Modifications of Eyebrow Position
With Botulinum Exotoxin A
Mimi S. Kokoska, MD; Jason B. Amato, MD; Christopher S. Hollenbeak, PhD; Dee Anna Glaser, MD
Objective:
To determine if clinically used botulinum
exotoxin A (Botox) injections to the forehead and gla-
bellar and crow’s-feet regions result in modifications of
eyebrow position.
Design:
Prospective study.
Setting:
Academic medical center in St Louis, Mo.
Subjects:
Twenty-nine adult patients treated with botu-
linum exotoxin A injections for rhytids.
Intervention:
The eyebrow position at 13 different sites
was measured before injection and 2 weeks after treat-
ment. The areas injected were based on patient prefer-
ence and physician assessment. Of the 29 patients, 14 re-
ceived injections into the glabella only and 15 received
injections into the glabella and forehead, with or with-
out treatment of the crow’s-feet.
Results:
In 29 patients at rest, we found no significant
(P value range, .17 to .97) change in eyebrow position,
except for a point depression at the right lateral eye-
brow. The 15 patients who received injections into the
forehead and glabella, with or without treatment of the
crow’s-feet, had no significant (P value range, .11 to .84)
change in eyebrow position, except for a point of depres-
sion at the left medial eyebrow. Both groups exhibited
eyebrow depression in the active state (eyebrow maxi-
mally elevated).
Conclusions:
Botulinum exotoxin A injections into the
forehead and glabellar, and crow’s-feet regions did not
significantly change the resting eyebrow position. How-
ever, forehead injections contributed to eyebrow depres-
sion in the active state.
Arch Facial Plast Surg. 2002;4:244-247
U
SE OF
botulinum exo-
toxin A (Botox; Allergan,
Inc, Irvine, Calif) has been
well described for the cos-
metic treatment of hyper-
functional facial rhytids.
1-3
For the upper
third of the face, the drug is commonly used
to paralyze muscles causing glabellar frown
lines, horizontal forehead furrows, and lat-
eral orbital crow’s-feet. Reversing the age-
associated ptosis of the eyebrow, tradition-
ally done using a surgical approach, gives
a youthful result that is cosmetically desir-
able. Other articles
4-6
that have examined the
effects of botulinum exotoxin A on eyebrow
position imply that it is possible to create a
chemical eyebrow-lift with selective use of
the medication. Some of the injections in
these previous studies were purposefully
placed to produce eyebrow elevation. In this
study,ourobjectivewastodetermineifmodi-
ficationsineyebrowpositionoccurwithclini-
cally used botulinum exotoxin A injections
for hyperfunctional facial rhytids of the fore-
head and glabellar, and crow’s-feet regions.
METHODS
Twenty-nine adult patients who presented to
Saint Louis University Hospital for botuli-
num exotoxin A injections into the upper third
of the face were enrolled into our study, and
informed consent was obtained. There were 2
male and 27 female patients (age range, 28-73
years). Fourteen of these patients received
injections into the glabella only, and 15 re-
ceived injections into the glabella and the fore-
head, with or without injection into the crow’s-
feet region. Selection of treated areas was based
on patient preference, along with physician rec-
ommendations. Measurements were taken be-
fore injection and 2 weeks after injection.
