
Emergencies in
Emergencies in
hematology
hematology
M. Zawartko, M.D.
M. Zawartko, M.D.
Department of Hematology,
Department of Hematology,
Pomeranian Medical University,
Pomeranian Medical University,
Szczecin
Szczecin

Emergencies in hematology
Emergencies in hematology
ATLS
ATLS
Hypercalcemia
Hypercalcemia
Spinal cord compression
Spinal cord compression
Superior vena cava syndrome
Superior vena cava syndrome
Leukocytostasis
Leukocytostasis
Hyperviscosity
Hyperviscosity
Pericardial effusion/tamponade
Pericardial effusion/tamponade
Intestinal obstruction
Intestinal obstruction
Urinary obstruction
Urinary obstruction
Malignant biliary obstruction
Malignant biliary obstruction
Increased intracranial pressure
Increased intracranial pressure
Neoplastic menigitis
Neoplastic menigitis
Other….
Other….
ATLS – Acute tumor lysis
ATLS – Acute tumor lysis
syndrome
syndrome
Is characterized by various combinations of:
Is characterized by various combinations of:
-
hyperuricemia;
hyperuricemia;
-
Hypergl
Hypergl
y
y
cemia;
cemia;
-
Hyperkalemia;
Hyperkalemia;
-
Hyperphosphatemia;
Hyperphosphatemia;
-
Hypocalcemia;
Hypocalcemia;
-
Lactic acidosis.
Lactic acidosis.
Is caused by the destruction of a large
Is caused by the destruction of a large
number of rapidly proliferating neoplastic
number of rapidly proliferating neoplastic
cells.
cells.
Frequently: acute renal failure develops as a
Frequently: acute renal failure develops as a
result of the syndrome.
result of the syndrome.
-Uric acid
-Glucose
-Potassium
-Phosphate
s
-Lactic acid

ATLS – Acute tumor lysis
ATLS – Acute tumor lysis
syndrome
syndrome
Most common offenders:
Leukemia
ALL & AML
Lymphoma
Aggressive or bulky
Also described in
MM, SCLC, breast, ovarian
ATLS usually occurs during or shortly (1-5 days)
ATLS usually occurs during or shortly (1-5 days)
after chemotherapy;
after chemotherapy;
In rare cases – spontaneous necrosis of
In rare cases – spontaneous necrosis of
malignancies causes ATLS – prior to chemotherapy.
malignancies causes ATLS – prior to chemotherapy.

ATLS – Acute tumor lysis
ATLS – Acute tumor lysis
syndrome
syndrome
Hyperuricemia:
Hyperuricemia:
May be present at the time of chemotherapy
May be present at the time of chemotherapy
Effective treatment kills malignant cells and
Effective treatment kills malignant cells and
leads to increased serum uric acid levels
leads to increased serum uric acid levels
from the turnover of nucleic acids.
from the turnover of nucleic acids.
Uric acid can precipitate in the tubules,
Uric acid can precipitate in the tubules,
medulla and collecting ducts of the kidney
medulla and collecting ducts of the kidney
leading to renal failure.
leading to renal failure.
Lactic acidosis and dehydratation may
Lactic acidosis and dehydratation may
contribute to the precipitation of uric acid in
contribute to the precipitation of uric acid in
the renal tubules.
the renal tubules.

ATLS – Acute tumor lysis
ATLS – Acute tumor lysis
syndrome
syndrome
Hyperphosphatemia
Hyperphosphatemia
Produces reciprocal depression in serum calcium
Produces reciprocal depression in serum calcium
Hypocalcemia – symptoms: neuromuscular
Hypocalcemia – symptoms: neuromuscular
irritability, tetany;
irritability, tetany;
Deposition of calcium phosphate in the kidney
Deposition of calcium phosphate in the kidney
and hyperphosphatemia may cause renal
and hyperphosphatemia may cause renal
failure.
failure.
Hyperkalemia
Hyperkalemia
-
In patients with renal failure may rapidly be life
In patients with renal failure may rapidly be life
– threatening.
– threatening.
-
Can cause ventricular arrhythmias and sudden
Can cause ventricular arrhythmias and sudden
death.
death.

ATLS – Acute tumor lysis
ATLS – Acute tumor lysis
syndrome
syndrome
The most important predictive factors:
The most important predictive factors:
-
tumor burden: hyperuricemia and high
tumor burden: hyperuricemia and high
levels of lactate dehydrogenase
levels of lactate dehydrogenase
(LDH>1500 U/l);
(LDH>1500 U/l);
-
Renal function
Renal function
Recognition & prevention are the most
Recognition & prevention are the most
important steps in the management of
important steps in the management of
this syndrome.
this syndrome.

