
Venous Thromboembolism
in the
general practice setting
.
Department of Family Medicine and Community Nursing.
Medical University of Bialystok, Poland. 2011
Jolanta Sawicka - Powierza

Polish guidelines for the prevention and
treatment of venous thromboembolism:
2009. Zawilska K, Jaeschke R, Tomkowski
W, Mayzner-Zawadzka E, Nizankowski R,
Olejek A, Pasierski T, Torbicki A, Undas A,
Jawień A, Gajewski P, Sznajd J, Brozek J. Pol
Arch Med Wewn. 2009;119 Suppl 1:1-69.
Review. Polish.

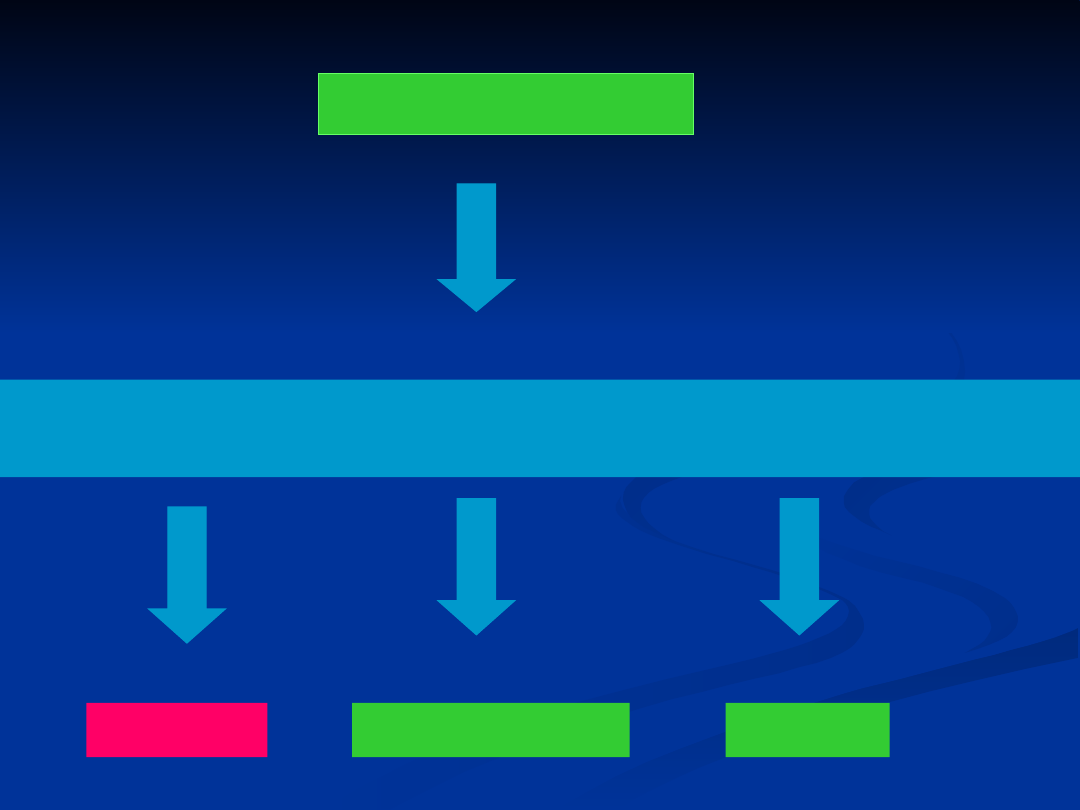
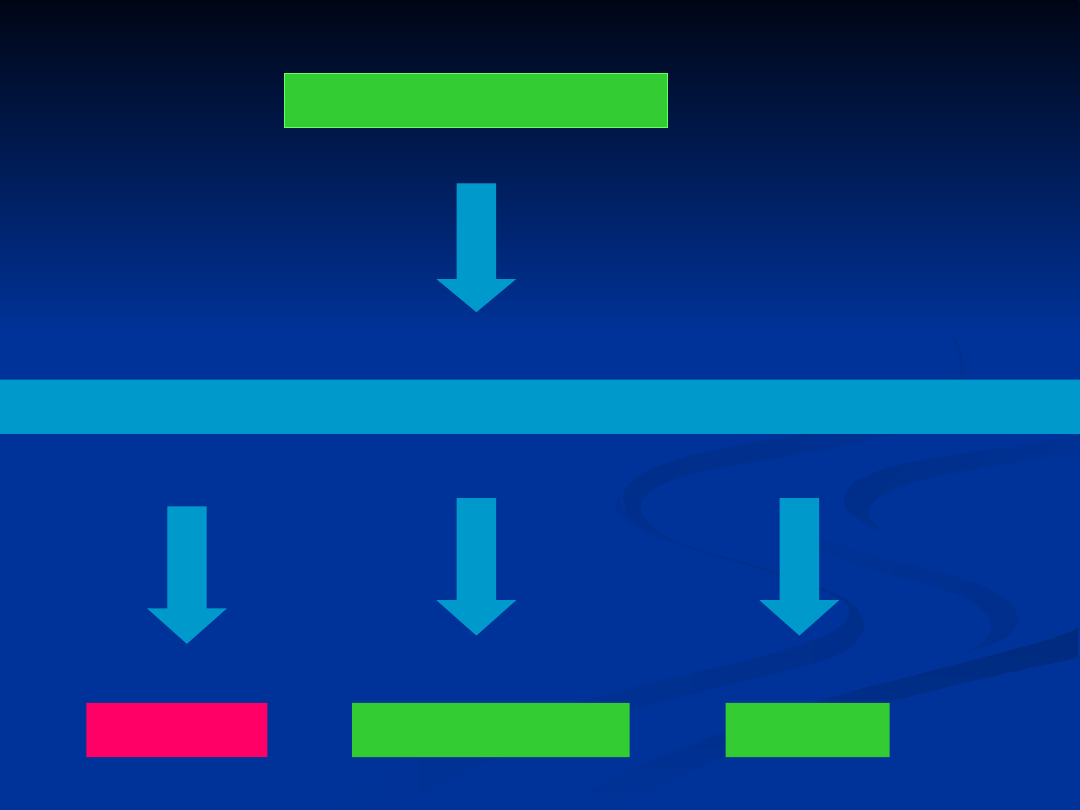
VTE (venous
thromboembolism)
mortality rates of 5-23%
DVT (deep vein
thrombosis)
PE (pulmonary embolism)

