
The next two articles in this series are on the
visual pathways – this first article relates to
examination of the optic disc and diseases
affecting the optic nerve. The next article will
discuss diseases affecting the optic chiasm, optic
tracts and radiations and the visual cortex.
The anterior visual pathway
Difficulties in diagnosis of diseases of the
anterior visual pathway lie in two areas: firstly,
while it may be relatively easy to recognise an
optic disc appearance as abnormal, it may be
difficult to decide whether that appearance
reflects disease or is simply a variation of
normality.
Secondly, diseases of the anterior visual
pathways may be missed because of failure to
consider whether there is evidence of abnormal
optic nerve function. In the early stages of optic
neuropathy, the optic disc may appear to be
normal and the visual acuity near normal, lulling
the practitioner into a false sense of security.
This article attempts to help practitioners
decide in practical terms whether a disc
appearance is normal or abnormal, and how
to decide if there is any evidence of optic nerve
disease.
It will also discuss some of the more
common disorders encountered in
neuro-ophthalmology with emphasis on
recognition of significant signs of each which
point towards diagnosis.
When looking at a suspicious disc, or
considering the possibility of anterior visual
pathway disease, it pays to ask yourself four
questions, which are detailed in Table 1.
Table 1
Questions to ask when faced with a
suspicious disc
1) Is this disc normal or abnormal?
2) Does the history give me a
clue?
3) Is there any evidence of optic
nerve dysfunction?
4) Do I need to be worried?
Disorders of the visual pathway:
from the optic disc to the visual cortex
Diagnosis of neuro-ophthalmological disorders has been transformed over the last 20 years with the advent of
CT (computed tomography) and MRI (magnetic resonance imaging) scanning to examine the brain and optic
nerves. However, before these examinations are performed, someone has to detect an abnormality of
appearance of the optic disc or reduced function of the afferent visual system to warrant expensive and
in the case of CT scan x-ray radiation potentially harmful investigations. Patients will often first present to their
optometrist with vague complaints, and their practitioner must make the decision whether or not to refer.
July 28, 2000 OT
Chris Hammond MRCP, FRCOphth, Consultant in Ophthalmology, Farnborough Hospital, Bromley
www.optometry.co.uk
Disc: normal or abnormal?
The first thing to say when looking at a disc and
trying to decide, for example, whether it is
swollen or not, is that is not always easy to tell,
even experienced neuro-ophthalmologists have
difficulty sometimes. They may be able to resort
to other investigations such as fluorescein
angiography, so if you are unable to decide,
referral is obviously the next step.
Most significant abnormalities have some
evidence of optic nerve damage, however slight,
or visual field changes, if examined carefully.
Many abnormal-looking discs with normal function
are congenital abnormalities, so any evidence of
an acquired change in the disc compared to
previous records must be treated with suspicion.
Experience of close examination of normal
discs make abnormal discs easier to recognise.
Optic discs have a rather limited repertoire;
therefore when examining a disc, you should ask
yourself whether there is swelling (papillitis,
papilloedema), pallor (optic atrophy) or new
vessels (diabetes). While indirect binocular
biomicroscopy using the slit-lamp will allow
three-dimensional examination of the disc, the
direct ophthalmoscope is still useful as it provides
better magnification to look for subtle signs such
as spontaneous venous pulsation.
Is the history helpful?
Consideration of previous medical and ophthalmic
history is obviously useful, as it may give a clue
as to the causes of visual pathway disease. Changes
may be secondary, such as optic atrophy after a
longstanding retinal detachment or secondary to
retinitis pigmentosa, or dragging of vessels after
significant retinopathy of prematurity. However,
although previous history will often be important,
do not allow it to explain all new symptoms.
We recently treated a patient with a history
of residual esotropia and amblyopia from
childhood who presented with a worsening
esotropia. Although she was initially reassured by
her optometrist, it was only when she developed
ipsilateral deafness and facial nerve palsy that her
acoustic neuroma was diagnosed – the worsening
esotropia was in fact a new sixth nerve palsy.
A careful history is vital when concerned
about anterior visual pathway disease. Many
patients present to their optometrists with
headaches (“Is it due to my eyes?”) and the
The College of Optometrists has
awarded this article 2 CET credits.
There are 12 MCQs with a
pass mark of 60%.
The College of
Optometrists
ABDO has awarded
this article
2 CET credits (LV).
✓
sponsored by
practitioner must decide, especially if he or she is
unsure about the presence of swollen discs,
whether the symptoms indicate benign headaches
(e.g. tension-type) or those of raised intracranial
pressure. The latter headaches are worse in the
morning on waking or at night because of the
increase in CSF pressure when lying flat (they
may also be worse when bending over or
straining), and are often associated with nausea
and/or vomiting.
Tension-type headaches are intermittent,
come on often later in the day and are absent on
waking, and are often described as a frontal or
retro-orbital band of tightness (see CPD module 2
part 5 OT 5/05/00 for a full review of the
differential diagnosis of headaches).
Other questions to raise when considering
anterior visual pathway disease include questions
about hypopituitarism associated with chiasmal
compression (loss of secondary sexual
characteristics and impotence in men and
amenorrhoea (absent periods) in women) or
previous transient neurological symptoms such as
paraesthesiae or weakness in multiple sclerosis.
Is there an optic neuropathy?
An important component of the examination is to
look for any evidence of abnormal optic nerve
function – in early stages of disease, the visual
acuity may be only slightly decreased. Therefore,
it is important to look for reduced colour vision,
either using colour test plates or in unilateral
disease it is easy to test for subjective loss of
colour vision (“Look at this red pen top with
each eye – is there any difference between the
two eyes?”). There will be a relative afferent
pupil defect in unilateral or asymmetric bilateral
optic neuropathy, and practitioners must be able
to detect this important sign.
Visual field loss is universal with anterior
visual pathway disease, and again an ability to
perform confrontational visual fields is extremely
useful, as well as use of automated perimetry.
Field defects described include the central
scotoma of an optic neuropathy as well as the
centrocaecal scotoma (extending to include the
blind spot) seen in a toxic or heredofamilial optic
neuropathy (these may be impossible to separate
clinically). The enlarged blind spot of a swollen
optic disc (and this is often the only field
abnormality with papilloedema) may not be
28
www.optometry.co.uk
29
even down to no perception of light. This is
followed by a gradual resolution, which lasts
weeks to months. Signs to look for include loss
of colour vision, a relative afferent pupillary
defect and a central scotoma on visual field
testing.
The disc usually appears to be normal,
although there may be a papillitis, particularly
in children in whom the condition is often
bilateral and associated with viral infection.
This has a better prognosis. Rarely, Leber’s
neuroretinitis is seen after an attack of optic
neuritis: exudates involving the macula can be
seen.
