AJR:175, September 2000
637
usculoskeletal sonography is a
rapidly evolving technique that is
gaining popularity for the evalua-
tion and treatment of joint and soft-tissue dis-
eases. Inherent advantages of sonography
include accessibility, quick scan time, low
cost, multiplanar capability, and the ability to
perform dynamic real-time imaging with con-
tralateral comparison. Advances in technology
with higher frequency transducers, power
Doppler sonography, and extended field-of-
view function have facilitated the progressive
development of sonography [1–3].
One notable drawback of sonography is op-
erator-dependency; the quality and consistency
An Illustrated Tutorial of Musculoskeletal Sonography:
Part 1, Introduction and General Principles
John Lin
1
, David P. Fessell, Jon A. Jacobson, William J. Weadock, Curtis W. Hayes
Received December 8, 1999; accepted after revision February 10, 2000.
1
All authors: Department of Radiology, The University of Michigan Medical Center, 1500 E. Medical Center Dr., TC 2910, Ann Arbor, MI 48109-0326. Address correspondence to J. Lin.
AJR
2000;175:637–645 0361–803X/00/1753–637 © American Roentgen Ray Society
Pictorial Essay
M
C
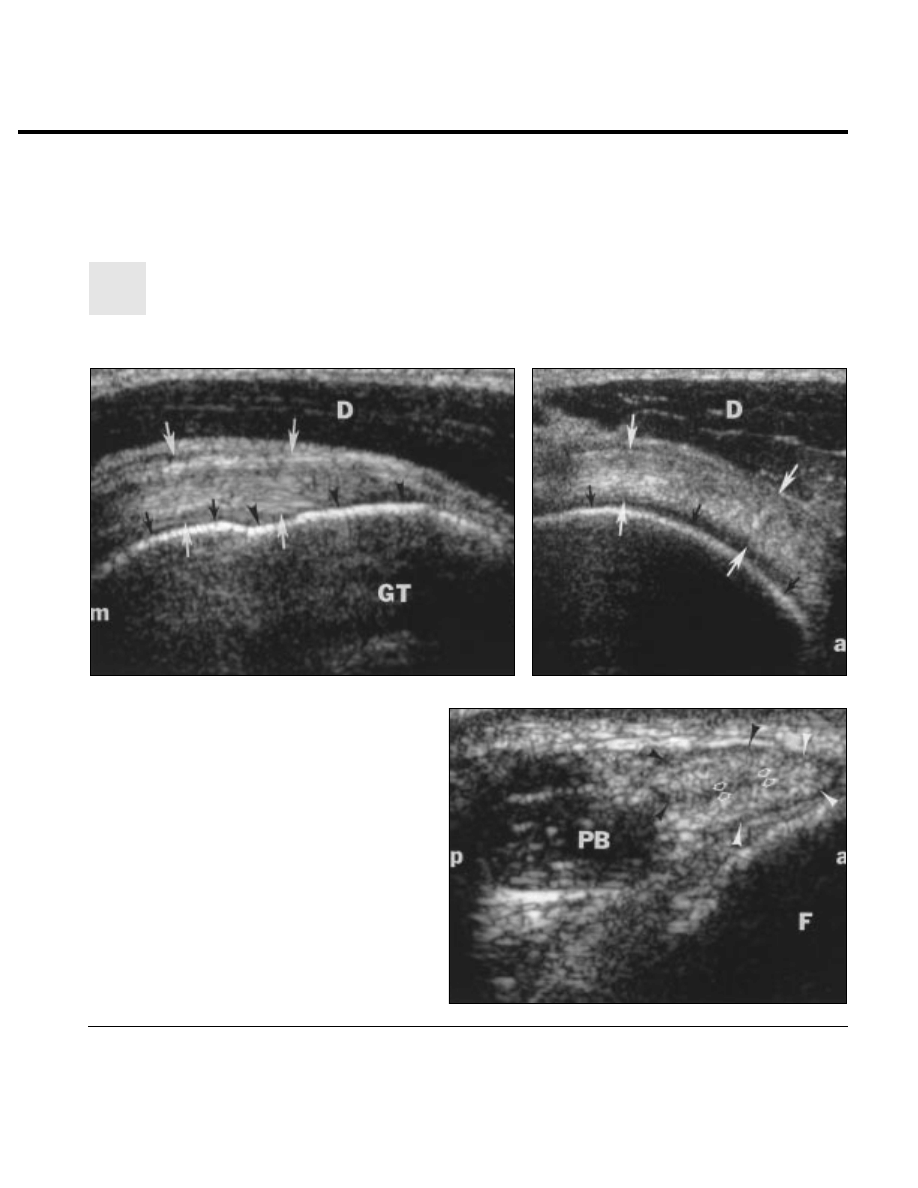
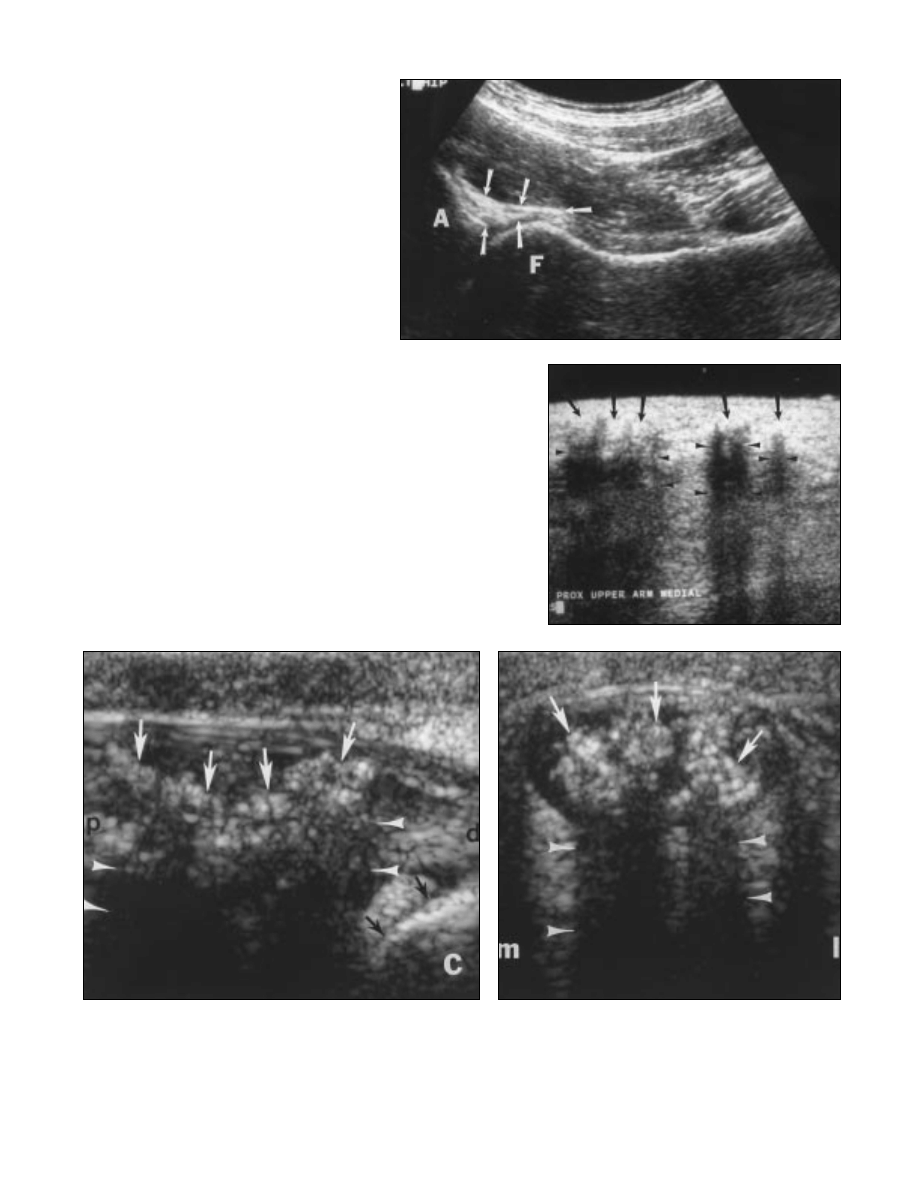
Fig. 1.—36-year-old asymptomatic man.
