INFECTIONS IN
INFECTIONS IN
PREGNANCY AND
PREGNANCY AND
PUERPERIUM
PUERPERIUM
Krzysztof Drews
Krzysztof Drews
Division of Perinatology and Women Diseases
Division of Perinatology and Women Diseases
Infection - pathogens’ invasion,
colonization and immune response of
the host organism.
This process depends on pathogenicity
and defense mechanisms of the host.
Prenatal infections:
– vertical
– ascending
Changes in immune system in
Changes in immune system in
pregnancy
pregnancy
Progesterone - decreases activity of lymphocytes
T
- activates function of Ts and NK
HCG - decreases activity of NK cells
- activates proliferation of
lymphocytes T
Estrogens - activate function of Ts cells
PGE2 - decreases activity of lymphocytes
T
Vertical infections
Vertical infections
TORCH - main vertical infection
with
similar symptoms:
T - toxoplasmosis
O - others (syphilis)
R - rubella
C - cytomegalovirus
H - herpes simplex, hepatitis,
human immunodeficiency virus
B
B
oth b
oth b
acterial and viral
acterial and viral
infections can result
infections can result
in:
in:
spontaneous abortion
stillbirth
preterm delivery
intrauterine growth retardation
congenital anomalies of the fetus
(hydrocephalus, chorioretinitis, cataract
hepatosplenomegaly, purpura, ascites, heart
defects)
congenital infections
About
2 - 3%
of congenital infections are
caused by
viruses.
Prenatal diagnosis
Prenatal diagnosis
serological screening of syphilis,
toxoplasmosis, hepatitis B
ultrasound examination
amniocentesis and isolation of
pathogenes (HSV, CMV, Rubella virus,
T.gondi)
cordocentesis and detection of the
cord - blood specific immunoglobulins
Rubella
Rubella
The virus causes cytolysis and decreases
mitotic activity.
Incubation period:
14 - 21 days.
Symptoms:
flu-like symptoms and after 1-
5 days macular rash with postauricular
and suboccipital lymphadenopathy
Specific IgM anti-bodies occur 14 days
after infection and are present for 3
months. IgG appear later and usually
persist for the whole life.
Congenital rubella
Congenital rubella
maternal infection in the first
trimester can induce spontaneous
abortion,
risk of transplacental infection: 22%
neonates born to mothers who
suffered from rubella in the first
trimester are affected and 10% as the
effect of rubella in the second
trimester
Classical triad of congenital
Classical triad of congenital
rubella symptoms described
rubella symptoms described
by Gregg:
by Gregg:
cataract
perceptive deafness
congenital heart defect
Other symptoms:
intrauterine growth retardation
retinopathy
meningoencephalitis
purpura
splenomegaly
mental retardation
pneumonia
hepatitis
Rubella - prevention /
Rubella - prevention /
treatment
treatment
There is no specific therapy.
Vaccinations: school children and
women at the reproductive age
who have no specific IgG anti -
bodies.
CMV
CMV
is considered to be the
is considered to be the
most common viral cause of
most common viral cause of
congenital infection
congenital infection
10% of infected neonates develop
classical congenital CMV infection
5% have non - typical symptoms
85% are asymptomatic
Transmission to the fetus occurs in
40% pregnencies with primary
CMV. Infection acquired earlier in
gestation results in a more severely
affected infant.
Symptoms of congenital
Symptoms of congenital
CMV infection:
CMV infection:
intrauterine growth retardation
microcephaly
periventricular calcifications
hepatosplenomegaly
non - immune hydrops
ascites
thrombocytopenia and purpura
perceptive deafness
pneumonia
jaundice
CMV
CMV
Approximately 5 - 15% of the
initially asymptomatic infants
develop the symptoms, such as
mild mental retardation or
hearing loss, by the age of two.
Hepatitis B
Hepatitis B
Fulminant hepatitis is more often during
pregnancy
(ascites,
encephalopathy,
rapidly shrinking liver, jaundice). The
mortality rate is 90%.
Infection:
transplancental or during
delivery
Most neonates at the time of delivery are
seronegative and asymptomatic but
within
3
months
they
become
seropositive.
Teratogenic effect is not proved.
Hepatitis B -
Hepatitis B -
prevention
prevention
All pregnant women should be screened for
HBsAg.
Women with a definite exposure to HBV
should be given HBIG within 7 days and
the second dose after a month.
Infants born to HBsAg - positive women
should receive HBIG and the first dose of
the recombinant HBV vaccine within 12
hours after birth. The second dose should be
given after a month and the third after 3
months. This treatment protects
70 - 75%
of
the infants.