The cause of optic neuritis is demyelination
and optic neuritis is the presenting feature of
multiple sclerosis (MS) in up to 25-50% of
patients with this disease. The risk of MS long-
term is up to 70% in those who have had an
attack of optic neuritis. Around 75-80% of MS
patients may develop optic neuritis (or evidence
of a previous attack) during the course of the
disease. Therefore, optic neuritis is strongly
associated with MS and even one attack may be
a forme fruste of MS. However, there are other
causes: post-viral (particularly in children),
granulomatous infiltration (such as sarcoidosis)
or associated with adjacent sinus infection.
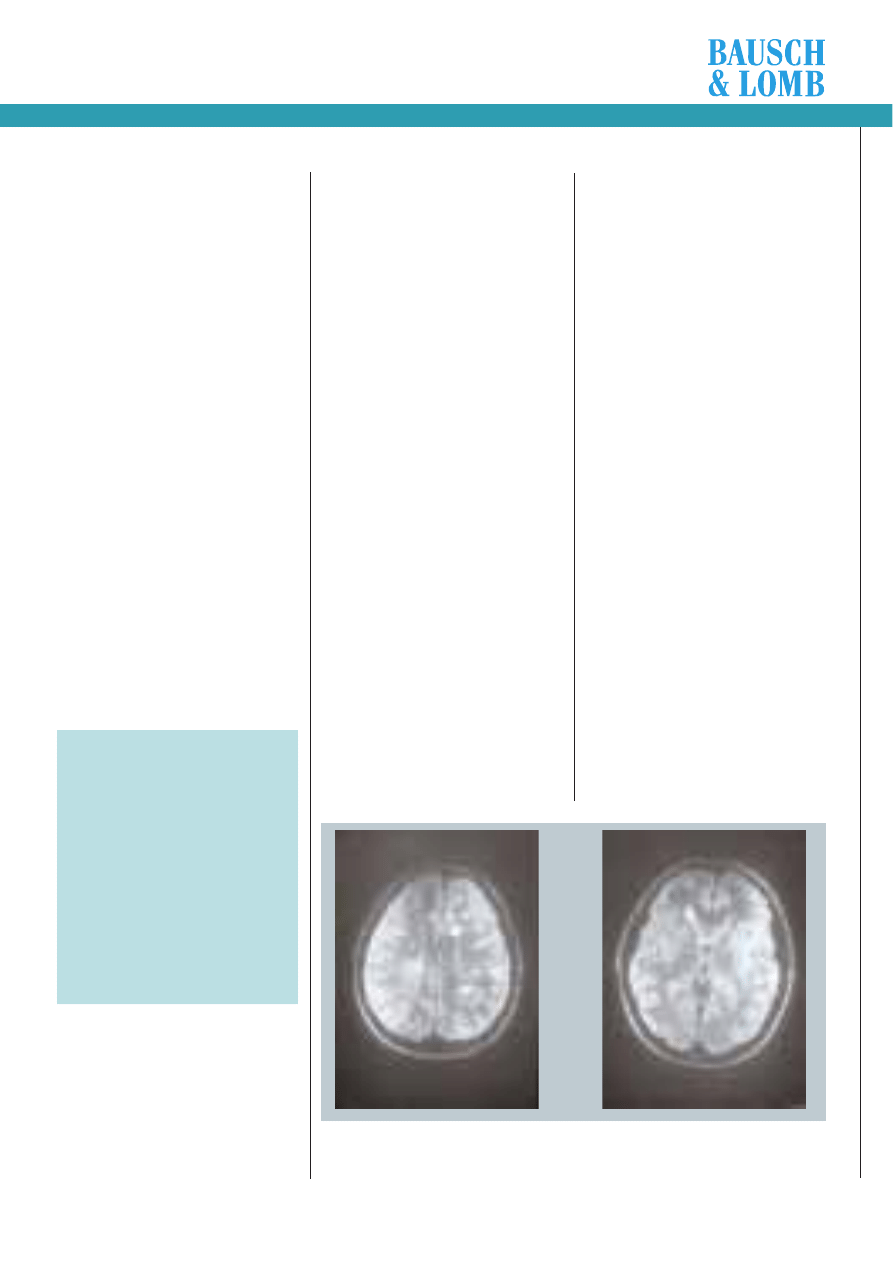
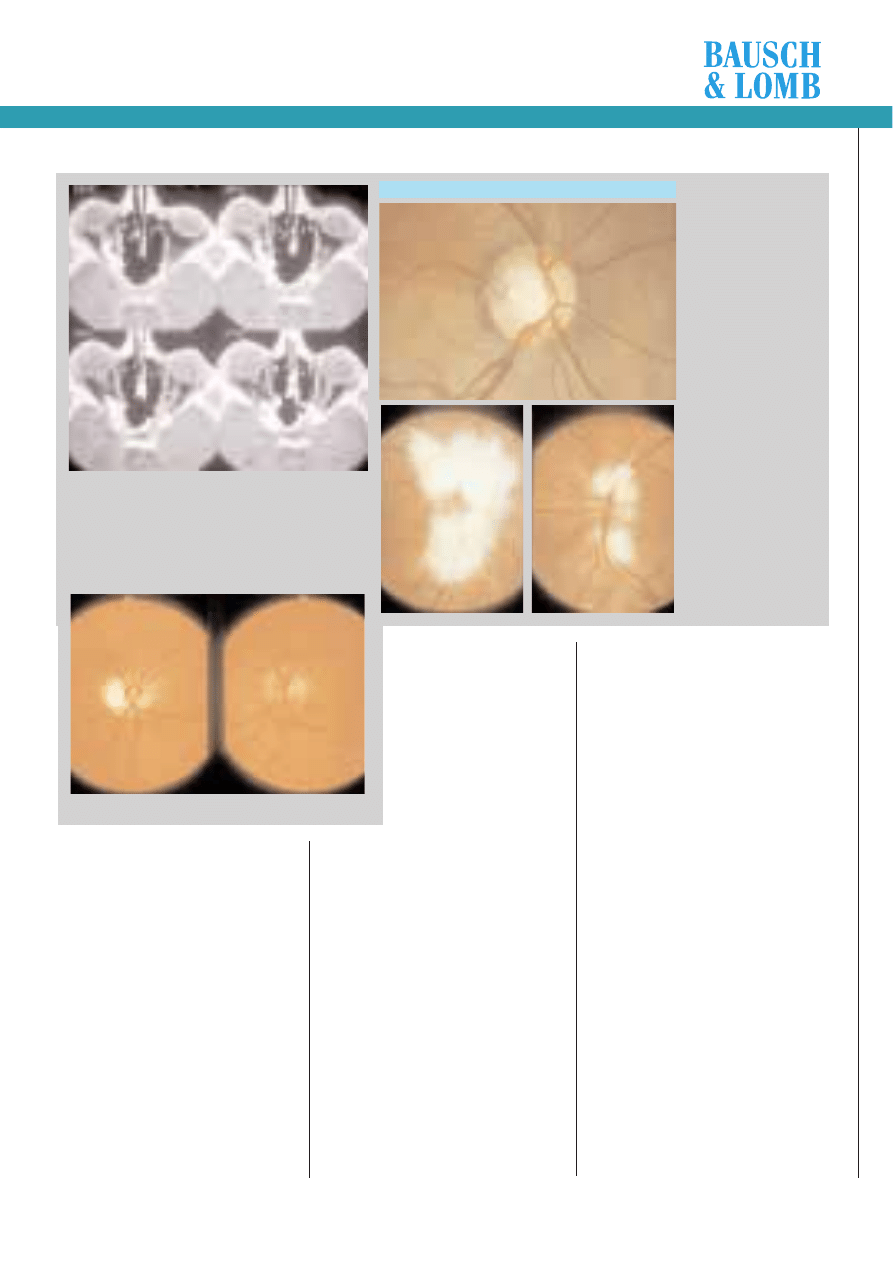
Investigations are not always needed in
classic optic neuritis. Identification of patients
who are more likely to develop MS is possible
with MRI scanning. This may show white lesions
in the periventricular grey matter (Figure 1).
