
Osteonecrosis
Karel Pavelka
MD, PhD
Associate Professor of Internal Medicine and Rheumatology; Director, Institute of Rheumatology;
Senior Lecturer, Charles University, Prague
Institute of Rheumatology, Na Slupi 4, 128 50 Prague 2, Czech Republic
Osteonecrosis (avascular necrosis, aseptic necrosis or subchondral avascular necrosis) is not a
speci®c disease entity but the ®nal common pathway of a number of conditions leading to bone
death. The main predisposing factors (trauma, glucocorticosteroids, alcoholism and connective
tissue disorders) should be carefully sought, but osteonecrosis can also be idiopathic in origin. Its
most common localization is to the femoral head, followed by the humeral head, the knee and
the small bones of the wrist and foot. New imaging techniques, especially magnetic resonance
imaging, have improved the early diagnosis of osteonecrosis as radiographs may be normal in
the initial stages. The outcome for the patient is in¯uenced by many factors, the size and
localization of the bone necrosis being of primary importance. Early intervention (both surgical
and non-surgical) has de®nitively improved the outcome, but still nearly 50% of cases of femoral
head osteonecrosis necessitate arthroplasty. In this chapter, we shall concentrate on patients at
high risk of osteonecrosis, on evidence-based diagnosis, especially in the early stages, and on
evidence-based treatment suited to the staging system of osteonecrosis.
Key words: osteonecrosis; avascular necrosis; osteochondritis dissecans; magnetic resonance
imaging.
Osteonecrosis (ON; avascular necrosis, aseptic necrosis or subchondral avascular
necrosis) is not a speci®c disease entity but the ®nal common pathway of a number of
conditions (
) mostly leading to an impairment of the blood supply to the bone.
The aetiological factors are well known in some conditions (trauma, caisson disease and
sickle-cell disease) but less clear in others (systemic lupus erythematosus [SLE],
corticosteroid administration, pancreatitis and excessive alcohol intake); idiopathic
forms are also frequent. In addition ON can develop during pregnancy. This probably
has a multifactorial aetiology and may involve mechanical, hormonal and coagulation
factors.
Idiopathic ON of the hip in twins has been reported
, as has familial idiopathic
ON, probably caused by hypo®brinolysis.
EPIDEMIOLOGY
There are few data on the incidence or prevalence of ON. The number of new cases
detected annually in the USA is estimated to be 15 000.
In one Japanese study of non-
traumatic ON, 34.7% of the cases were caused by corticosteroid treatment and 21.8%
by alcohol abuse, 37.1% being considered idiopathic; other conditions mentioned were
less frequent.
A systematic review of the published literature estimated the incidence
1521±6942/00/020399+16 $35.00/00
*
c 2000 Harcourt Publishers Ltd
BaillieÁre's Clinical Rheumatology
Vol. 14, No. 2, pp. 399±414, 2000
doi:10.1053/berh.2000.0072, available online at http://www.idealibrary.com on
12
of ON of the hip in long-term steroid treatment after transplantation to be 8%.
In SLE
in long-term observation (so-called late lupus), ON has been shown to develop in
The incidence of ON in trauma with fracture of the femoral neck, especially in
the subcapital region, is estimated to be 30% in displaced fractures. In haemophilia, the
prevalence of reported ON is 2.8%.
The most commonly aected sites are the femoral
head
, the humeral head
, the knees (femoral condyles and proximal tibia
), the small
bones of the foot
, the small bones of the hand (including the scaphoid and lunate
) and the vertebrae.
Many of these, especially from the group of idiopathic
ON occurring in childhood or adolescence, have historical names.
PATHOGENESIS
ON is the result of an interruption of the circulation, which leads to a disparity
between the oxygen need of the bone cell and the ability of the local circulation to
supply that need. This may be caused by vascular compression (external pressure),
trauma or occlusion of the vessels by nitrogen bubbles (in caisson disease) or rigid
sickle cells (in sickle-cell anaemia). The mechanism of ischaemia and necrosis in other
non-traumatic ON is not clear. Several possible mechanisms have been proposed to
explain ON
:
1. microfractures and osteoporosis;
2. primitive vascular problems (including vessel infarction, stenosing arteritis, arterio-
sclerotic disease, extraosseous arterial involvement or extraosseous venous
abnormality);
3. fat embolism;
4. venous intra-osseous factors;
5. the hypertrophy of fat cells;
6. compartment syndrome (compression of the bone microvasculature).
Table 1. Conditions associated with avascular necrosis of the femoral head.
Fracture of the femoral neck
Traumatic dislocation of the hip
Slipped capital femoral epiphysis
Reconstructive hip surgery, involving femoral head dislocation
Perthes disease
Caisson and diver's disease
Gaucher's disease
Sickle-cell disease and sickle-cell variants
Miscellaneous haemoglobinopathies and coagulopathies
Radiotherapy
High-dose corticosteroid treatment and Cushing's disease
Disturbances of lipid metabolism
Excessive alcohol intake
Pancreatitis and Weber±Christian disease
Gout
Arteriosclerosis and other occlusive vascular disorders
Osteomalacia and other metabolic bone diseases
Systemic lupus erythematosus and other connective tissue disorders
Pregnancy
HIV infection
Idiopathic
400 K. Pavelka

CLINICAL MANIFESTATIONS
The clinical features of ON are non-speci®c, being in¯uenced by localization, size,
associated conditions and the evolutive phase of the process. There appear to be
several dierent variants of this condition. The severity ranges from asymptomatic to
severely disabling. The outcome can also range from healing to destruction of the joint
and a necessity for arthroplasty.
Pain is the most common presentation of ON. In ON of the femoral head, the pain
is most frequently located to the groin or anterior thigh, but it can also involve the
buttock or the knee. Many cases of ON are, however, asymptomatic.
