
C H A P T E R
17
Interventional
Neuroradiology
Jose A. Bauza
Interventional neuroradiology is a new discipline that is gain-
ing acceptance in medicine as an alternate form of therapy
for selected neurological lesions. It has been made possible
because of the development of small catheters and guide-
wires that can be navigated into selected branches of the
inlracranial or extracranial vasculature.' Embolic materials
have become available that allow vascular occlusion of very
small vessels. Catheters and guidewires, as small as 2 and 3
French, allow selective catheterization of even the smallest
arteries. This permits the angiographer to investigate lesions
discretely. Embolic materials, now available, include solid
agents (polyvinyl alcohol particles, Gelfoam powder, coils,
or balloons) or liquid agents (cyanoacrylates or dehydrated
ethanol). The choice of embolic material is dictated by the
location of the lesion and the end point or goal of the
procedure.
INDICATION
Interventional neuroradiology may be indicated in the non-
operative treatment of some solid tumors of the central or
peripheral nervous system. This includes meningiomas and
the intraarterial chemotherapy of malignant brain tumors.
Many vascular lesions, such as some arteriovenous malfor-
mations, dural arteriovenous fistulae, traumatic arteriove-
nous fistulae, vein of Galen malformations, intracranial an-
eurysms, and spinal vascular malformations are ideally
suited for interventional neuroradiology.
4
Thrombolysis of
intracranial vascular disease is a new form of therapy that is
gaining favor for use of interventional radiology in the
treatment of cerebrovascular disease. Likewise percutaneous
transluminal angioplasty of major branches of the carotid
and vertebrobasilar systems is indicated in selected cases of
blood vessel spasm or occlusive vascular disease.
SOLID LESIONS
MENINGIOMAS
These vascular lesions arise from the meningothelial cells lo-
cated throughout the meninges, most commonly adjacent to
the arachnoid villae and the dura which surrounds the exit of
the cranial nerves.
2
They receive their blood supply from dural
vessels but may parasitize pial vessels to supply their surface.
3
The definitive treatment of a meningioma is surgical resection.
Selective embolization of supplying branches can result in
devascularization of the lesion, causing tumor necrosis and a
decrease in size. Preoperative embolization will shorten the
operative time and reduce the surgical blood loss.
4
Preoperative embolization consists of selectively catheter-
izing and performing angiograms of all arterial feeders to the
meningioma. Embolization is usually performed using poly-
vinyl alcohol microparticles (PVA) 150 to 300 p-m (Fig.
17-1). Smaller particles (Gelfoam powder) or liquid agents
may provide a deeper penetration into the tumor but carry
increased risk of undesirable side effects. The cranial nerves
are also supplied by branches of the external carotid artery.
Preservation of the petrosal branch that supplies the facial
nerve is paramount.
3
'
5
PARAGANGLIOMAS
Paragangliomas, also known as glomus tumors or chemo-
dectomas, arise from nonchromaffin paraganglioma cells
located at the carotid artery bifurcation, middle ear, or the
ganglion nodosum of the vagus nerve. Less-common loca-
tions include the larynx, orbit, nose, or aortic arch.