Hep
Hep
a
a
titis
titis
C
C
75%
patients are asymptomatic
25%
develop symptoms of past
hepatitis B
50%
of cases become a chronic
infection
5%
of fetuses born to HCV – positive
mothers are infected and even more if
there is a co-infection of HCV and HIV
Human
Human
Immunodeficiency
Immunodeficiency
Virus
Virus
Pregnancy provokes rapid progression of
HIV infection and developing symptoms,
mainly Pn. carini pneumonia.
There is also higher risk of spontaneous
abortion, preterm delivery, IUGR, PROM.
HIV is usually transmitted during
delivery, but also transplancetal infection
and infection through breast - feeding are
possible (risk of about 20%).
Prevention
Prevention
of
of
vertical
vertical
HIV
HIV
infection
infection
Zidovudine prophylaxis since 14th week of
pregnancy and elective caesarean section
reduce transmission rate to 6 - 7% (but
some researches revealed no differences
in the infection rate during spontaneous
delivery and caesarean section)
Prophylaxis of Pn. carini pneumonia:
trimetoprim/ sulphametoxazol
Avoid amniocentesis, chorionic villous
sampling, cordocentesis and other invasive
procedures (also spontaneous delivery)
Avoid breast - feeding
Toxoplasmosis
Toxoplasmosis
Fetal infection occurs only with
acute maternal toxoplasmosis.
The likelihood of transmission
varies with gestational age - it
is more frequent, but less
severe in late weeks of
pregnancy.
Maternal reinfection is not
dangerous for the fetus.
Acute primary
Acute primary
toxoplasmosis can result
toxoplasmosis can result
in:
in:
spontaneous abortion
preterm delivery
intrauterine growth retardation
central nervous system defects
hepatosplenomegaly
Symptoms of congenital
Symptoms of congenital
toxoplasmosis:
toxoplasmosis:
chorioretinitis
periventricular calcifications
hydrocephaly
– microcephaly
– jaundice
– anaemia
– hepatosplenomegaly
– thrombocytopenia
– lymphadenopathy
– mental retardation
– visual deficits
classical
triad
Toxoplasmosis - treatment
Toxoplasmosis - treatment
In early pregnancy: spiramycin -
without side
effects in first trimester
In the second and third trimester:
pyrimethamine
and sulfadiazine
- the most effective
treatment,
but
teratogenic
Syphylis
Syphylis
Treponema palidum passes
through the placenta and
attacks the fetus after the 5
th
month of pregnancy.
It can cause preterm delivery,
stillbirth and congenital
infection even 2 - 3 years after
mother's infection.
Each pregnant woman
Each pregnant woman
should be screened for
should be screened for
syphilis infection
syphilis infection
Serological tests:
VDRL (Venereal Disease Research
Laboratory) sensitivity
50 - 70%
TPHA
(Treponema
Palidum
Haemaglutination Assay) – sensitivity
70 - 90%
FTA – ABS (Fluorescent Treponemal
Antibody Absorbed) - sensitivity
70 -
90%
Ascending infections –
Ascending infections –
risk factors of intra-
risk factors of intra-
amniotic infection (IAI)
amniotic infection (IAI)
duration of labor
duration of PROM
number of vaginal examinations
coexistence of bacterial vaginosis (BV)
amniocentesis, cordocentesis
internal fetal monitoring
malnutrition
nulliparity
Premature rupture of membranes
is associated with increased risk
of infection concerning both fetus
and mother.
Microorganisms are present in
amniotic
fluid
in
66,6%
of
patients with PROM
IAI -
IAI -
definition
definition
Acute clinical infection of the amniotic fluid
and intrauterine contents during pregnancy.
Occurs in 0,5 – 10% of all pregnancies
Risk of:
– Premature delivery
– PROM – the cause or consequence of IAI?