ATLS – Acute tumor lysis
ATLS – Acute tumor lysis
syndrome
syndrome
Prophylaxis
Prophylaxis
Maintain hydratation by administration of ivf
Maintain hydratation by administration of ivf
at 3000 ml/m2 per day
at 3000 ml/m2 per day
Keep urine pH at 7,0 or greater by
Keep urine pH at 7,0 or greater by
administration of sodium bicarbonate
administration of sodium bicarbonate
Administer allopurinol at 300 mg/m2 per day
Administer allopurinol at 300 mg/m2 per day
Monitor serum chemistry.
Monitor serum chemistry.
Start chemotherapy when serum uric acid <8,0
Start chemotherapy when serum uric acid <8,0
mg/dl; serum creatinine <1,6 mg/dl; urine pH
mg/dl; serum creatinine <1,6 mg/dl; urine pH
>7,0.
>7,0.
If an urgent anticancer therapy is needed
If an urgent anticancer therapy is needed
consider dialysis.
consider dialysis.
ATLS – Acute tumor lysis
ATLS – Acute tumor lysis
syndrome
syndrome
In some cases, uric acid levels cannot be lowered sufficiently with the standard preventive
approach.
Rasburicase
can be effective in these instances.
Rasburicase
Recombinant urate oxidase enzyme
In humans, gene for this is inactivated
Converts uric acid to allantoin
Acts rapidly, decreasing uric acid levels within hours
Xanthine
Xanthine
Xanthin
e
oxidase
Uric Acid
Uric Acid
Allantoin
Allantoin
Urate Oxidase
Allopurin
ol
Hypoxanthi
Hypoxanthi
ne
ne
Xanthine
oxidase
Rasburicase
ATLS – Acute tumor lysis
ATLS – Acute tumor lysis
syndrome
syndrome
Despite aggressive
Despite aggressive
prophylaxis ATLS
prophylaxis ATLS
and/or oliguric or
and/or oliguric or
anuric renal failure
anuric renal failure
may occur;
may occur;
Dialysis is often
Dialysis is often
