RECONSTRUCTIVE SURGERY
269
more freely moveable, such as the neck and trunk, the transposition fl ap is occasionally used in tight-skinned
regions, such as in the head, to cover a defect (e.g., nasocutaneous fi stula) (Figure 6.44a). The length and width
of a transposition fl ap should be slightly longer and wider than the defect itself. In the case of pedicle skin fl aps,
the work of Hinchcliff, et al. showed a positive correlation between fl ap width and viable length.
11
Since the
transposition fl ap’s length decreases as the arc of rotation increases and the horse’s skin lacks the extensibility
seen in small animals, the fl ap should be created as close to the lesion as possible (Figure 5.41). Often in tight-
skinned regions, a small defect may remain and need to heal by second intention (Figure 6.44f). For more
information regarding the use of a transposition fl ap for the repair of nasocutaneous fi stula, see Chapter 6.
Vascularized Free Tissue Transfers
Large wounds, particularly those involving the distal limb, remain diffi cult to treat using reconstructive
surgical techniques. Vascularized free tissue transfers, based on axial pattern fl aps and using microvascular
anastomosis, are commonly used in small animals.
17,53–55
Attempts have been made to adapt this approach for
use in the horse.
56
In the horse, a large free axial pattern skin fl ap and microvascular anastomosis using the deep
circumfl ex iliac artery and vein
57,58
and a smaller skin fl ap using the saphenous artery and medial saphenous
vein have been described.
59
In these experimental studies none of the transferred skin fl aps survived longer
than 4 to 6 days. Failure was believed to result from ischemia reperfusion injury, vascular thrombosis, and poor
perfusion as a result of vasospasm, known as a “no-refl ow” phenomenon, within the skin fl ap. An experimental
study showed no difference in the accumulation of neutrophils, a signifi cant source of oxygen free radicals,
between the control myocutaneous fl ap and those subjected to ischemia and reperfusion.
60
More work is needed
to defi ne the potential benefi ts of this approach.
Conclusion
The aim of reconstructive surgery is to shorten healing time, improve cosmesis of the site over that
which would be achieved by second intention healing, and return the horse to performance as soon as possible.
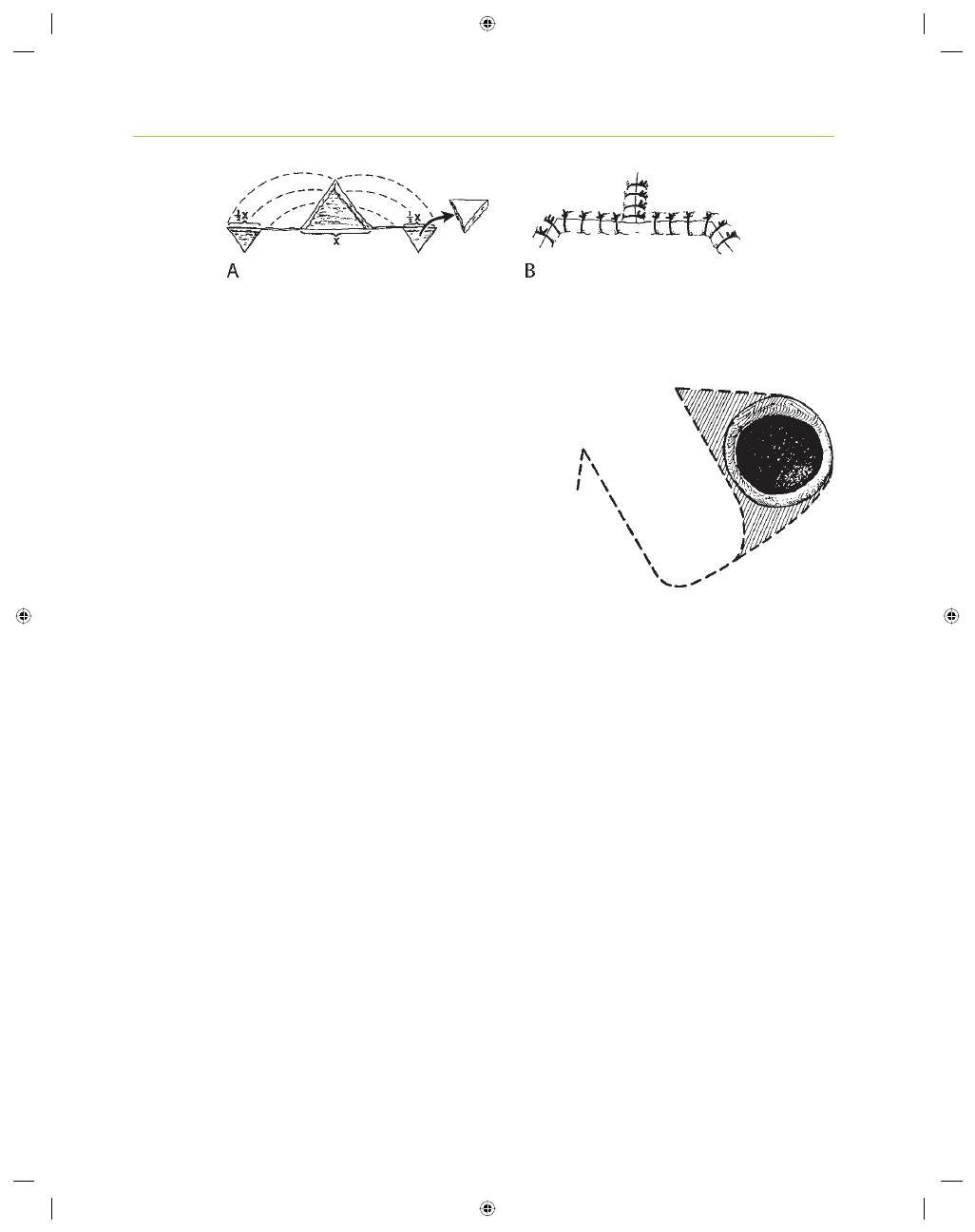
Figure 5.40. Triangular-shaped defect with loose skin available on either side. (A) Two inverted triangles, equaling 1/2 X, are
created several base-widths away from the defect. The skin is undermined (dotted lines) in preparation for mobilization and closure.
(B) Simple interrupted sutures are used for skin apposition.
Figure 5.41. A transposition fl ap is created to cover a full-thickness circular
defect (solid black). Dotted lines indicate incisions. The solid line indicates the
circular defect. Oblique lines surrounding the circular defect represent further
skin removal required to accommodate transposition of the skin fl ap from left
to right.
Wyszukiwarka
Podobne podstrony:
00283, b3d48a8e52ed45c007a5454e95d02d18
00283, ef1f3a62a628f300b8c7f958ad10a522
00283, dbfd715416f9d57c86c58af24d20cbda
00283, b3d48a8e52ed45c007a5454e95d02d18
(00283) Point Remove Creek current M1791
00283, ef1f3a62a628f300b8c7f958ad10a522
więcej podobnych podstron