6
The
majority of these lesions are nonsecretory, but in 5 percent
of cases where the lesion secretes catecholamine, manipula-
333
334 CHAPTER 17
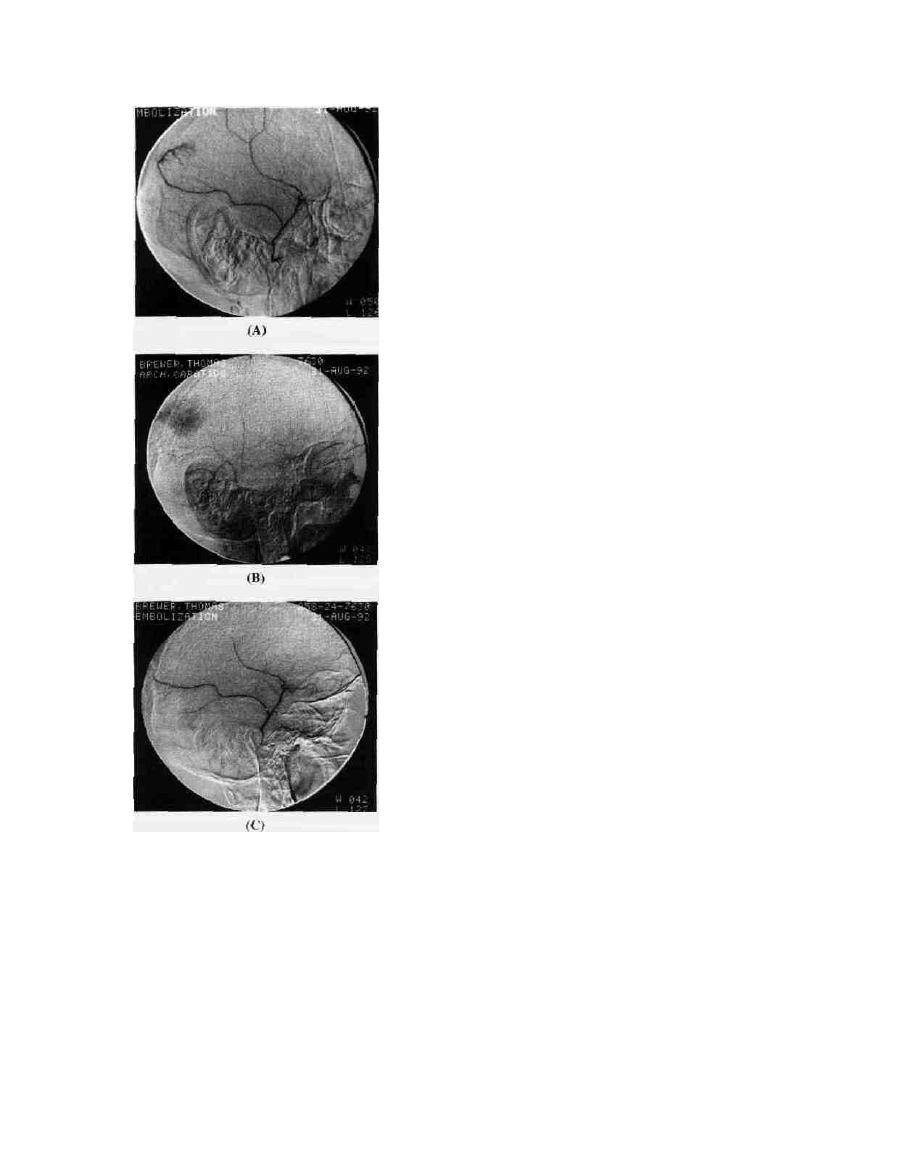
Figure 17-1 Meningioma. A. Selective middle meningeal artery
injection shows early tumoral blush from posterior branch. B.
Capillary phase shows tumoral blush. C. Microparticles show
absence of tumoral blush.
tion can precipitate a hypertensive crisis.
5
-
7
Rarely surgical
removal or embolization of these lesions can produce severe
hypotension. Because of these two worrisome features of
paragangliomas, suspected secretors should be evaluated for
urinary vanillylmandelic acid (VMA) or 5-hydroxyindole-
acetic acid (5-HIAA), and patients should be treated with
alpha blockers and volume expanders prior to any surgical
procedure.
Tumors involving the carotid body and vagus nerve gan-
glion are usually supplied by the external carotid artery, while
those located in the jugulotympanic region receive their blood
supply primarily from the ascending pharyngeal branch of the
external carotid artery, occasionally parasitizing blood from
the vertebrobasilar system. Selective catheterization of the in-
ternal and external carotid arteries should be accomplished in
the vascular territory of the lesion. Embolization can be per-
formed immediately after the diagnostic angiogram. Micropar-
ticles or liquid agents can be utilized.
7
-
8
INTRAARTERIAL CHEMOTHERAPY OF
BRAIN TUMORS
The systematic administration of chemotherapeutic agents is
frequently part of the overall surgical treatment of primary
malignant brain tumors. Because of the toxic side effects of
chemotherapeutic agents, the intraarterial approach has often
been recommended.
8
Interventional neuroradiologists are
often called upon to catheterize selectively arteries supplying
a malignant brain tumor so that chemotherapeutic agents
may be infused intraarterially.