necessary and
necessary and
should be considered
should be considered
early in the course.
early in the course.
The prognosis is
The prognosis is
good, and renal
good, and renal
function recovers
function recovers
after the uric acid
after the uric acid
level is lowered to <
level is lowered to <
10 mg/dl.
10 mg/dl.
If:
If:
Serum K+ > 6mEq/l
Serum K+ > 6mEq/l
Serum uric acid >10
Serum uric acid >10
mg/dl
mg/dl
Serum
Serum
creatinine>10 mg/dl
creatinine>10 mg/dl
Serum
Serum
phosphate>10mg/dl
phosphate>10mg/dl
or increasing
or increasing
symptomatic
symptomatic
hypocalcemia
hypocalcemia
present
present
Treatment
Treatment
Begin
Begin
hemodialysis
hemodialysis
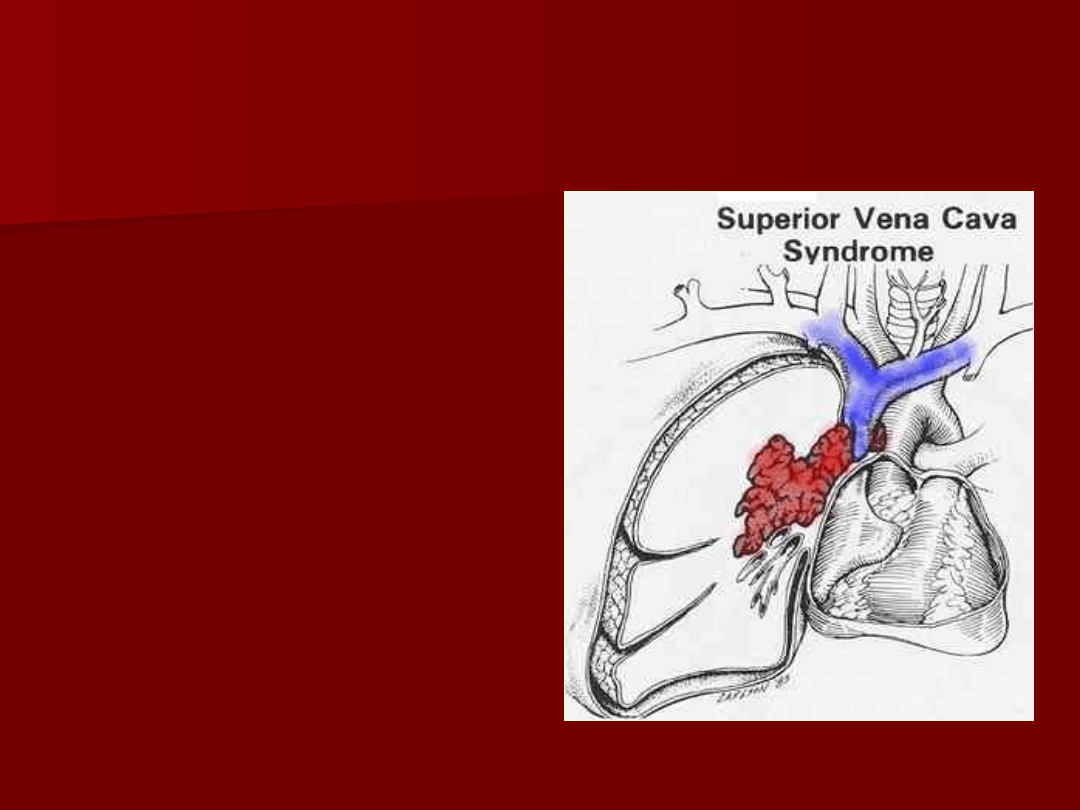
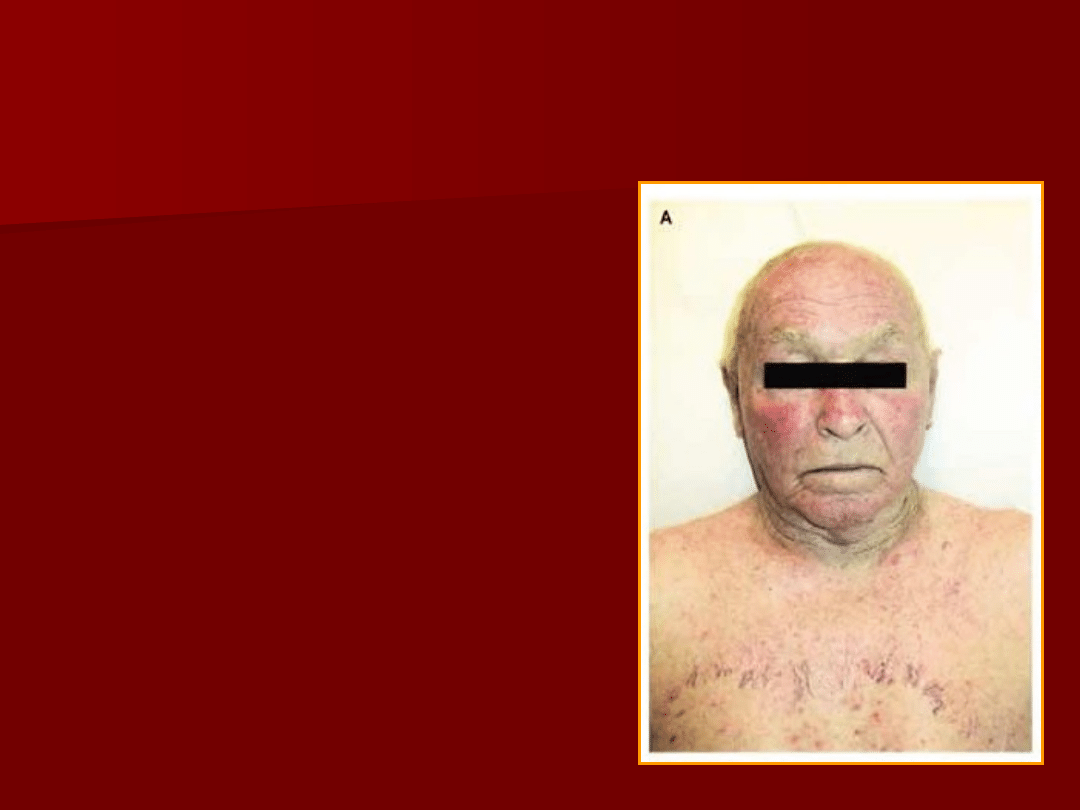
Superior vena cava syndrome
Superior vena cava syndrome
(SVCS)
(SVCS)
The superior vena
The superior vena
cava syndrome is
cava syndrome is
the group of
the group of
symptoms that
symptoms that
result from
result from
compression of the
compression of the
large vein (superior
large vein (superior
vena cava) that
vena cava) that
transmits blood to
transmits blood to
the heart from the
the heart from the
head, neck and
head, neck and
upper extremities.
upper extremities.
Superior vena cava
Superior vena cava
syndrome
syndrome
SVCS is the clinical
manifestation of the SVC
obstruction
– External (mass effect)
– Internal (thrombus)
Etiology
Malignancy (78-85%)
- Lung (small-cell and squamous-
cell histologies, accounts for
~85% off all cases of
malignant origin)
-
Lymphoma => YOUNG
Lymphoma => YOUNG
ADULTS!!
ADULTS!!
- Others (primary mediastinal
germ cell, thymoma)
Infection
Thrombosis