A and B, Longitudinal (A) and transverse (B) sonograms reveal normal su-
praspinatus tendon (
white arrows). Note hyperechoic cortex of humerus
(
black arrows), including cortex (arrowheads) of greater tuberosity (GT) in A.
Deltoid muscle (D) is overlying supraspinatus tendon. m = medial, a = anterior.
C, Transverse sonogram reveals normal peroneus brevis (white arrowheads)
and peroneus longus (
black arrowheads) tendons. Note border between per-
oneus tendons (
arrows) and peroneus brevis muscle (PB). a = anterior, p =
posterior, F = fibula.
B
A
638
AJR:175, September 2000
Lin et al.
of sonographic studies rely on the expertise of
the examiner. Other limitations include a long
learning curve and a physician time–intensive
examination, particularly for beginners. Mus-
culoskeletal sonography is a widely accepted
and available tool in Europe and other parts of
the world, in which it is often the principal
technique performed for many clinical indica-
tions. However, in the United States, sonogra-
phy is relatively underused because of the wide
availability of MR imaging and the small num-
ber of training programs offering instruction
and experience in musculoskeletal sonography.
Additionally, physicians, including radiolo-
gists, are often unaware of the potential appli-
cations of sonography for the assessment of
joint and soft-tissue disease. Sonography offers
a cost-effective alternative for imaging muscu-
loskeletal disorders in many situations [1–3].
We discuss basic principles, advanced im-
aging functions, scan artifacts, and general
characteristics of key musculoskeletal struc-
tures. Subsequent articles will feature abnor-
malities pertaining to specific joints, and the
final installment will focus on musculoskele-
tal tumors, sonographically guided interven-
tions, and miscellaneous topics. Our intent is
to review current accepted clinical applica-
tions of musculoskeletal sonography and
generate interest in what we believe to be an
underused technique. We hope to inspire
physicians to consider musculoskeletal
sonography as a viable, and frequently pri-
mary, option in the assessment of joint and
soft-tissue disorders.
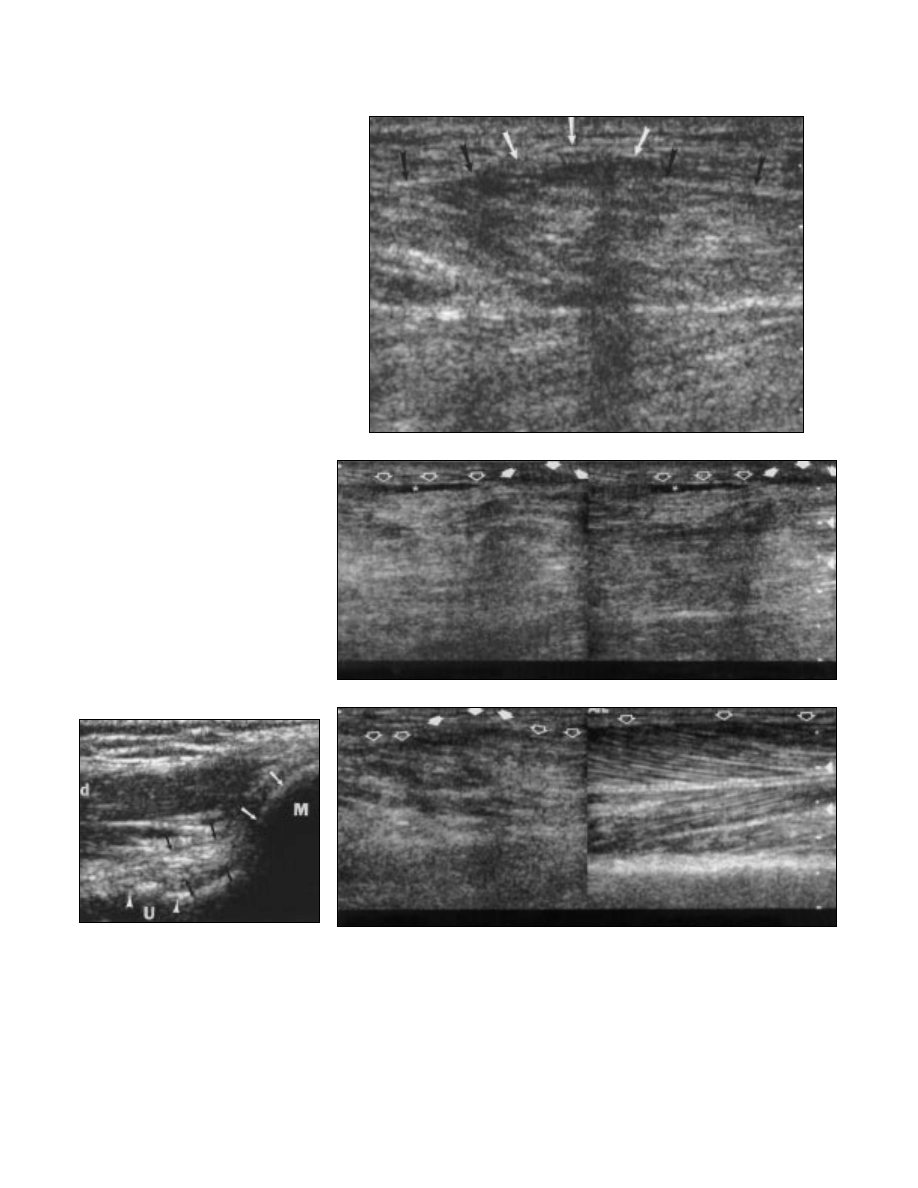
Fig. 2.—30-year-old woman without symptoms. Longi-
tudinal sonogram reveals normal ulnar collateral liga-
ment (
black arrows) of elbow. Note medial epicondyle
(M and
white arrows) and proximal ulna (U and arrow-
heads). d = distal.