In other
instances, the patient develops pain that persists for weeks before radiographs show
any changes. This is called the pre-radiological state, and the radiographic evidence of
ON may remain undetected until 6±10 weeks after the onset of the pain. The pain
usually occurs on weight-bearing, as in osteoarthritis, but is also very often present at
rest. Later on in the disease, patients may develop limping and a decrease of function.
The physical ®ndings are non-speci®c. They may be absent, or pain may be present
only in extreme rotation. The range of motion is usually limited after collapse of the
femoral head, when shortening of the limb can also develop.
The clinical picture of ON of the humeral head is also non-speci®c. There is usually
pain, often at rest, limitation of motion being a very late event as lack of movement at
the glenohumeral joint can be compensated for by motion at the scapulothoracic joint.
The onset of pain in ON of the knee is usually sudden and is often associated with
increased physical activity. Examination reveals tenderness over the involved area,
synovitis and joint eusion may be present, so that it really mimics osteoarthritis of the
knee. There seem to be at least two distinct forms of this condition.
The ®rst one is
often related to corticosteroid treatment, sometimes being associated with ON of the
hip. This aects younger patients, is often bilateral and often aects both the tibial
plateaux and the femoral condyles. The second form of the condition aects an older
age group and is most often limited to a femoral condyle, most frequently on the
medial side, favoured by genu varum.
Avascular ON of the carpal bones follows corticosteroid therapy or trauma, may
remain asymptomatic but usually presents with wrist pain, limitation of motion and
tenderness in the anatomical snubox.
ON of the tarsal navicular is characterized by pain, an antalgic gait and localized
tenderness and swelling over the navicular bone.
EVIDENCE-BASED DIAGNOSIS OF ON
The diagnosis of ON relies heavily on imaging methods, which include plain
radiography, conventional tomography, computed tomography (CT), scintigraphy and
magnetic resonance imaging (MRI). Invasive methods include bone marrow pressure
determinations and bone marrow biopsy. Although the appearance of ON on
conventional radiographs is well documented, these changes are often delayed.
Radionuclide bone scans oer a unique possibility for the non-invasive detection of the
early stages of osteoarthritis. The method of ®rst choice today is MRI.
Radiographic changes
In the earliest stages of ON, plain radiographs are normal and pathological changes
must be detected by other techniques, for example MRI.
Osteonecrosis 401
Early radiographic changes in the femoral head include mottled radiodense areas
scattered in the anterosuperior region and a faint band of diminished density in the
anterosuperior subchondral bone (the crescent sign) (
), loss of sphericity, a
grossly triangular zone of sclerosis in the weight-bearing area, and initially subtle
¯attening of the femoral contour, best seen on pro®le views. Later on, there is
¯attening and often gross collapse of the femoral head (
). The joint space and
acetabulum are still normal. Later still, secondary osteoarthritis can develop, with joint
space narrowing and sclerotic and cystic changes in the acetabulum. A total
destruction of the femoral head can sometimes be observed (
Figure 1. Central area of radiolucency (the crescent sign), indicating a subchondral fracture.
Figure 2. Later changes include ¯attening and gross collapse of the femoral head.
402 K. Pavelka

Computed tomography
CT images display early sclerosis in the central part of the femoral head (the
asterisk sign) and joint eusion. Some minimal anterior collapses can be detected by
CT scanning.
Scintigraphy
Bone scanning using methylene bisphosphonate labelled with technetium-99m has
been used in the investigation of ON. The technique is very useful in the early stages,
when radiographic pictures are normal, and to map the extent of the disease in
patients with multiple sites of ON. It has been documented that pre-treatment bone
scanning in slipped capital femoral epiphysis is a sensitive predictor of the development
of ON.
Bone scanning usually shows increased uptake either because of new bone
formation or as a result of metabolic activity around the necrotic area. Bone-scanning
might show cold areas at very early stages, when the necrotic bone is not taking up
isotope and new bone formation has not started yet. The technique is, however,
relatively insensitive in the early pre-collapse stages, when it gives a positive result in
only 70% of cases.
Bone scanning is also totally non-speci®c.
Magnetic resonance imaging
This technique has brought new quality into the diagnosis of ON, for several reasons.
MRI has been shown clearly to be more sensitive than plain radiography, CT or bone
scanning, especially in the early stages. MRI has been shown to have 97% sensitivity in
dierentiating osteonecrosis from a normal hip, and 85% sensitivity in dierentiating
ON of the femoral head from other hip disorders, giving an overall sensitivity of 91%.
Gadolinium-enhanced spin echo sequences and fat-suppressed images have further
improved speci®city (
). Many investigators have proved that MRI is accurate as
a method of detecting ON before clinical and radiographic changes become evident.
MRI has also been shown to be a better predictive test for subsequent femoral head
Figure 3. Total destruction of the femoral head.
Osteonecrosis 403
collapse (31%) than bone scanning.
MRI is indispensable in the accurate staging of ON
because it re¯ects the size of the lesion and the rough stage of the disease. MRI is today
the `gold standard' of non-invasive diagnostic methods in ON. Its sensitivity is 100% in
the post-collapse stages but only 80±100% in the pre-collapse stages. The speci®city of
MRI is 75±100%.
MRI images re¯ect histological changes. A central area of high signal intensity above
or within a low signal intensity ring corresponds to necrotic bone and marrow that has
not been reached by invading capillaries and mesenchymal tissue. The low signal
intensity band or ring represents the repair tissue interface of the mesenchymal and
®brous tissue, cellular debris and thickened trabecular bone adjacent to the necrotic
Most importantly, it can be followed from one corticle to the other on coronal
and saggital views, in contrast to the abnormalities caused by subchondral bone
fracture. Joint eusion is also demonstrated by T2-weighted MRI images.