The dilemma is then what to tell the
patient. We cannot predict when the next
attack of demyelination will occur (if ever),
have no preventive treatment, and patients
imagine, with the diagnosis of possible MS, the
worst scenario, while in fact there is a spectrum
of disease from very mild to fatal. Therefore,
the current practice is not to discuss the
possibility of MS in a patient with optic neuritis
unless they ask or if they have had previous
neurological episodes making MS very likely.
Electrodiagnostic tests show delayed Visual
Evoked Potentials which can be useful if the
diagnosis is in doubt.
A large multicentre optic neuritis treatment
trial reported no difference in visual outcome in
those treated with oral or intravenous steroids
or placebo, although steroids speed up recovery
a little. They did initially report that
intravenous steroid (methylprednisolone)
reduced the risk of subsequent MS, although
further follow-up has shown that the long-term
risks were the same for all groups.
We await newer treatments, such as the
controversial beta interferon. This has been
shown to reduce the number of relapses in a
specific sub-group of patients with regularly
relapsing/remitting disease. Its cost (£10,000
per patient per year) has led to a
recommendation from the National Institute of
Clinical Excellence (NICE) that it should not be
routinely prescribed.
Visual outcome is on the whole good -
many patients have near normal acuity,
although there are almost always subtle colour
vision defects (and delayed visual evoked
potentials). The final acuity does not reflect
the severity of loss of visual function, and so
too, the degree of optic disc atrophy does not
reflect final vision. In particular, children may
have a very pale optic disc but an extremely
good visual acuity.
.
Anterior ischaemic
optic neuropathy (AION)
Anterior ischaemic optic neuropathy is an
important diagnosis to consider, as it may herald
potentially blinding disease which needs urgent
treatment. There are two forms: the non-arteritic
form and the arteritic form. The latter is the
more serious, but the former is more common.
Figure 1 MRI scan
Two slices of the MRI scan of a 23-year-old patient with optic neuritis. The white lesions are typical of those
seen in the periventricular area in multiple sclerosis, and mean that this person is at high risk of developing
further neurological problems.
sponsored by
Module 2 Part 8
diagnosed by automated fields but comparison
with your own blind spot on confrontation fields
may detect it. Peripheral constriction and good
vision are observed in the optic atrophy seen
after papilloedema. An altitudinal field defect is
seen in retrolaminar vascular occlusion, such as
anterior ischaemic optic neuropathy (AION).
Do I need to be worried?
If the optic disc is swollen, then this may signify
raised intracranial pressure or a papillitis, both of
which may require investigation and treatment, so
urgent referral is indicated. It is important to
emphasise that visual function may be normal in
early papilloedema (apart from a slightly enlarged
blind spot which is not easy to diagnose), so this
should not put you off referral. By contrast, other
disc abnormalities with no optic neuropathy are
unlikely to be serious.
Optic atrophy does not occur overnight –
research involving transection (cutting) the optic
nerve acutely shows that optic atrophy is only
apparent four to six weeks later. Therefore a
patient presenting with pale optic discs is
unlikely to have a problem that has only just
occurred requiring immediate attention – the
problem has been brewing. However, a pale
swollen disc often does occur overnight. This
signifies an ischaemic optic neuropathy which has
been shown to be most likely to occur on waking,
possibly due to hypotension overnight
(papilloedema results in a pink swollen disc). In
this instance, the possible diagnosis of giant cell
arteritis must be considered, one of the few
neuro-ophthalmological emergencies.
First, I will discuss the acquired optic
neuropathies, which are summarised in Table 2.
Table 2 - Acquired optic neuropathies
Optic neuritis
■ Idiopathic/demyelination
■ post-viral
■ Granulomatous inflammation
■ Adjacent infection
Anterior ischaemic optic neuropathy
■ Non-arteritic
■ Arteritic
Diabetic papillopathy
Toxic optic neuropathies
Leber’s hereditary optic neuropathy
Papilloedema
Tumours
■ Glioma
■ Meningioma
Optic neuritis
Optic neuritis is one of the commonest forms of
optic neuropathy in the population, and
typically affects young women between the ages
of 20 to 40. They may present with pain on eye
movements or retro-orbital headache, which
often resolves over a week or so, associated
with monocular progressive visual loss.
The visual loss tends to worsen over a week
to ten days, and may be slight or profound,
o
t
July 28, 2000 OT
www.optometry.co.uk
30
Arteritic AION affects people aged 60 and
older, and women more than men. The reason
why it is such an important diagnosis to
consider is that visual loss if the condition is
not treated becomes bilateral rapidly – possibly
in 65% of people within three weeks.
Therefore, the diagnosis of arteritic AION
must be considered in any elderly patient
presenting with visual loss and a swollen disc,
or systemic symptoms, and requires urgent
hospital referral. The diagnosis is suggested by a
raised ESR (Erythrocyte Sedimentation Rate)
blood test, which demonstrates inflammation in
the arteries, and a temporal artery biopsy proves
the diagnosis (characteristic “giant cells” are
seen in the artery wall on microscopy).
This procedure is performed under local
anaesthetic. However, treatment is often
instituted before this, to try to control the
inflammation and prevent further visual loss.
Treatment consists of high dose oral steroids
(80mg prednisolone is often prescribed) which is
tailed off over a couple of years, according to
symptoms and blood tests. High doses of steroid
are not without complications in this group of
elderly patients, and include mood disturbances,
diabetes, hypertension and osteoporosis (bone
thinning).