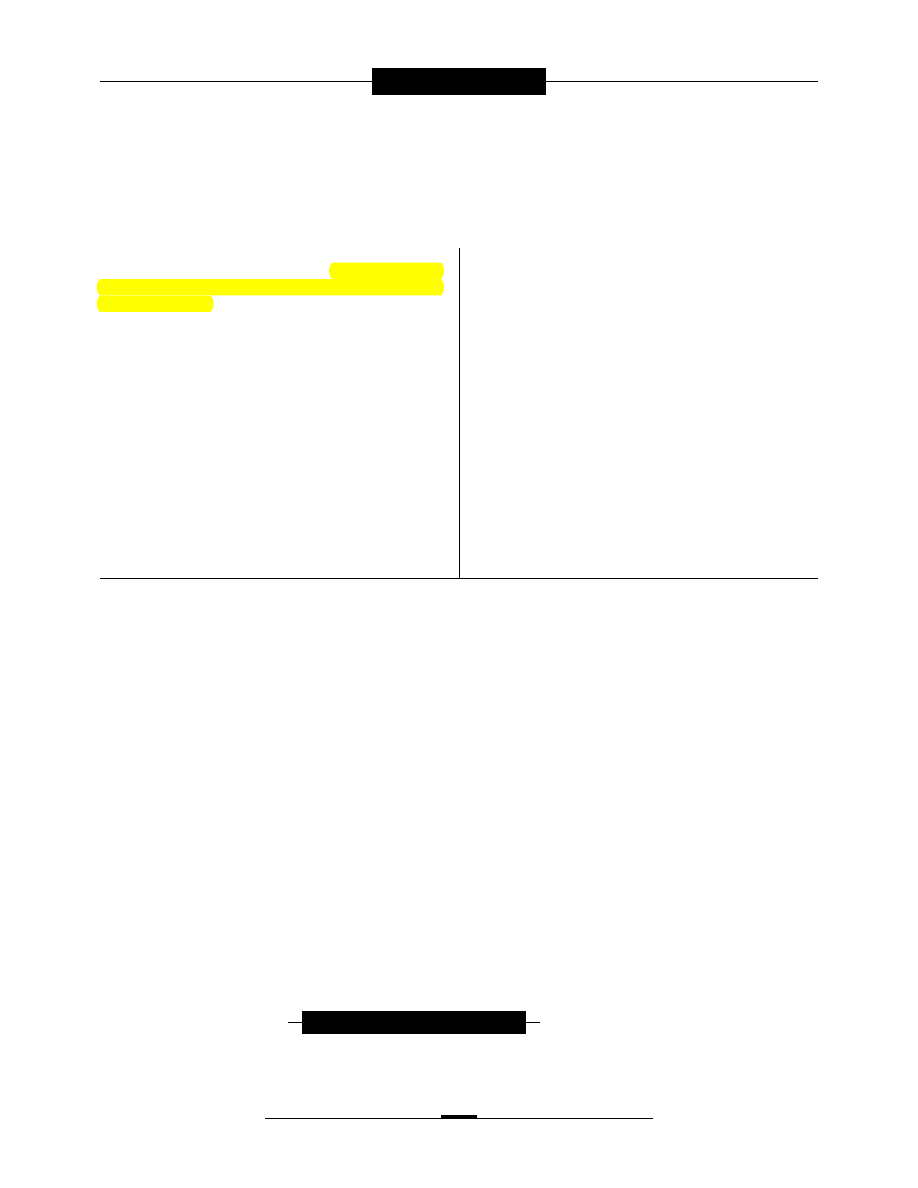
Thirteen measurements were taken with
the eyelids closed and the eyebrow relaxed, and
again in the active state, with the eyebrow maxi-
mally elevated (
Figure 1
). Vertical measure-
ments A, B, and C were taken from the upper
eyelid margin to the upper eyebrow margin at
the lateral canthus, the mid eyelid line, and the
medial canthus, respectively. Vertical measure-
ments D, E, and F were taken from the upper
eyebrow margin to the hairline at the lateral
canthus, the mid pupillary line, and the me-
dial canthus, respectively. The intereyebrow
distance was also measured. Subscripts R and
L denote the right and left sides of the face, re-
spectively.
Botulinum exotoxin A was prepared by di-
luting a 100-U vial with 2.0 mL of sterile pre-
servative-free isotonic sodium chloride solu-
tion for a final concentration of 5 U/0.1 mL. A
1.0-mL tuberculin syringe and a 30-gauge
needle were used for percutaneous injections
into the muscular layer.
ORIGINAL ARTICLE
From the Department of
Otolaryngology–Head and
Neck Surgery, Indiana
University School of Medicine,
Indianapolis (Dr Kokoska); the
Department of Dermatology,
Saint Louis University Health
Sciences Center, St Louis, Mo
(Drs Amato and Glaser); and
the Department of Surgery,
Graduate Health
Administration Program,
The Pennsylvania State
University–College of Medicine,
Hershey, Pa (Dr Hollenbeak).
(REPRINTED) ARCH FACIAL PLAST SURG/ VOL 4, OCT-DEC 2002
WWW.ARCHFACIAL.COM
244
©2002 American Medical Association. All rights reserved.
