
ORIGINAL ARTICLE
Pain following stroke: A prospective study
A.P. Hansen
1
, N.S. Marcussen
1
, H. Klit
1
, G. Andersen
2
, N.B. Finnerup
1
, T.S. Jensen
1,2
1 Danish Pain Research Center, Aarhus University Hospital, Denmark
2 Department of Neurology, Aarhus University Hospital, Denmark
Correspondence
Anne Petrea Hansen
E-mail: anne.hansen@ki.au.dk
Funding sources
The study has been funded by the Danish
Research Council, the Elsass Foundation and
the Velux Foundation.
Conflicts of interest
None declared.
Accepted for publication
26 January 2012
doi:10.1002/j.1532-2149.2012.00123.x
Abstract
Background: Post-stroke pain is common and affects the quality of life
of stroke survivors, but the incidence and severity of headache, shoulder
pain, other joint pain and central post-stroke pain following stroke still
remain unclear. The aim of this prospective study was to determine the
incidence and intensity of these different types of post-stroke pain.
Methods: A total of 299 consecutive stroke patients, admitted to the
Department of Neurology at Aarhus University Hospital, underwent a
structured interview and a short sensory examination within 4 days of
admission. Follow-up was conducted by phone 3 and 6 months after
stroke onset, with 275 patients completing the whole study. Pain with
onset in relation to stroke onset or following stroke was defined as ‘newly
developed pain’.
Results: At the 6-month follow-up, newly developed pain was reported
by 45.8% of the patients; headache by 13.1%, shoulder pain by 16.4%,
other joint pain by 11.7%, other pain by 20.0% and evoked pain by light
touch or thermal stimuli by 8.0%. More than one pain type was
reported by 36.5% of the patients with newly developed pain. According
to pre-defined criteria, 10.5% of the patients were classified as having
possible central post-stroke pain. There was a moderate to severe impact
on daily life in 33.6% of the patients with newly developed pain.
Conclusions: Pain following stroke is common, with almost half of the
patients reporting newly developed pain 6 months after stroke.
1. Background
Pain is an often overlooked consequence of stroke
although it has been reported in 15–49% of patients
within the first 2 years after stroke (Widar et al., 2002,
2004; Kong et al., 2004; Lundstrom et al., 2009; Naess
et al., 2010). The most common types of post-stroke
pain are headache, shoulder pain and central post-
stroke pain (CPSP). Headache in the acute phase of
stroke has been reported in 27–31% of patients,
depending on the type of stroke (Vestergaard et al.,
1993; Tentschert et al., 2005; Verdelho et al., 2008),
whereas headache with late onset has shown preva-
lence rates of 3.5–11% within the first 2 years (Ferro
et al., 1998; Widar et al., 2002; Jonsson et al., 2006).
Shoulder pain has been reported in 15–40% of patients
within 6 months after stroke (Langhorne et al., 2000;
Gamble et al., 2002; Ratnasabapathy et al., 2003;
Lindgren et al., 2007), and CPSP is seen in 5–11% of
stroke patients (Andersen et al., 1995; Bowsher, 2001;
Weimar et al., 2002; Widar et al., 2002).
The large majority of post-stroke pain studies are
retrospective with different follow-up periods. Few
studies have distinguished between the stroke-affected
side and the unaffected side of the body and only few
studies have tried to differentiate between pre-existing
pain condition and post-stroke pain. Since most
studies focus on only one type of pain, the incidence of
1128
Eur J Pain 16 (2012) 1128–1136 © 2012 European Federation of International Association for the Study of Pain Chapters
the various types of post-stroke pain in the individual
patient is not known. These issues can only be clarified
in a prospective study.
The aim of this prospective study was to examine
the incidence of headache, shoulder pain, other joint
pain, evoked pain and possible CPSP after stroke in
consecutively admitted patients with a 6-month
follow-up and to describe each pain type.
2. Methods
2.1 Patients
All consecutively admitted stroke patients at the
Stroke Unit at the Department of Neurology, Aarhus
University Hospital, between 1 February and 30 Sep-
tember 2007, and 1 February and 31 July 2008, were
considered for inclusion in the study. Inclusion criteria
were a stroke diagnosis (ICD-10 codes: I61, I63, I649,
I676, I677), age over 18 years and informed consent.
Exclusion criteria were a diagnosis of transitory cere-
bral ischaemic attack (G459) or subarachnoid haem-
orrhage (I609), communication problems (e.g. severe
aphasia or dysarthria), severe dementia, somnolence,
lack of consent to participate or lack of Danish lan-
guage skills.
2.2 Primary interview and sensory examination
Eligible patients were included within the first 4 days
of admission. Patients underwent a structured inter-
view. Patients were asked about pain prior to stroke
defined as any persistent or recurring pain within the
last 3 months including description of location, fre-
quency and pain intensity using the numeric rating
scale (NRS 0–10). Then patients were asked about
headache, shoulder pain, other joint pain, touch- or
cold-evoked pain and other pain experienced in close
temporal relation to stroke onset. Information on loca-
tion, frequency, intensity and a description was
obtained for each pain type.
A brief standardized sensory examination was con-
ducted bilaterally on both sides of the body on the
forearm, thenar, cheek, anterior part of the lower leg,
and dorsum of the foot using a brush (Somedic, Hörby,
Sweden), a cotton ball, a thermo roller (20 °C,
Somedic) and No. 5.88 g von Frey monofilament
(Stoelting, Wood Dale, IL, USA). A full neurological
examination was not conducted in relation to the
study. All interviews and examinations were con-
ducted by one of two investigators (N.S.M. and A.P.H.).
All accessible hospital records including the Scandi-
navian Stroke Scale (SSS) score (Lindenstrøm et al.,
1991), imaging results and information on risk factors
were obtained.