Based on the results of dierent studies that compare histological and MRI ®ndings,
the following classi®cation system of MRI signal abnormalities may help to improve the
evaluation of ON:
. Type I. A band- or ring-like pattern with low signal intensity that surrounds a high
signal intensity central zone.
. Type II. A segmental pattern with a low signal intensity on T1-weighted images
(
) and an increase in signal intensity in the distal portions on T2-weighting.
. Type III. A segmental pattern with a low signal intensity on both T1- and
T2-weighted images (
). This classi®cation scheme may be extended to include
a diuse pattern of marrow abnormality with a low signal intensity on T1-weighting
and a high signal intensity on T2-weighting, which may indicate early ON in the
absence of radiographic ®ndings or focal subchondral MRI signal changes.
MRI may be employed prior to more costly interventional procedures used to detect
ON, such as core biopsy and decompression. MRI is also indicated in those patients in
whom the distinction between dierent hip disorders is dicult using other techniques.
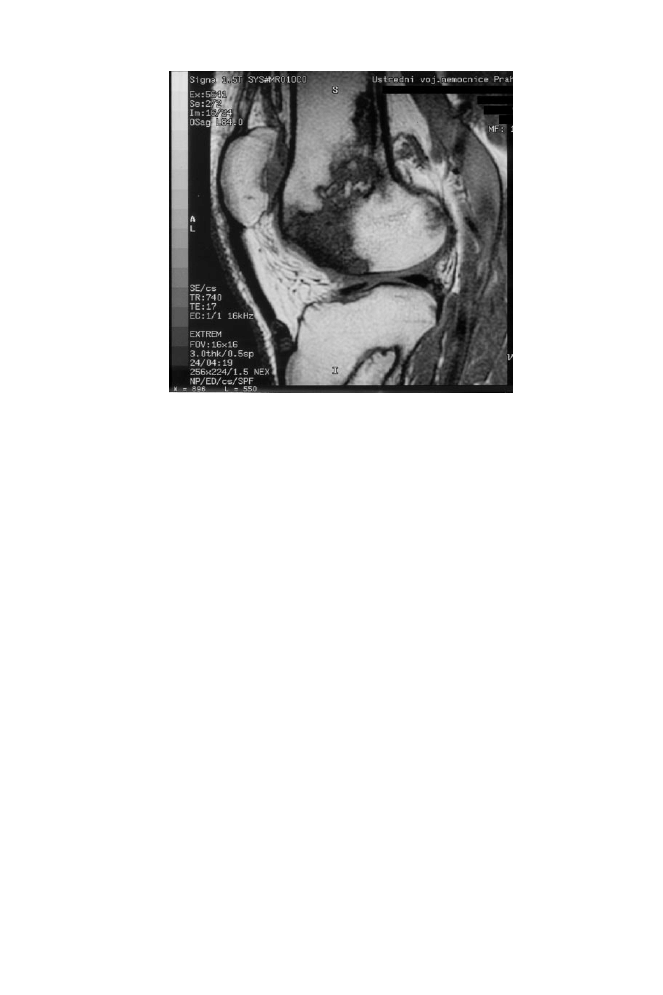
Figure 4. Large area of osteonecrosis of the knee on a T1-weighted frontal image. This shows stage III disease
in the femoral condyle.
404 K. Pavelka
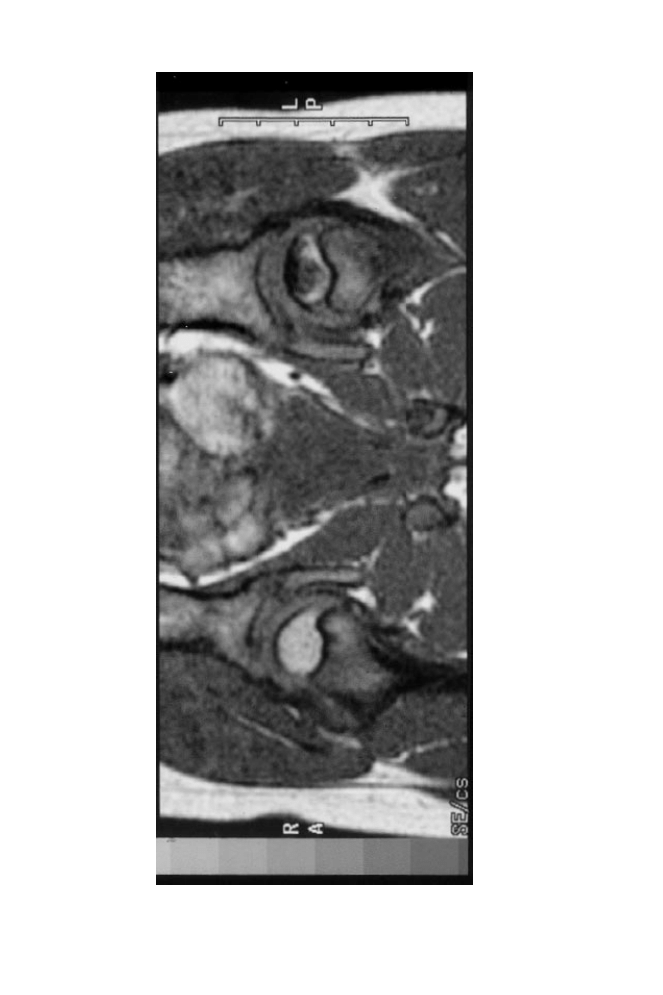
Figu
re
5.