Superior vena cava
Superior vena cava
syndrome
syndrome
Up to 60% with SVCS
will not have prior
cancer diagnosis
History:
-
Dyspnea
-
facial swelling, head fullness,
cough, arm swelling, chest pain,
-
dysphagia,
-
orthopnea,
-
distorted vision,
-
hoarseness,
-
stridor,
-
headache,
-
nasal stuffiness,
-
nausea,
-
light-headedness.
Physical:
Physical:
-
venous distension of the neck
venous distension of the neck
and chest wall,
and chest wall,
-
facial edema,
facial edema,
-
upper extremity edema,
upper extremity edema,
-
mental changes,
mental changes,
-
plethora,
plethora,
-
cyanosis,
cyanosis,
-
papilledema,
papilledema,
-
stupor,
stupor,
-
c
c
oma
oma
-
b
b
ending forward or lying down
ending forward or lying down
may aggravate the symptoms
may aggravate the symptoms
and signs.
and signs.

Superior vena cava
Superior vena cava
syndrome
syndrome
Chest radiographic
findings: widening of
the superior
mediastinum, most
commonly on the right
side.
However, a normal
chest radiographs is
still compatible with
the diagnosis if other
characteristic findings
are present
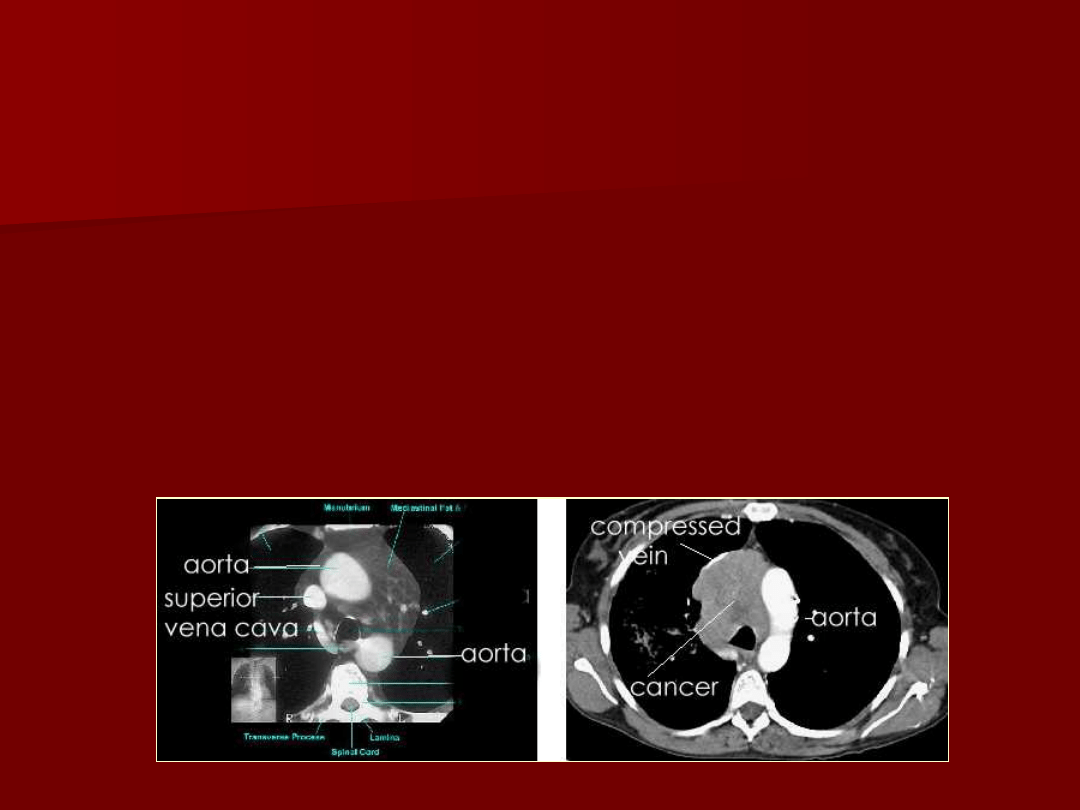
Superior vena cava
Superior vena cava
syndrome
syndrome
Image with CT (MRI if can’t use contrast) –
computed tomography provides the most
reliable view of the mediastinal anatomy.
Tissue diagnosis (bronchoscopy,
percutaneous needle biopsy,
mediastinoscopy, and even thoracotomy)

Superior vena cava
Superior vena cava
syndrome
syndrome
Treatment
Underlying cause:
-
Radiation therapy for SVCS caused by non – small cell lung
cancer and other metastatic solid tumors.
-
Chemotherapy for:
Small cell carcinoma of the lung
Lymphoma
-
Surgery – may provide immediate relief for patients in whom a
benign process is the cause.
-
Corticosteroids
- No benefit in patients with lung cancer
- May be useful at shrinking lymphoma masses
PROGNOSIS:
PROGNOSIS:
-
Clinical improvement - in most patients, although this
improvement may be due to the development of adequate
collateral circulation.
-
The mortality associated with SVCS does not relate to caval
obstruction, but rather to the underlying cause.

Spinal cord compression
Spinal cord compression
D
D
evelops in 1-5% (5-10%) of patients with systemic cancer.
evelops in 1-5% (5-10%) of patients with systemic cancer.
It should be considered as emergency, as
It should be considered as emergency, as
treatment delays
treatment delays
may result in irreversible paralysis and loss of bowel and
may result in irreversible paralysis and loss of bowel and
bladder function
bladder function
.
.
Etiology:
Etiology:
-
Extradural metastases (95%) – usually tumor
Extradural metastases (95%) – usually tumor
involvement of the vertebral column. A tumor may
involvement of the vertebral column. A tumor may
occasionally metastasize to the epidural space without
occasionally metastasize to the epidural space without
bony involvement.
bony involvement.
-
Site of involvement:
Site of involvement:
thoracic spine (70%)
thoracic spine (70%)
lumbosacral spine (20%)
lumbosacral spine (20%)
cervical spine (10%)
cervical spine (10%)
-
Most common malignancies: lung, breast & prostate
Most common malignancies: lung, breast & prostate
cancer, multiple myeloma, lymphomas, melanoma, renal
cancer, multiple myeloma, lymphomas, melanoma, renal
cancer and gastrourinary cancer.
cancer and gastrourinary cancer.
Spinal cord compression –
Spinal cord compression –
history
history
Worsening back pain
Worsening back pain
- in about 90% of adult patients.
- in about 90% of adult patients.
Pain often precedes other symptoms associated with spinal cord
Pain often precedes other symptoms associated with spinal cord
compression by days, weeks to 2-4 months. However, once
compression by days, weeks to 2-4 months. However, once
symptoms other than pain appear, symptom progression may be
symptoms other than pain appear, symptom progression may be
rapid.
rapid.
Pain is exacerbated by movement and by coughing or sneezing.
Pain is exacerbated by movement and by coughing or sneezing.
Radicular pain in the cervical or lumbosacral areas may be
Radicular pain in the cervical or lumbosacral areas may be
unilateral or bilateral.
unilateral or bilateral.
Radicular pain from the thoracic roots is often bilateral and is
Radicular pain from the thoracic roots is often bilateral and is
described by patients as a feeling of tight, band-like constriction
described by patients as a feeling of tight, band-like constriction
around the thorax and abdomen.
around the thorax and abdomen.
Typical cervical radicular pain radiates down the arm; in the lumbar
Typical cervical radicular pain radiates down the arm; in the lumbar
region the radiation is down the legs.
region the radiation is down the legs.
Bladder and bowel disturbances often occur late, with the exception
Bladder and bowel disturbances often occur late, with the exception
of the cauda equina compression syndrome, in which they are an
of the cauda equina compression syndrome, in which they are an
early feature.
early feature.
PATIENTS WITH CANCER WHO DEVELOP BACK
PATIENTS WITH CANCER WHO DEVELOP BACK
PAIN SHOULD BE EVALUATED FOR SPINAL
PAIN SHOULD BE EVALUATED FOR SPINAL
CORD
CORD
COMPRESSION AS QUICKLY AS POSSIBLE.
COMPRESSION AS QUICKLY AS POSSIBLE.