2.3 Follow-up interviews
A structured follow-up telephone interview was con-
ducted 3 and 6 months after stroke onset. Patients were
asked if they had experienced any pain during the
previous week. Pain was divided into headache, shoul-
der pain, other joint pain, other pain and pain evoked
by touch or cold/warm stimuli. Dysesthesia did not
qualify as pain. In order to distinguish between pre-
and post-stroke pain, patients were asked specifically
about the onset for each pain type, and this information
was compared with the information about pre-existing
pain given at the time of stroke onset. Pain with onset
in relation to stroke onset or after the stroke with
presence within the last week up to the follow-up was
defined as ‘newly developed pain’ and further classified
as being either in the stroke- or non-stroke-affected
side. Frequency, intensity (NRS 0–10) and description
of each pain type within the previous week were
recorded.
All patients with newly developed pain completed
the 7-item Douleur Neuropathique 4 (DN4) question-
naire (Bouhassira et al., 2005, 2008) with a note on
the specific pain type which the item was related to.
Then they were asked about the impact of pain on
their daily life according to a 4-point scale ranging
from no impact to severe impact and their need for
pain medication within the last week prior to phone
call.
If the patients could not be reached by phone, a
questionnaire about newly developed pain was sent
out with a limited number of questions on newly
developed pain, location, intensity (NRS 0–10) and
description. A reminder was sent out once, and non-
responders were categorized as lost to follow-up.
What’s already known about this topic?
•
Post-stroke pain is common with an incidence of
15–49% within 2 years following stroke.
What does this study add?
•
Post-stroke pain incidence of 45.8% with a
moderate to severe impact on daily life in one of
three patients at a 6-month follow-up.
•
A distinction between different types of pain and
reports on more than one type of pain in 36.5%
at a 6-month follow-up.
A.P. Hansen et al.
Post-stroke pain
1129
Eur J Pain 16 (2012) 1128–1136 © 2012 European Federation of International Association for the Study of Pain Chapters

A short questionnaire on development of pain fol-
lowing stroke was sent out once 6 months after stroke
to the excluded patients from 1 February to 30 Sep-
tember 2007.
2.4 Data analysis
Shoulder pain was defined as pain located to the
shoulder joint and nearby region. Other joint pain was
defined as pain in all other joints than the shoulders.
Reported pain that did not fit into any of the pain
groups was classified as other pain. Moderate to severe
pain was defined as pain with an intensity of 4 or
above on the NRS scale (NRS
ⱖ 4).
Data on all newly developed shoulder pain, other
joint pain, other pain and touch-, heat- or cold-evoked
pain on the stroke-affected side at the 6-month
follow-up were systematically reviewed by two of the
authors (H.K. and A.P.H.). Patients were identified as
having ‘possible CPSP’ [based on the proposed grading
system for CPSP (Klit et al., 2009)] if they fulfilled the
following three criteria: (1) development of pain with
onset at or after the stroke; (2) pain located on the
stroke-affected side of the body; and (3) no other
plausible cause of the pain, including pain isolated to
the shoulder joint and nearby region.
The stroke aetiology was categorized according to
the TOAST classification (TOAST) by two of the
authors (N.S.M. and A.P.H.) (Adams et al., 1993;
Kolominsky-Rabas et al., 2001). Stroke severity was
measured using the SSS (0–58) and a score below 45
was considered to be a severe stroke. The study was
approved by the local ethics committee (ID 20060116)
and the Danish Data Protection Agency (ID 2006-41-
6900) and was conducted in accordance with the Dec-
laration of Helsinki.
2.5 Statistical analysis
Data were analysed with STATA 9.1 software (Stata-
Corp LP, Collage Station, TX, USA). Pearson’s
c
2
test or
Fisher’s exact test was conducted for comparison of
categorical variables. T-test and Wilcoxon rank-sum
were applied for continuous variables. Probability
p-values
< 0.05 were considered significant. Missing
data were less than 3.0%.
3. Results
3.1 Study population
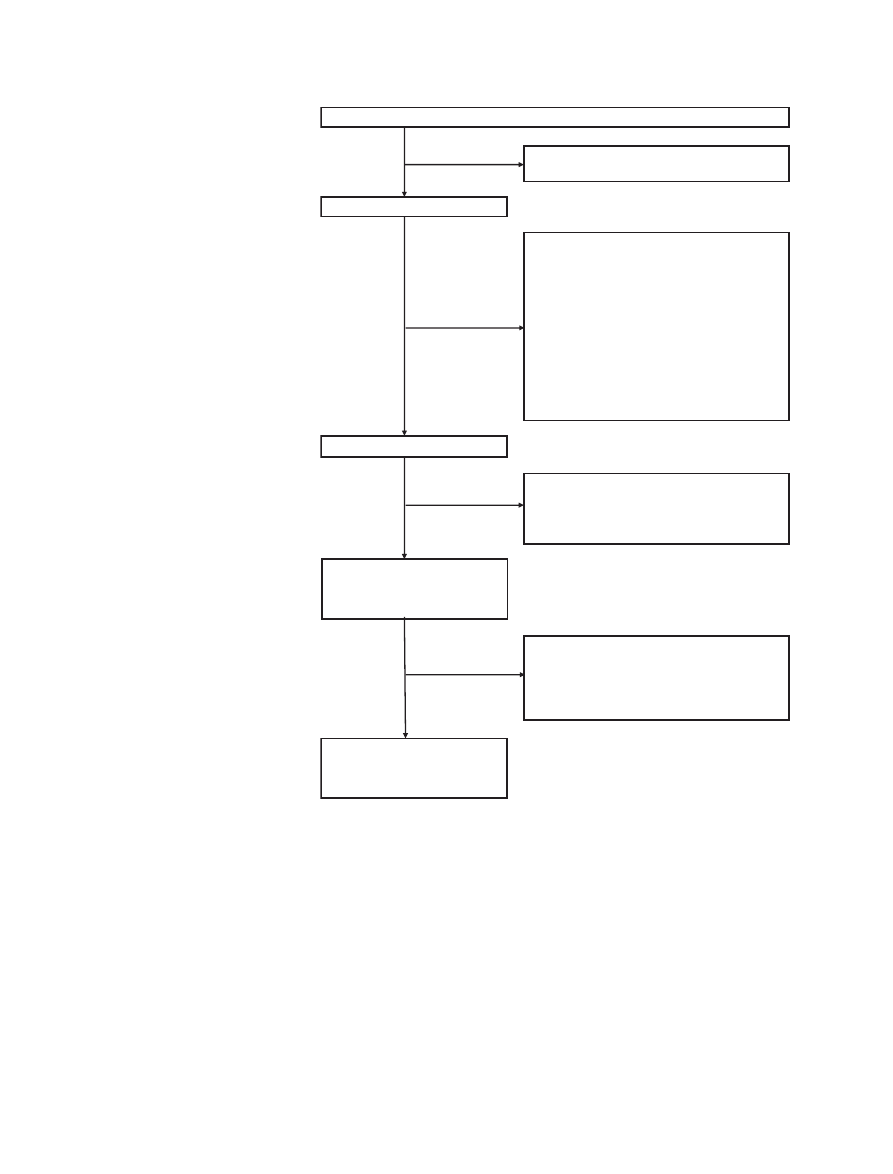
A total of 640 consecutive stroke patients were con-
sidered for inclusion at stroke onset. The stroke diag-
nosis was abandoned in 91 patients and 250 were
excluded, which left 299 patients eligible for inclusion
(Fig. 1).