T1
-w
ei
gh
te
dc
or
on
al
im
ag
eo
ft
he
pe
lv
is
de
m
on
st
ra
tin
ge
ar
ly
-st
ag
eO
No
ft
he
fe
m
or
alh
ea
do
nt
he
le
ft
sid
e.
Osteonecrosis 405
Other investigations
Functional bone investigation can be carried out by the measurement of bone marrow
pressure, and intramedullary venography, demonstrating a decreased blood ¯ow with
increased bone marrow pressure, which is present in the early stages of all cases of
ON. Superselective angiography has now been replaced by MRI.
STAGING SYSTEMS FOR ON
The severity of ON has been categorized using several dierent staging systems. For
example, Ficat and Arlet
proposed a system based on radiographic, haemodynamic
and symptomatic criteria, which had four stages: stages 1 and 2 were the early stages,
with reversible bone changes, stages 3 and 4 being described as end-stage disease with
irreversible destruction of the bone and joint structures. The nomenclature
subcommittee of ARCO (l'Association de Recherche en Circulation Osseuse) has
recently proposed a new internationally accepted system of classi®cation of the various
stages of ON (
).
This system should help researchers carrying out comparative
epidemiological studies, as well as when comparing dierent methods of treatment.
OSTEONECROSIS IN PATIENTS WITH SLE
Osteonecrosis has been recognized as an important cause of disability in lupus,
occurring in 10% of patients followed for a long period of time.
Up to two-thirds of
Figure 6. A T1-weighted saggital image shows marked hypointensity of the condyle and surface irregularity
of the patellar cartilage consistent with chondromalacia.
406 K. Pavelka
patients with SLE who develop ON are receiving high-dose steroids. They are usually
younger and have active disease with multiple organ involvement.
The hip is the most commonly involved joint, but other joints can also be aected.
We have reported young women who have developed seven sites of ON after 2 years
of SLE treated with high steroids.
The mechanism of the pathology of ON in SLE
patients is unclear. Vasculitis has been found in only a minority of histological samples
from osteonecrotic bones. Nagasawa et al have proposed abnormal haemostatic states
in these patients.
They detected abnormalities on MRI investigation of the hip in 35%
of patients with SLE with hip pain and a negative radiograph. The prevalence of ON in
SLE patients with anti-phospholipid antibodies is unknown.
ON IN PATIENTS TREATED WITH CORTICOSTEROIDS
Steroid-induced ON is a disease of modern medicine. The mechanism of ON in these
patients is not well known. Speculation has revolved around fat metabolism, with fat
embolization causing vascular occlusion.
Other biochemical factors may, however, be
involved, for example cellular cytotoxic factors. Pathology may result from a direct
metabolic eect on the osteogenic cells.
In a study of patients receiving gluco-
corticosteroid replacement therapy, the incidence of ON was 2.4%.
In renal trans-
plant patients on steroid therapy, the incidence is 5%.
Brinker et al
reported a high incidence of ON in patients treated for a short time
(6 weeks) with high-dose steroids (20 mg or more). Estimating the incidence of ON in
patients with rheumatoid arthritis and other connective tissue diseases is dicult
because of the possible in¯uence of underlying active disorder. It is generally accepted
that the risk of low-dose corticosteroids is relatively small and that even patients
treated for a long time will not develop ON.
Nevertheless, many questions regarding corticosteroid-induced ON have still to be
answered, for example concerning (a) the dose, route and duration of corticosteroid
Table 2. ARCO staging of osteonecrosis.
Stage
Findings
Diagnostic Techniques
0
All imaging methods are normal or
non-diagnostic; necrosis on biopsy
Biopsy and histology
1
Radiographs and CT scan normal
Positive result from at least one of the
techniques opposite
Radionuclide scan, MRI
Functional bone investigation
2
Radiographic abnormalities without
collapse (sclerosis, cysts, osteopenia)
Biopsy and histology
3
Crescent sign
Radiographs
4
Flattening or evident collapse
CT scan initially
5
As for stage 4, with narrowing of the
joint space
Radiographs only
6
As for stage 5, with destruction of
the joint
CT computed tomography; MRI magnetic resonance imaging.
Osteonecrosis 407

therapy necessary to induce ON, (b) the minimum and maximum time intervals
between corticosteroid usage and the onset of ON, and (c) host factors that modulate
these events.
OTHER FORMS OF ON
There are a number of other conditions of undetermined aetiology that represent
variants of avascular necrosis, some of which predominantly involve children.
These include Legg±Calve±Perthes disease, KoÈhler's disease, Freiberg disease, osteo-
chondritis dissecans and various other conditions. Dierent areas of the body can be
aected, and the treatment and prognosis often vary considerably from those
described in the treatment of ON of the femoral head in the adult.
Congenital dislocation of the hip in infants
ON in congenital dislocation of the hip (CDH) may result from abduction splinting.
During the one-stage surgical treatment of CDH, it was shown to develop in 3 out of
33 hips.
The rate of ON was comparable to that developing when traction was used.
The application of Pavlik's harness is also associated with a high incidence of ON
Legg±Calve±Perthes disease.
Perthes disease usually aects children between 4 and 12 years of age. It can be uni- or
bilateral and is probably related to an alteration of the blood supply to the femoral
There is usually no history of trauma.
Perthes disease has many variations. The prognosis varies with the size of the
aected segment and the age of the child. When disease appears early in life, the
processes of repair are most active. Sometimes large areas or even a whole necrotic
femoral head may be gradually replaced by viable bone. The remodelling process may
lead to a ¯attening and enlargement of the head and a broadening of the neck,
although in some patients the femoral head can be nearly normal. The more residual
distortion there is, the more likely the patient is later to develop secondary
osteoarthritis.
