calvé Perthes disease in Japan
Femoral head vascularisation in Legg Calvé Perthes disease comparison of dynamic gadolinium enhanced
A recurrent mutation in type II collagen gene causes Legg Calvé Perthes disease in a Japanese family
Acute chondrolysis complicating Legg Calvé Perthes disease
Legg Perthes disease in three siblings, two heterozygous and one homozygous for the factor V Leiden
Perthes Disease
więcej podobnych podstron