Diabetic papillopathy
This is rare, and usually affects people with type
1 diabetes, often occurring in their second and
third decade. The patients present with a
swollen optic disc, which is bilateral in 75% of
cases, and often asymptomatic – there are no
symptoms of visual loss. The aetiology is
presumed to be vascular, and it does not seem
to be related to diabetic control. Diabetic
papillopathy usually resolves spontaneously with
good visual outcome, but obviously other causes
of swollen discs must be considered before
attributing it to diabetes.
Toxic optic neuropathy
This condition has been labelled with various
names such as toxic amblyopia and tobacco-
Non-arteritic AION
This typically affects men, aged from 50 to 70.
They present with a sudden, painless visual loss,
usually one-off, although a small proportion may
develop stepwise loss of vision. The actual extent
of the acuity and colour vision loss is variable.
Commonly, there is an altitudinal field defect, i.e.
the field loss is either the upper or the lower
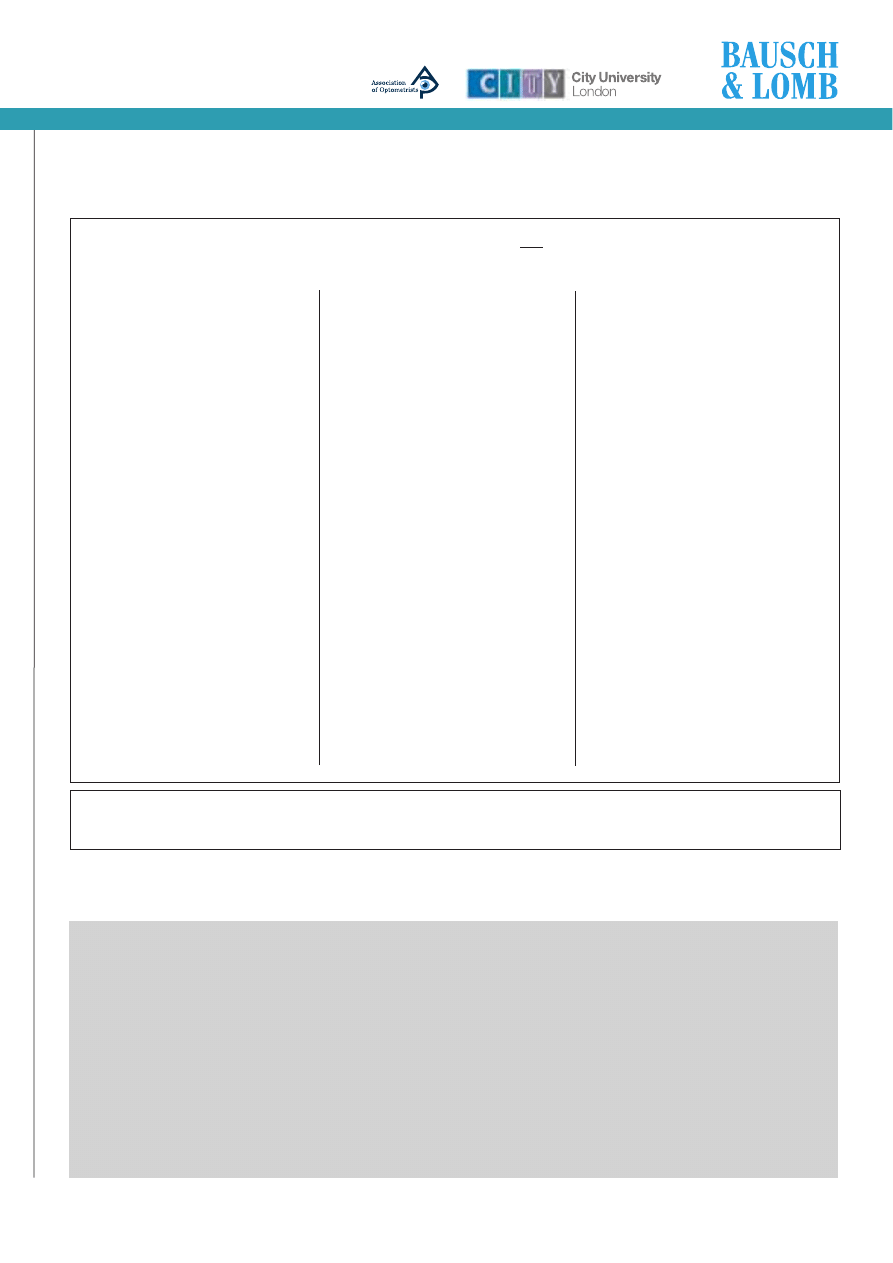
field. Acutely, sectoral infarction of disc is seen:
the optic disc appears swollen and pale,
especially in the area that has infarcted (Figure
2 a,b).
Subsequently, the disc is atrophic. We now
recognise that people susceptible to AION have a
“disc at risk” – a small hypermetropic-looking
disc. This has led to a belief that these discs are
at risk because of an anatomical predisposition
to infarction of the short posterior ciliary
arteries.
A general medical referral is appropriate in
patients with non-arteritic AION because some
series report up to 40% of patients with
hypertension, and 20% diabetes. There is no
known treatment to limit the amount of visual
loss and to prevent future loss of vision in the
fellow eye, which seems to have up to a 40% risk
of visual loss, occurring months or even years
later. Some authors have suggested that aspirin
might have a role.
Arteritic AION
This disease associated with giant cell arteritis
results in the same optic disc appearance, that of
acute infarction, so the disc is swollen and pale.
There may be associated nerve fibre layer
haemorrhages or even choroidal infarcts.
However, the visual loss tends to be more severe.
In addition to the visual loss, there are usually
systemic features of headache (often severe and
associated with scalp tenderness), malaise,
fever, weight loss and jaw claudication. This
causes pain in the jaw during chewing or
talking such that the person has to stop
chewing until the pain subsides – the jaw
muscles are ischaemic, as the artery is critically
narrowed.
alcohol amblyopia. The latter name gives a clue
as to the patients who present with this
problem: they are often heavy drinkers and
smokers with poor nutrition. Always consider
this diagnosis in people who neglect themselves
who present with unexplained visual loss.
Various agents may cause a toxic optic
neuropathy, including thiamine deficiency
(vitamin B1), vitamin B12 deficiency (seen in
bowel absorption problems), drugs (e.g.
ethambutol and isoniazid used in the treatment
of tuberculosis), and ingestion of methanol and
ethylene glycol (antifreeze).
The patients present with a centro-caecal
scotoma and progressive loss of vision.
Smoking cigarettes exposes an individual to
cyanides which may play a role in this disease –
another reason (if one were needed!) not to
smoke.
Some of the effects may be reversible,
particularly in that related to ethambutol
ingestion for TB treatment (these patients are
usually warned about visual loss, but anyone
presenting requires urgent referral).
For the other forms of toxic neuropathy,
referral is not as urgent: vitamin replacement is
attempted using thiamine infusions or vitamin
B12 injections, often without much success.