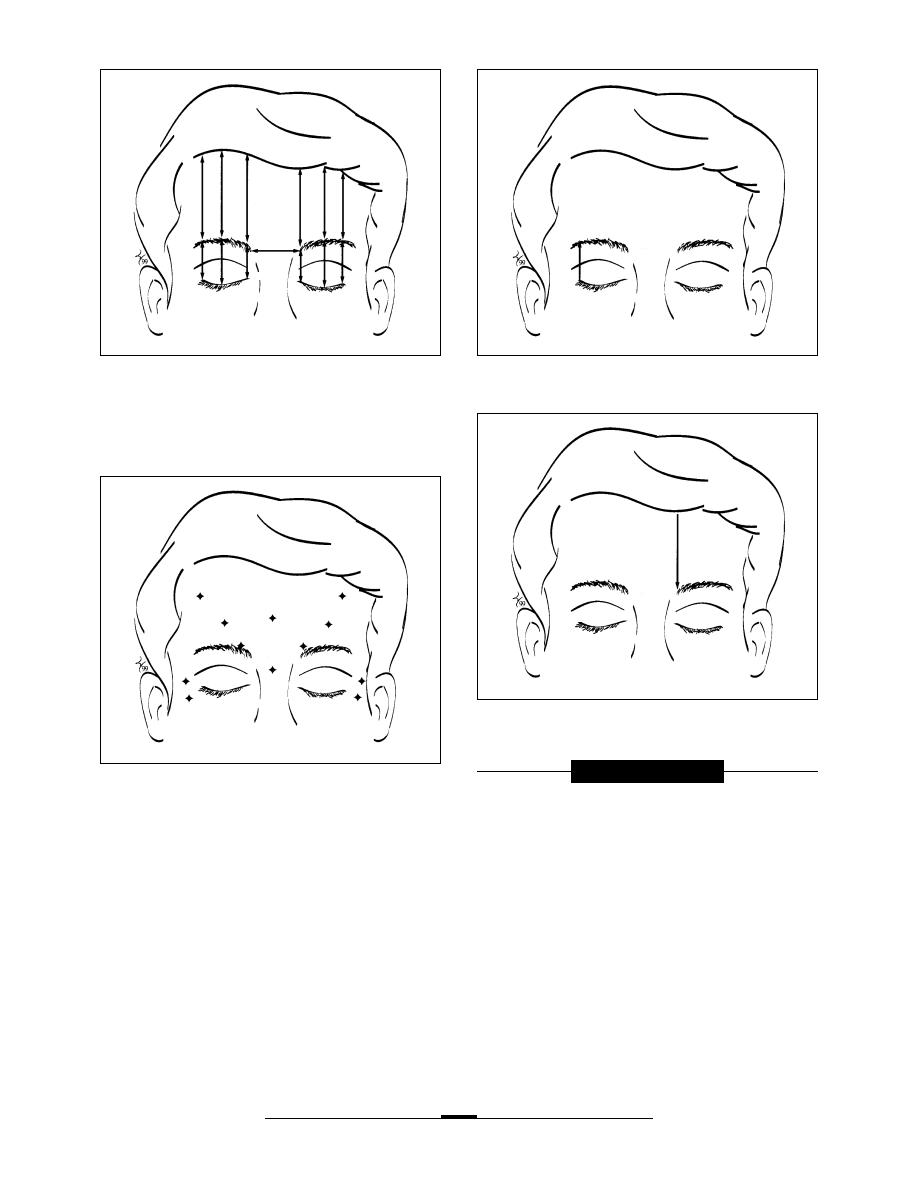
Botulinum exotoxin A injection doses and sites were se-
lected based on the typical injections used for treatment of the
upper third of the face in our practice (
Figure 2
). For treat-
ment of the forehead, 5 injection sites were used, with 4 U per
injection, for a total of 20 U. Three 5-U injections were used
to treat the glabella, for a total of 15 U. Each lateral orbital re-
gion was injected at 2 sites, with 4 U each, for a total of 16 U to
treat the bilateral crow’s-feet regions.