– Neonatal complications (prematurity, pneumonia,
sepsis, NEC, intraventricular hemorrhage)
– Puerperal infections
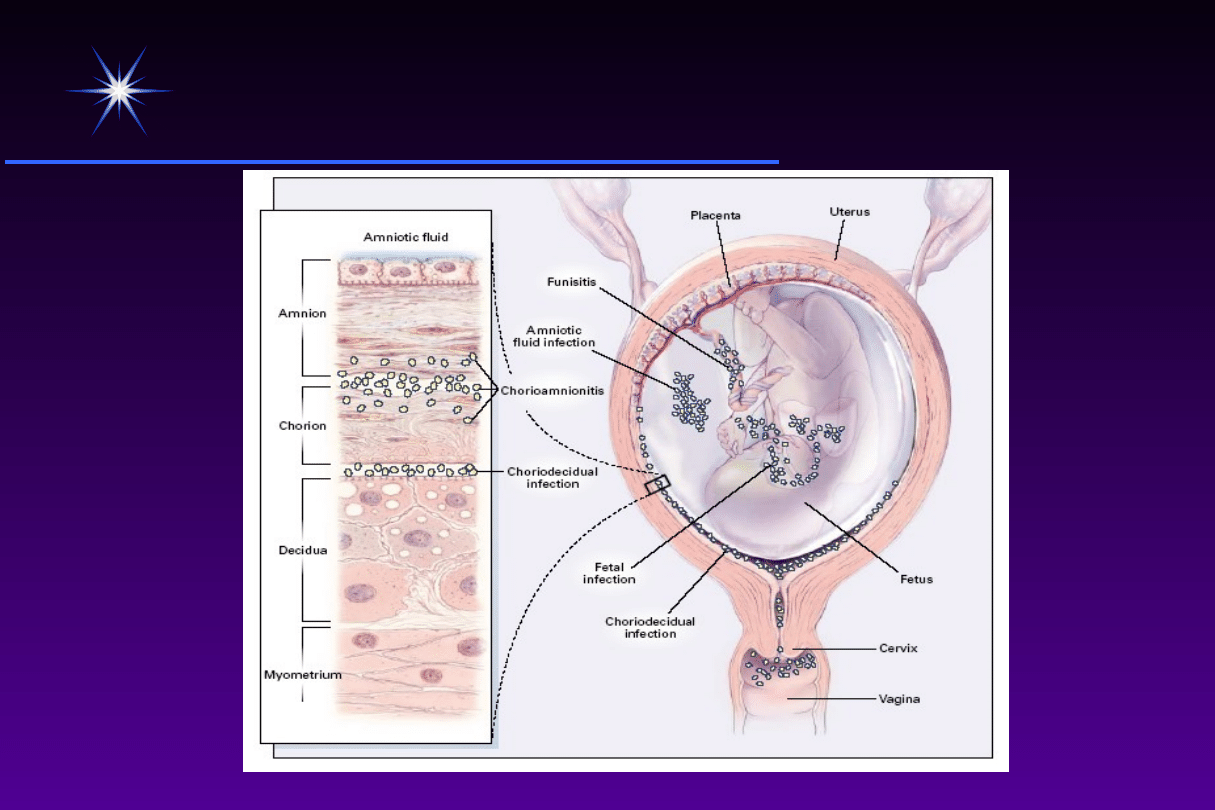
Potential pathways of infection
Potential pathways of infection
Goldenberg et al. N Eng J Med. 2000
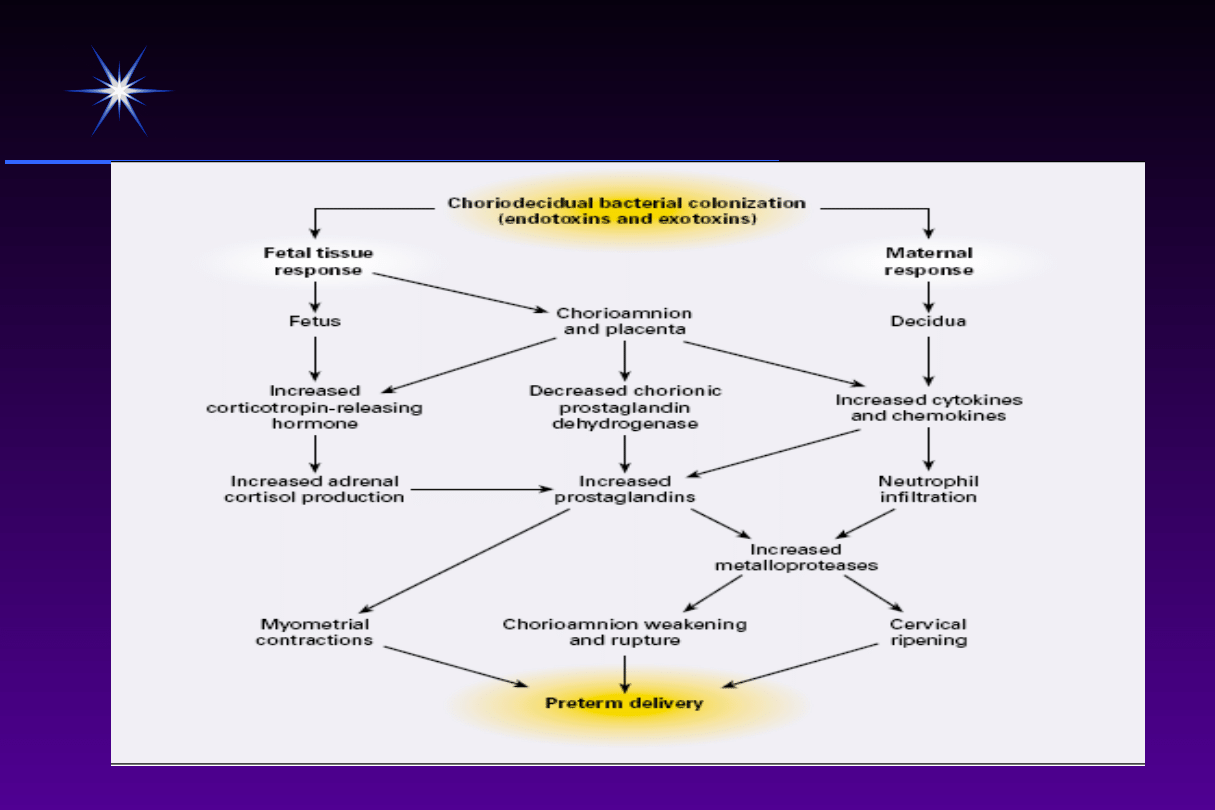
Bacterial colonization and
Bacterial colonization and
preterm delivery
preterm delivery
Goldenberg et al. N Eng J Med. 2000
Probiot
Probiot
ics
ics
Hydrogen peroxide (H
2
O
2
)-producing strains
of Lactobacillus have been found in 61% of
pregnant women with normal flora, yet in only
5%
of women with BV.
H
2
O
2
has been shown to be toxic to BV-causative
organisms, namely, Gardnerella vaginalis and
Prevotella bivia.
Diagnosis of IAI
Diagnosis of IAI
The
early
stage
of
IAI
is
asymptomatic
Later - symptoms are neither
sensitive nor specific
Only results of laboratory tests
enable to diagnose an early
infection.
IAI
IAI
SYMPTOMS
fever
leukocytosis
uterine tenderness
tachycardia of the
fetus and/or
mother
foul amniotic fluid
(in cases with
PROM)
TREATMENT
antibiotic therapy
elective cesarean
section, that
enables to
eliminate the
possibility of
spreading of the
infection.
IAI – strategy of
IAI – strategy of
antibiotic therapy
antibiotic therapy
result
of
bacteriological
examination
most
frequent
microorganisms
associated with IAI
drug administration as early as
possible
combination of two antibiotics with
various anti-bacterial spectrum
Cytokiny Il-1, Il-6, TNF
Arachidonic acid
Prostaglandins E
2
i F2
Fosfolipase A
2
i C
Arachidonic acid
Prostaglandins
E
2
, F
2
Bacterial toxins
Bacterial toxins
Contractions
Il-8
Cervical dilatation
Intra-amniotic infection
Intra-amniotic infection
Management
Management
Antibiotic treatment