LeberÕs hereditary
optic neuropathy
This is an interesting, but rare, cause of optic
neuropathy. It is inherited through
mitochondrial mutations, which means that the
inheritance is through the maternal side.
It affects men far more than women (9:1)
and the peak incidence is in the teens. There is
a rapid onset of unilateral loss of central vision,
followed by the other eye within a year, often
in the context of a family history.
Examination acutely shows pseudo-disc
oedema (the disc looks swollen, but does not
leak on fluorescein angiography) and
circumpapillary telangiectasia (web-like dilated
blood vessels). Visual loss is variable but often
severe.
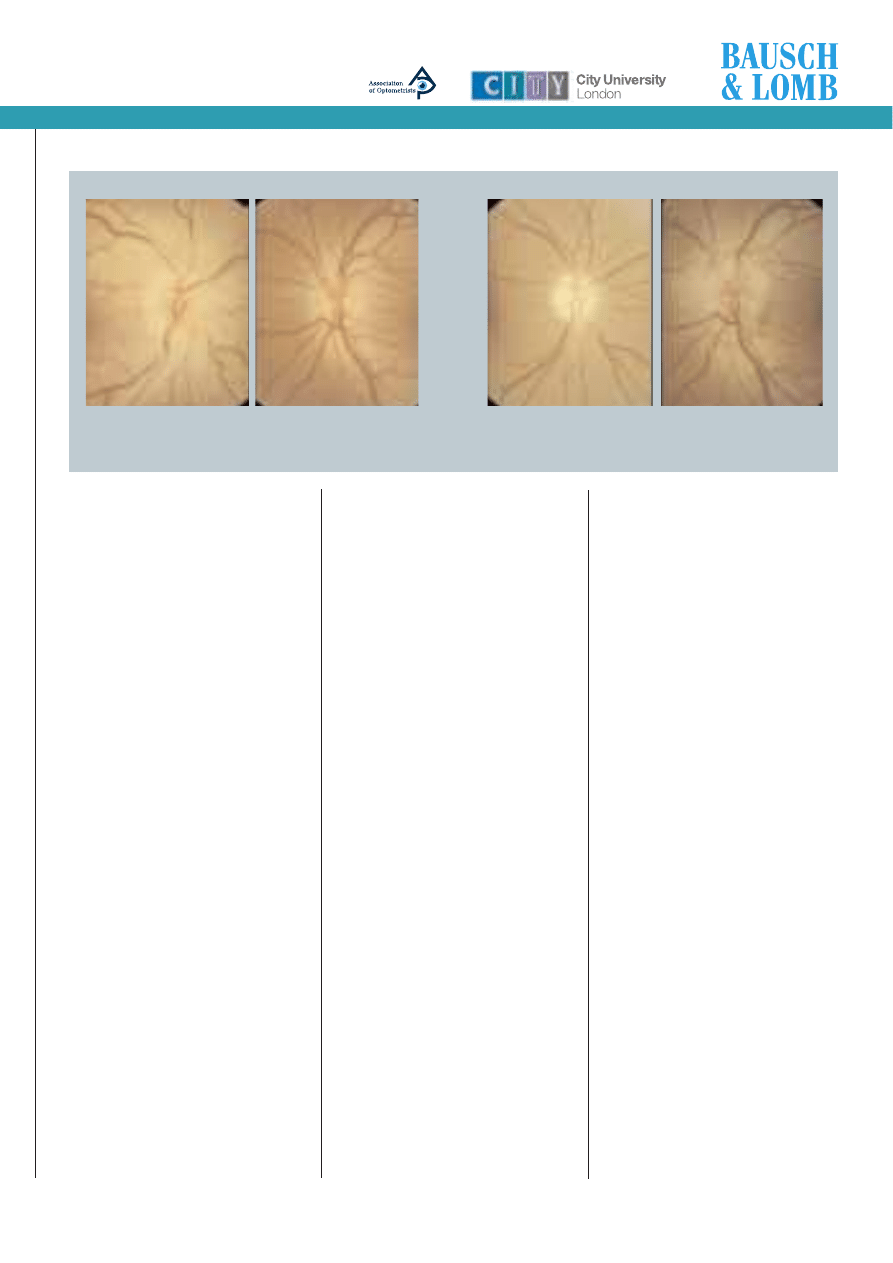
Figure 2 Anterior Ischaemic Optic Neuropathy
Figure 2a shows the discs of a 48 year-old man with AION affecting his
right eye, with a classic pale swollen disc associated with a nerve fibre layer
haemorrhage, and the small “disc at risk” can also be noted in the left.
Figure 2b shows the same patient’s discs photographed 9 months later: he
has optic atrophy in the right disc but has unfortunately presented with
vision loss in his left eye and has AION affecting this eye now.
sponsored by
www.optometry.co.uk
31
Module 2 Part 8
sponsored by
Papilloedema
Papilloedema is defined as swollen optic discs
due to raised intracranial pressure, and it is
very important to recognise the signs. If
papilloedema is detected, emergency referral is
required. Many patients will present with
headache, and it is important to be able to
exclude swollen discs. The history will often
help, as detailed above, and sometimes
patients may complain of obscurations, sudden
blanking of the vision lasting seconds, often
with postural changes or the valsalva
manoeuvre (which increases intracranial
pressure).
The practitioner must try to differentiate
papilloedema from pseudopapilloedema, the
causes of which are discussed below.