9
This can be done by one of
two approaches. In the first, the catheter is placed in the
internal carotid artery with its tip in the cervical segment of
the vessel. Injections in this location can produce optic
complications including pain, increased intraocular tension.
and visual loss.
10
The second approach is to place the
intraarterial catheter beyond the origin of the ophthalmic
artery. While this protects the ophthalmic artery and the
eyes, it increases the neurotoxic effects of the chemothera-
peutic agents.
8
The neurotoxic effects include progressive
dysfunction in the ipsilateral hemisphere.
11
-
12
The neurotoxic
effects are dose-related and are dependent on the interval
between procedures and the cumulative dose. Nitrosoureas
appear to have the least-adverse side effects.
12
VASCULAR LESIONS
ARTERIOVENOUS MALFORMATIONS (AVMs)
Central nervous system arteriovenous malformations
(AVMs) may be fed entirely from branches of the internal
carotid artery (purely pial malformations) or fed entirely by
branches of the external carotid artery system (purely dural
malformations). In many instances, the blood supply to the
AVM comes from branches of both the internal and external
carotid systems (mixed pial-dural malformations).
13
Definitive treatment of AVMs may require surgery alone,
surgery after endovascular occlusion, radiosurgery and sur-
gery, or radiosurgery and endovascular occlusion. Interven-
tional neuroradiology for AVMs involves supraselective cath-
eterization and arteriography of each suspected feeding vessel.
If branches to normal brain arise from the blood vessel feeding
the malformation, that blood vessel cannot be embolized. In
those instances where vital portions of the brain are thought to
be irrigated by the same vessels supplying the malformation,
sodium amytal may be injected and the patient evaluated for
INTERVENTIONAL NEURORADIOLOGY
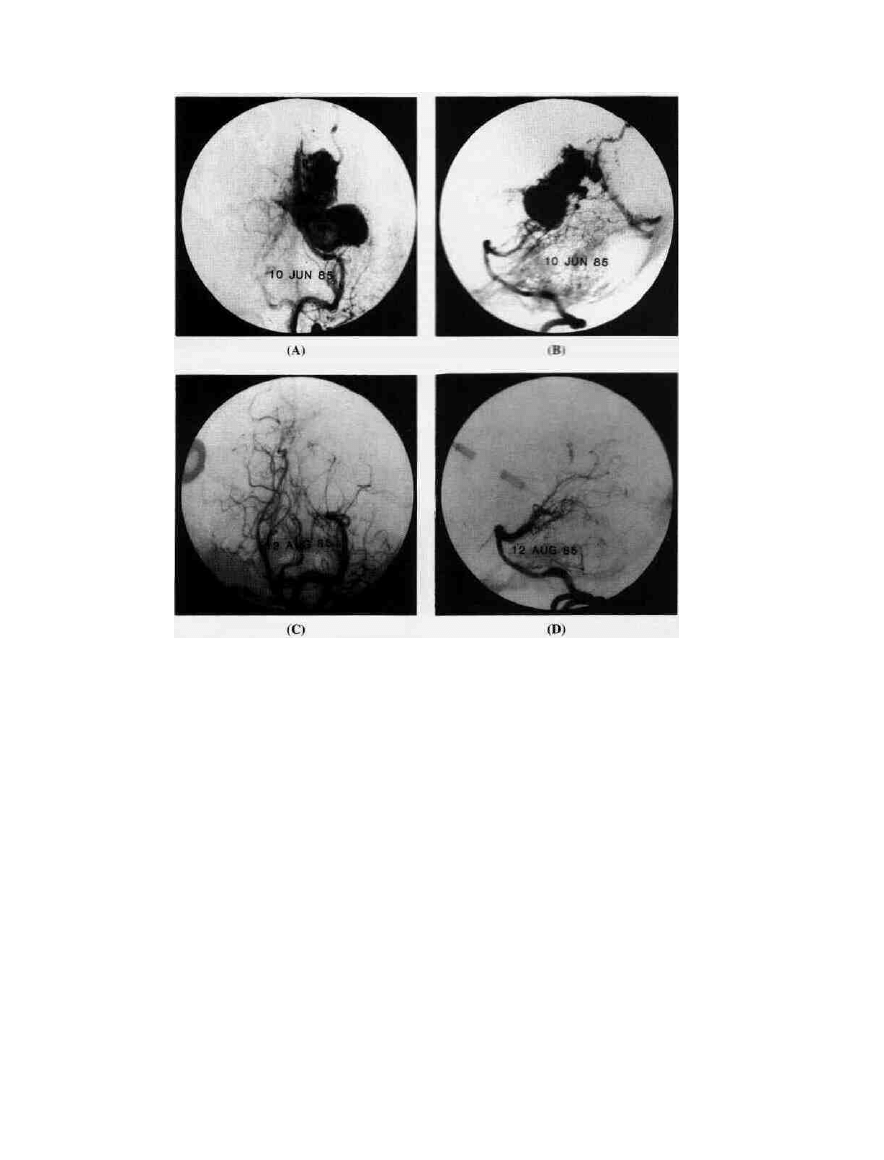
Figure 17-2 Arteriovenous malformation. A, B. AP and lateral projection reveal an AVM with
its main supply from the left posterior cerebral artery with early venous drainage. C, D.