Start of treatment – as quick as possible,
even before pathogen identification.
2 or 3 antibiotics
Duration of treatment – 2 days longer than
the symptoms are present.
Treatment - newborn
Treatment - newborn
Treatment decision depends on the
symptoms developed by the infant and
results of examinations.
If antibiotic therapy is necessary,
recommended drugs are ampicilin with
gentamycin.
FIRS as a predictor of impared
FIRS as a predictor of impared
neurologic outcome
neurologic outcome
FIRS (Fetal Inflammatory Response Syndrome) – usually
subclinical activation of fetal immune system, defined by
elevations in the levels of specific cytokines, especially
interleukin-6 (Il-6) in amniotic fluid and fetal plasma
Histological funisitis is more specific predictor of
neurologic outcome than Il-6 (PPV 86% vs 59%)
Mittendorf 2004
FIRS as a predictor of
FIRS as a predictor of
impared neurologic
impared neurologic
outcome
outcome
Fetal plasma Il-6 concentration > 10pg/mL and
histological funisitis are associated with variety of adverse
neonatal outcomes: intraventricular hemorrhage, sepsis,
meningitis, cerebral palsy, perinatal death
Mittendorf 2004
Fetal
Inflammatory
Response
Fetal
Inflammatory
Response
Preterm
birth
Preterm
birth
Intrauterine
infection
Intrauterine
infection
WMD/CP
WMD/CP
Dammann et Leviton, Early Hum Develop, 2004
Dammann et Leviton, Early Hum Develop, 2004
Hypoxic obstetric events and
Hypoxic obstetric events and
cerebral palsy
cerebral palsy
1862 William John Little
- the link between cerebral
palsy and events complicating the perinatal period
Hypoxic obstetric events are responsible for only 8–10%
of the cases of cerebral palsy and in most cases the
condition remains unexplained
Intraamniotic infection ?