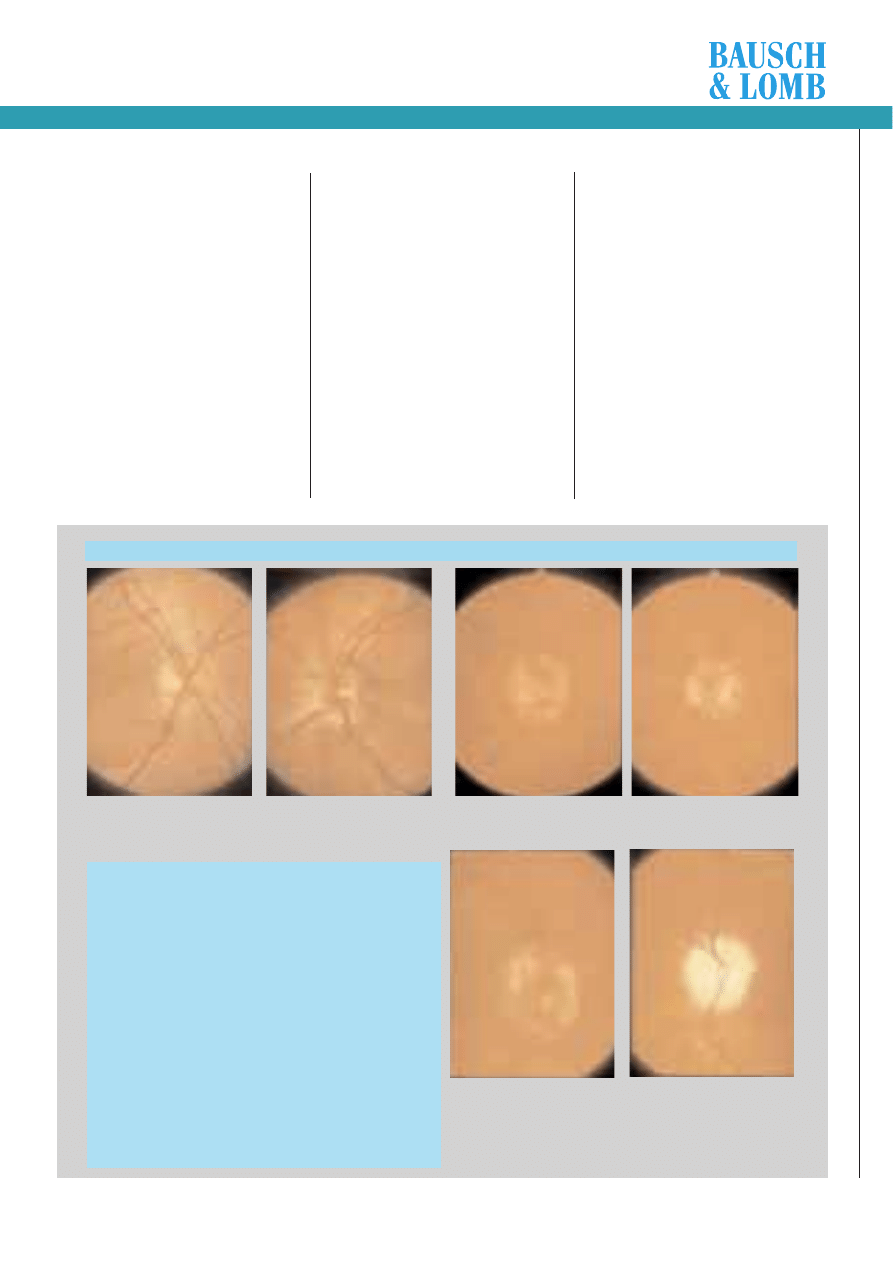
Papilloedema has been divided into early,
acute, chronic and vintage stages – the latter
stages are usually extremely obvious, but it is
the early changes that may be difficult to
detect (Figure 3 a,b,c). Remember that
children can also present with papilloedema, so
attempt to examine their discs when they
present with headaches.
The signs of papilloedema can be divided
into mechanical and vascular, and they are
detailed in Table 3. The early signs are the
important ones: blurring of the optic disc
margins as nerve axons swell, hyperaemia of
the disc and loss of spontaneous venous
pulsation. This is an important sign, as when
spontaneous venous pulsation is present, raised
intracranial pressure is extremely unlikely. The
best way of observing this is with the direct
ophthalmoscope, and to look at a vein just as
it leaves the disc margin. In 80% of normal
subjects, the veins can be seen to pulsate.
Although it is not present in 20% of normals, it
can sometimes be induced by gentle pressure
on the side of the globe.
The two main causes of pseudo-papilloedema
are hypermetropic discs, which are small and
crowded and therefore may appear swollen with
an absent optic cup, or myopic tilted discs which
appear swollen superonasally (Figure 4 a,b).
Obviously hypermetropes can get papilloedema,
so in these patients where spontaneous venous
pulsation is absent and there is a suggestive
history, referral may be required. The other main
diagnostic confusion is with buried disc drusen,
which are discussed later. These are commonly
associated with abnormal retinal vasculature, in
particular trifurcation of retinal vessels at the
disc, so look at the vascular pattern when
querying the diagnosis of papilloedema. Finally,
papilloedema is often associated with secondary
vascular changes as detailed in Table 3.
Table 4 details a systematic approach to
whether papilloedema is present or not.
Once a diagnosis of papilloedema has been
made, particularly with symptoms in keeping
with the diagnosis (headache and obscurations),
and visual field analysis showing an enlarged
blind spot, other neurological signs can be
looked for. These include a sixth nerve palsy (‘a
Figure 3a shows blurring of the nasal optic disc margin and a hyperaemic
disc, and it would be important to look for lack of spontaneous venous
pulsation to confirm the suspicious appearance.
Table 3 Signs of Papilloedema
Mechanical
■ elevation of optic nerve head
■ Blurring of optic disc margins
■ Filling in of physiological cup
■ Oedema of peripapillary nerve fibre layer
■ Retinal and/or choroidal folds
■ Vintage: early pallor and white refractile bodies on disc surface
Vascular
■ hyperaemia of the disc
■ Loss of spontaneous venous pulsation
(20% of normals)
■ Anomalous vessels not present
■ Peripapillary haemorrhages (flame haemorrhages)
■ Exudates in the disc or peripapillary area
■ Nerve fibre layer infarcts (cotton wool spots)
Figure 3b shows established papilloedema with elevated nerve head and
loss of the optic disc cup.
Figure 3c shows vintage papilloedema in the right disc with some
refractile white crystals on the surface, and the left disc is already
atrophic due to chronic papilloedema – this eye has already lost
significant vision in a 24-year-old patient with idiopathic intracranial
hypertension.
These three sets of optic disc photographs show early, established and chronic papilloedema.
o
t
June 30, 2000 OT
www.optometry.co.uk
32
pseudo-localising sign’ – the nerve is
stretched by the raised intracranial
pressure) resulting in diplopia. Again, it
is important to note that visual function
in papilloedema is often normal, and
visual field constriction only occurs in the
late stages.