Arteriogram after embolization with cyanoacrylates shows obliteration of the AVM.
(Case courtesy of Paul Pevsner.)
alterations in the electroencephalogram (EEG) and the neuro-
logical picture.
14
Embolization of those malformations will be
performed only if no adverse effects are noted on the EEG or
the neurological examination.
Acrylics are the most popular materials used in emboliz-
ing AVMs because of their ability to penetrate deeply into
the nidus of the malformation and permanently occlude it.
Other materials used include PVA, silk sutures, and bal-
loons. The use of acrylics decreases the chances of emboliz-
ing the venous drainage of the malformation or allowing
embolic particles to become pulmonary emboli.
15
Small AVMs can be completely obliterated by emboliza-
tion alone (Fig. 17-2). Larger lesions with multiple feeding
vessels usually require surgical excision or radiosurgery.
15
-
16
In many of these cases, preoperative embolization reduces a
portion of the blood flow to the malformation.
DURAL ARTERIAL FISTULAE
Dural arterial fistulae are abnormal connections between
arteries and veins that occur within the dura, most often
within the wall of a dural sinus. The arterial inflow is
usually from meningeal vessels, although on occasion pial
recruitment may occur.
17
-
19
Therapeutic methods for these
lesions include vascular compression, transarterial emboli-
zation, transvenous embolization, or surgical excision. If
the lesion involves the transverse or the sigmoid sinus, the
initial treatment may consist of manual compression of the
occipital artery behind the mastoid for up to 30 min.
18
The
diminished inflow can induce thrombosis. This technique
should not be performed on patients with cortical venous
drainage, hemorrhage, or infection. In patients with cavern-
ous sinus fistulae, manual compression of the carotid jugu-
lar vessels can be attempted. Again, patients with carotid
artery atherosclerotic disease, underlying hypercoagulable
states, high platelet counts, or patients receiving epsilon-