RISK FACTORS ASSOCIATED WITH VTE:
I. General
Older age
Immobility,
p
aresis
Ma
li
gnancy
O
b
esity
P
revious VTE
Family history of VTE
Oral contraceptive pill, hormone replacement,
tamoxifen
Venous insufficiency/varicose
v
eins

II.
High risk clinical situations
Surgery (especially hip and knee surgery or major
surgery for malignancy)
Pregnancy/puer
p
erium
Acute medical illness
Congestive cardiac and respiratory failure
Trauma
Central venous c
a
theter

III.
Diseases associated with a
prothrombotic state
Myeloproliferative disorders
Antiphospholipid syndrome
Paroxysmal nocturnal haemoglobinuria
Nephrotic syndrome
Hyperviscosity syndrome
Inflammatory bowel disease

IV.
Inherited thrombophilia
Factor V Leiden mutation
Antithrombin, protein C and protein S deficiency
Prothrombin gene mutation (Factor II G20210A
mutation
)
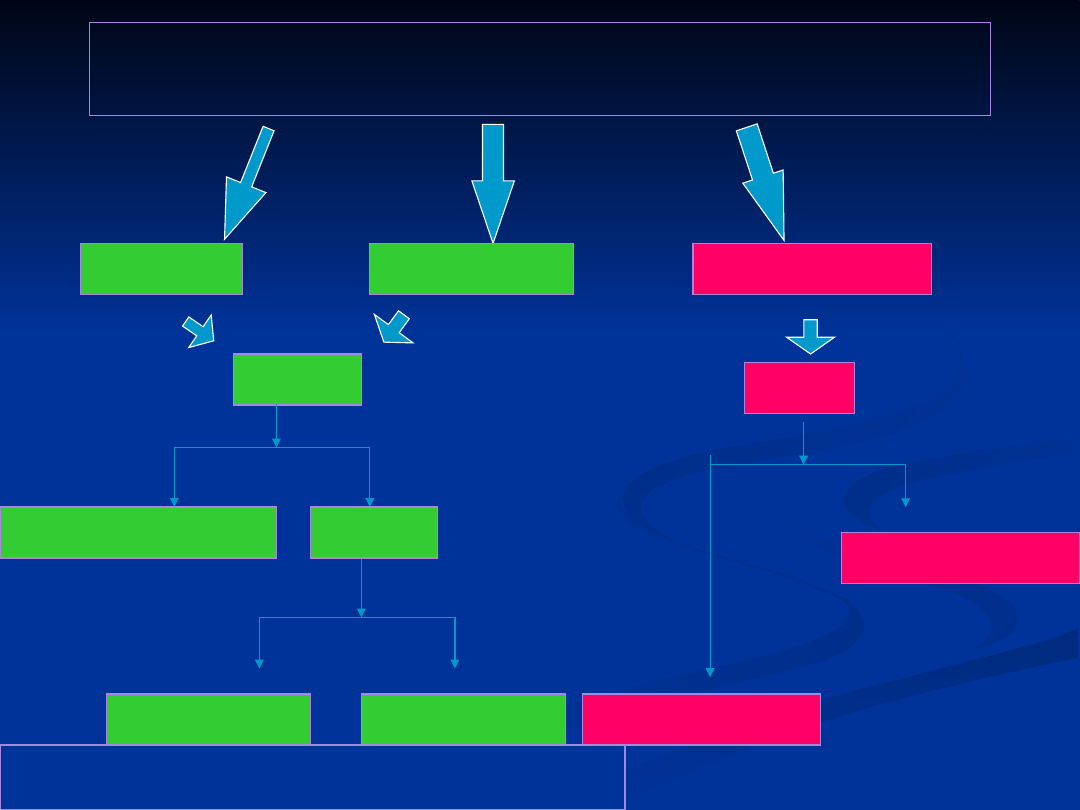
Assessment clinical probability
of DVT
due to the Wells
score
DVT suspected
high
low
moderate