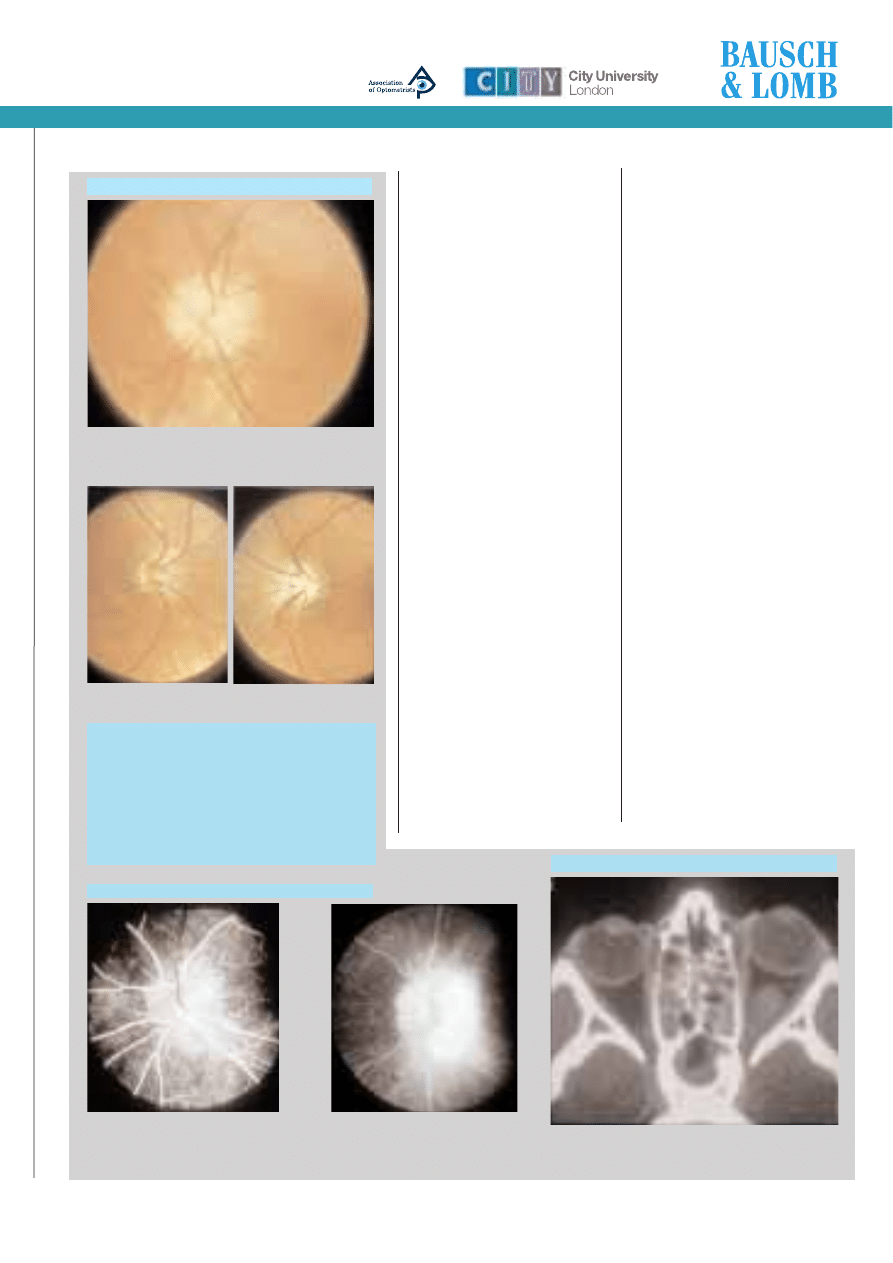
If there is doubt about the presence
of swollen discs, fluorescein angiography
is helpful (Figure 5 a,b). The early
angiogram shows a dilated capillary
network over the disc, and the late
angiogram shows leakage of fluorescein
from the disc.
The causes of papilloedema include
intracranial mass lesions (brain tumours,
both benign and malignant),
hydrocephalus (blockage of the flow of
cerebrospinal fluid), meningitis and
idiopathic intracranial hypertension
(pseudotumor cerebri).
CT or MRI brain scanning will usually
point towards a diagnosis, and a lumbar
puncture is sometimes required, to
examine the cerebrospinal fluid.
Idiopathic intracranial
hypertension
(Benign intracranial hypertension)
Idiopathic intracranial hypertension (IIH)
was previously known as benign
intracranial hypertension, but it is not
benign as its main complication is
blindness. The American term for the
condition is pseudotumor cerebri. IIH
presents with headache and raised
intracranial pressure, but is not due to a
brain tumour.
The typical person affected is an
obese, young woman, with no other
neurological problems. Other associations
have been reported including
tetracyclines, steroid use/withdrawal, and
vitamin A, but the commonest is recent
Pseudopapilloedema
Figure 4a shows buried disc drusen. The disc looks swollen,
but note the irregular “lumpy” edge to the disc, the
anomalous retinal vessels and the yellowish appearance.
Figure 4b illustrates tilted small discs, which are sometimes
confused for swollen discs, especially the temporal edge.
Table 4.
Questions to ask when querying papilloedema
■ Is there a headache suggestive
of raised intracranial pressure?
■ What is the refraction of the eye?
■ Is there spontaneous venous pulsation?
■ Is there an anomalous retinal vascular pattern?
■ Are there other retinal vascular changes
(eg haemorrhages, exudates)?
Figure 5b shows the late photograph of
this disc with fluorescein leakage from
the optic disc.
Fluorescein angiogram of an optic disc with papilloedema
Figure 5a is the early arterial phase of the dye
transit and shows dilated capillaries over the
surface of the optic disc. The arteries are filled
with dye (white) and the veins still empty (black).
weight gain. The cause of the raised
intracranial pressure is unknown, but
probably involves reduced CSF drainage. A
venous sinus thrombosis can mimic IHH
and so a MRI scan is often performed to
exclude this condition. By definition,
patients suffering from IIH reveal normal
scans.
Treatment usually includes advice and
support about weight loss, which may
cure the raised intracranial pressure,
although this is often unsuccessful
because of the patients’ difficulty in
losing weight. Acetazolamide (Diamox)
reduces CSF production (as well as
aqueous secretion) and often improves
headache and pressure, but if there is
evidence of visual field constriction on
serial field measurements, shunting or
optic nerve sheath fenestration may be
required.
Shunting involves a neurosurgical
procedure to divert CSF from the lumbar
region into the peritoneum
(lumboperitoneal) or from the brain’s
ventricles into the peritoneum
(ventriculoperitoneal). An optic nerve
sheath fenestration involves slitting the
optic nerve sheath behind the globe to
create a window to allow CSF to leak, and
to also form a band of scar tissue to
protect the optic nerve head from further
damage.
Compressive
optic neuropathies
There are two main tumours which cause
visual loss by compressing the optic
nerve: the optic nerve glioma and the
optic nerve sheath meningioma
(Figure 6 a, b). 75% of gliomas present
with visual loss in first decade of life and
90% by the age of 20, so it is a disease
of young people, although there is a more
Compressive optic neuropathies
Figure 6a shows the CT scan of a child with a swelling of
the optic nerve which is an optic nerve glioma.
sponsored by
Congenital disc
anomalies
Congenital disc anomalies are
common, and are often confused
with papilloedema. They may also
give rise to visual field defects, or
be associated with central nervous
system defects and may cause
macular problems. The most
common anomaly that causes
confusion with papilloedema is
buried optic drusen.
Optic disc drusen
Optic disc drusen occur commonly, affecting
0.3% to 1% of the population. In this condition,
calcified hyaline-like material is deposited at the
optic nerve head for unknown reasons. It may be
inherited in an autosomal dominant fashion, and
is usually bilateral (75% of individuals). It is
usually asymptomatic, but may cause visual field
defects. The diagnosis is usually obvious when
the drusen have appeared on the surface of the
disc, and a characteristic white, lumpy
appearance is seen, but when they are buried
there may be considerable confusion.
