
CHRONIC VIRAL
HEPATITIS

THE TERM VIRAL HEPATITIS
GENERALLY REFERS TO DISEASE
CAUSED BY THE 5 WELL-
DESCRIBED HEPATOTROPIC
VIRUSES, WHICH ARE DIVIDED
INTO ENTERAL AND
PARENTERAL GROUPS ON THE
BASIS OF THEIR MODE OF
TRANSMISSION

LABORATORY DIAGNOSIS
• AMINOTRANSFERASES (ALT, AST)
• BILIRUBIN
• PROTHROMBIN TIME (INR,
PROTROMBIN RATIO)
• SEROLOGIC MARKERS

HEPATITIS B VIRUS (HBV)
• Hepadnaviridae
• DNA VIRUS (the HBV genome is a
CIRCULAR, PARTIALLY DOUBLE-
STRANDED DNA)
• INCUBATION PERIOD: 1-6 MONTHS
• PARENTERAL TRANSMISSION (+++),
SEXUAL TRANSMISSION (+++),
PERINATAL TRANSMISSION (+++)

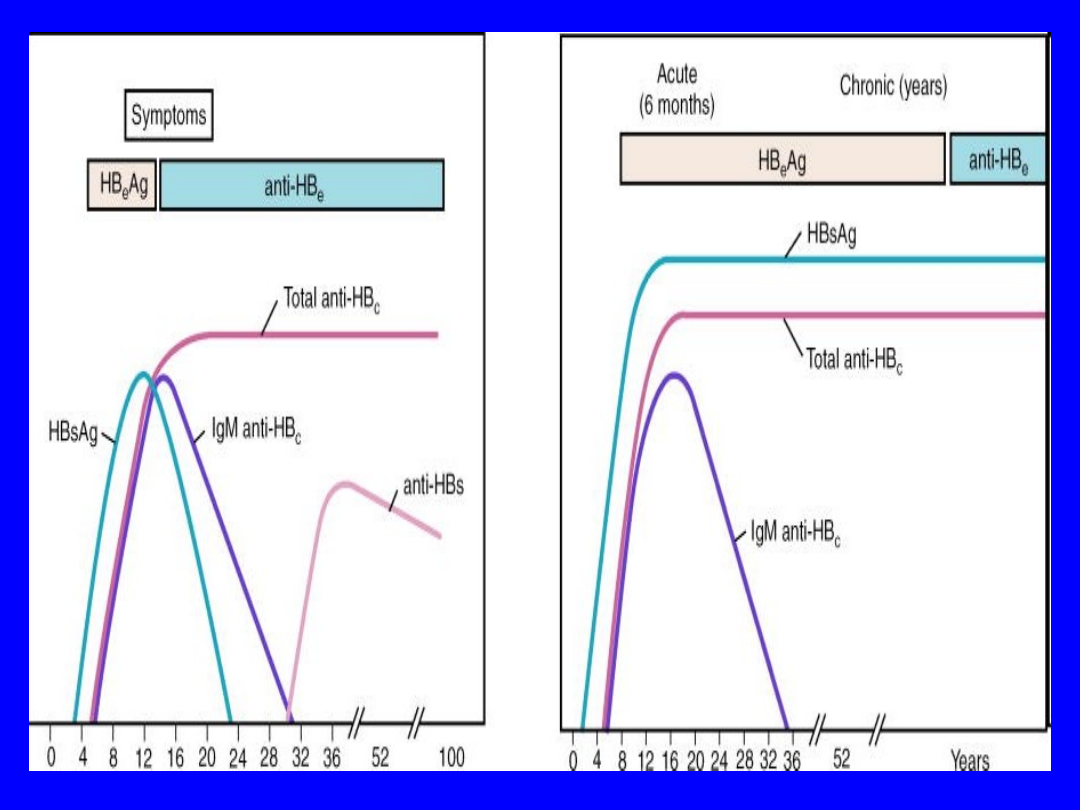
DIAGNOSIS
HBsAg (+)
IgG anti-HBc Ab (+)

HEPATITIS C VIRUS (HCV)
• NANB HEPATITIS
• Flaviviridae
• ss(+) RNA VIRUS (the HCV genome is
a SINGLE-STRANDED, POSITIVE-
SENSE RNA)
• INCUBATION PERIOD: 15-150 DAYS
• PARENTERAL TRANSMISSION (+++),
SEXUAL TRANSMISSION (+),
PERINATAL TRANSMISSION (+)

HEPATITIS D VIRUS (HDV)
• Deltaviridae
• INCOMPLETE RNA VIRUS
(REQUIRES HBsAg TO COMPLETE ITS REPLICATIVE CYCLE)
• INCUBATION PERIOD: 2-8 WEEKS
• PARENTERAL TRANSMISSION (++),
SEXUAL TRANSMISSION (++),
PERINATAL TRANSMISSION (+)
• CO-INFECTION / SUPERINFECTION

SPECIFIC AREAS THAT HAVE A
HIGH PREVALENCE OF HBV
CARRIERS INFECTED WITH
HDV INCLUDE the AMAZON
BASIN IN SOUTH AMERICA,
CENTRAL AFRICA, the
MEDITERRANEAN BASIN AND
the MIDDLE EAST.