Wells criteria
– Clinical probability of DVT
active cancer (treatment ongoing, within previous 6 months,
or palliative)
paralysis, paresis, or recent plaster immobilization of the
lower extremities
recently bedridden >3 days or major surgery within 4 weeks
localized tenderness along the distribution of the deep
venous system
entire leg swollen
calf swelling 3 cm larger than on the asymptomatic side
(measured 10 cm below tibial tuberosity)
pitting edema (greater in the symptomatic leg)
collateral superficial veins (non-varicose)
alternative diagnosis as likely or greater than that of DVT
+1
+
1
+
1
+
1
low =<0
moderate 1-2
high >=3
+
1
+
1
-2
+
1
+
1
P.S. Wells i wsp., Lancet, 1997; 350:
1795-1798
clinical probability
Diagnostic tests to confirm
DVT
Low risk
Moderate risk
High risk
DD
+
--
clinical follow-up
CUS
+
--
treat DVT
repeat CUS
treat DVT
CUS
repeat CUS
--
+
DD - D-dimer; CUS - commpression ultrasound
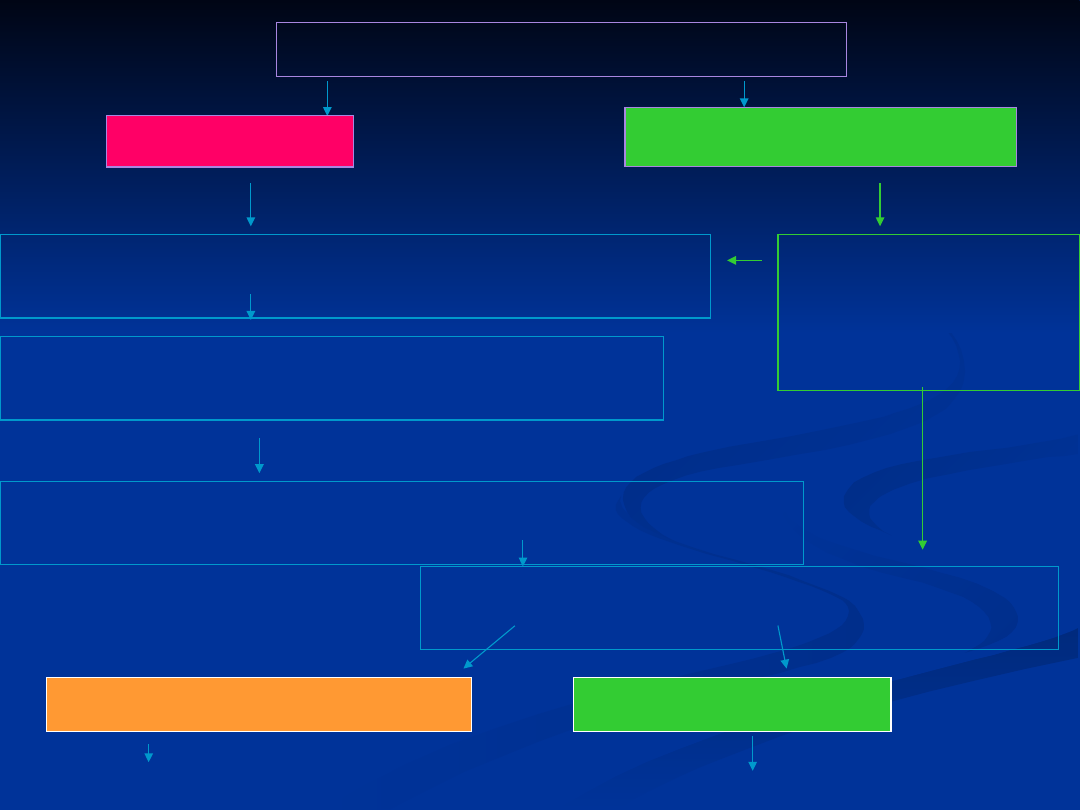
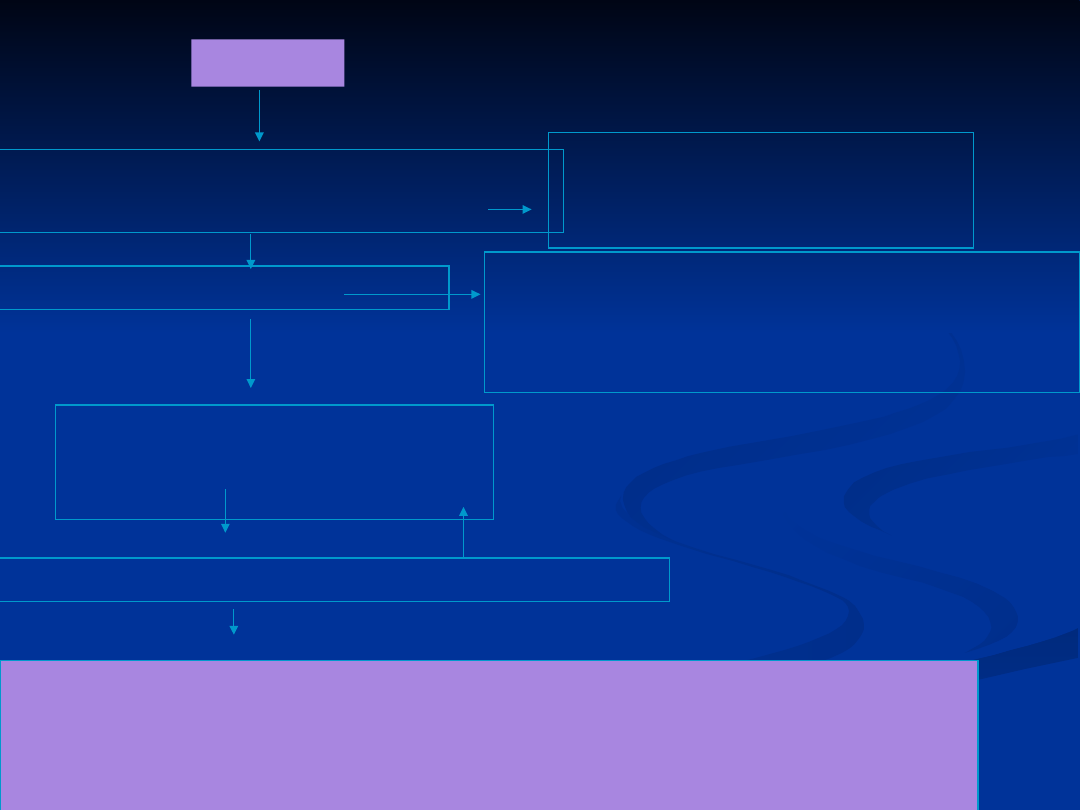
MANAGEMENT OF DVT
Morphology, blood group, APTT, INR,
creatinine
Start the treatment with LMWH, UFH, or
fondaparinux
To asses if are there any contraindications
for antithrombotic therapy
To order D-dimer and CUS detecting
DVT
Confirmed DVT
Excludet DVT
Without treatment
high
low or moderate
Is it possible to
perform D-
dimer and
CUS?
yes
no
Treatment