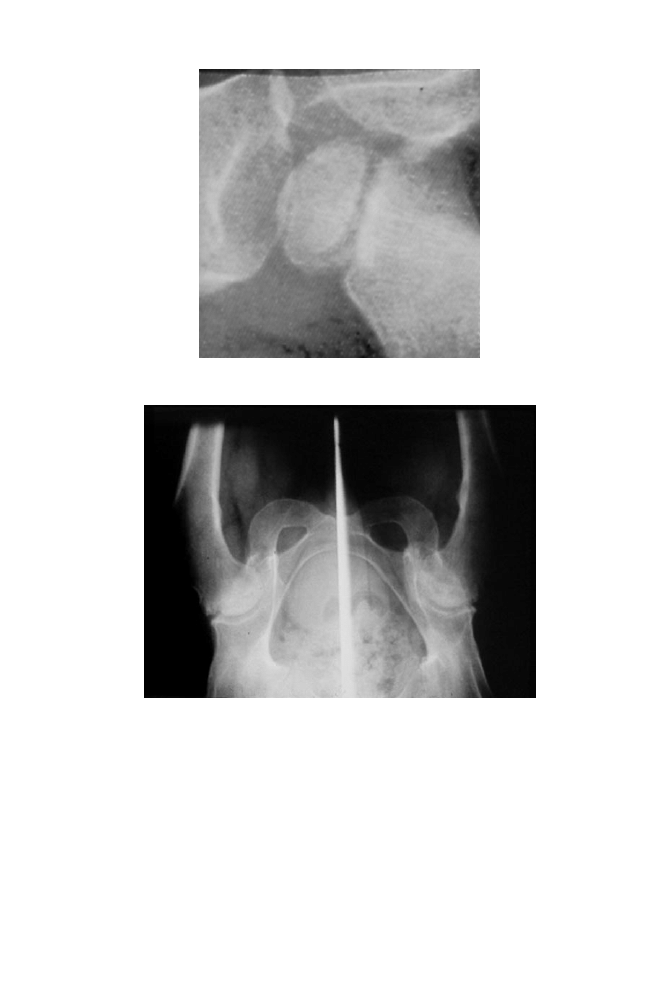
shows radiographs of a boy with Perthes disease, who was
operated on at the age of 15 (pelvic osteotomy) and again on his hips 10 years later, at
the age of 25.
The treatment of Perthes disease can be either surgical or non-surgical. Remodelling
of the femoral head is best if it can be contained within the acetabulum during the
healing process. The aected limb should therefore be maintained in a moderate
degree of abduction by the use of any one of a number of splinting or bracing devices.
In this position, full weight-bearing is often allowed. The surgical procedures, including
osteotomies of the pelvis and of the proximal femur, provide better coverage and
containment of the femoral head within the acetabulum, improving anatomical
relationships and eliminating the need for years of bracing in abduction.
Trauma
Intracapsular fractures or compressive fractures, as well dislocations, can compromise
the blood supply to the femoral head, which can lead to a higher incidence of ON. The
408 K. Pavelka

exact prevalence data are unknown. Trauma is also a common factor in ON of the
carpal (especially the semilunar and scaphoid) bones.
Osteochondritis dissecans
Osteochondritis dissecans is a speci®c condition in which a fragment composed of
articular cartilage and subchondral bone becomes demarcated and often separated
from the surrounding bone and cartilage. The aetiology of this condition is unknown;
local ischaemia and trauma have been implicated so it is similar to ON in this respect.
The most commonly aected site is the distal femur, but the talus, elbow and hips can
be aected as well. The clinical manifestations are usually knee pain, swelling, eusion,
functional impairment and limping.
Radiographically, osteochondritis dissecans appears as a well-circumscribed sclerotic
lesion, which is separated from the surrounding bone by a radiolucent line.
The
osteochondral fragment may remain in situ or it may be separated from the subchondral
bone and displaced into the joint (
). When evaluating the extent of involvement,
other imaging methods (tomography and MRI) or arthroscopy can be employed.
Figure 7. Morbus Legg±Calve±Perthes, showing a smoothly ¯attened femoral head and acetabular margin
with a prominent greater trochanter. (The patient developed morbus Perthes in 1987 when he was 13, an
osteotomy being performed in 1989, result as shown in 1999.)
Osteonecrosis 409
The prognosis and treatment of osteochondritis dissecans depend on the joint
involved, the size of the lesion and the age of the patient. The chance of spontaneous
healing is better in the young, skeletally immature patient. Treatment is either
conservative (including immobilization) or surgical. Many of the surgical procedures are
performed arthroscopically. The replacement of necrotic cartilage by osteochondral
allograft is sometimes necessary, with acceptable results. Surgery should be considered
only when skeletal growth is over as some of the images are mere aberrant loci of
ossi®cation.
MANAGEMENT OF ON
Preventative measures must, whenever possible, be instigated. Hyperlipidaemia and
diabetes should be treated and alcohol intake minimized. All cases of new applications of
corticosteroids, especially if for longer than a month or if given in a higher dose, should
be carefully considered. Most decompression accidents can be avoided if all decom-
pressions follow the established rules (slow resurfacing with a staged decompression).
The principal decision at the beginning of the treatment is that of surgical versus
non-surgical management. This decision is highly in¯uenced by the potential reversi-
bility of the process, based on the staging of the ON. In Ficat's staging, the reversible
stages are stages I and II.