A
B
C
Fig. 3.—60-year-old man with muscle herniation caused by remote trauma.
A, Longitudinal sonogram of anterolateral lower extremity, in region of focal bulge, reveals herniation of anterior
tibial muscle (
white arrows) through defect in fascia (black arrows).
B, Longitudinal split-screen sonogram obtained in same location as A shows minimal motion of anterior tibial
muscle with dynamic imaging between dorsiflexion (left-sided image) and plantar flexion (right-sided image).
Note muscle herniation (
solid arrows), fascia (open arrows), and small subfascial fluid collection (asterisk).
C, Longitudinal split-screen sonogram shows comparison of muscle echotexture between scarred, herniated
symptomatic leg (left-sided image) and normal contralateral asymptomatic leg (right-sided image). Note fascia
(
open arrows) and muscle herniation (solid arrows).
Principles of Musculoskeletal Sonography
AJR:175, September 2000
639
General Principles
When performing musculoskeletal sonog-
raphy, the proper equipment is essential to
facilitate optimal image quality and diagnos-
tic examinations. In general, the structures
examined will be superficial; therefore, high-
frequency (
≥
7–12 MHz) linear array trans-
ducers are usually the most appropriate
choice. The high resolution attainable allows
detailed anatomic depiction of pertinent
structures [1]. Proper positioning of the pa-
tient is of paramount importance in obtaining
high-quality studies. Different sonographic
techniques have been described, with the
universal goal of optimizing the visualization
of structures of interest.
Musculoskeletal Structure Characteristics
In this section, we describe the sono-
graphic characteristics of key musculoskele-
tal structures.
The evaluation of tendon abnormality is
the most common clinical indication for
musculoskeletal sonography. Whether the
tendon is in the shoulder, wrist, or ankle, the
sonographic appearance of a normal tendon
is fairly uniform. On sonography, tendons
should have a fibrillar pattern of parallel hy-
perechoic lines in the longitudinal plane and
a hyperechoic round-to-ovoid shape in the
transverse plane [4] (Fig. 1).
Ligaments have an appearance similar to
tendons but are static stabilizers connecting
bone to bone. Ligaments can be differentiated
from tendons by noting their more compact
fibrillar, hyperechoic pattern [1]. Superficial
ligaments, such as the anterior talofibular liga-
ment or elbow ulnar collateral ligament (Fig.
2), are readily visualized. Deeper internal liga-
ments, such as the anterior cruciate ligament,
are more difficult to consistently identify.
Normal skeletal muscle shows low- to
mid-level echogenicity with hyperechoic fas-
cial planes [1] (Fig. 1). Partial and complete
tears can be characterized on sonography,
and the degree of retraction, if any, can be
accurately measured. Dynamic imaging with
contraction of the affected muscle can some-
times better illustrate the abnormality and
provide functional information (Fig. 3).
Larger peripheral nerves can also be accu-
rately identified on sonography [5]. Normal
peripheral nerves typically appear as
echogenic fascicular structures and tend to
be slightly less echogenic than tendons or
ligaments [6] (Fig. 4). This appearance is
somewhat variable depending on the location
and orientation of the nerve but can usually
be identified by the nerve distribution.
On sonography, the bone cortex appears
as an echogenic surface with posterior shad-
owing (Fig. 1). Only the superficial surface
of the bone can be consistently evaluated on
sonography. Radiographically occult frac-
tures can be detected on sonography, seen as
a “step off” cortical disruption [1, 7] (Fig. 5).
A thin hypoechoic rim paralleling the
echogenic articular cortical surface repre-
sents hyaline cartilage (Figs. 1 and 6). Ongo-
ing research on the potential clinical
applications of sonography of fibrocartilage
is promising. Sonography may play a more
significant role in the assessment of labral
and meniscal lesions as technology contin-
ues to improve [1] (Figs. 7 and 8).