TWO CLINICAL SCENARIOS
OF ACUTE HDV INFECTION
• COINFECTION WITH ACUTE HBV INFECTION
– RESULTS IN AN ACUTE HEPATITIS
INDISTINGUISHABLE FROM ACUTE
HEPATITIS B, BUT IT IS USUALLY SEVERE –
DEATH IN 2-20% OF CASES
• SUPERINFECTION IN A PATIENT
CHRONICALLY INFECTED WITH HBV –
THERE IS USUALLY A SIGNIFICANT
EXACERBATION OF PREEXISTING HBV
LIVER DISEASE

DIAGNOSIS
• CO-INFECTION
• IgM anti-HDV Ab
(+)
• HBsAg (+)
• IgM anti-HBc Ab
(+)
• SUPERINFECTION
• IgM anti-HDV Ab
(+)
• HBsAg (+)
• IgM anti-HBc Ab (-)

HEV INFECTION HAS RECENTLY
BEEN ASSOCIATED WITH CHRONIC
HEPATITIS IN SOLID
ORGAN-TRANSPLANT RECIPIENTS.
Kamar N, Selves J, Mansuy JM, et al.
„Hepatitis E virus and chronic
hepatitis in organ-transplant
recipients”.
N Engl J Med. Feb 21 2008;358(8):811-
7
THERAPY OF ACUTE VIRAL
HEPATITIS
TYPE
MAJOR FOCUS
COMMENTS
Hep A
Symptomatic therapy only
Observe for FHF
OLT
Hep B
Symptomatic therapy;
consider oral therapy for severe
acute Hep B
Observe for FHF
OLT
Hep C
(PEG)IFN-α therapy
TRT efficacious in
acute Hep C
Hep D
Vaccination against HBV
infection
Liver disease
clinically more
severe than Hep B
alone
Hep E
Symptomatic therapy only
FHF in pregnant
women

HBV IS A GLOBAL HEALTH
PROBLEM WITH AN
ESTIMATED 350 MILLION
HBV CARRIERS
WORLDWIDE AND 500 000
DEATHS EACH YEAR
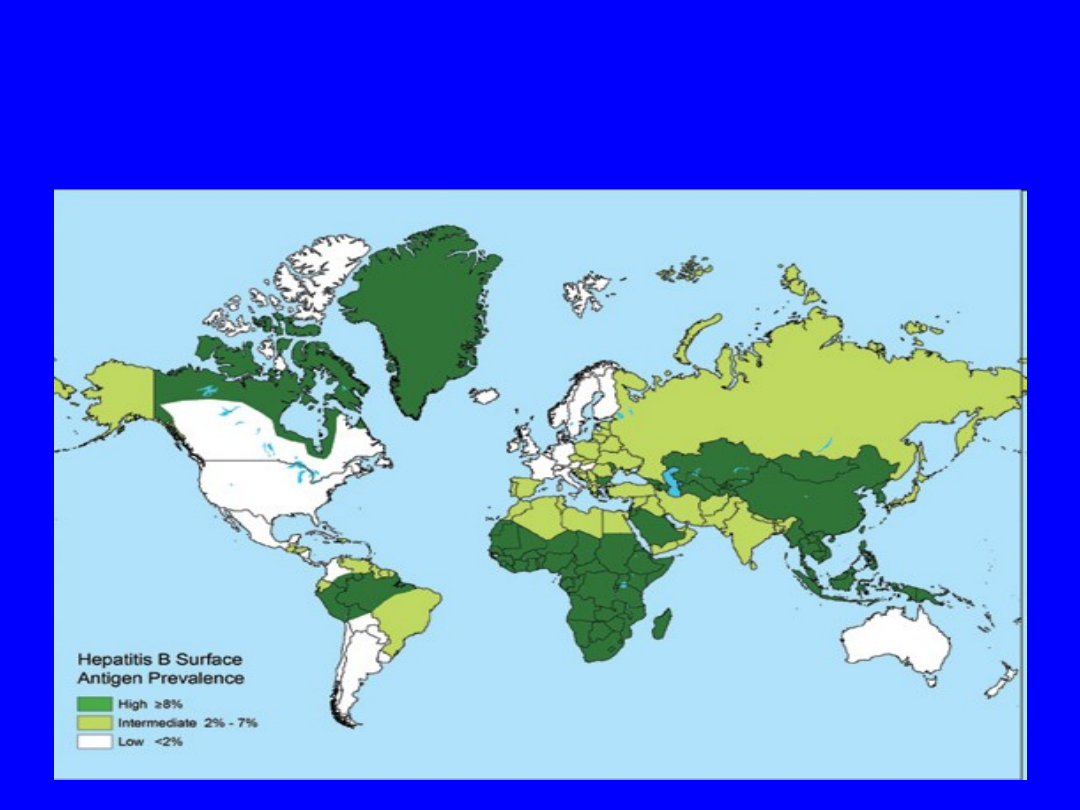
PREVALENCE OF CHRONIC INFECTION WITH HBV,
BY COUNTRY, 2006 (CDC)