Statistical analyses were performed using SAS statistical soft-
ware, version 6.12 (SAS Institute Inc, Cary, NC). Observations
were paired measurements of the distance before and after treat-
ment with botulinum exotoxin A; therefore, we used a paired t
test in our statistical analysis.
7
Posttreatment measurements were
subtracted from pretreatment measurements, and the average dif-
ference was tested using a null hypothesis that the average dif-
ference was 0. We performed one statistical test for each of the
13 sites for the entire sample and for the subsample of 15 pa-
tients who received injections into the forehead and the glabella.
Results were considered significant if P
⬍.05.
RESULTS
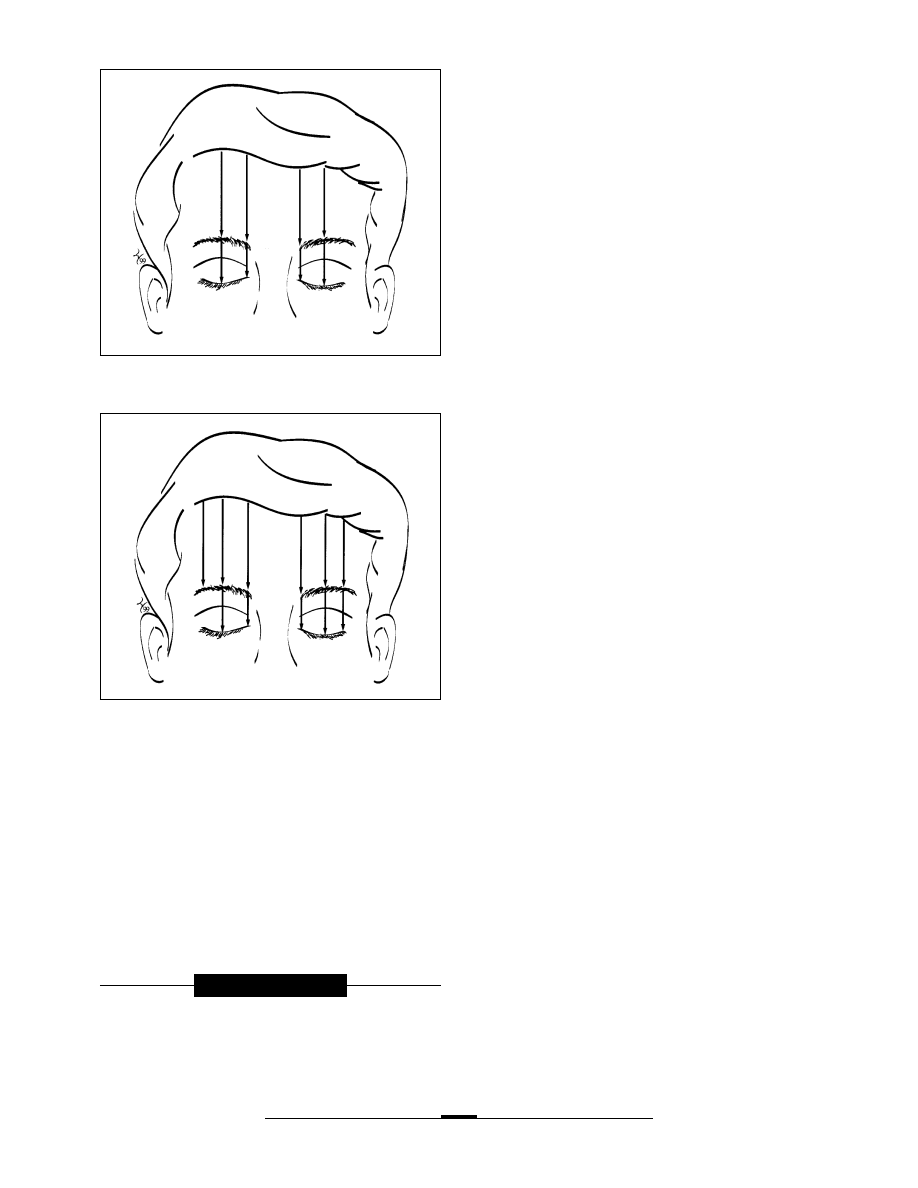
We first tested whether modifications in eyebrow posi-
tion could be detected for resting positions. In all 29 pa-