A
B
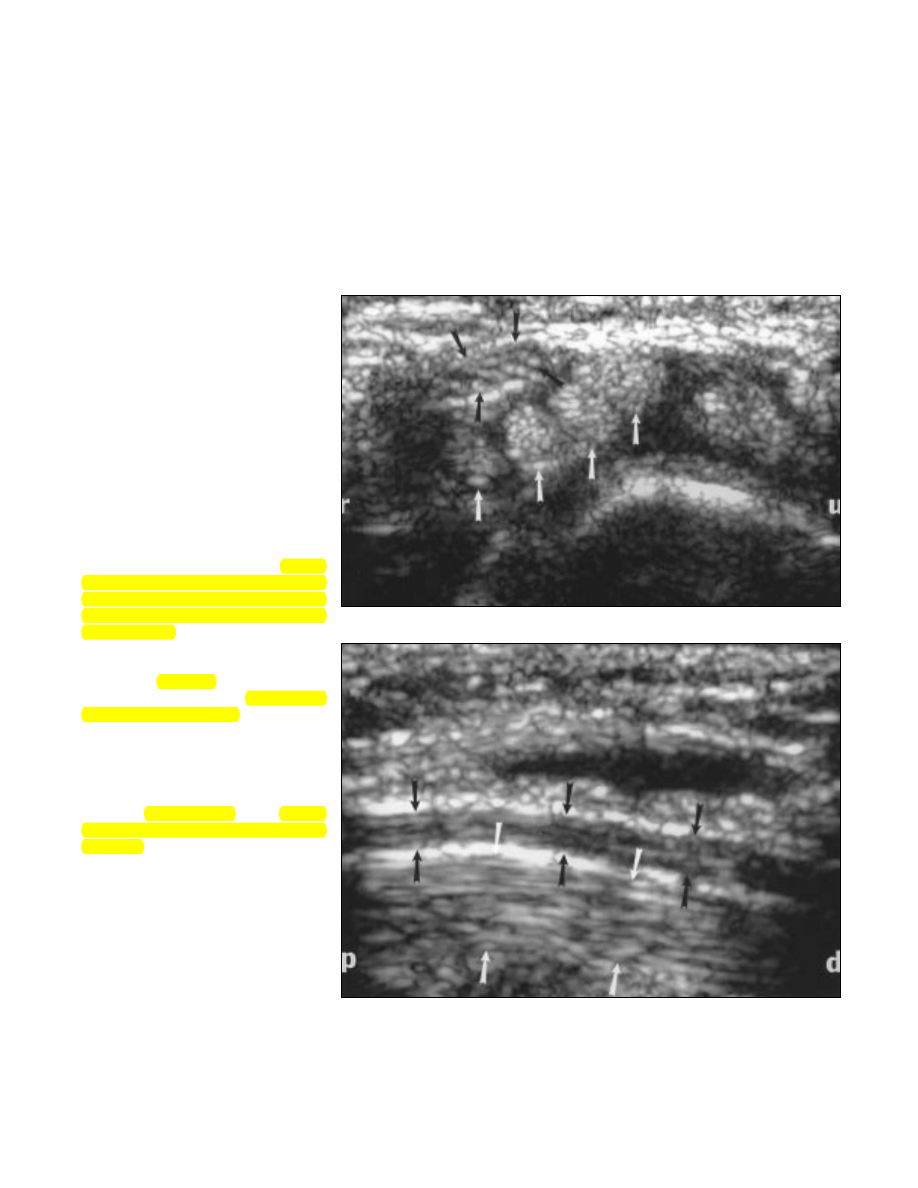
Fig. 4.—32-year-old asymptomatic man.
A and B, Transverse (A) and longitudinal (B) sonograms of carpal tunnel of wrist show normal appearance of me-
dian nerve (
black arrows) and flexor tendons (white arrows). r = radial, u = ulnar, p = proximal, d = distal.
640
AJR:175, September 2000
Lin et al.
Calcifications typically exhibit increased
echogenicity with associated posterior acous-
tic shadowing (Fig. 9). However, the presence
of shadowing depends on the size of the cal-
cification [8]. When calcification is present
within the substance of a tendon, it com-
monly represents calcific tendonitis (Fig. 10).
Examination
Although sonography is operator-depen-
dent, the interaction between the examiner
and the patient is invaluable. Additional clin-
ical history about the precise location and
character of symptoms, direct feedback
about tenderness with probe palpation, and
positions or movements that elicit or aggra-
vate symptoms can assist in the accurate in-
terpretation of findings.
The flexibility and dynamic capability of
sonography allow a targeted examination, spe-
cific for each individual. Dynamic imaging
can readily reveal certain transient conditions
related to specific positions or movements,
which can be absent during static examination
[2] (Fig. 11).
Compression from applying transducer
pressure under real-time visualization can re-
veal important information about the compo-
sition of underlying structures and allows
increased conspicuity or detection of abnor-
malities that may be otherwise hidden [2]
(Fig. 12).
Contralateral comparison is easily per-
formed in the musculoskeletal system; it dis-
tinguishes significant findings from normal
variants and occasionally reveals unsus-
pected abnormalities, which can be crucial to
the treatment of a patient (Figs. 13 and 14).
Technical Features
Color and power Doppler sonography fea-
tures show the degree of vascularity associ-
ated with inflammatory processes and solid
masses. Power Doppler sonography can be