COMPLICATIONS OF CHRONIC
VIRAL HEPATITIS
• EXTRAHEPATIC MANIFESTATIONS OF
CHRONIC VIRAL HEPATITIS
• LIVER CIRRHOSIS
• HEPATOCELLULAR CARCINOMA (HCC)

EXTRAHEPATIC MANIFESTATIONS
OF HBV INFECTION
• POLYARTERITIS NODOSA
• GLOMERULONEPHRITIS
• CRYOGLOBULINEMIA (controversial)

EXTRAHEPATIC MANIFESTATIONS
OF HCV INFECTION
• CRYOGLOBULINEMIA
• GLOMERULONEPHRITIS
• IDIOPATHIC THROMBOCYTOPENIC PURPURA
• LICHEN PLANUS (controversial)
• Raynaud syndrome
• Sjögren syndrome
• Porphyria cutanea tarda
• Necrotizing cutaneous vasculitis
• Non-Hodgkin lymphoma

EVALUATION OF PATIENTS
WITH CHRONIC VIRAL
HEPATITIS
• AMINOTRANSFERASES
• HBV DNA (VIRAL LOAD) / HCV
GENOTYPE
• LIVER BIOPSY
• COMORBIDITIES / COINFECTIONS

TREATMENT OF CHRONIC
HEPATITIS B
INTERFERON
(without
RIBAVIRIN !!)
ORAL ANALOGS:
• LAMIVUDINE
• ADEFOVIR
• ENTECAVIR
• TENOFOVIR
• TELBIVUDINE
TREATMENT OF CHRONIC
HEPATITIS C
INTERFERON (IFN) + RIBAVIRIN (RBV)
THE BEST CHOICE IS PEG-IFN + RBV

Reduced Responsiveness for
antiviral therapy of chronic
hepatitis C
• Genotype 1
• HCV-RNA > 2 milion copies/ml
• Long-duration disease
• Age > 40
• Immunosupresion
• African American
• Obesity
• Hepatic steatosis
• Reduced adherence

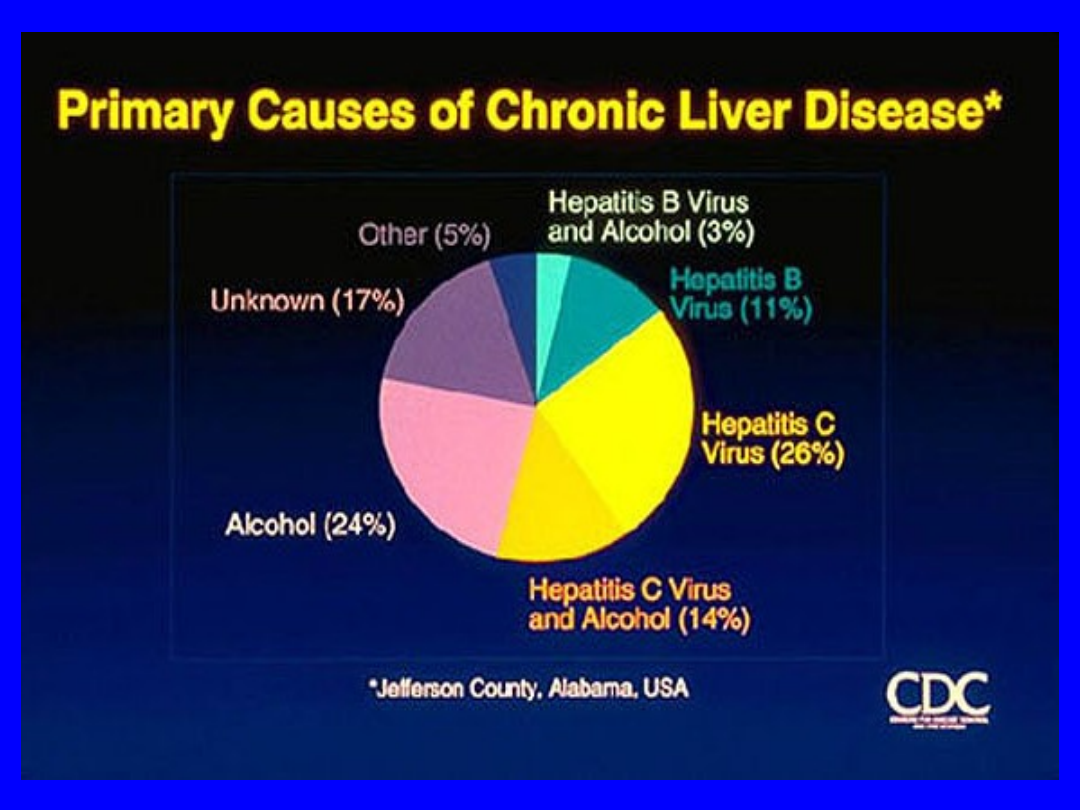
MOST COMMON CAUSES OF
CIRRHOSIS IN THE UNITED
STATES
• HEPATITIS C (26%)
• ALCOHOLIC LIVER DISEASE (21%)
• HEPATITIS C plus ALCOHOLIC LIVER
DISEASE (15%)
• CRYPTOGENIC CAUSE (18%)
• HEPATITIS B, which may be
coincident with hepatitis D (15%)