Confirmed DVT - treatment
Is it the threatening of
leg lossing ?
Is it extensive acute
proximal DVT?
Are there any
contraindications for
antithrombotic therapy?
Is it the cancer
coexisting ?
To start or continue the
treatment with LMWH, UFH, or
fondaparinux
Are there any contraindications for
VKAs?
Start of vitamin K antagonists (VKAs) together with LMWH, UFH, or
fondaparinux on the first treatment day, and stop heparin preparations
when the international normalized ratio (INR) is >2.0 for at least 24 h.
Are there any
contraindicatio
ns for
thrombolytic
therapy?
Think of placement of an vena caval
filter
LMWH for the first 3 to 6
months
, next
VKA or LMWH
indefinitely or until the
cancer is resolved
no
yes
no
n
o
no
yes
yes
yes
n
o
Think of venous
thrombectomy.
Think of catheter-
directed
thrombolysis
(CDT) or systemic
thrombolytic
therapy
yes

All patients should undergo rapid risk stratification PE-
related early mortality rate
PE (
pulmonary embolism) -
confirmed or
evaluated
Clinical: shock or hypotension
non high
Markers of right ventricle dysfunction/injury
or markers of myocardial injury ( cardiac
troponin)
high >15%
Intermediate 3-
15%
low <3%
absent
present
yes
no
guidelines ESC 2008

Hypotension is defined as:
Systolic blood preasure < 90 mmHg
or
Decrease of blood preasure ≥ 40mmHg lasting
more than 15 min.
guidelines ESC 2000

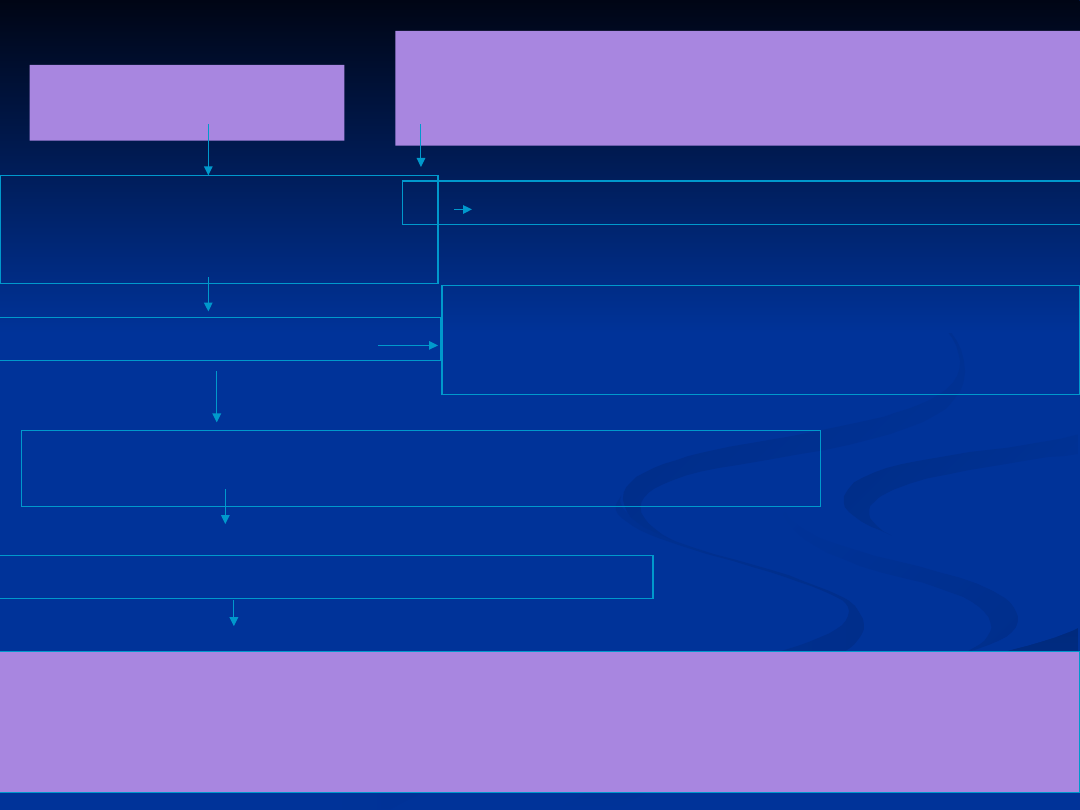
PE - High-risk
MANAGEMENT
Start the treatment of hypoxemia, shock or
hypotension
Morphology, blood group, APTT, INR,
creatinine
To asses if are there any contraindications for antithrombotic
therapy
Echocardiograp
hy
Is it possible to perform a computed tomography
CT (spiral CT or CT angiography)?
Start the treatment with UFH, LMWH or
fondaparinux
Is it right ventricle overload?
Search for other
causes
Is it CT available?
Are there any contraindications for thrombolytic
therapy?
Treatment with
thrombolytic
therapy
Pulmonary Embolectomy or mechanic
fragmentation
of the clot or usunięcie zakrzepu przez
cewnik
no
yes
yes
CT
+
-
Search
for
other
causes
no
no
yes
yes
no
no
Thrombolytic
therapy
Pulmonary Embolectomy or mechaniczna
fragmentacja lub usunięcie zakrzepu przez
cewnik
Are there any
contraindications for
antithrombotic therapy
Is it the cancer coexisting?
Start the treatment with UFH, LMWH or
fondaparinux
Are there any contraindications for VKA
Start of vitamin K antagonists (VKAs) together with LMWH, UFH, or
fondaparinux on the first treatment day, and stop of these heparin
preparations when the international normalized ratio (INR) is >2.0
for at least 24 h.
Think of placement of an vena caval filter
LMWH for the first 3 to 6 months,
next long-therm therapy with VKA or
LMWH or until the cancer is resolved
no
no
no
yes
yes
Assess clinical probability
of PE
by the Wells score for PE
PE - non high risk
high
low
moderate
Wells criteria
– Clinical probability of PE
Clinical signs and symptoms of DVT (min. of leg swelling and
pain with palpation of the deep vein)
Alternative diagnosis less likely than PE
Heart rate >100/min
Immobilisation (>3d) or surgery in the previous 4 weeks
Previous PE or DVT
Hemoptysis
Maligancy (receiving treatment,treated in the last 6 months
or palliative)
+3,0
+3,0
+1,5
+1,5
low 0-1
moderate 2-6
high
>=7
+1,5
+1,
0
+1,
0
P.S. Wells et al, Thromb. Haemost., 2000; 83: 416-420
3 levels