Chorioamnionitis and
Chorioamnionitis and
cerebral palsy
cerebral palsy
Clinical chorioamnionitis was associated with:
cerebral palsy RR 1,9 Cl (1,4-2,5)
periventricular leukomalacia RR 3,0 Cl (2,2-4,0)
cerebral palsy
RR 1,9
Cl (1,4-2,5)
periventricular leukomalacia
RR 3,0
Cl (2,2-4,0)
Histologic chorioamnionitis was associated with:
Histologic chorioamnionitis was associated with:
cerebral palsy RR 1,6 Cl (0,9-2,7)
periventricular leukomalacia RR 2,1 Cl (1,5-2,9)
cerebral palsy
RR 1,6
Cl (0,9-2,7)
periventricular leukomalacia
RR 2,1
Cl (1,5-2,9)
Wu et Colford, JAMA 2000
Wu et Colford, JAMA 2000
BRAIN DAMAGE
PVL
The role of TNF-
The role of TNF-
in
in
the pathophysiology of PVL
the pathophysiology of PVL
fetal hypotension
and brain ischaemia
stimulating the production
of a tissue factor
activation of the
haemostatic system
coagulation
necrosis of white matter
release of platelet
activating factor
direct cytotoxic effect of
TNF on oligodendrocytes
Leviton A. Dev Med Child Neurol 1993
Infections in puerperium
Infections in puerperium
Infection of perineum
Infection of wounds
Endometritis
Sepsis
Mastitis
Infections in puerperium
Infections in puerperium
Fever is the most common symptom of infections in puerperiumist
Body temperature
>38 C
Early
<48h after delivery
Late
>48h after delivery
Infections in puerperium
Infections in puerperium
Reasons of fever in puerperium:
Retention of lochia
Endometritis
Complicated healing of wound
Mastitis
Thrombophlebitis
Pyelonephritis
Sepsis
Pneumonia
Infection of episiotomy wound
Is not very common but very uncomfortable
post-partum complication.
Concern 0,035 - 3% of every delivery
It may lead to more serious complications
(sepsis, necrotizing fasciitis)
Treatment: surgical + antibiotics
Infections in puerperium
Infections in puerperium
Post Caesarean Section Wound Infection
• Concern 1,6 - 10% of cesarean sections
• Increased risk: long operation time, increased blood lost,
obesity, age, intraaniotic infection, bacterial vaginosis.
• Treatment: surgical + antibiotics
Infections in puerperium
Infections in puerperium
Endometritis
• Endometritis is an infection of the endometrium or decidua,
with extension into the myometrium
.
• Risk of endometritis after c. section is 30 times higher
then after vaginal delivery
• Treatment: antibiotics (mono or polytherapy)
Bacteria isolated from uterus of women with endometritis
Peptostreptococcus
Bacterodes sp.
Entorococcus
Streptococcus B, A
Escherichia coli
Clostridium
Chlamydia
Gardnerella vaginalis
Infections in puerperium
Infections in puerperium
Mastitis
• Etiology: S.aureus
• Symptoms: edema, pain, tenderness,
redness of mammary gland and fever
• Treatment: antibiotics
• Prophylaxis
Infections in puerperium
Infections in puerperium
Thank you for your
Thank you for your
attention
attention
Document Outline
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Slide 45
- Slide 46
- Slide 47
- Slide 48
- Slide 49
- Slide 50
- Slide 51
Wyszukiwarka
Podobne podstrony:
PROF DREWS Infections in pregn and puerp (1)
PROF DREWS Infections in pregn and puerp (1)
2010 6 NOV Current Topics in Canine and Feline Infectious Diseases
The pathogenesis of Sh flexneri infection lessons from in vitro and in vivo studies
Transient TLR Activation Restores Inflammatory Response and Ability To Control Pulmonary Bacterial I
Estimation of Dietary Pb and Cd Intake from Pb and Cd in blood and urine
automating with step 7 in lad and fbd simatic (1)
Key Concepts in Language and Linguistics
Guide to the properties and uses of detergents in biology and biochemistry
2008 4 JUL Emerging and Reemerging Viruses in Dogs and Cats
2002 3 MAY Lasers in Medicine and Surgery
In vivo MR spectroscopy in diagnosis and research of
Numerical methods in sci and eng
conceptual storage in bilinguals and its?fects on creativi
20090602 01 ANSF, Coalition Forces further disable IED?lls in Khowst and Zabul
01 [ABSTRACT] Development of poplar coppices in Central and Eastern Europe
więcej podobnych podstron