PREVENTION
• GENERAL MEASURES
• PASSIVE IMMUNIZATION =
IMMUNOGLOBULIN
• ACTIVE IMMUNIZATION
=VACCINATION

HBV PREVENTION -
VACCINATION
SUCESSFUL VACCINATION NOT ONLY IS
EFFECTIVE IN PREVENTING HEPATITIS B
INFECTION BUT ALSO PREVENTS THE
SEQUELAE OF CHRONIC HEPATITIS B
INFECTION AND THIS IS THE FIRST
EXAMPLE THAT CANCER CAN BE
PREVENTED BY VACCINATION

HBV PREVENTION
• RECOMBINANT VACCINE (HBsAg)
• THE BEST VACCINATION SCHEDULE
IS 0-1-6 MONTHS
• PROTECTIVE LEVEL OF IMMUNE
RESPONSE AFTER VACCINATION IS
DEFINED AS LEVEL OF anti-HBs Ab
(GREATER THAN 10 IU/L)

PREVENTION OF PERINATAL
TRANSMISSION OF HBV
THE CURRENT RECOMMENDATION IS TO
PROVIDE PASSIVE-ACTIVE IMMUNIZATION TO
NEWBORNS OF CARRIER MOTHERS.
INFANTS SHOULD RECEIVE BOTH HBIG (0,06
mL/kg) AND VACCINE, AND THE FIRST DOSE OF
VACCINE SHOULD BE GIVEN WITHIN 12 HOURS
OF BIRTH AND THE SECOND AND THIRD DOSES
AT 1 AND 6 TO 12 MONTHS, RESPECTIVELY.
THIS REGIMEN HAS A PROTECTIVE EFFICACY OF
95%.

A combination vaccine
(Twinrix), which expresses both
HBsAg and hepatitis A virus, is
also available and is approved
for use in adults in the United
States and Europe. This
vaccine is typically used for
convenience when protection
against both viruses is needed.
Document Outline
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
Wyszukiwarka
Podobne podstrony:
Chronic Hepatitis B
Long term Management of chronic hepatitis B
ABC Chronic viral hepatitis
Hepatitis E Virus
1-Kefir chroni przed mutacjami w DNA, ZDROWIE-Medycyna naturalna, Poczta Zdrowie
Dozwolony użytek chronionych utworów, Kulturoznawstwo UAM, Ochrona właśności intelektualnej
Nauczyciele będą chronieni jak funkcjonariusze publiczni, 03. DLA NAUCZYCIELI
Gładysz A Interteron alfa w przewlekłych hepatitis
Jak chronić własne dziecko przed narkotykami
Bóg chroni swoich wiernych
Witamina B17 - lekarstwo na raka, @P PROD. KTÓRE CHRONIĄ PRZED RAKIEM @, Rak i terapia
Dlaczego należy chronić drzewa, KARTY PRACY MÓJ ŚWIAT 5
Testosteron może chronić przed anoreksją i bulimią, anoreksja ,bulimia, ortoreksja ... -zaburzenia o
Chronic Pain Syndromes After Ischemic Stroke PRoFESS Trial
Antyoksydanty chroniace organizm
kwiaty chronione 11.03, ozdoby z makaronu, konpekty świetlica, Dokumenty
Jak chronić adres e-mail na stronie przed spamem stosując przekierowanie, PHP Skrypty
więcej podobnych podstron