aminocaproic acid (EACA) should not be treated in this
manner.
If compression techniques fail, transarterial embolization
of the feeders should be attempted. PVA particles should be
used since liquid and polymerizing agents carry a great risk
of producing cranial nerve paralysis or stroke, i
7
336 CHAPTER 17
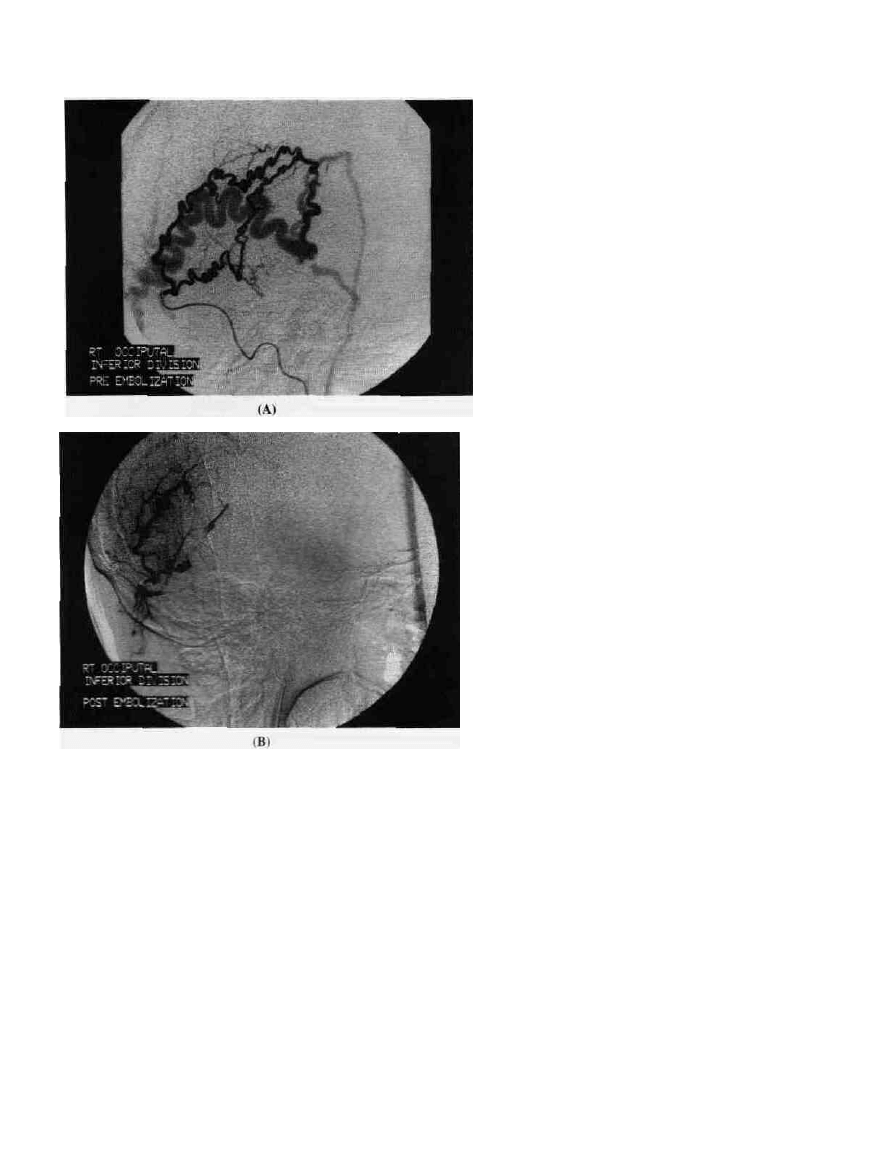
Figure 17-3 Traumatic arteriovenous (AV) fistula. A.
Supraselective arteriogram of the occipital artery shows two
prominent branches draining directly to a markedly dilated
draining vein. B. Arteriogram after embolization with PVA
microparticles and coils show nonfilling of the draining vein.
(Case courtesy nf Victor Toro.)
TRAUMATIC ARTERIOVENOUS FISTULAE
Traumatic arteriovenous fistulae represent abnormal com-
munications between an artery and a vein secondary to
traumatic laceration of the vessels (Fig- 17-3). Rarely they
arise spontaneously from preexisting aneurysms or angio-
dysplasia.
20
The most-common example of these is the trau-
matic carotid-cavernous fistula. Treatment of carotid cavem-
Ous fistulae is through endovascular occlusion with
detachable balloons. This is performed through a transfem-
oral approach with inflation of the balloon within the cav-
ernous sinus itself (Fig. 17-4).
20
-
21
In selected cases, a trans-
venous approach can be performed through the inferior
petrosal sinus with deposition of coils into the cavernous
sinus.
22
Rarely, a retrograde ophthalmic vein catheterization
is performed with the deposition of coils within the cavern-
ous sinus.
23
Emergency treatment of carotid cavernous fistu-
lae should be considered if the patient presents progressive
visual loss, rapidly increased intraocular pressure, severe
epistaxis, sphenoid sinus pseudoaneurysm, acute hemiplegia
without intracerebral hematoma, or subarachnoid hemor-
rhage.
Fistulae involving the vertebral system often involve the
vertebral artery and its epidural venous plexus or the internal
carotid artery and the adjacent internal jugular vein. These
may be treated with balloons, PVA, liquid agents, or coils.