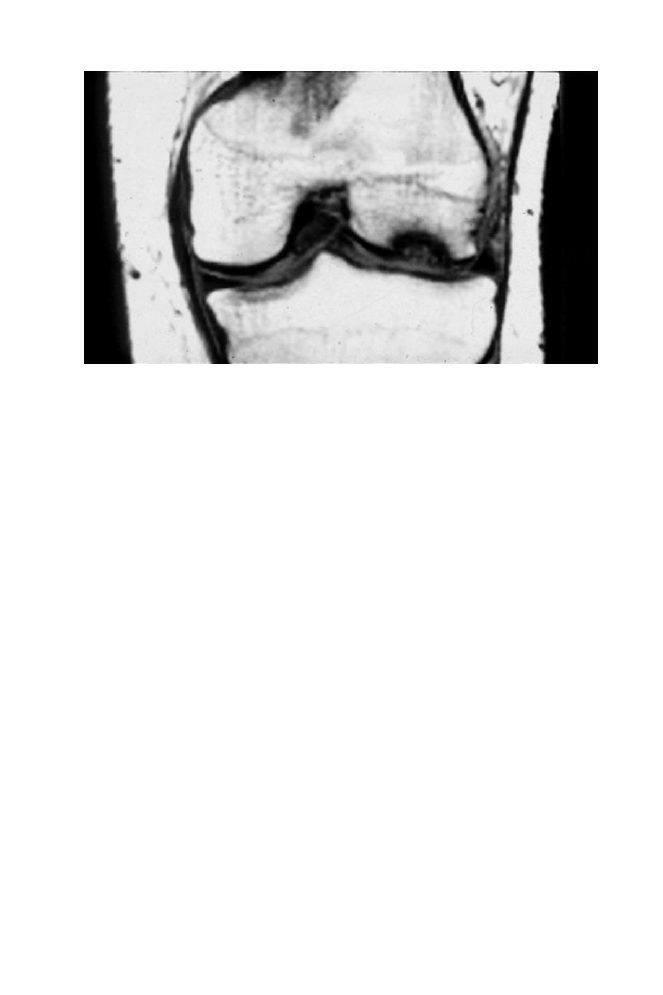
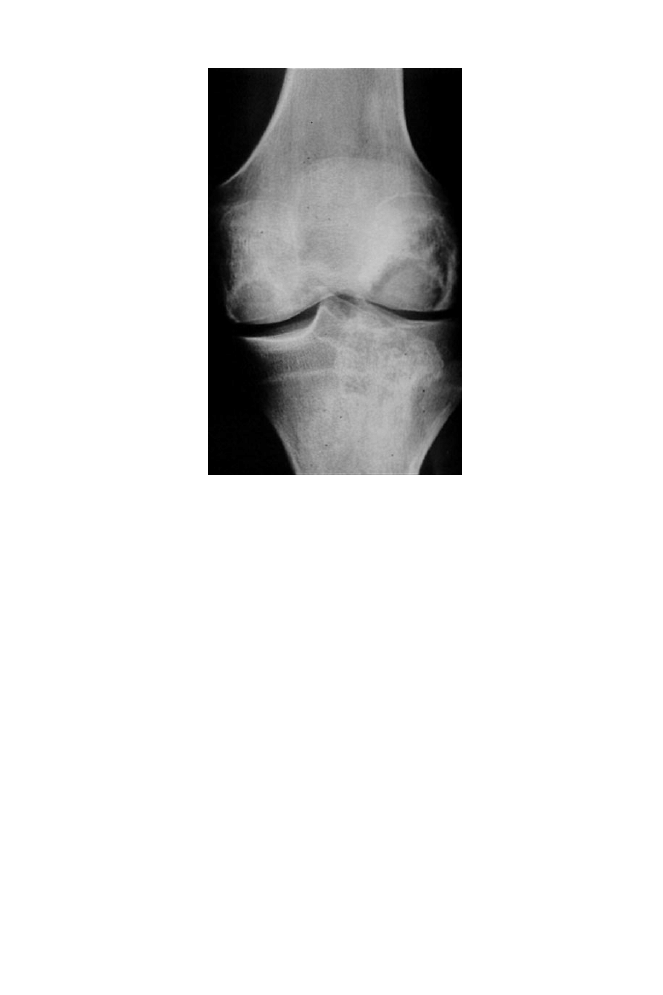
Figure 8. Osteochondritis dissecans. A frontal view showing subchondral ¯attening and a radiolucent
area along the medial femoral condyle. There is a transchondral fracture, the bone fragment having remained
in situ.
410 K. Pavelka

Conservative treatment
The discontinuation of weight-bearing for at least 4±8 weeks, using high crutches, is
necessary. This may be eective, especially in ON with involvement of the medial
aspect of the femoral head and an extent of less than one-quarter of the diameter of
the head.
Surgical treatment
Core decompression decreases intramedullary pressure within the femoral head and
neck, and improves circulation in the femoral head. Mont and Hungerford
have
reviewed 42 reports and found satisfactory clinical results in 63.5% after surgery
compared with only 22.7% after non-operative treatment. When considering only pre-
collapse hips, the results were good in 41.0% and 35.4% respectively. Decompression
can be accompanied by bone grafting using cortical or cancellous bone.
Dierent osteotomies have been used in various planes. Belal and Reichelt
reviewed the results of trochanteric rotational osteotomies. The results tended to
deteriorate over time. Despite the overall unsatisfactory results at ®nal follow-up, the
procedure was valuable as it delayed the need for total hip arthroplasty. The mean
time to arthroplasty was nearly 7 years.
In the later stages, the method of choice is total hip replacement. The results of this
operation in ON are not as good as those in other diseases of the hip (such as
osteoarthritis). The outcome after arthroplasty is also related to the aetiology, better
results being obtained in idiopathic ON (92.3% good results) than in alcohol-induced
ON (87%), renal transplantation (78%) and SLE (62.5%).
The choice of surgical procedure must be made according to the stage of the
disease. It is extremely important to evaluate by proper methodology the integrity of
the subchondral plate. In the pre-collapse stages, core decompression may be
successful. In cases with the crescent sign or a little ¯attening of the femoral head,
osteotomy or bone grafting can be used. In cases of evident collapse, total hip
replacement is the most important method.