Included
patients
were
younger
than
excluded patients [mean age 65.9 vs. 71.2 years
(p
< 0.0001)] with no significant difference in gender
(included 55.2% male vs. excluded 47.2% male,
p
= 0.062). The following results are based on the 275
patients who completed both the 3-and 6-month
follow-up; stroke characteristics and risk factors are
presented in Table 1. The median for time of follow-up
at 3 months was 95 days (10th and 90th percentiles:
90–113 days) and 189 days for the 6-month follow-up
(10th and 90th percentiles: 183–225 days).
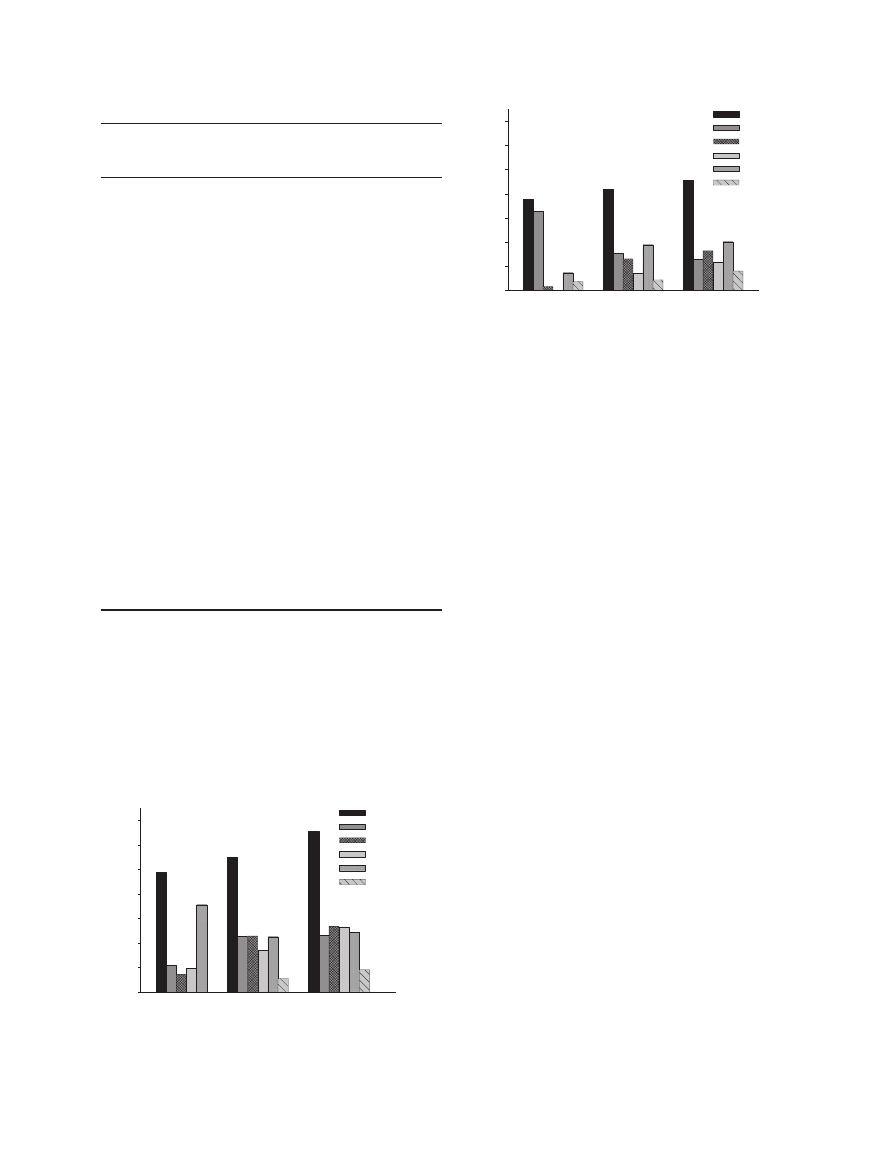
3.2 Pain
Pain within 3 months before the stroke was reported
by 49.1%. Total pain prevalence including all pain,
both pain with onset before stroke and newly devel-
oped pain was 55.3% at 3 months and 65.8% at 6
months (Fig. 2).
3.3 Newly developed pain
The incidence of newly developed pain was 37.8% at
stroke onset, 41.8% at the 3-month follow-up and
45.8% at the 6-month follow-up (Fig. 3). The impact
of newly developed pain on daily life for the patients
from phone interviews was moderate in 20.0% and
severe in 16.4% of patients at 3 months, while mode-
rate in 25.4% and severe in 8.2% at 6 months. A
total of 53.2% of the patients reported usage of pain
medication within the last week and 34.9% on the day
of the phone call at the 3-month follow-up while
52.9% reported usage within the last week and 31.9%
on the day of phone call at the 6-month follow-up.