24
VEIN OF GALEN MALFORMATIONS
Yasargil divides vein of Galen aneurysms into four types:
type I: fistulae located in the wall of a varix arising from
feeders from the anterior and posterior choroidal and/or the
pericallosal arteries; type II: fistulae with feeders from trans-
mesencephalic and transdiencephalic arteries; type III: a
combination of types I and II; type IV: diencephalic and
mesencephalic arteriovenous malformations draining into an
enlarged, but otherwise normal, vein of Galen.
25
INTERVENTIONAL NEURORADIOLOGY 337
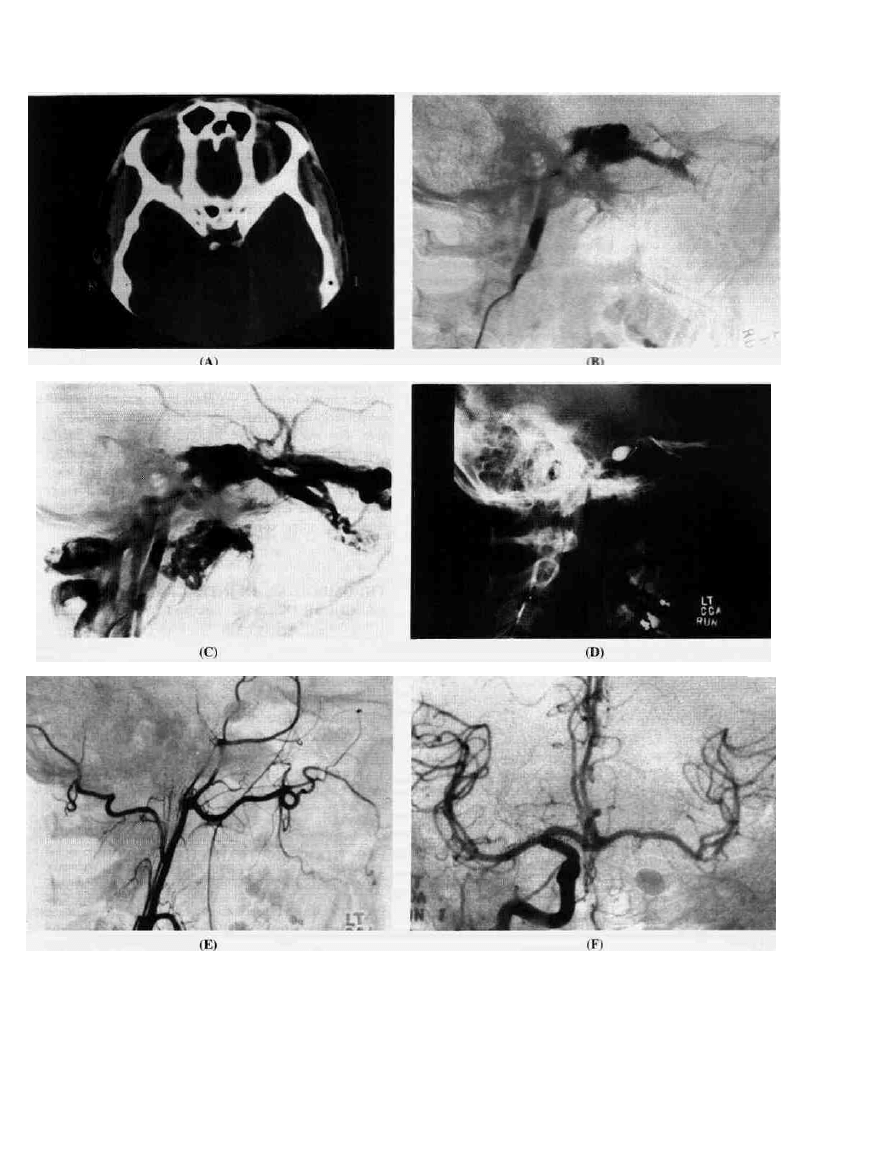
Figure 17-4 Carotids—cavernous fistula. A. Contrast-enhanced
CT through orbit demonstrates an enlarged left superior ophthalmic
vein (SOV). B, C. Lateral projection of left internal carotid artery
with opacification cavernous sinus and SOV. D. Lateral skull film
showing a balloon with radiopaque contrast material. E. Lateral
projection of left common carotid shows occlusion of the internal
carotid due to balloon placement. F. Right common carotid shows
crossflow to the left internal carotid artery territory.