used to characterize musculoskeletal inflam-
mation in cellulitis, abscess, synovitis, myo-
sitis, and bursitis [9] (Fig. 15).
The split-screen function that is available
on most sonography units can expand the
field of view to approximately double the
width or can be used for side-by-side com-
parisons (Figs. 13 and 14). The extended
field-of-view function, available on the
Sonoline Allegra sonographic unit (Siemens
Medical Systems, Iselin, NJ), can display
very large continuous sections of anatomy,
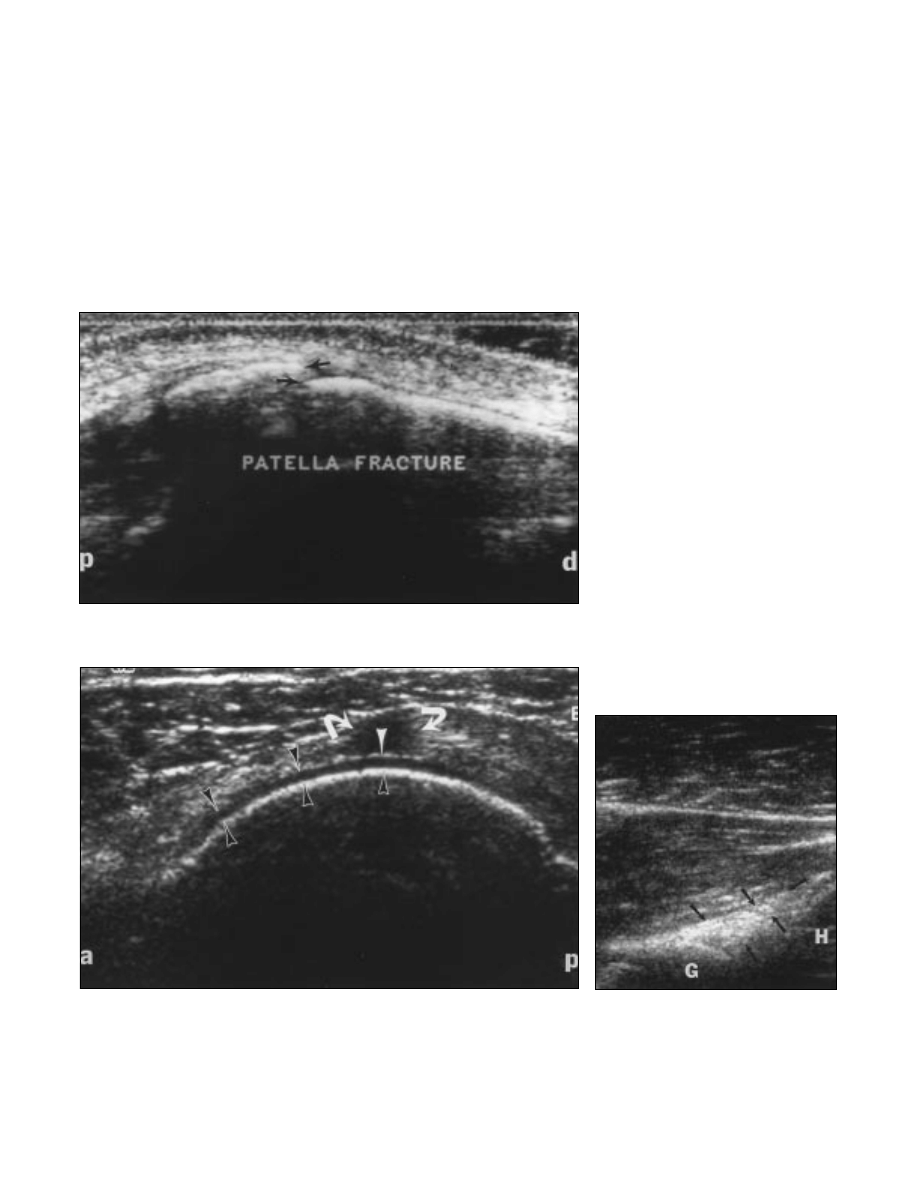
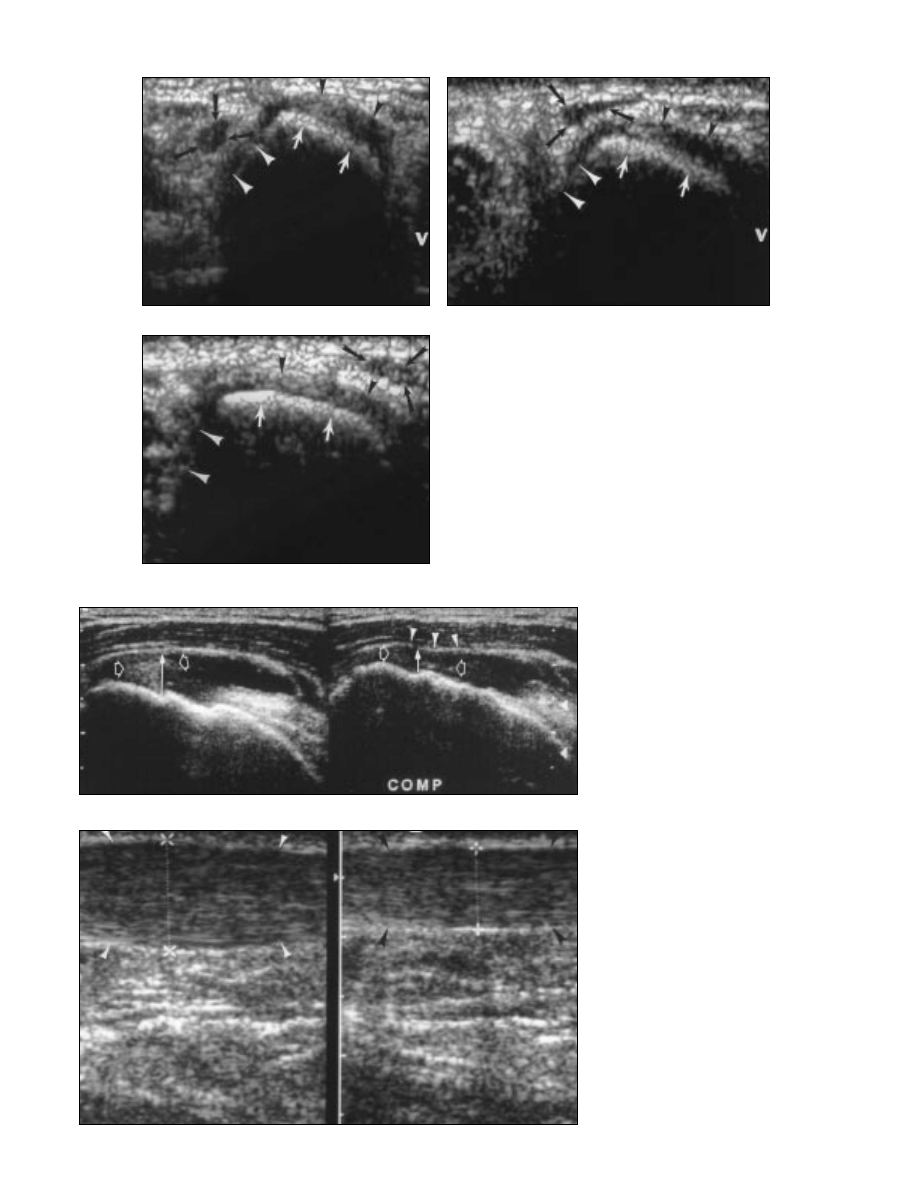
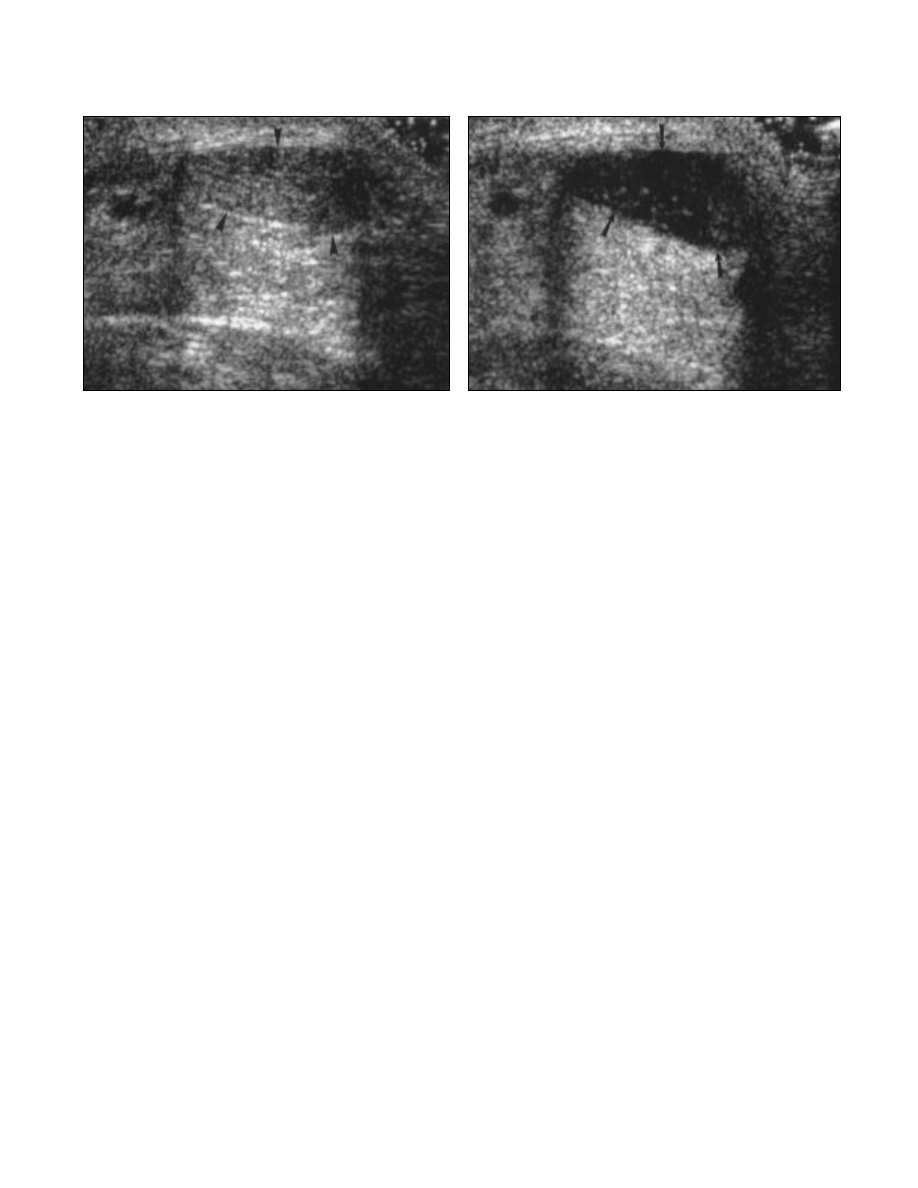
Fig. 6.—80-year-old woman with rotator cuff tear. Transverse sonogram reveals small full-thickness tear (curved ar-
rows) in distal supraspinatus tendon. Note hypoechoic hyaline articular cartilage (black arrowheads) of humeral
head. Fluid present within defect of supraspinatus tear accentuates echogenicity at surface of hyaline cartilage
(
white arrowhead). a = anterior, p = posterior.
Fig. 5.—36-year-old woman with patellar fracture. Longitudinal sonogram shows mildly displaced fracture of patella
(
arrows) that was not revealed on radiographs of knee. p = proximal, d = distal.
Fig. 7.—37-year-old man with shoulder pain. Trans-
verse sonogram of posterior glenohumeral joint shows
normal posterior glenoid labrum (
arrows). Note gle-
noid (G) and humeral head (H). Pain was caused by
torn rotator cuff tendon (not shown).
Principles of Musculoskeletal Sonography
AJR:175, September 2000
641
preserving spatial resolution without distort-
ing structural relationships [10, 11] (Fig. 16).
Recent innovative functions such as three-
dimensional imaging (Fig. 17) and tissue
harmonics (Fig. 18) may provide further im-
provement in the diagnostic effectiveness of
sonography. The role of these functions in
the assessment of musculoskeletal disorders
is currently under investigation [3].
Artifact
Anisotropy is an important artifact that can
affect the image and should be considered