tients at rest, only the right lateral eyebrow elevation (po-
sition A
R
in Figure 1) was significant (mean, −1.34 mm;
P=.006) (
Figure 3
). There was no significant (P value
range, .17 to .97) change in intereyebrow or other eye-
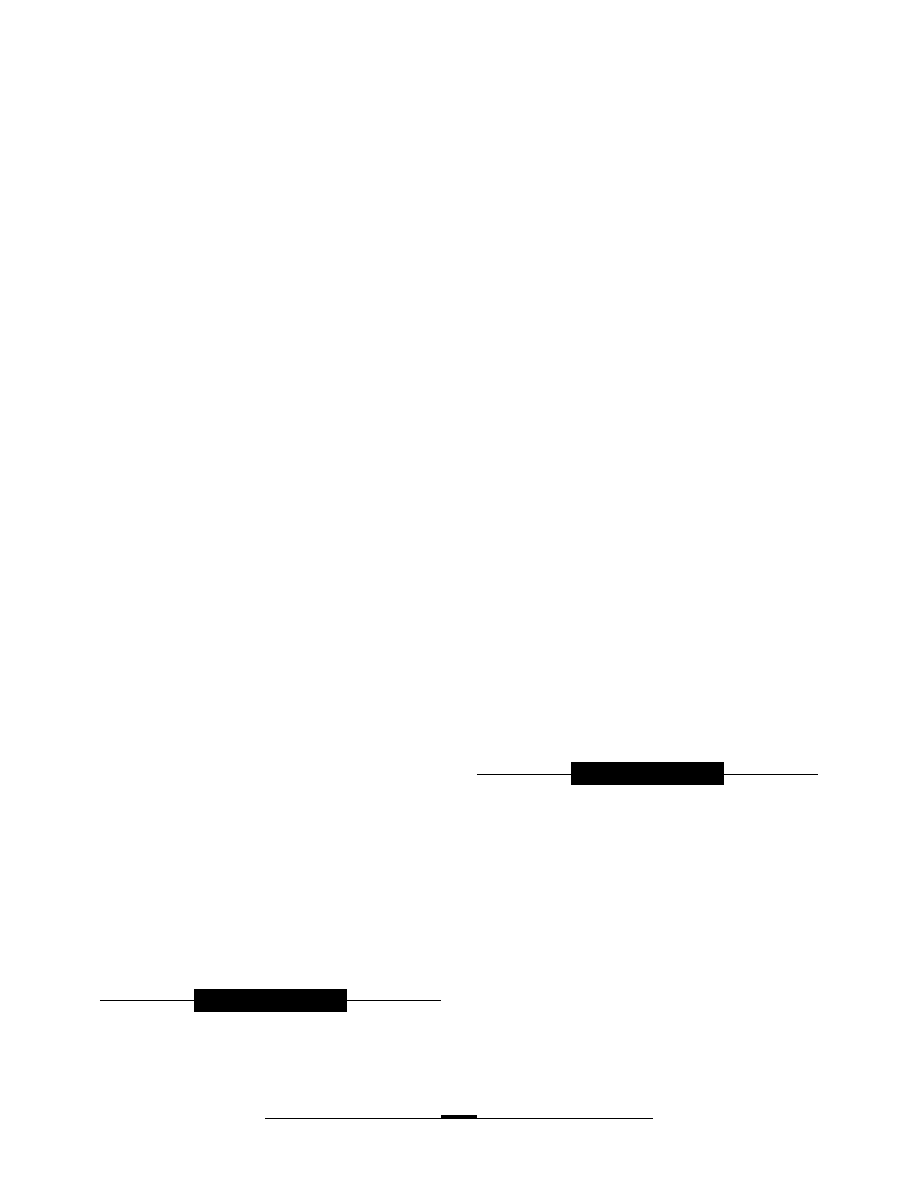
brow distances. In the subsample of 15 patients who re-
ceived injections into the forehead and glabella, with or with-
out treatment of the crow’s-feet, the left medial eyebrow
(position F
L
in Figure 1) was significantly depressed (mean,
−1.87 mm; P=.03) (
Figure 4
). No other significant (P value
range, .11 to .84) changes were found in other eyebrow po-
sitions or in the intereyebrow distance. A separate analy-
sis of the 14 patients who received glabellar injections with-
out forehead injections produced no significant (P value
range, .18 to .73) changes in eyebrow position.