Spinal cord compression
Spinal cord compression
If cord compression is
If cord compression is
suspected the patient
suspected the patient
should be investigated with
should be investigated with
plain spinal radiography,
plain spinal radiography,
which may show evidence
which may show evidence
of lytic lesions (as, for
of lytic lesions (as, for
example, in myeloma).
example, in myeloma).
The definitive investigation
The definitive investigation
is magnetic resonance
is magnetic resonance
imaging to delineate the
imaging to delineate the
level of the lesion and to
level of the lesion and to
help plan further treatment
help plan further treatment
(MRI is to be done in first
(MRI is to be done in first
24 hours)
24 hours)
Spinal Cord Compression
Clinical suspicion:
back pain
back pain
, weakness, motor/sensory
loss,
increased tone, hyperreflexia, loss of sphincter tone
Suspicious for
myelopathy
Symptomatic
treatment
Corticosteroids
10
10
-
-
100 mg bolus
100 mg bolus
,
then 4 mg
qid
Assess pain control
Need for foley
catheter
Review recent bone
scan if available
Radiation oncology
consult
MRI scan
MRI scan
Spinal cord
Spinal cord
compressio
compressio
n present
n present
on MRI
on MRI
scan?
scan?
Urgent radiation oncology
evaluation
Consider neurosurgical
consult for:
- Previously radiated area
- No previous history of
cancer
(for tissue diagnosis)
- Spinal instability or bony
compression of spinal cord
- Radioresistant tumors
(renal, melanoma)
- Neurologic deterioration on
radiation
Yes
No
Yes
No
Reassess patient
Consider other
pathology for spinal
cord dysfunction

Spinal Cord Compression
Radiation therapy plus
Radiation therapy plus
glucocorticoids is generally the initial
glucocorticoids is generally the initial
treatment of choice.
treatment of choice.
Up to 75% of patients treated when
Up to 75% of patients treated when
still ambulatory remain ambulatory,
still ambulatory remain ambulatory,
but only 10% of patients with
but only 10% of patients with
paraplegia recover walking capacity.
paraplegia recover walking capacity.

Hyperviscosity Syndrome
Hyperviscosity Syndrome
Blood viscosity is a function of the
Blood viscosity is a function of the
concentration and composition of its
concentration and composition of its
components. A marked increase in plasma
components. A marked increase in plasma
proteins or cellular constituents (for
proteins or cellular constituents (for
example, white blood cells in acute
example, white blood cells in acute
leukemia) will raise the overall blood
leukemia) will raise the overall blood
viscosity.
viscosity.
Increased serum viscosity
Increased serum viscosity
due to
due to
increased
increased
circulating serum immunoglobulins can be
circulating serum immunoglobulins can be
seen in Waldenström macroglobulinemia
seen in Waldenström macroglobulinemia
(IgM) and multiple myeloma.
(IgM) and multiple myeloma.
Blood viscosity is increased also in:
Blood viscosity is increased also in:
- Pol
- Pol
y
y
cythaemia
cythaemia
- High white cell count (hyperleucocytosis)
- High white cell count (hyperleucocytosis)