when examining any musculoskeletal soft-tis-
sue structure. This finding is most obvious with
tendons and ligaments, caused by the highly
Fig. 8.—18-year-old woman with contralateral hip pain. Longitudi-
nal sonogram of asymptomatic left hip shows normal anterior ace-
tabular labrum (
arrows). Note acetabulum (A) and femoral head (F).
Fig. 9.—27-year-old woman with dermato-
myositis. Transverse sonogram of medial
upper arm in region of several small non-
tender palpable nodules shows several
subcutaneous echogenic foci (
arrows)
with distal shadowing (
arrowheads) that
represent superficial calcifications.
B
A
Fig. 10.—21-year-old man with calcific tendonitis of Achilles tendon.
A and B, Longitudinal (A) and transverse (B) sonograms of Achilles tendon at distal insertion reveal extensive calcifications (white arrows) within tendon, consistent with calcific ten-
donitis. Note distal shadowing (
arrowheads), and note superoposterior aspect of calcaneus (C and black arrows) in A. p = proximal, d = distal, m = medial, l = lateral.
642
AJR:175, September 2000
Lin et al.
B
A
Fig. 11.—50-year-old man with intermittent ulnar nerve subluxation.
A–C, Transverse dynamic sonograms of cubital tunnel region reveal tran-
sient dislocation of ulnar nerve (
black arrows) out of cubital tunnel (white
arrowheads) with progressive flexion. Note medial epicondyle (white ar-
rows) and origin of common flexor tendons (black arrowheads), which
appear hypoechoic because of anisotropy artifact (see Figs. 17 and 18).
v = volar.
C
Fig. 12.—64-year-old man with rotator cuff tear. Split-
screen image shows complete full-thickness tear of
distal supraspinatus tendon. Manual compression
(COMP) of transducer (right-sided image) reveals vol-
ume loss (
solid arrows) and bursal contour deformity
(
arrowheads) confirming diagnosis of full-thickness
tear. Note echogenic debris (
open arrows) present in
tear defect. Secondary sonographic findings of full-
thickness rotator cuff tear will be discussed in part 2,
“Upper Extremity.”