We did find significant (P value range,
⬍.001 to .01)
changes in eyebrow position for the active state, with the
D
R
E
R
F
R
A
R
B
R
F
L
E
L
D
L
C
L
B
L
A
L
C
R
Figure 1. Measurements taken in the relaxed position and then with maximal
eyebrow elevation. Vertical measurements A, B, and C were taken from the
upper eyelid margin to the upper eyebrow margin at the lateral canthus, the
mid eyelid line, and the medial canthus, respectively. Vertical measurements
D, E, and F were taken from the upper eyebrow margin to the hairline at the
lateral canthus, the mid pupillary line, and the medial canthus, respectively.
Subscripts R and L denote the right and left sides of the face, respectively.
Figure 2. Standardized injection sites (diamonds).
Figure 3. All 29 patients at rest, showing no change except for a right lateral
eyebrow elevation (arrow).
Figure 4. The 15 patients who received injections into the forehead and
glabella had only a left medial eyebrow depression (arrow).
(REPRINTED) ARCH FACIAL PLAST SURG/ VOL 4, OCT-DEC 2002
WWW.ARCHFACIAL.COM
245
©2002 American Medical Association. All rights reserved.
eyebrow maximally elevated. For the 29 patients in the
active position, the medial two thirds of the eyebrow (po-
sitions B, C, E, and F in Figure 1) were depressed
(
Figure 5
). The numbers were bilaterally consistent, with
absolute means ranging from 1.93 to 7.86 and P values
ranging from .01 to
⬍.001. The subsample of 15 pa-
tients also had a depression of the entire eyebrow in the
active position at all sites shown in Figure 1, except site
A
R
(
Figure 6
). Again, the effects were bilaterally con-
sistent, with absolute means ranging from 2.93 to 11.53
mm (P value range,
⬍.001 to ⬍.01).
COMMENT
Functional facial rhytids result from tension of the under-
lying mimetic facial musculature on the overlying skin.
Botulinum exotoxin A acts as a peripheral neuromuscular
blockade and, thus, weakens the underlying muscles of fa-
cial expression, causing a flattening of the overlying skin.
This results in an improved cosmetic appearance.
8
The pri-
mary functional upper facial rhytids include the glabellar
frown lines, the horizontal forehead furrows, and the crow’s-
feet. The medial frontalis, the procerus, the corrugator su-
percilii, and the medial orbicularis oculi muscles contrib-
ute to the glabellar frown lines. Contraction of the frontalis
muscle causes the horizontal forehead furrows, and con-
traction of the lateral orbital portion of the orbicularis oculi
muscles results in the crow’s-feet rhytids.
9
Eyebrow position is determined by underlying skel-
etal shape, resting muscular tone, and overlying skin
tone. It is generally accepted that the eyebrow is elevated
by the frontalis muscle and depressed by the procerus,
the corrugator supercilii, and the orbicularis oculi
muscles.
1
In their retrospective study of 29 patients injected
with 20 U of botulinum exotoxin A into the procerus and
corrugator supercilii muscles, Frankel and Kamer
5
found
that 8 (32%) of 25 patients had an elevation of the me-
dial eyebrow, 12 (48%) of 25 patients had an elevation
at the mid pupillary eyebrow, and 17 (59%) of the 29 pa-
tients had an increase in intereyebrow distance with mea-
surements from standardized photographs. A subjec-
tive comparison of the photographs by blinded observers
found that 18 (62%) of the 29 patients have a higher me-
dial eyebrow. Although this is not stated in their article,
further interpretation of their results suggests that 17
(68%) of their 25 patients had either a depression or no
change in medial eyebrow position, 13 (52%) of the 25
patients had either a depression or no change in mid pu-
pillary eyebrow position, and 12 (41%) of the 29 pa-
tients had either a depression or no change in intereye-
brow distance. Huilgol et al
4
reported that 5 of 7 women
showed an eyebrow elevation of 1 to 3 mm with selec-
tive botulinum exotoxin A treatment of the eyebrow de-
pressors. They injected a total of 10 to 14 U into the gla-
bellar region and the supralateral eyebrow, and measured
from the mid pupillary line to the lowest portion of
the eyebrow to make this determination. One difference
from the present study is that the subjects in the study
by Huilgol et al received lateral eyebrow injections. No
statistical analysis was performed in either of these stud-
ies; therefore, the results should be interpreted with this
in mind.