Hyperviscosity Syndrome
Hyperviscosity Syndrome
History:
History:
Tendency to bleed is the most common
Tendency to bleed is the most common
symptom of hyperviscosity syndrome.
symptom of hyperviscosity syndrome.
►
►
Spontaneous gum bleeding
Spontaneous gum bleeding
►
►
Epistaxis
Epistaxis
►
►
Rectal
Rectal
bleeding
bleeding
►
►
Menorrhagia
Menorrhagia
►
►
Persistent bleeding
Persistent bleeding
after minor procedures
after minor procedures
Visual changes range from blurred vision to
Visual changes range from blurred vision to
vision loss.
vision loss.
Neurologic manifestations are frequent and
Neurologic manifestations are frequent and
varied. The neurologic symptoms of
varied. The neurologic symptoms of
hyperviscosity have been referred to as the
hyperviscosity have been referred to as the
Bing-Neal syndrome.
Bing-Neal syndrome.
Other manifestations may include heart
Other manifestations may include heart
failure, fatigue, and anorexia.
failure, fatigue, and anorexia.
Hyperviscosity Syndrome
Hyperviscosity Syndrome
Physical:
Physical:
Bruises, epistaxis, or gum bleeding.
Bruises, epistaxis, or gum bleeding.
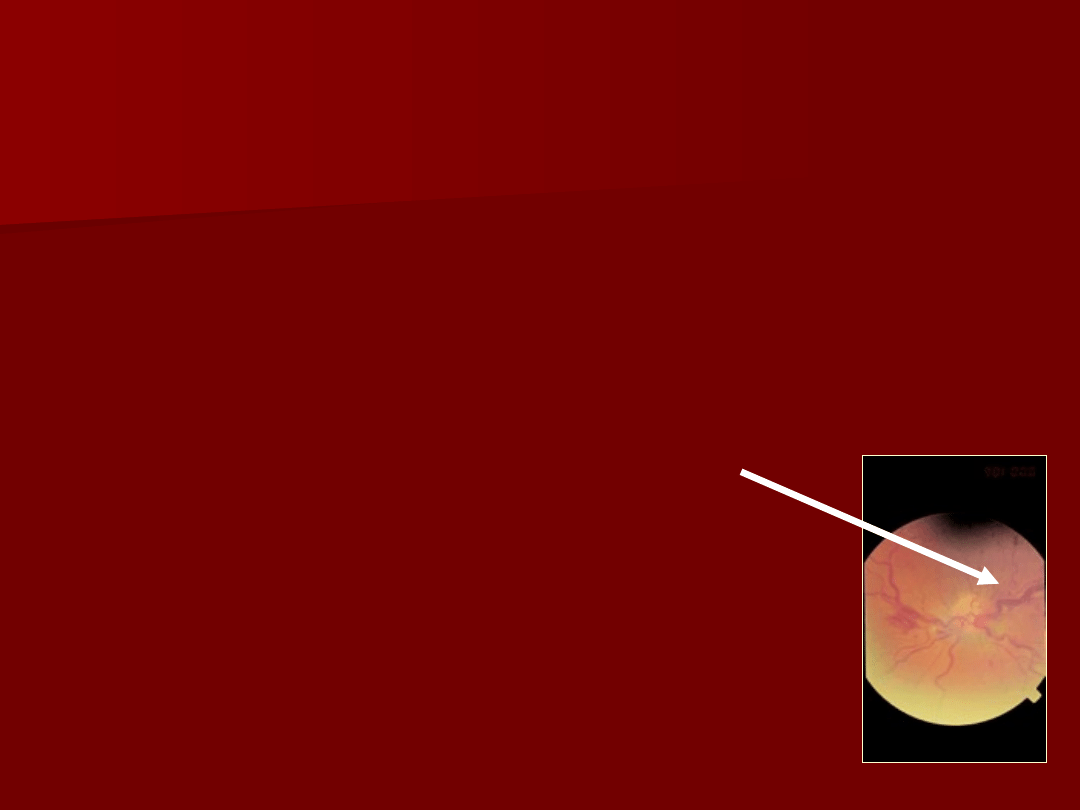
Ophthalmic examination may reveal
Ophthalmic examination may reveal
decreased visual acuity, dilated
decreased visual acuity, dilated
retinal veins, sausage-linked retinal
retinal veins, sausage-linked retinal
veins, or retinal hemorrhages.
veins, or retinal hemorrhages.
Neurological examination may reveal
Neurological examination may reveal
various findings, including
various findings, including
diminished mental status, confusion,
diminished mental status, confusion,
ataxia, or nystagmus
ataxia, or nystagmus
, h
, h
eadaches
eadaches
,
,
s
s
eizures
eizures
, s
, s
omnolence progressing to
omnolence progressing to
stupor and coma.
stupor and coma.
Hyperviscosity Syndrome
Hyperviscosity Syndrome
Lab Studies:
Lab Studies:
Total protein level;
Total protein level;
IgG, IgA,
IgG, IgA,
IgM
IgM
serum
serum
levels.
levels.
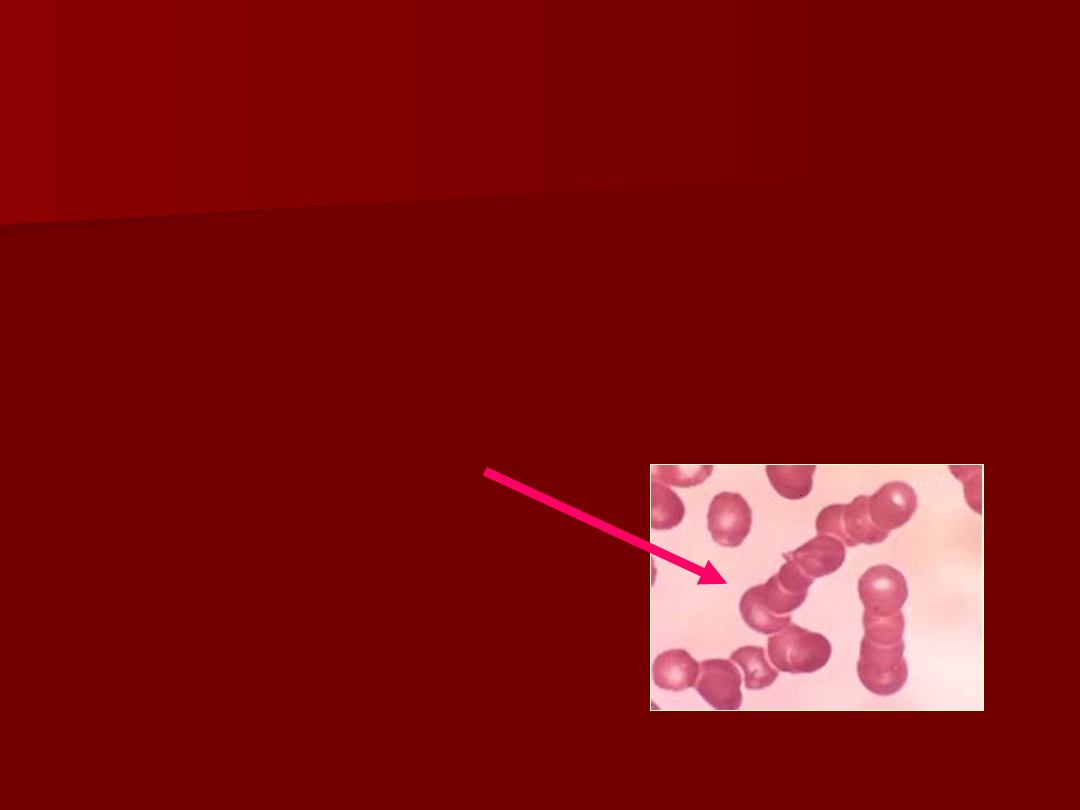
P
P
eripheral blood
eripheral blood
smear.
smear.
Rouleaux
Rouleaux
formation
formation
is often
is often
present with
present with
increased serum
increased serum
viscosity.
viscosity.