More than one type of pain was reported by 32.2% of
patients with newly developed pain at 3 months and
by 36.5% at 6 months. At the 6-month follow-up, a
previous history of stroke and of acute myocardial
infarct at stroke onset was more frequent in the group
of patients with newly developed pain (p
= 0.040 and
0.045, respectively), and these patients were younger
than patients without newly developed pain (mean
age 63.3 vs. 67.5 years, p
= 0.008). There was no dif-
ference in sex, stroke type, SSS score, thrombolysis or
other stroke risk factors than above mentioned
between patients with or without newly developed
pain. Pain solely in the stroke-affected side was
reported by 18.9% and 22.6% of all patients at the 3-
and 6-month follow-up.
The questionnaire on newly developed pain sent
out to 145 of the excluded stroke patients from the
Post-stroke pain
A.P. Hansen et al.
1130
Eur J Pain 16 (2012) 1128–1136 © 2012 European Federation of International Association for the Study of Pain Chapters
first inclusion period was returned by 42 patients.
Compared with the 45.8% of the included patients
reporting newly developed pain in this study, 35.7%
(15/42) of the excluded patients reported newly
developed pain 6 months after stroke (non-significant
difference p
= 0.220).
3.4 Headache
A total of 10.9% of the patients reported having
experienced persistent or recurrent headache 3
months prior to stroke. Headache with onset in close
temporal relation to stroke was experienced by
33.5%. The probability of reporting headache at
stroke onset if having experienced headache prior to
stroke was 20.0%, and only 6.5% if not having
experienced
headache
prior
to
stroke.
Patients
reporting headache at stroke onset were younger
(mean age 62.5 vs. 67.2 years, p
= 0.0061) and more
likely to be women (60% vs. 36.7%, p
< 0.0001) as
compared with patients without headache. Headache
at stroke onset was more common with large-artery
disease or cardio-embolism as compared with small
vessel occlusion (p
= 0.034). No relation between
Patients considered for inclusion between February 1, 2007 and July 31, 2008,
n=640
Eligible patients,
n= 549
Excluded patients,
n=250
- 55 due to communication problems (e.g.
aphasia)
- 56 due to weariness or loss of consciousness
- 16 due to lack of knowledge of the Danish
language
- 18 due to declination to participate
- 57 not possible to examine on 0-3 days of
admission
- 48 due to other causes (Alzheimer’s disease,
instrument problems, deceased before
examination, etc.)
Included at stroke onset,
n=299
Non-eligible patients,
n=91
- Due to desertion of stroke diagnosis
3-month follow-up,
n =282
-263 by phone interview
-19 by letter with questionnaire
Lost to follow-up at 3-month follow-up,
n =17
-7 deceased
-7 non-responders
-3 various reasons
Lost to follow-up at 6-month follow-up,
n =7
-3 deceased
-2 non-responders
-2 various reasons
6-month follow-up,
n =275
-260 by phone interview
-15 by letter with questionnaire
Figure 1 Flow chart of patients.
A.P. Hansen et al.
Post-stroke pain
1131
Eur J Pain 16 (2012) 1128–1136 © 2012 European Federation of International Association for the Study of Pain Chapters
haemorrhage and headache at stroke onset was
found (p
= 0.66).
Headache was reported by 23.0% at 3 months and
23.4% at 6 months, and newly developed headache
was reported by 15.3% (NRS
ⱖ 4: 64.3%) and 13.1%
(NRS
ⱖ 4: 66.7%), respectively. See Table 2 for
further characteristics. The main descriptor of newly
developed headache was pressing, reported by 44.4%
at stroke onset, 43.0% at 3 months and 58.3% at 6
months. Movement did not induce or aggravate head-
ache in 73.8% and 66.7% of patients at the 3- and
6-month follow-up, respectively. Patients with newly
developed headache were younger than patients
without headache (p
< 0.05), but there was no gender
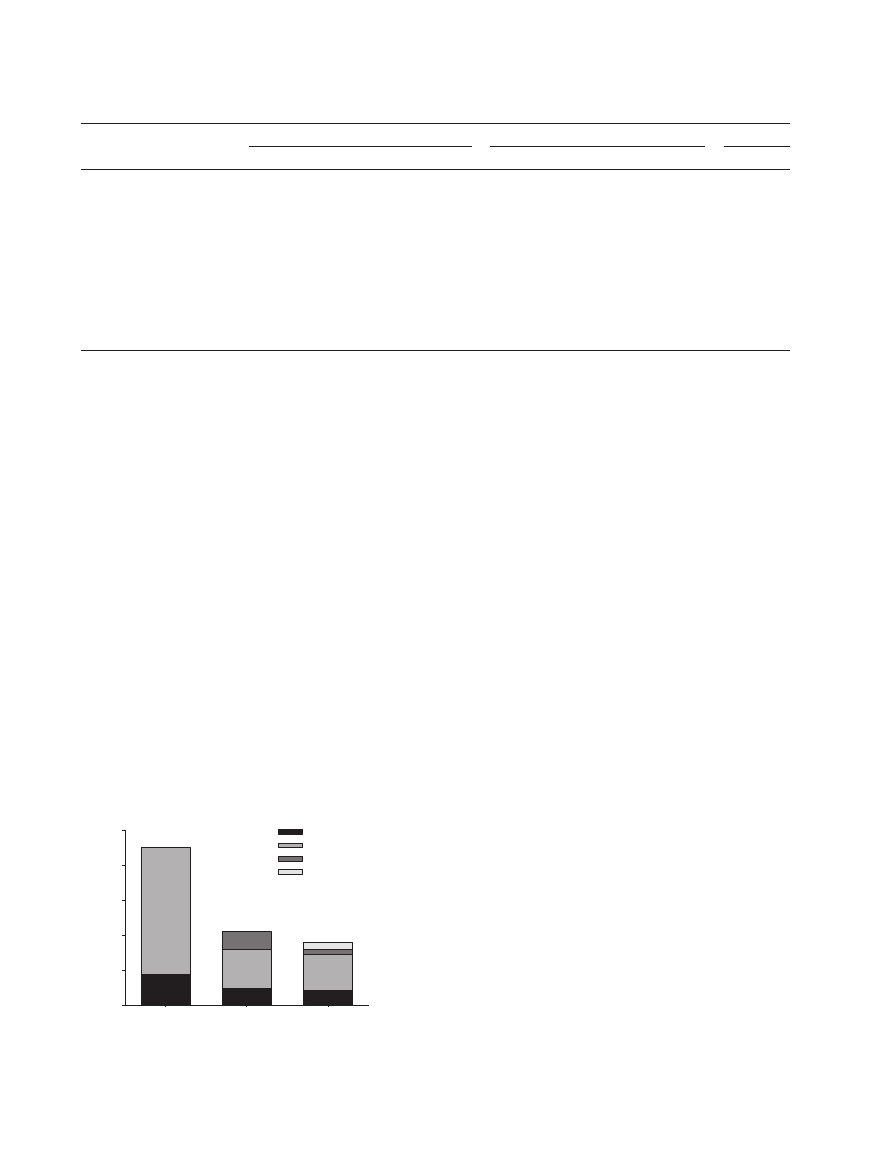
difference. The time of headache onset is depicted in
Fig. 4 and the likelihood of continued newly devel-
oped headache at 3-month follow-up was 69.0% and
70.3% at 6-month follow-up in patients with head-
ache at stroke onset. Accordingly, headache at stroke
onset was correlated to the presence of headache at 6
months (p
< 0.001).