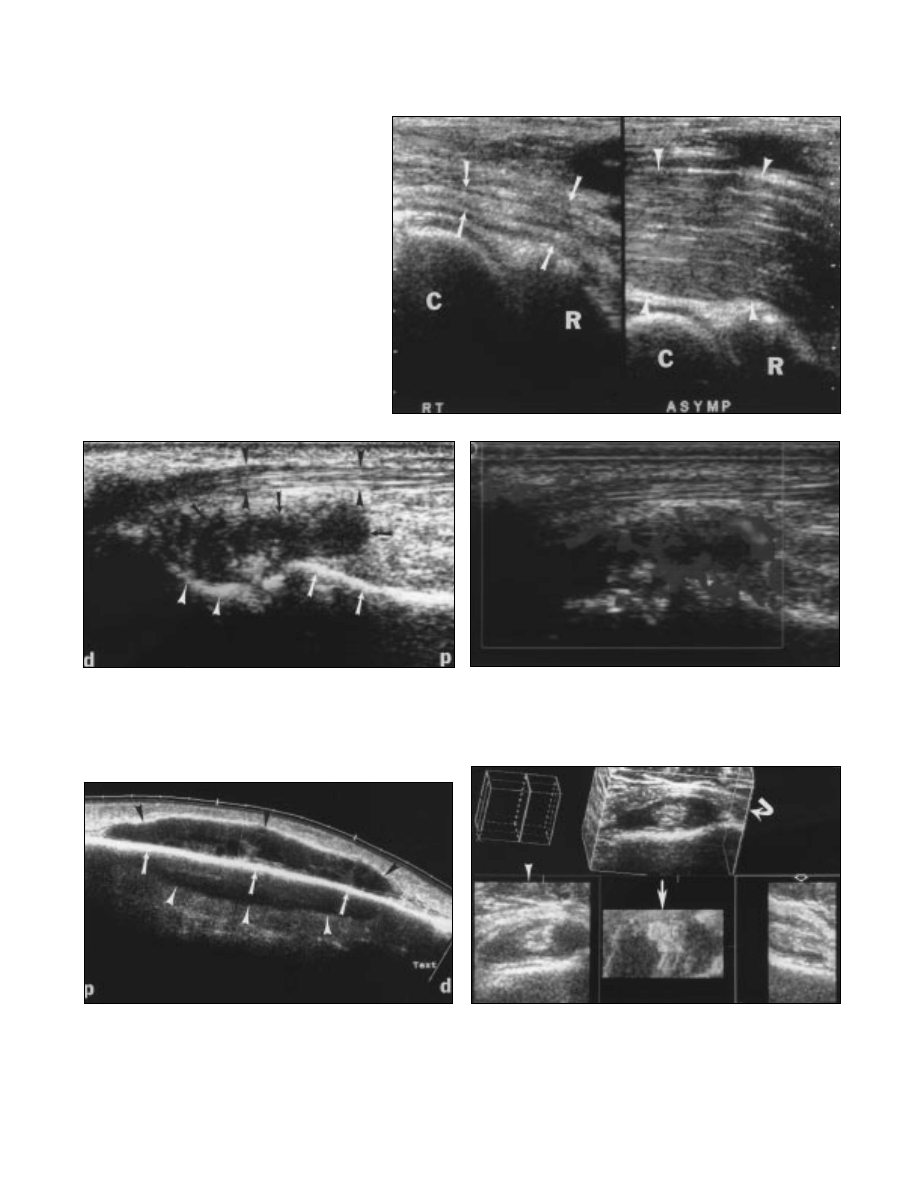
Fig. 13.—48-year-old woman with left Achilles tendi-
nosis. Longitudinal split-screen image compares ab-
normal focally thickened left Achilles tendon (
white
arrowheads, left-sided image), consistent with tendi-
nosis, with asymptomatic normal-caliber right Achil-
les tendon (
black arrowheads, right-sided image).
Principles of Musculoskeletal Sonography
AJR:175, September 2000
643
Fig. 14.—36-year-old man with right brachial muscle atrophy.
Split-screen image compares severely atrophied right brachial
muscle (
arrows) at anterior aspect of elbow with normal appear-
ance of left brachial muscle (
arrowheads). Note capitellum (C)
and radial head (R). Contralateral comparison provides internal
control, particularly for difficult or unsuspected findings.
B
Fig. 15.—56-year-old woman with rheumatoid arthritis.
A, Longitudinal sonogram of radial aspect of left wrist shows hypoechoic periarticular lesions consistent with synovial hyperplasia and pannus (black arrows). Note ab-
ductor pollicis longus tendon (
black arrowheads), distal radius (white arrows), and scaphoid (white arrowheads). d = distal, p = proximal.
B, Longitudinal power Doppler sonogram obtained in same location as A shows markedly increased flow consistent with inflammation.
A
Fig. 16.—68-year-old woman with large hematoma caused by falling. Longitudinal
extended field-of-view sonogram of anterior aspect of right leg reveals large pretibial
hematoma (
black arrowheads), which measured 10 cm in length. Extended field-of-
view function allows full coverage of this lesion. Note tibial cortex (
arrows). Mirror-
image artifact (
white arrowheads) is present. p = proximal, d = distal.
Fig. 17.—66-year-old woman with left shoulder pain. Three-dimensional image of intact
long head of biceps tendon with joint effusion extending into bicipital tendon sheath shows
three standard orthogonal planes: axial (
solid arrowhead), coronal (straight arrow), and
sagittal (
open arrowhead). Oblique plane (curved arrow) was chosen by sonographer. Clin-
ical use of this function for musculoskeletal sonography is under investigation.
644
AJR:175, September 2000
Lin et al.
ordered, parallel pattern of collagen fibers that
shows the greatest degree of reflectivity when
examined perpendicular to the ultrasound
beam. Anisotropy occurs when the ultrasound
beam is not perpendicular to the fibrillar struc-
ture of the tendon, resulting in the absence of
specular reflectors and an artifactual hypo-
echoic to anechoic appearance [4] (Figs. 19 and
20). The sonographer should be aware of
proper transducer position and may need to
manipulate the heel–toe and fore–aft angula-
tion of the probe to avoid this artifact [12].
When a tendon has a curving course, the effects
of anisotropy cannot be entirely eliminated.
Each separate portion of the tendon must be ex-
amined individually, and the evaluation of ten-
don integrity should be primarily determined
during real-time scanning.