Hyperviscosity Syndrome
Hyperviscosity Syndrome
Plasmapheresis is the treatment of
Plasmapheresis is the treatment of
choice for paraproteins related
choice for paraproteins related
hyperviscosity syndrome.
hyperviscosity syndrome.
–
As plasmapheresis removes the circulating
As plasmapheresis removes the circulating
paraproteins, the serum viscosity
paraproteins, the serum viscosity
decreases and symptoms improve.
decreases and symptoms improve.
–
While arranging for plasmapheresis, treat
While arranging for plasmapheresis, treat
hemorrhage, CHF, and metabolic
hemorrhage, CHF, and metabolic
imbalances with standard therapies.
imbalances with standard therapies.

Hyperleukocytosis
Hyperleukocytosis
Definition: peripheral leukocyte count greater
Definition: peripheral leukocyte count greater
than 100,000/mm3 (100 G/L).
than 100,000/mm3 (100 G/L).
Hyperleukocytosis is present at diagnosis in 5-
Hyperleukocytosis is present at diagnosis in 5-
13% of patients with AML, 10-30% of patients
13% of patients with AML, 10-30% of patients
with ALL, and nearly all adults with
with ALL, and nearly all adults with
CML
CML
.
.
Leucocytostasis c
Leucocytostasis can also occur in CLL when
WBC > 400,000/mm3.
Physical findings result from the increased
Physical findings result from the increased
viscosity associated with blast cell aggregates
viscosity associated with blast cell aggregates
and thrombi in combination with damage to
and thrombi in combination with damage to
vessels and secondary hemorrhage. Resultant
vessels and secondary hemorrhage. Resultant
clinical findings primarily include respiratory
clinical findings primarily include respiratory
and neurologic signs.
and neurologic signs.
Hyperleukocytosis
Hyperleukocytosis
Respiratory signs:
Respiratory signs:
-
dyspnea
dyspnea
-
hypoxia.
hypoxia.
Neurologic signs:
Neurologic signs:
-
focal deficit,
focal deficit,
-
ataxia,
ataxia,
-
agitation,
agitation,
-
confusion,
confusion,
-
delirium,
delirium,
-
stupor.
stupor.
Other signs include:
Other signs include:
-
plethora,
plethora,
-
cyanosis,
cyanosis,
-
papilledema, and
papilledema, and
retinal artery or
retinal artery or
retinal vein
retinal vein
distension.
distension.

Hyperleukocytosis
Hyperleukocytosis
Specific antileukemic therapy is the
Specific antileukemic therapy is the
treatment of choice for decreasing the
treatment of choice for decreasing the
peripheral leukocyte count.
peripheral leukocyte count.
PRBC transfusions increase the
PRBC transfusions increase the
viscosity of blood and should be
viscosity of blood and should be
avoided, if possible, in the context
avoided, if possible, in the context
of hyperleukocytosis.
of hyperleukocytosis.
Platelet transfusions do not
Platelet transfusions do not
significantly change the viscosity of
significantly change the viscosity of
circulating blood, and platelets may
circulating blood, and platelets may
be transfused safely if indicated.
be transfused safely if indicated.
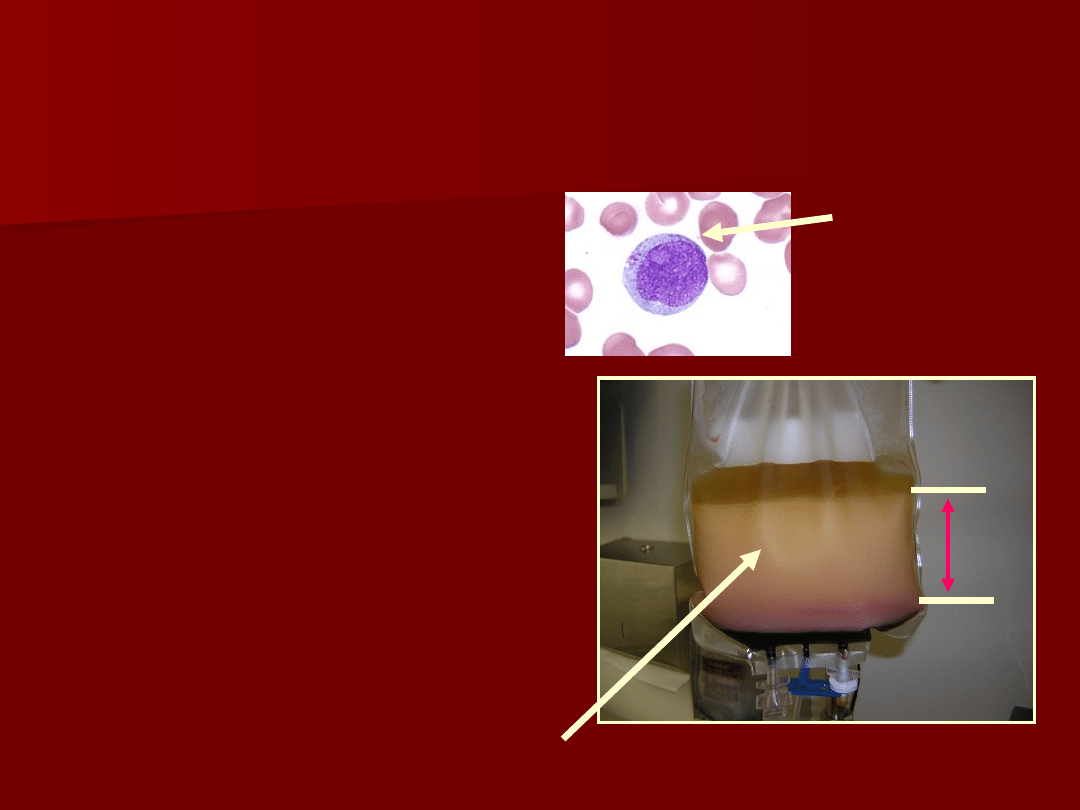
Leukoreduction Apheresis
Leukoreduction Apheresis
(LRA)
(LRA)
The process of
The process of
removing unwanted
removing unwanted
WBC or blasts from the
WBC or blasts from the
circulation
circulation
The procedure is
The procedure is
indicated for the rapid
indicated for the rapid
correction of
correction of
hyperleukocytosis
hyperleukocytosis
.
.
One procedure
One procedure
generally removes
generally removes
between 20-80% of
between 20-80% of
WBC by processing 7-
WBC by processing 7-
10 liters of blood
10 liters of blood
WBC/Blast layer
WBC/Blast layer
Blast cell