PE - non high risk
Assess clinical probability
of DVT
Morphology, blood group,
APTT, INR, creatinine
Are there any
contraindications for
antithrombotic therapy
high
CT
Start the treatment with
LMWH UFH, or
fondaparinux
D-dimer + morphology, blood
group, APTT, INR,
creatinine
Moderate and
low
Are there any
contraindications for
antithrombotic therapy
no
yes
yes
Start the treatment with
LMWH UFH, or
fondaparinux
no
yes
D-dimer
+
-
-
No treatment, investigate further
+
Treatment
CT +
Are there any contraindications for
antithrombotic therapy
Is it the cancer coexisting ?
Start the treatment with
LMWH,
UFH, or fondaparinux
Are there any contraindications for VKA
Start of vitamin K antagonists (VKAs) together with
LMWH, UFH, or fondaparinux on the first treatment day,
and discontinuate of these heparin preparations when the
international normalized ratio (INR) is >2.0 for at least 24
h.
Think of placement of an
vena
caval filter
LMWH for the first 3 to 6 months,
next long-therm therapy with VKA
or LMWH or until the cancer is
resolved
no
no
no
yes
yes
yes

Thank you
Document Outline
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
Wyszukiwarka
Podobne podstrony:
ŻCHZZ 2010 wykład
Matura 2010 angielski PP wypracowania
matura 2010 angielski poziom podstawowy
Matura 2010 angielski PP odp
Odmiana, Filologia angielska - UP - lic - 2010-2013, Rok I
plan - 2010.11, filologia angielska
język angielski- matura- poziom podstawowy- maj 2010 Matura j. angielski (maj 2010)- transkrypcja
4.angielski 2010 klucz pr cz1
Egzamin z Gramatyki Opisowej 2010, Anglistyka Filologia angielska UG, II rok BA Translatoryka, Grama
III deklinacja, Filologia angielska - UP - lic - 2010-2013, Rok I
zjazdy 2010-2011, filologia angielska
Panecka, Filologia angielska - UP - lic - 2010-2013, Rok II, Semestr IV
plan - 2010.12, filologia angielska
plan - 2010.10, filologia angielska
Matura z J angielski poziom p 2010 id 69090
Word list - christmas paegant, Filologia angielska - UP - lic - 2010-2013, Rok II, Semestr III
Listening odpowiedzi, Filologia angielska - UP - lic - 2010-2013, Rok I
Gramatyka angielska dla bystrzakow 2010 313p
więcej podobnych podstron