B
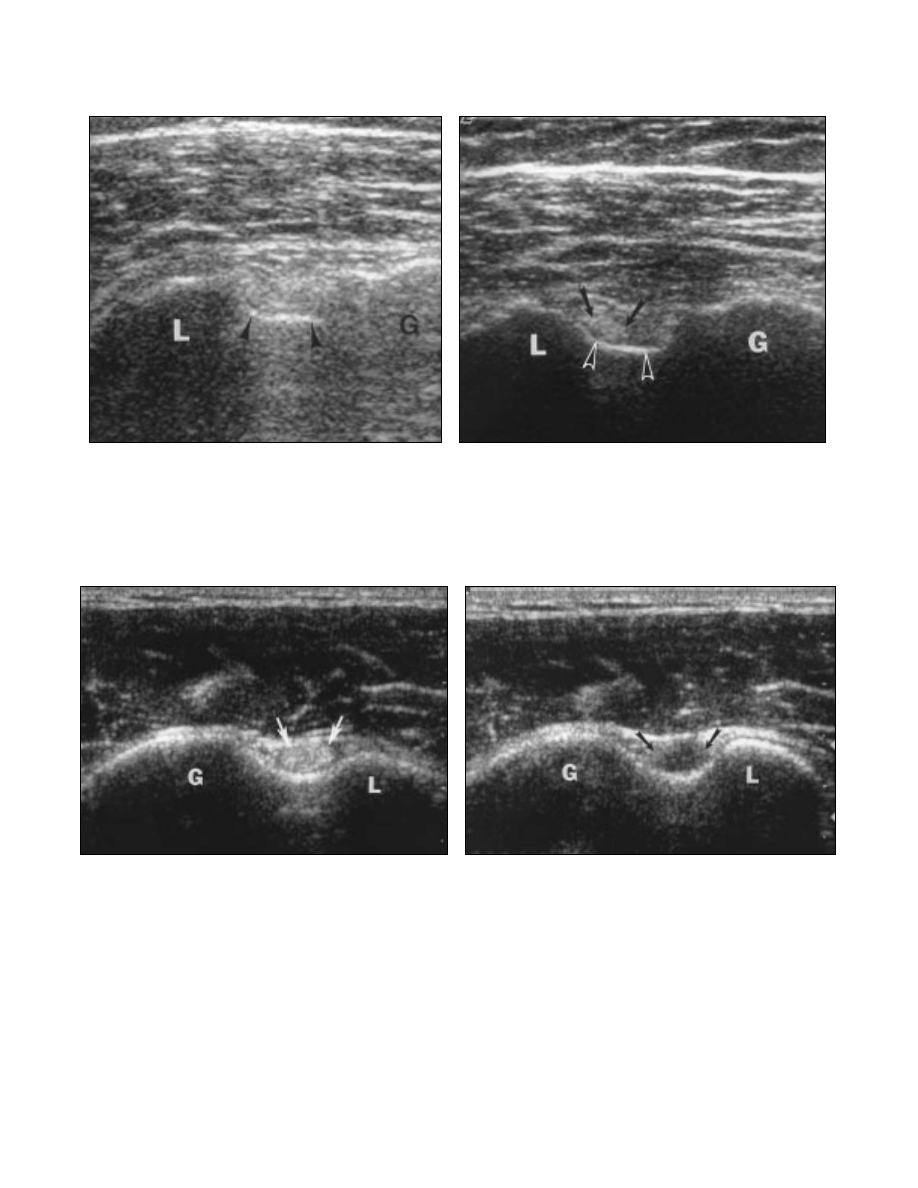
Fig. 18.—62-year-old man with left shoulder pain. L = lesser tuberosity, G = greater tuberosity.
A, Standard transverse sonogram of long head of biceps tendon is poorly visualized because of deep location of biceps tendon caused by large body habitus of patient.
Note bicipital groove (
arrowheads).
B, Transverse sonogram with tissue harmonics function reveals intact long head of biceps tendon (arrows) discretely in bicipital groove (arrowheads).
A
B
Fig. 19.—36-year-old asymptomatic man. L = lesser tuberosity, G = greater tuberosity.
A, Transverse sonogram shows normal long head of biceps tendon (arrows).
B, Transverse sonogram obtained at same location as A shows effect of anisotropy with artifactual hypoechogenicity in expected location of tendon (arrows).
A
Principles of Musculoskeletal Sonography
AJR:175, September 2000
645
References
1. Jacobson JA, van Holsbeeck MT. Musculoskele-
tal ultrasonography.
Orthop Clin North Am
1998
;
29:135–167
2. Jacobson JA. Musculoskeletal sonography and
MR imaging: a role for both imaging methods.
Radiol Clin North Am
1999
;37:713–735
3. Adler RS. Future and new developments in mus-
culoskeletal ultrasound.
Radiol Clin North Am
1999
;37:623–631
4. Martinoli C, Derchi LE, Pastorino C, Bertolotto
M, Silvestri E. Analysis of echotexture of tendons
with US.
Radiology
1993
;186:839–843
5. Fornage BD. Peripheral nerves of the extremities:
imaging with US.
Radiology
1988
;167:179–182
6. Silvestri E, Martinoli C, Derchi LE, Bertolotto M,
Chiarmondia M, Rosenberg I. Echotexture of pe-
ripheral nerves: correlation between US and his-
tologic findings and criteria to differentiate
tendons.
Radiology
1995
;197:291–296
7. Griffith JF, Rainer TH, Ching AS, Law KL,
Cocks RA, Metreweli C. Sonography compared
with radiography in revealing acute rib fracture.
AJR
1999;173:1603–1609
8. Farin PU, Jaroma K. Sonographic findings of ro-
tator cuff calcifications. J Ultrasound Med 1995;
14:7–14
9. Newman JS, Adler RS, Bude RO, Rubin JM. De-
tection of soft-tissue hyperemia: value of power
Doppler sonography. AJR 1994;163:385–389
10. Barberie JE, Wong ADW, Cooperberg PL, Carson
BW. Extended field-of-view sonography in mus-
culoskeletal disorders. AJR 1998;171:751–757
11. Lin EC, Middleton WD, Teefey SA. Extended
field of view sonography in musculoskeletal im-
aging. J Ultrasound Med 1999;18:147–152
12. Fornage BD. The hypoechoic normal tendon:
a pitfall. J Ultrasound Med 1987;6:19–22
B
Fig. 20.—49-year-old asymptomatic man.
A, Transverse sonogram of normal Achilles tendon (arrowheads) is echogenic except for slightly hypoechoic area relative to pre-Achilles fat.
B, Transverse sonogram obtained at same location as A shows effect of anisotropy with artifactual hypoechogenicity in expected location of tendon (arrows).
A
Wyszukiwarka
Podobne podstrony:
Musculoskeletal Sonography,Part 2, Upper Extremity, leido
Introduction to Differential Geometry and General Relativity
Local and general anaesthetics Nieznany
SHSBC419 ARCBreaks and Generailities
ielts speaking part 1 topics and tenses
Marxism, the Resource Mobilization Theory, and General?ono
kurs rysowanie basic painting and drawing principles 56R3OH6IXOXH3MLLJUG4HH6IFQRMWM3PU6JGLFI
ideas general principles rules politics
Introduction To General Relativity G T Hooft
Local and general anaesthetics Nieznany
William Pelfrey Billy, Alfred, and General Motors, The Story of Two Unique Men, a Legendary Company
Introduction to the Principia Discordia
Einstein A Relativity the special and general theory (free web version, Methuen, 1920) (115s)
Einstein, Special and General Relativity
saint saens bizet introducion and rondo capriccioso [vl pf]
więcej podobnych podstron