The features of optic disc drusen include an
irregular disc margin, an absent optic cup, with
anomalous branching of retinal vessels on the
disc surface (often a trifurcation of the retinal
vessels at the disc (Figure 4a)). The disc
appears pink/yellow, not hyperaemic as in
papilloedema. In addition, as opposed to
papilloedema, the veins are not dilated or
obscured by the swollen nerve axons.
No treatment is needed, but if doubt exists
www.optometry.co.uk
Module 2 Part 8
sponsored by
aggressive variant which can affect older people.
The glioma may be associated with
neurofibromatosis, a disease causing neuromas
(benign nerve tumours) on many nerves
throughout the body. The disease follows a
benign course and cannot be removed without
severing the optic nerve, so the usual
management is conservative. Occasionally surgery
is performed for cosmetic reasons in a blind eye.
It may behave in a more aggressive way in
adults and require more aggressive treatment.
Optic nerve sheath meningiomata,
meanwhile, affect adults, typically middle-aged
women, and present with a ‘classic’ triad of
visual loss, optic atrophy, and optociliary shunts.
These are shunt vessels between the posterior
ciliary and retinal circulation on the disc. If the
meningioma is intra-orbital, the patient may
present with proptosis. Some of these tumours
are hormone-dependent, so treatment is directed
to this end, and radiotherapy may slow down
spread. Surgery is difficult, as the tumour can
rarely be removed.
Figure 7b displays
myelinated nerve fibres,
and are commonly
misdiagnosed as
exudates.
Figure 6b shows the CT scan of a patient with an optic nerve
sheath meningioma which can be seen on the different cuts
as the tortuous thickened and calcified nerve sheath of the
right optic nerve (seen on the left of the picture). The optic
discs of this patient are seen in Figure 6c; the left disc is
normal but the right disc displays the classic triad of signs of
optic atrophy, disc swelling and optociliary shunt vessels.
as to whether there are drusen present (or if
there is papilloedema), their presence can be
confirmed on ultrasound (a dense shadow will be
visible) or on CT scan (a white calcium deposit
at the nerve head will be visible). Fluorescein
angiography shows autofluorescence
(fluorescence before the dye is injected into a
vein) and no late leakage.
Other congenital anomalies
Tilted optic discs and the small discs associated
with hypermetropia may cause confusion with
papilloedema (Figure 4b).
The important thing is to consider the
questions raised in Table 4, to ask yourself
whether these discs are in fact swollen or not.
Other congenital anomalies seen include optic
disc pits (which may cause a serous elevation of
the macula with subretinal fluid – Figure 7a),
myelinated nerve fibres (Figure 7b), which are
often confused with exudates, and colobomas
both of the optic nerve head as well as larger
ones involving the inferior retina due to
incomplete closure of the optic cup in utero.
In conclusion, the important points to
remember when diagnosing anterior visual
pathway disease are firstly to consider the
diagnosis, secondly to be able to discriminate
between congenital abnormalities of the optic
disc and papilloedema, and thirdly to be able to
look for signs of an optic neuropathy and to
consider the possible causes of this so that the
relative urgency of referral can be established.
The next instalment will consider disorders of
the optic chiasm and further back along the
visual pathway up to the visual cortex.
Congenital disc abnormalities
Figure 7a is an example
of an optic disc pit (a
small pit on the temporal
edge of the disc) which
may result in visual loss
due to serous fluid
leaking underneath the
macula.Figure 7a is an
example of an optic disc
pit (a small pit on the
temporal edge of the
disc) which may result in
visual loss due to serous
fluid leaking underneath
the macula.
33
Figure 6c
o
t
July 28, 2000 OT
www.optometry.co.uk
sponsored by
1. Signs of an optic neuropathy may
include all of the following except:
a.
central scotoma
b.
slightly reduced visual acuity
c.
relative afferent pupil defect
d.
absent spontaneous venous pulsation
2. Adult patients with optic neuritis
usually present with which one of the
following?
a.
peripheral field constriction
b.
pain on eye movements/headache
c.
a swollen optic disc
d.
bilateral visual loss
3. Which one of the following is correct
regarding non-arteritic anterior
ischaemic optic neuropathy?
a.
It typically affects females
b.
It occurs in large myopic “discs at risk”
c.
It may produce an altitudinal field defect
d.
Visual loss is always confined to one eye
4. Which one of the following is correct
regarding diabetic papillopathy?
a.
It is common
b.
It generally affects people with Type II
diabetes
c.
Bilateral swelling of the optic disc occurs
in 75% of cases
d.
Patients will generally complain of
extensive visual loss
5. Causes of toxic optic atrophy include all
of the following except:
a.
Vitamin C deficiency
b.
Vitamin B12 deficiency
c.
Methanol
d.
Vitamin B1 deficiency
6. Which one of the following regarding
Leber’s hereditary optic neuropathy is
incorrect?
a. It affects males more than females
b.
The peak incidence of the condition
occurs in the teens
c.
At the initial stages, patients suffer a
bilateral loss of vision
d.
Inheritance is through the maternal side
7. Patients with early papilloedema
usually present with which one of the
following?
a.
a central scotoma
b.
enlarged blind spots
c.
a relative afferent pupillary defect
d.
severe loss of vision
8. Clinical signs of early papilloedema
include which one of the following?
a.
optociliary shunt vessels
b.
retinal and choroidal folds
c.
loss of spontaneous venous pulsation
d.
venous sheathing
Multiple choice questions -
Disorders of the visual pathway: from the optic disc to the visual cortex
9. Symptoms of raised intracranial
pressure may include all the following
except:
a.
obscurations
b.
nausea and vomiting
c.
diplopia
d.
ptosis
10. Optic nerve sheath meningioma:
a.
peaks in incidence in the second decade
of life
b.
may cause proptosis
c.
rarely causes visual loss
d.
is associated with Neurofibromatosis
11. Optic disc drusen affects
approximately what proportion of the
population?
a.
1%
b.
5%
c. 10%
d.
50%
12. Optic disc drusen are usually:
a.
unilateral
b.
the cause of reduced visual acuity
c.
associated with anomalous retinal
branching
d.
caused by myelinated nerve fibres
An answer return form is included in this issue.
It should be completed and returned to: CPD Initiatives (NOE8),
OT, Victoria House, 178Ð180 Fleet Road, Fleet, Hampshire, GU13 8DA by September 6.
About the author
Chris Hammond trained as a senior registrar at St Thomas’s Hospital and the National Hospital for Neurology.
He has recently been appointed Consultant at Farnborough Hospital, Bromley NHS Trust.
Please note there is only ONE correct answer
Correction
Due to a typographical error, in CPD module 2, part 6, OT 2/06/00 page 34 under ‘Aetiology of nerve lesions’, the separation between the two images
increases in the direction opposite the side of the palsy ”and with” head tilt towards the side of the palsy.
34
Wyszukiwarka
Podobne podstrony:
więcej podobnych podstron