Ahn et al
6
examined subjects with only injections
to the supralateral eyebrow. The purpose of the injec-
tions was to produce an eyebrow-lift, not to treat rhytids.
No injections were performed in the crow’s-feet area in-
ferior to the lateral canthus. There was significant lat-
eral and mid eyebrow elevation after supralateral eye-
brow injection. The injection sites differ significantly from
those in the present study; therefore, no direct compari-
sons can be made.
In our study, eyebrow position was assessed after
injections of botulinum exotoxin A for cosmetic treat-
ment of hyperfunctional facial rhytids on the upper third
of the face. The 29 patients at rest had no statistically sig-
nificant change in eyebrow position after injection, ex-
cept in the right lateral eyebrow measurement. These same
patients had a depression of the medial two thirds of the
eyebrow in the active position. This change can be ex-
plained by the toxin’s effect on the frontalis muscle, the
Figure 5. All 29 patients with maximal elevation, showing a depression of
the medial two thirds of the eyebrow (arrows).
Figure 6. The 15 patients who received injections into the forehead and
glabella in the active position had a depression of the entire eyebrow
(arrows), except at the right lateral eyebrow position.
(REPRINTED) ARCH FACIAL PLAST SURG/ VOL 4, OCT-DEC 2002
WWW.ARCHFACIAL.COM
246
©2002 American Medical Association. All rights reserved.
only eyebrow elevator. In patients who received injec-
tions into the forehead and the glabella, with or without
crow’s-feet injections, there was no significant change in
eyebrow position at rest, except for the left medial eye-
brow measurement. These patients also had a depres-
sion of the eyebrow in the active eyebrow-raising posi-
tion 2 weeks after injection, also explained by the
botulinum exotoxin A effect on the frontalis muscle.
These results can be correlated with facial anatomi-
cal features. The corrugator supercilii muscle is situated
in a horizontal or diagonal plane. The procerus is a ver-
tical muscle, and the orbicularis oculi is a circumferen-
tial muscle. These eyebrow depressors, however, are rela-
tively smaller in muscle mass than the frontalis muscle
and, therefore, in most patients, contribute less to eye-
brow elevation or depression than the frontalis muscle.
The frontalis muscle inserts into the skin of the eye-
brows and the nasal root.
10
Therefore, botulinum exo-
toxin A injections at the eyebrow level will likely affect
the most inferior portion of the frontalis muscle, in ad-
dition to the corrugator supercilii muscles. This relation-
ship may explain the lack of eyebrow elevation with in-
jections into the medial eyebrow area. The horizontal or
oblique orientation of the corrugator supercilii muscle
explains its dominant role in eyebrow medialization and
its more minor role as an eyebrow depressor, creating the
vertical wrinkles at the glabella. The 2 sites that showed
a statistically significant change at rest, the right lateral
eyebrow and the left medial eyebrow, may change with
a larger sample size.
We found that it was more difficult to measure from
the eyebrow to the hairline than from the eyebrow to the
closed eyelid margin. The exact margin of the hairline
was sometimes ambiguous and more difficult to repro-
duce at the 2-week follow-up. Despite this, the eyebrow-
to-hairline measurements were generally confirmatory
with respect to eyebrow position.
A subpopulation of subjects in this study (n=10) who
were classified as hypertonic (defined in the pretreat-
ment consultation as having clinically constant corru-
gator and/or frontalis muscle contraction) were not sig-
nificantly different from the general population. This may
be secondary to the small numbers in the subpopula-
tion in our study. Another possible explanation is that
the subjects were asked to purposefully relax the upper
third of their face for the resting measurements, which
may have reduced their baseline muscular hypertonic-
ity. Two of us (M.S.K. and D.A.G.) have clinically ob-
served subjects who are hypertonic who have more ex-
aggerated eyebrow position changes after botulinum
exotoxin A injections. In other words, some patients who
constantly raise their eyebrows, even at rest, have a dra-
matic depression in their resting eyebrow position after
botulinum exotoxin A injection into the frontalis muscle.