SUMMARY
Osteonecrosis is not a speci®c disease entity but the ®nal common pathway of a number
of conditions that lead to impairment of the blood supply to the bone. The reasons for
this can be traumatic or non-traumatic. Pathogenetic factors are well known in some
cases of non-traumatic ON but poorly understood in others. In serious studies of non-
traumatic ON, the majority of cases occurred in patients treated with corticosteroids, in
patients with systemic connective disease (such as SLE) and in alcoholics. The most
commonly aected sites are the femoral head, the humeral neck, the knees and the
small bones of the hands and feet. The clinical picture is non-speci®c, and depends on
localization, size, associated conditions and the evolutive phase. The evidence-based
diagnosis of ON initially relies heavily on imaging methods and eventually on bone
marrow pressure determinations and bone marrow biopsy. Because the early stages of
ON are radiographically silent, MRI is the gold standard of diagnosis at this stage.
Radiographic changes include diuse osteopenia and a central subchondral of
radiolucency (the crescent sign, indicating a subchondral fracture); later changes include
¯attening and gross collapse of the bone. The process terminates in severe secondary
osteoarthritis.
Osteonecrosis 411
For proper treatment and prognosis, many staging systems have been developed, of
which the ARCO system is now internationally accepted. Therapy can be conservative
or surgical. Conservative therapy involves a discontinuation of weight-bearing for
at least 8 weeks but is eective only in the earlier stages of ON. The alternatives in
surgical treatment are core decompression, various osteotomies and ®nally total joint
replacement.
Acknowledgement
The author would like to thank Dr Gatterova for help with radiographic documentation, and
Dr CharvaÂt for help with MRI documentation.
Practice points
When should one think about osteonecrosis?
The clinical symptoms of ON are absolutely non-speci®c, and the radiographic
picture is negative in the early stages of the disease. An early diagnosis can be made
by more sophisticated (and expensive) techniques, so the timing of these
investigations is of critical importance. When should we thus consider these
investigations?
. sudden, intensive pain of the hip, which persists, often present at rest, with
minimum signs of OA on a radiographic picture
. pain in other less frequent localizations of ON in at-risk patients, especially in
the shoulder, knee and small joints of the hands and feet
. any history of trauma with or without dislocation
. the special risk group who might have caisson or diver's disease
. related to the age of the patient: in young patients, think of Perthes disease
and other special forms of avascular necrosis; in old patients, think also of
tumours, arteriosclerosis and other occlusive vascular disorders, gout and
metabolic bone disease
. think of ON when facing any hip pain in patients with risk factors of ON
(SLE, corticosteroid therapy or alcohol abuse)
. MRI is the gold standard for diagnosis in the early stages
Research agenda
. the aetiopathogenesis of idiopathic and other forms of ON needs to be
investigated
. exact early diagnosis in the pre-collapse stage is necessary
. a study should be made of the therapeutic use of bone morphogenic proteins
and bone marrow stem cells
412 K. Pavelka

REFERENCES
1. Montela BJ, Nunley JA, Urbaniak JR et al. Osteonecrosis of the femoral head associated with pregnancy.
Journal of Bone and Joint Surgery 1999; 81A: 790±798.
2. Nobillo R, Le Pare JM, Benwit J et al. Idiopathic osteonecrosis of the hip in twins. Annals of the Rheumatic
Diseases 1994; 53: 702.
3. Gluck CJ, Gluck H, Welch M et al. Familial idiopathic osteonecrosis mediated by familial hypo®brinolysis
with high levels of plasminogen activator inhibitor. Thrombosis and Haemostasis 1994; 71: 195±198.
* 4. MazieÁres B. Osteonecrosis of the femoral head. Rheumatology in Europe 1999; 28: 68±72.
* 5. Ninomija S. An Epidemiological Survey of Idiopathic Avascular Necrosis of the Femoral Head in Japan. Annual
Report of Japanese Investigation Committee for Intractable Disease. Osaka: University Publisher, 1984.
6. Veenstra DL, Pharm D, Best JH et al. Incidence and long-term cost of steroid-related side eects after
renal transplantation. American Journal of Kidney Disease 1999; 33: 829±839.
* 7. Zizic TM, Marcoux C, Hungerford DS et al. Corticosteroid therapy associated with ischemic necrosis of
bone in systemic lupus erythematosus. American Journal of Medicine 1985; 79: 596±609.
8. Killoyne RF & Nuss R. Femoral head osteonecrosis in a child with hemophilia. Arthritis and Rheumatism
1999; 42: 1550±1557.
9. Cushner FD & Friedman RJ. Osteonecrosis of the femoral head. Orthopedic Reviews 1988; 17: 29±34.
10. Frostick SP & Wallace WA. Osteonecrosis of the humeral head. Clinical Rheumatology 1989; 3: 651±657.
11. Heenkeler M & Gerster JC. Osteonecrosis of the femoral condyle. Case reports of 7 patients and
literature review. Revue Medicale de Suisse Romande 1995; 115: 127±131.
12. Drury P & Sartoris DJ. Osteonecrosis in the foot. Journal of Foot Surgery 1991; 30: 477±483.
13. Jensen C & Leicht P. Idiopathic avascular necrosis of the scaphoid in a child. Scand J Plast Reconstr Surg
Handtung 1995; 29: 359±360.
14. Dumontier C. Kienbock's disease. Current data. Annales de Radiologie de Paris 1992; 35: 373±383.
15. Heick A. Juvenile avascular necrosis of the odontoid process. A review on the etiology of os
odontoideum and absentia odontoidei. Danish Medical Bulletin 1996; 43: 363±366.