338
CHAPTER ]'
Vein of Galen malformations may be approached through
transarterial or transvenous routes. They can be approached
transvenously through a retrograde femoral vein catheterization
or through a transtorcular approach following craniectomy. The
approach will depend on the type of lesion, the patient's condi-
tion, and the experience of the interventional neuroradiologist.
Emergent embolization of vein of Galen malformations
should be considered in newboms with refractile congestive
heart failure, symptomatic hydrocephalus, or severe neuro-
logical symptoms.
26
'
27
The type of embolic material will depend on the interven-
tional neuroradiologist's experience. For those lesions re-
quiring a transarterial approach, liquid glue or coils can be
used. These should be placed as close to the fistula as
possible. In the transvenous approach, coils are usually used.
ENDOVASCULAR TREATMENT OF
INTRACRANIAL ANEURYSMS
The endovascular treatment of intracranial aneurysms was
first described by Serbinenko in 1974.
28
: Indications for endovascular treatment include:
28
.
29
1. Prior surgical exploration of an aneurysm with inability
to clip the neck
2. Anatomic locations that are difficult to approach surgi-
cally
3. Fusiform aneurysms without a well-defined neck
4. Inability of the patient to tolerate general anesthesia
5. Patients with poor collateral circulation for whom by-
pass surgery is not possible
6. Aneurysms with high surgical risk because of their size
or location
Currently, a retrograde transfemoral approach is used; the
most widely used embolic agents are silicone balloons filled
with liquid glue. One or several balloons may be needed for
complete obliteration of the aneurysm lumen. Occasionally
coils are used to supplement the balloons.
29
-
31
Incomplete occlusion of the lumen of the aneurysm may
allow regrowth of die aneurysm or shift of the balloon
within the aneurysm lumen.-*
9
Other complications of bal-
loon occlusion of aneurysms include premature detachment
of the balloon, which may result in parent vessel occlusion
or distal embolization; aneurysm rupture during balloon in-
flation; or delayed thromboembolic events in an incomple-
tely treated aneurysm.
^Gulielmi has developed a platinum coil system coupled
with electrothrombosis, which induces clot formation within
the coil after the application of an electric current.
32
ENDOVASCULAR TREATMENT OF SPINAL
VASCULAR MALFORMATION
Spinal cord AVMs are true vascular lesions of congenital
origin.
33
The nidus may be purely intraparenchymal, on the
surface of the spinal cord or perimedullary. The blood sup-
ply is usually from the anterior and posterior radiculomedul-
lary arteries.
Embolization should be considered a first-line technique
in the treatment of spinal arteriovenous malformations.
33
-"
Currently, microparticles are the embolic agents of choice
since they present little risk to the patient. Their drawback is
a high frequency of arterial recanalization. Embolization
with liquid acrylic may produce permanent occlusion but is
more likely to cause acute ischemia. Spinal cord infarction
can occur, particularly when the anterior spinal artery i^
involved in the malformation.
VERTEBRAL HEMANGIOMAS
These tumors involve a vertebral body and may extend into
its posterior arch. They may be quiescent or quite aggres-
sive. For the aggressive lesions, embolization should be
considered prior to surgical intervention. This can be accom-
plished by percutaneously puncturing the vertebral body and
injecting acrylic within it (vertebroplasty). Particulate embo-
lization of the tumor can reduce or eliminate the compres-
sion of the spinal cord frequently seen with this lesion.
THROMBOLYSIS IN INTRACRANIAL OCCLUSIVE
VASCULAR DISEASE
Fibrinolytic therapy has a place in the treatment of acute
stroke due to a thrombus or embolus.
36
-
37
Urokinase or tissue
plasminogen activator (tpa) has been used for this purpose
but it is not indicated for many cerebral infarctions.
The thrombolytic agent is delivered by infusion through a
microcatheter positioned as closely to the site of the occlu-
sion as possible.
Complications of this form of therapy include intraparen-
chymal hemorrhage or propagation of a secondary thrombus.
PERCUTANEOUS TRANSLUMINAL
ANGIOPLASTY (PTA)
Percutaneous transluminal angioplasty (PTA) is an estab-
lished, efficacious method of treating arterial occlusive va-
scular disease.