3.5 Shoulder pain
The incidence of shoulder pain was 7.3% before
stroke, 22.9% at 3 months and 26.9% at 6 months
after stroke. Newly developed shoulder pain was
present in 1.5% at stroke onset, 13.1% at 3 months
and 16.4% at 6 months. Of those with shoulder pain
at 3-month follow-up, the probability of still reporting
this pain at 6-month follow-up was 48.9%. There was
no difference in age or gender between patients with
and without newly developed shoulder pain at follow-
up. Newly developed shoulder pain in the stroke-
affected side was reported by 10.2% at 3 months (NRS
ⱖ4: 71.4%) and 12.0% at 6 months (NRS ⱖ 4:
75.8%). The shoulder pain in the stroke-affected side
was aggravated or induced by movement in 71.4% at
the 3-month follow-up and in 71.9% at the 6-month
follow-up. Further characteristics are displayed in
Table 2. There was no association between stroke
severity (SSS
< 45) on admission and the development
of shoulder pain in the stroke-affected side at 3-month
Table 1 Stroke characteristics and risk factors at stroke onset.
Patients who
completed study
n
= 275
Sex, male, % (n/N)
55.6 (153/275)
Age, mean (range) years
65.6 (24–92)
Stroke type, % (n/N)
Infarct
90.5 (249/275)
Haemorrhage
9.5 (26/275)
Toast classification, % (n/N)
Large-artery atherosclerosis
12.9 (32/249)
Cardio-embolism
19.7 (49/249)
Small vessel occlusion/lacunar
38.1 (95/249)
Stroke of other determined etiology
4.8 (12/249)
Stroke of undetermined etiology
23.3 (58/249)
Not enough information to classify
1.2 (3/249)
SSS (n
= 205), median (range)
51 (2–58)
Thrombolysis, % (n/N)
17.6 (48/273)
Diabetes, % (n/N)
15.0 (34/227)
Hypertension, % (n/N)
64.2 (145/226)
Atrial fibrillation, % (n/N)
12.7 (25/197)
History of acute myocardial infarction, % (n/N)
8.0 (21/262)
Intermittent claudication, % (n/N)
6.6 (16/242)
Prior stroke, % (n/N)
17.9 (47/263)
Prior TIA (transient ischemic attack), % (n/N)
7.6 (19/249)
Alcohol,
>14 and 21 (women and men)
units/week, % (n/N)
10.6 (29/275)
Smoker, % (n/N)
Current
40.7 (112/275)
Prior
32.0 (88/275)
Never
27.3 (75/275)
SSS, Scandinavian Stroke Scale.
Percentage
0
10
20
30
40
50
60
70
Total
Headache
Shoulder pain
Joint pain
Other pain
Evoked pain
Prior
3-month
6-month
Figure 2 Prevalence of pain 3 months before stroke not including evoked
pain and within the week leading up to the follow-up interviews.
Pe
rcentage
0
10
20
30
40
50
60
70
Total
Headache
Shoulder pain
Joint pain
Other pain
Evoked pain
Onset
3-month
6-month
Figure 3 Incidence of newly developed pain at stroke onset and within
the week leading up to the follow-up interviews.
Post-stroke pain
A.P. Hansen et al.
1132
Eur J Pain 16 (2012) 1128–1136 © 2012 European Federation of International Association for the Study of Pain Chapters
(p
= 0.348) and 6-month (p = 0.084) follow-up.
Detailed information on arm function was otherwise
not available. At the 6-month follow-up, 57.6% of the
patients described their shoulder pain on the stroke-
affected side as a deep pain while the pain was
described as both deep and superficial by 21.2%.
3.6 Other joint pain
Other joint pain was reported by 9.8% of the patients
prior to the stroke. None of the patients reported other
joint pain at stroke onset, while 17.1% had other joint
pain at 3 months and 26.6% at 6 months. A minority
of the patients reported newly developed other joint
pain: 7.4% at 3 months and 11.7% at 6 months. The
newly developed other joint pain at 6 months was
located on the hips (21.9%), knees (21.9%), finger
joints (15.6%), elbows (12.5%), feet (9.4%), pelvis
(6.3%), leg (6.3%), wrists (3.1%) and back (3.1%).
Only 1.8% had joint pain solely in the stroke-affected
side at 3-month follow-up (NRS
ⱖ 4: 100%) and
5.1% at 6-month (NRS
ⱖ 4: 85.7%) follow-up.