16. Mirzai R, Chang C, Greenspan A et al. The pathogenesis of osteonecrosis and the relationship to
corticosteroids. Journal of Asthma 1999; 36: 77±95.
*17. Chang C, Greenspan A & Gerschwin M. Osteonecrosis: current perspectives on pathogenesis and
treatment. Seminars in Arthritis and Rheumatism 1993; 23: 47±69.
18. Steinberg E & Steinberg DD. Osteonecrosis. In Kelly WN, Harris ED, Ruddy S & Sledge CB (eds)
Textbook of Rheumatology, pp 1749±1773. Philadelphia: WB Saunders, 1984.
*19. Shinoda S, Hasegawa Y, Karonsahi S et al. Magnetic resonance imaging of osteonecrosis in divers:
comparison with plain radiographs. Skeletal Radiology 1997; 26: 354±359.
20. Rhoad RC, Davidson RS & Heyman S. Pretreatment bone scan in SCFE. A predictor of ischemia and
avascular necrosis. Journal of Pediatric Orthopedics 1999; 19: 164±168.
*21. MazieÁres B, Arlet J, Boussaton M et al. Assessment of intramedullary pressure versus bone scintigraphy
in the diagnosis of osteonecrosis of femoral head. In Arlet J & MazieÁres B (eds) Bone Circulation and Bone
Necroses, pp 264±266. Berlin: Springer-Verlag, 1990.
22. Glickstein MF, Benk DL, Schreibeer ML et al. Avascular necrosis versus other diseases of the hip:
sensitivity of MRI imaging. Radiology 1988; 169: 213±216.
23. Kokubo T, Takatori Y, Ninomiya S et al. Magnetic resonance imaging and scintigraphy of avascular
necrosis of femoral head. MR Imaging and Scintigraphy 1992; 27: 54±60.
24. Jergesen HE, Lang P, Moseley ME & Genant HK. Histologic correlation in magnetic resonance imaging of
femoral head osteonecrosis. Clinical Orthopaedics 1990; 253: 150±163.
25. Turner DA, Templeton AC, Selzer P et al. Femoral capital osteonecrosis: MR ®ndings of diuse marrow
abnormalities without focal lesions. Radiology 1989; 171: 135±140.
*26. Ficat RP & Arlet J. Ischemia and Necrosis of Bone. Baltimore: Williams & Wilkins, 1980.
27. Pavelka K, Gatterova J & Pavelkova A. Multiple osteonecrosis by patient with systemic disease, treated by
corticosteroids. CÆeska Revmatologie 2000 (in press).
*28. Nagasawa K, Tsukamoto H, Tada J et al. Imaging study on the mode of development and changes
in avascular necrosis of the femoral head in systemic lupus erythematosus: long term observations.
British Journal of Rheumatology 1994; 33: 343±347.
29. Glimcher MJ & Kenzora JE. The biology of osteonecrosis of the human femoral head and its clinical
implications: tissue biology. Clinical Orthopaedics 1979; 138: 284±309.
30. Vreden SG, Hermus AR & Liessu PA. Aseptic bone necrosis in patients on glucocorticosteroid
replacement therapy. Netherlands Journal of Medicine 1991; 39: 153±157.
31. Brinker MR, Rosenberg AG, Kull L et al. Primary total hip arthroplasty using noncemented porous
coated femoral components in patients with ON of the femoral head. Arthroplasty 1994; 9: 457±468.
Osteonecrosis 413

32. Langkamer VG, Clerke NMP & Witherow P. Complications of splinting in congenital dislocation of the
hip. Archives of Disease in Childhood 1991; 66: 1322±1325.
33. Galpin RD, Roach JW, Wenger DR et al. One stage treatment of congenital dislocation of the hip in
older children including femoral shortening. Journal of Bone and Joint Surgery 1989; 71A: 734±741.
34. Suzuki S & Yamemuro T. Avascular necrosis in patients treated with the Pavlik harness for congenital
dislocation of the hip. Journal of Bone and Joint Surgery 1990; 72A: 1048±1055.
35. Suramo J, Puranen J & Heikkinen E. Disturbed patterns of venous drainage of the femoral neck in
Perthes' disease. Journal of Bone and Joint Surgery 1974; 563: 443±453.
*36. Resnick D & Niwayama G. Diagnosis of Bone and Joint Disorders, vol. 5. Philadelphia: WB Saunders, 1988.
37. Mont MA & Hungerford DS. Non-traumatic avascular necrosis of the femoral head. Journal of Bone and
Joint Surgery 1995; 77A: 459±474.
*38. MazieÁres B. Osteonecrosis. In Klippel JH & Dieppe PA (eds) Rheumatology, 2nd edn, pp 8.47 1. London:
Mosby 1998.
39. Belal MA & Reichelt A. Clinical results of rotational osteotomy for treatment of avascular necrosis of the
femoral head. Archives of Orthopedic and Trauma Surgery 1996; 115: 80±84.
414 K. Pavelka
Document Outline
- Osteonecrosis
- EPIDEMIOLOGY
- PATHOGENESIS
- CLINICAL MANIFESTATIONS
- EVIDENCE-BASED DIAGNOSIS OF ON
- STAGING SYSTEMS FOR ON
- OSTEONECROSIS IN PATIENTS WITH SLE
- ON IN PATIENTS TREATED WITH CORTICOSTEROIDS
- OTHER FORMS OF ON
- MANAGEMENT OF ON
- SUMMARY
- Acknowledgement
- REFERENCES
- Tables
- Figures
Wyszukiwarka
Podobne podstrony:
Experimental avascular osteonecrosis
Experimental avascular osteonecrosis
13 przebudowa osteonu
więcej podobnych podstron