Hypercalcemia
It occurs in an estimated 10% to 20% of all
It occurs in an estimated 10% to 20% of all
adults with cancer.
adults with cancer.
Causes
Causes
-
increase in the amount of calcium absorbed
increase in the amount of calcium absorbed
from the bones,
from the bones,
-
and an inability of the kidneys to excrete
and an inability of the kidneys to excrete
excess calcium.
excess calcium.
-
s
s
ome cancer cells secrete substances that
ome cancer cells secrete substances that
cause calcium to be absorbed into the
cause calcium to be absorbed into the
bloodstream from bones.
bloodstream from bones.
-
Immobility, dehydration, anorexia, nausea,
Immobility, dehydration, anorexia, nausea,
and vomiting may also increase calcium levels.
and vomiting may also increase calcium levels.

Hypercalcemia
• History: Advanced
malignancy, especially:
multiple myeloma, breast
cancer, non-small cell lung
cancer
• Symptoms:
- Polydipsia, polyuria
- Anorexia
- Nausea, vomiting
- Lethargy, drowsiness
- Constipation, obstipation
• Signs:
- Dehydration, hypotension
- Hyporefllexia, muscle
weakness, confusion,
seizure, coma
- Ileus
• ECG
- Bradycardia
- Shortened P-R interval
- Shortened Q-T interval
- Wide T-waves
- Supraventrial and
ventricular arrhythmia
Hypercalcemia of Malignancy
Suspect hypercalcemia
Diagnosis
Diagnosis
-Measure blood pressure and heart rate lying and standing (if
possible)
-ECG
-Measure serum calcium, phosphate, albumin, urea, creatinine
-Correct serum calcium
Corrected Ca = measured Ca(mmol/L) + [40 - serum albumin (g/L)] x
0.027
Determine urgency of
treatment
Outpatient-based treatment
Outpatient-based treatment
-Serum calcium < 3.0 mmol/L
-Alert and oriented
-No significant nausea
-Adequate intravascular
volume
-Normal renal function
-No significant ECG
abnormality
-mild constipation
Hospital-based treatment
Hospital-based treatment
-Serum calcium > 3.0 mmol/L
-Altered level of consciousness
-Nausea or vomiting
-Intravascular volume
contraction
-Renal Dysfunction
-Significant ECG abnormality
-obstipation, ileus
Hypercalcemia of Malignancy
Treatment
(treat underlying malignancy when
(treat underlying malignancy when
possible)
possible)
General Measures
General Measures
-Avoid immobilization (if possible)
-Discontinue calcium supplements, vitamin D, cimetidine, NSAIDs,
thiazides
Hospital -based treatment
Hospital -based treatment
- Replacing fluids is the first and most
important step in treating moderate or
severe hypercalcemia.
-Use furosemide 20-40 mg IV if concerns
of volume overload
-Drugs that may help stop the
breakdown of bone include calcitonin,
plicamycin (mithramycin),
bisphosphonates (etidronate,
pamidronate, and clodronate), and
gallium nitrate.
-Steroids and phosphate may also be
used to treat hypercalcemia.
-Dialysis is used in patients with kidney
failure.
-Combinations of drugs may also be
used.
Outpatient-based
Outpatient-based
treatment
treatment
-Maintain adequate oral fluid
intake
-Correct serum phosphate
with oral supplements
-For breast cancer,
lymphomas or myelomas
give prednisone 40-100 mg
PO daily
-Arrange for urgent follow-up
with oncologist
1.
http://www.bccancer.bc.ca/HPI/Chemotherap
yProtocols/SupportiveCare/default.htm
2.Cancer: Principles and Practice of Oncology
(4th ed.) 1997: DeVita S, Hellman S,
Rosenberg S,
ed.. Vol. 2, Section 3 Metabolic
Emergencies:Hypercalcemia, pages 2486-
2493.
Document Outline
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
Wyszukiwarka
Podobne podstrony:
Emergencies in haematology
Emergency Survival Safety Preparations Food And Water In An Emergency
Byrd, emergence of village life in the near east
PBO G 03 C05 Emergency response check list collision in in
Emergency ultrasound in trauma patients Chest in trauma
więcej podobnych podstron