3.7 Other pain
Other pain was reported by 35.6% before stroke, 7.3%
at stroke onset, 22.2% at 3 months, and 24.0% at 6
months. Newly developed other pain was reported by
18.9% at 3 months and 20.0% at 6 months, and this
pain was on the stroke-affected side in 8.4%
(NRS
ⱖ 4: 87.0%) and 8.9% (NRS ⱖ 4: 75.0%),
respectively.
3.8 Evoked pain
Pain evoked by light touch or cold stimuli was
reported by 3.6% during the interview at stroke onset.
At the follow-up interviews, light touch, cold or warm
stimuli was reported by 5.5% and 9.1%, respectively,
at 3-month and 6-month follow-up. The evoked pain
was reported to be newly developed by 4.4% at
3-month follow-up (NRS
ⱖ 4: 91.0%) and 8.0% at
6-month follow-up (NRS
ⱖ 4: 72.7%). A total of 3.6%
reported evoked pain in the stroke-affected side at
the 3-month follow-up and 5.5% at the 6-month
follow-up.
Table 2 Overview of newly developed headache, shoulder pain on the stroke-affected side and possible CPSP.
Headache
Shoulder pain on the stroke-affected side
Possible CPSP
Onset
3-month
6-month
Onset
3-month
6-month
6-month
Total, n (%)
90 (33.5)
42 (15.3)
36 (13.1)
3 (1.1)
28 (10.2)
33 (12.0)
29 (10.6)
Male, n (%)
36 (40.0)
a
21 (50.0)
17 (48.6)
2 (66.7)
15 (53.6)
18 (54.6)
11 (37.9)
a
Age, mean (range)
62.5 (24–87)
b
61.4 (33–86)
b
60.7(30–86)
b
59.7 (49–67)
62.8 (33–86)
61.9 (33–80)
60.4 (39–76)
b
Frequency, n (%)
Constantly
57 (63.3)
4 (9.5)
4 (11.1)
0 (0.0)
5 (17.8)
6 (19.4)
6 (26.1)
c
Daily
–
13 (31.0)
9 (25.0)
–
14 (50.0)
16 (51.6)
16 (59.3)
c
ⱖTwice a week
–
12 (28.5)
12 (33.3)
–
8 (28.6)
8 (25.8)
4 (14.8.)
c
ⱕTwice a week
–
13 (31.0)
11 (30.6)
–
1 (3.6)
1 (3.2)
1 (3.7)
c
Pain intensity, NRS (0–10)
Median (range)
4 (0–9)
d
5 (1–8)
e
5 (1–10)
e
1 (0–3)
5 (2–10)
e
4.5 (1–9)
e
5 (1–10)
e
Movement induced/aggravation
–
11 (26.2)
12 (33.3)
–
20 (71.4)
23 (71.9)
–
CPSP, central post-stroke pain; NRS, numeric rating scale.
a
Significantly more women than men with pain (p
< 0.05).
b
Significantly younger patients with pain than patients without pain (p
< 0.05).
c
Only patients from phone interviews.
d
Intensity within the last 4 h prior to interview. Only including the 70 patients still having headache at interview time and including one patient who scored
a constant headache at 0 on the NRS.
e
Intensity within the last 1 week leading up to phone interview.
Stroke onset
3-month
6-month
Nu
mber
of p
atie
nts
0
20
40
60
80
100
Prior to stroke
At stroke onset
Between 0 and 3 months
Between 3 and 6 months
Onset of headache:
Figure 4 Time of headache onset.
A.P. Hansen et al.
Post-stroke pain
1133
Eur J Pain 16 (2012) 1128–1136 © 2012 European Federation of International Association for the Study of Pain Chapters

3.9 Central post-stroke pain
Possible CPSP was identified in 10.5% (NRS
ⱖ 4:
75.9%). Further characteristics are displayed in
Table 2. Patients with possible CPSP were more often
women (p
= 0.042), and they were slightly younger
than the remaining patients (mean age 60.4 vs. 66.2
years, p
= 0.025). The pain was located in the upper
extremity in 37.9%, the lower extremity in 20.7%, in
both upper and lower extremities in 10.3%, in the
head in 16.0%, in both head and lower extremity in
3.4%, and in one entire side of the body in 10.3%. The
pain was spontaneous in 65.5% of the patients with
possible CPSP, both spontaneous and evoked in
20.7%, and solely evoked in 13.8%. The DN4 scale
was applied on the 27 patients who were followed up
by phone and a score of 3 or more on the 7-item DN4
concerning items related to the possible CPSP was
found in 48.1% of these patients. The item pins and
needles was experienced by 63.0.%, tingling by 48.1%,
burning by 29.6%, numbness by 37.0%, while electric
shocks, painful cold and itching were experienced by less
than 20% of the patients with possible CPSP.
4. Discussion
To our knowledge, this study is the first to examine the
incidence of all common pain types following stroke in
a prospective study with 3-month and 6-month
follow-up interviews. Since we did not include a
control group, we cannot determine how much of the
pain is attributed to the stroke. Nevertheless, the fact
that two-thirds of all stroke patients reported pain 6
months after stroke and nearly half of the patients with
pain reported the pain to be newly developed indicates
that pain is an important consequence of stroke.
In a retrospective study, Naess et al. (2010) found
that 44.6% had post-stroke pain 1 year after stroke,
similar to the 45.8% at 6 months found in this study.
Lundstrom et al. (2009) found stroke-related pain
defined as pain that started after stroke and was
located in the paretic side of the body in 21% 1 year
after stroke, which corresponds to our 22.6% of
patients with pain in the stroke-affected side at 6
months. Thus, our study indicates a high incidence of
newly developed already 6 months after stroke.