38
-
40
Angioplasty of the carotid artery has been
performed in patients who are poor surgical candidates or
those in whom intensive anticoagulation therapy has failed
to control neurological symptoms. Some patients with severe
vasospasm secondary to subarachnoid hemorrhage have suc-
cessfully undergone PTA.
39
Subclavian artery PTA has been
performed on stenotic subclavian arteries as well as homola-
teral and contralateral vertebral arteries.
40
Complications of PTA include transient ischemia during
angioplasty or arterial spasm after angioplasty.

37. Levy DE: Medical treatment of acute, ischemic stroke. Neuroi-
maging Clinics of North America 3:597-605, 1992.
38- Tsai FY, Higashida R, Meoli C: Percutaneous transluminal
angioplasty of extracranial and intracranial arterial stenosis in
head and neck. Neuroimaging Clinics a/North America 2:371-
384. 1992.
39. Pistoia F, Horton JA, Sekhar L, Horowitz M: Imaging of blood
glow changes following angioplasty for treatment of vaso-
spasm.AJNR 12:446-448, 1991.
40. Theron AJ: Angioplasty of brachioeephalic vessels, in Vinuela
F, Halbach VV, Dion JE (eds): Interventional Neuroradiology:
Endovascular Therapy of the Central Nervous System. New
York, Raven, 1992, chap 13, pp 167-180.
STUDY QUESTIONS
1. A 27-year-old female had the sudden onset of headache
followed by a left hemiparesis and left-sided apraxia, which
persisted. A CT scan reveals a vascular malformation in the
left occipital lobe measuring 7 cm in greatest diameter.
There is a small subcortical hematoma in the posterior
parietal area. The malformation is fed by the right middle
and posterior cerebral arteries.
1. How could the malformation be most clearly outlined?
2. What alternate method might be used to outline the
lesion? 3. What method might be considered to reduce blood
flow to the malformation? 4. How would endovascular oc-
clusion assist the surgeon? 5. What is the alternate therapy?
n. A 38-year-old male is seen in the emergency room
because of seizures involving the left face and arm. The
seizures have been occurring for about 3 mo but were now
followed by a left hemiparesis. A noncontrasting MRI shows
an isodense mass in the right sylvian fissure, which is quite
vascular. After injection of contrast, the tumor takes on a
high signal. It includes not only the temporal fossa but also
extends into the calvarian. Angiography reveals blood sup-
ply from the branches of the right middle cerebral artery and
the temporal branch of the external carotid. •
1. What is the most likely diagnosis? 2. What is the defini-
tive therapy? 3. How can the feeding vessels be best identi-
fied? 4. How can the feeding vessels be occluded? 5. What
substances might be used to occlude the feeding vessels?
IB. A 22-year-old male sustains a closed head injury with
loss of consciousness for about 30 min. When he recovers he
notes a "buzzing" in the left ear, and there is swelling of the
left eye, which persists. There is infection of the conjunctiva
on the left.
1. What is the most likely diagnosis? 2. How can the
lesion be outlined? 3, What forms of treatment have been
used? 4. What interventional consideration might be consid-
ered? 5. Using current techniques, what are the chances for
occluding the fistula leaving the carotid artery patent?
IV. A hydrocephalic male infant is found to have an aneur-
ysmal mass above the quadrigeminal plate. The mass is fed
by branches of the posterior choroidal artery and branches of
the ipsilateral pericollosal artery.
1. What is the lesion? 2. What is the most likely cause of
the hydrocephalus? 3. What forms of therapy might be
considered (a) for the hydrocephalus and (b) for the malfor-
mation? 4. Where are the most common complications of a
vein of Galen aneurysm? 5. How might these be prevented?
V. A 26-year-old female develops a left foot drop at the time
of an acute episode of back pain. An MRI suggests a spinal
AVM with a nidus located posteriorly behind the twelfth
thoracic vertebra. The lesion is fed by a radicular branch
located between Til and T12 on the right.
1. What are the alternative forms of treatment? 2. How
might the lesion be embolized (technically)? 3. What materi-
als might be considered for embolization? 4. When should
this patient be treated? 5. Where is the artery of Adamkie-
wicz most likely located?
Wyszukiwarka
Podobne podstrony:
więcej podobnych podstron