Further study of this subpopulation is warranted.
CONCLUSIONS
We present a prospective and statistically analyzed study
of botulinum exotoxin A–induced effects on eyebrow po-
sition. We found that glabellar, including procerus, cor-
rugator with or without depressor supercilii, and crow’s-
feet (lateral orbicularis oculi), injections did not
significantly change resting eyebrow positions. Fore-
head injections resulted in depression of the eyebrow in
the active state. This translates into a decreased ability
for upward excursion of the eyebrow after injection into
the forehead.
Our findings are important for patient counseling
before injection with botulinum exotoxin A. While it may
be possible to modify the eyebrow with botulinum exo-
toxin A injections, the resultant modification of the eye-
brow position in the relaxed state is not consistently pre-
dictable. When treating the forehead for rhytids, the
physician should modify the injections in a patient with
a ptotic eyebrow to avoid further lowering of the eye-
brow in the extended position. In other words, patients
who constantly and actively raise their eyebrows will likely
be perceived as having eyebrow ptosis after botulinum
exotoxin A injections to the frontalis muscle, because their
eyebrows will be relatively depressed. It is helpful in the
pretreatment patient consultation to manually lift or de-
press the patient’s eyebrows to demonstrate the possible
modification in eyebrow position and the varying de-
grees of resultant upper eyelid skin redundancy. This pro-
vides the patient with a better understanding of the pos-
sible aesthetic changes in the upper third of the face after
botulinum exotoxin A injection.
This study suggests that botulinum exotoxin A in-
jections to the upper third of the face do not universally
lift the eyebrows. Based on this study and our review of
the literature, botulinum exotoxin A may result in eye-
brow depression, eyebrow elevation, or no change in eye-
brow position. The resultant effect on the eyebrows is
likely multifactorial, including the site(s) and dosage of
injections, the extent of muscular paralysis, the state of
muscle activity, and individual anatomical variations.
Accepted for publication January 8, 2002.
Corresponding author: Mimi S. Kokoska, MD, Depart-
ment of Otolaryngology–Head and Neck Surgery, Indiana
University School of Medicine, 550 N University Blvd, Room
3170, Indianapolis, IN 46202.
REFERENCES
1. Carruthers A, Carruthers J. Clinical indications and injection technique for the
cosmetic use of botulinum A exotoxin. Dermatol Surg. 1998;24:1189-1194.
2. Blitzer A, Binder WJ, Aviv JE, Keen MS, Brin MF. The management of hyperfunc-
tional facial lines with botulinum toxin: a collaborative study of 210 injection sites
in 162 patients. Arch Otolaryngol Head Neck Surg. 1997;123:389-392.
3. Klein AW. Dilution and storage of botulinum toxin. Dermatol Surg. 1998;24:
1179-1180.
4. Huilgol SC, Carruthers A, Carruthers JDA. Raising eyebrows with botulinum toxin.
Dermatol Surg. 1999;25:373-376.
5. Frankel AS, Kamer FM. Chemical browlift. Arch Otolaryngol Head Neck Surg. 1998;
124:321-323.
6. Ahn MS, Catten M, Maas CS. Temporal brow lift using botulinum toxin A. Plast
Reconstr Surg. 2000;105:1129-1139.
7. Daniel WW. Biostatistics. 6th ed. New York, NY: John Wiley & Sons Inc;
1995.
8. Binder WJ, Blitzer A, Brin MF. Treatment of hyperfunctional lines of the face with
botulinum toxin A. Arch Otolaryngol Head Neck Surg. 1997;123:393-396.
9. Wieder JM, Moy RL. Understanding botulinum toxin. Dermatol Surg. 1998;24:
1172-1174.
10. Woodburne RT. Essentials of Human Anatomy. 6th ed. New York, NY: Oxford
University Press Inc; 1978:199-212.
(REPRINTED) ARCH FACIAL PLAST SURG/ VOL 4, OCT-DEC 2002
WWW.ARCHFACIAL.COM
247
©2002 American Medical Association. All rights reserved.
Wyszukiwarka
Podobne podstrony:
więcej podobnych podstron