The high incidence of headache at stroke onset in
one-third of the patients is similar to the 27% with
headache in relation to stroke found by Vestergaard
et al. (1993). The patients with headache in our study
were younger at stroke onset and more often female,
which is consistent with other studies (Tentschert et al.,
2005). Patients were asked about prior headache at the
time of their stroke where other major symptoms and
signs may have obscured the perception of headache or
the likelihood to report that symptom leading to a
possible underestimation. Headache at stroke onset
was a predictor for headache 6 months after stroke. Our
results indicate that headache following stroke gener-
ally resembles a tension-type headache with the main
description of the headache being pressing, not aggra-
vated by movement and with a moderate intensity
(mean NRS 4–5), in consistency with previous studies
(Vestergaard et al., 1993; Widar et al., 2002).
Newly developed shoulder pain was reported by
16.4% (45/275) at 6 months and the majority of these
patients (33) had pain in the stroke-affected side. The
underlying mechanisms of shoulder pain and its rela-
tion to stroke are not examined in this study but have
previously been associated with paresis, abnormal
joint postures, muscle overuse or nerve damage
(Gamble et al., 2002; Roosink et al., 2011).
Possible CPSP was suspected in 10.5%. This figure of
CPSP is slightly higher than the incidence of 8.0%
reported by Andersen et al. (1995) and the incidence of
7.3% reported by Klit et al. (2011). Half of the patients
with possible CPSP (48.1%) had a DN4 score
ⱖ 3,
which may indicate a low sensitivity. However, we are
not in a position based on the present results to deter-
mine the sensitivity or specificity of the DN4 to detect
neuropathic pain. The sensitivity and specificity of the
DN4 to detect neuropathic pain has been found to be
much higher in other studies (Bouhassira et al., 2005).
In the present study, we have only used a telephone
interview and only included items that were reported
in an area in close proximity to the area of the possible
CPSP to classify the pain. Therefore, it is likely that the
DN4 score would be higher if the patient sample was
restricted to patients with probable or definite CPSP. We
are currently carrying out a detailed examination
including a DN4 questionnaire of these patients with
possible CPSP to find out who has definite or probable
neuropathic pain (Klit et al., manuscript in prepara-
tion). We cannot exclude that some of the patients
classified with shoulder pain in fact have CPSP, and the
incidence of possible CPSP would have been 13.5% if
patients with shoulder pain fulfilling the pre-defined
criteria for CPSP were included (Klit et al., 2011;
Roosink et al., 2010).
We believe that the reason for the negative trend of
the development of shoulder pain and CPSP at
follow-up interviews in relation to stroke onset is that
these pain types develop over time whereas headache
often starts simultaneously with stroke. The preva-
lence of CPSP may be underestimated in this study
due to the relatively short follow-up period.
Post-stroke pain
A.P. Hansen et al.
1134
Eur J Pain 16 (2012) 1128–1136 © 2012 European Federation of International Association for the Study of Pain Chapters

Forty-five percent of the consecutively admitted
patients were not included in the studies due mainly
to aphasia, dementia, weariness and loss of conscious-
ness. Therefore, our result may not be representative
for a non-selected group of stroke patients. However,
an analysis of excluded patients suggested similar inci-
dence of newly developed pain as in the included
patients.
Part of the reported pain in this study might be
attributed to other factors, e.g. cardiovascular disease
with the higher incidence of previous stroke and acute
myocardial infarction in the patients with newly deve-
loped pain. Prior post-stroke pain might be an influence
on reported pain and be a potential pre-existing pain
condition which involves 17.9% of the patients. In this
study, we have explicitly concentrated on newly devel-
oped pain after the actual stroke and therefore believe
that a former stroke-related pain condition does not
have a major influence on the present results. Another
factor for influencing reported pain is treatment with
dipyridamole (Persantine®) inducing a newly deve-
loped headache in the patients with headache at the
follow-up interviews.
The strength of our study is its prospective character
and that it distinguishes between pain before stroke
and pain after stroke by questioning the patients about
pre-existing pain at the time of admission. Since we
asked for pain during the previous 3 months, we cannot
exclude some recall bias for this parameter and it is
possible that patients may neglect some of their prior
pain when submitted to a hospital for a critical illness.
Recall bias at follow-up was minimized by asking the
patients about their pain in the last week before the
interviews. However, the narrow time frame makes it
impossible to classify the pain as chronic pain.
5. Conclusion
The high incidence of pain following stroke suggests
that pain in stroke survivors should be recorded,
analysed and managed if severe. Patients may have
more than one type of pain which could complicate
their rehabilitation.
References
Adams, H.P., Jr, Bendixen, B.H., Kappelle, L.J., Biller, J., Love,
B.B., Gordon, D.L., Marsh, E.E., 3rd. (1993). Classification of
subtype of acute ischemic stroke. Definitions for use in a
multicenter clinical trial. TOAST. Trial of Org 10172 in Acute
Stroke Treatment. Stroke 24, 35–41.
Andersen, G., Vestergaard, K., Ingeman-Nielsen, M., Jensen, T.S.
(1995). Incidence of central post-stroke pain. Pain 61, 187–
193.
Bouhassira, D., Attal, N., Alchaar, H., Boureau, F., Brochet, B.,
Bruxelle, J., (2005). Comparison of pain syndromes associated
with nervous or somatic lesions and development of a new
neuropathic pain diagnostic questionnaire (DN4). Pain 114,
29–36.
Bouhassira, D., Lanteri-Minet, M., Attal, N., Laurent, B.,
Touboul, C. (2008). Prevalence of chronic pain with neuro-
pathic characteristics in the general population. Pain 136,
380–387.
Bowsher, D. (2001). Stroke and central poststroke pain in an
elderly population. J Pain 2, 258–261.
Ferro, J.M., Melo, T.P., Guerreiro, M. (1998). Headaches in
intracerebral hemorrhage survivors. Neurology 50, 203–
207.
Gamble, G.E., Barberan, E., Laasch, H.U., Bowsher, D., Tyrrell,
P.J., Jones, A.K. (2002). Poststroke shoulder pain: a prospec-
tive study of the association and risk factors in 152 patients
from a consecutive cohort of 205 patients presenting with
stroke. Eur J Pain 6, 467–474.
Jonsson, A.C., Lindgren, I., Hallstrom, B., Norrving, B.,
Lindgren, A. (2006). Prevalence and intensity of pain after
stroke: a population based study focusing on patients’ perspec-
tives. J Neurol Neurosurg Psychiatry 77, 590–595.
Klit, H., Finnerup, N.B., Andersen, G., Jensen, and T.S. (2011).
Central poststroke pain: A population-based study. Pain 152,
818–824.
Klit, H., Finnerup, N.B., Jensen, T.S. (2009). Central post-stroke
pain: clinical characteristics, pathophysiology, and manage-
ment. Lancet Neurol 8, 857–868.
Kolominsky-Rabas, P.L., Weber, M., Gefeller, O., Neundoerfer,
B., Heuschmann, P.U. (2001). Epidemiology of ischemic
stroke subtypes according to TOAST criteria: incidence, recur-
rence, and long-term survival in ischemic stroke subtypes: a
population-based study. Stroke 32, 2735–2740.
Kong, K.H., Woon, V.C., Yang, S.Y. (2004). Prevalence of chronic
pain and its impact on health-related quality of life in stroke
survivors. Arch Phys Med Rehabil 85, 35–40.
Langhorne, P., Stott, D.J., Robertson, L., MacDonald, J., Jones,
L., McAlpine, C., Dick, F., Taylor, G.S., Murray, G. (2000).
Medical complications after stroke: a multicenter study. Stroke
31, 1223–1229.
Lindenstrøm, E., Boysen, G., Christiansen, L.W., Hansen, B.R.,
Nielsen, P.W. (1991). Reliability of Scandinavian neurological
stroke scale. Cerebrovasc Dis 1, 103–107.
Lindgren, I., Jonsson, A.C., Norrving, B., Lindgren, A. (2007).
Shoulder pain after stroke: a prospective population-based
study. Stroke 38, 343–348.
Lundstrom, E., Smits, A., Terent, A., Borg, J. (2009). Risk factors
for stroke-related pain 1 year after first-ever stroke. Eur J
Neurol 16, 188–193.
Naess, H., Lunde, L., Brogger, J., Waje-Andreassen, U. (2010).
Post-stroke pain on long-term follow-up: the Bergen stroke
study. J Neurol 257, 1446–1452.
Ratnasabapathy, Y., Broad, J., Baskett, J., Pledger, M., Marshall,
J., Bonita, R. (2003). Shoulder pain in people with a stroke: a
population-based study. Clin Rehabil 17, 304–311.
Roosink, M., Geurts, A.C., Ijzerman, M.J. (2010). Defining post-
stroke pain: diagnostic challenges. Lancet Neurol 9,344; author
reply 344–345.
Roosink, M., Renzenbrink, G.J., Buitenweg, J.R., van Dongen,
R.T., Geurts, A.C., Ijzerman, M.J. (2011). Somatosensory
symptoms and signs and conditioned pain modulation in
chronic post-stroke shoulder pain. J Pain 12, 476–485.
A.P. Hansen et al.
Post-stroke pain
1135
Eur J Pain 16 (2012) 1128–1136 © 2012 European Federation of International Association for the Study of Pain Chapters

Tentschert, S., Wimmer, R., Greisenegger, S., Lang, W.,
Lalouschek, W. (2005). Headache at stroke onset in 2196
patients with ischemic stroke or transient ischemic attack.
Stroke 36, e1–e3.
Verdelho, A., Ferro, J.M., Melo, T., Canhao, P., Falcao, F. (2008).
Headache in acute stroke. A prospective study in the first 8
days. Cephalalgia 28, 346–354.
Vestergaard, K., Andersen, G., Nielsen, M.I., Jensen, T.S. (1993).
Headache in stroke. Stroke 24, 1621–1624.
Weimar, C., Kloke, M., Schlott, M., Katsarava, Z., Diener, H.C.
(2002). Central poststroke pain in a consecutive cohort of
stroke patients. Cerebrovasc Dis 14, 261–263.
Widar, M., Ek, A.C., Ahlstrom, G. (2004). Coping with long-term
pain after a stroke. J Pain Symptom Manage 27, 215–225.
Widar, M., Samuelsson, L., Karlsson-Tivenius, S., Ahlstrom, G.
(2002). Long-term pain conditions after a stroke. J Rehabil Med
34, 165–170.
Post-stroke pain
A.P. Hansen et al.
1136
Eur J Pain 16 (2012) 1128–1136 © 2012 European Federation of International Association for the Study of Pain Chapters

Copyright of European Journal of Pain is the property of Wiley-Blackwell and its content may not be copied or
emailed to multiple sites or posted to a listserv without the copyright holder's express written permission.
However, users may print, download, or email articles for individual use.
Wyszukiwarka
Podobne podstrony:
Pain Following Stroke A Population Based Follow Up Study
Pain following stroke, initially and at 3 and 18 months after stroke, and its association with other
Ebsco Bialosky Manipulation of pain catastrophizing An experimental study of healthy participants
Ebsco Bialosky Manipulation of pain catastrophizing An experimental study of healthy participants
Chronic Pain Syndromes After Ischemic Stroke PRoFESS Trial
Evidence for Therapeutic Interventions for Hemiplegic Shoulder Pain During the Chronic Stage of Stro
Prospective Demographic Study
Chronic Pain Syndromes After Ischemic Stroke PRoFESS Trial
Changes in Negative Affect Following Pain (vs Nonpainful) Stimulation in Individuals With and Withou
Effect of sensory education on school children’s food perception A 2 year follow up study
Badania obserwacyjne prospektywne (kohortowe)
A Behavioral Genetic Study of the Overlap Between Personality and Parenting
Aneks nr 2 Prospekt PKO BP 05 10 2009
CEREBRAL VENTICULAR ASYMMETRY IN SCHIZOPHRENIA A HIGH RESOLUTION 3D MR IMAGING STUDY
więcej podobnych podstron