Management
Dilemmas in Cervical
Cancer
02-11-02
03:24 A
M
Management Dilemmas in Cervical Cancer- Prof. S.N.Panda
2
Cervical Cancer
• 500,000 new cases identified each year
• 80% of the new cases occur in
developing countries
• At least 200,000 women die of cervical
cancer each year
• Cervical cancer is the third most
common cancer worldwide
• YET - Cervical cancer is a preventable
disease
Magnitude of the Problem: -
Please see notes
page.
02-11-02
03:24 A
M
Management Dilemmas in Cervical Cancer- Prof. S.N.Panda
3
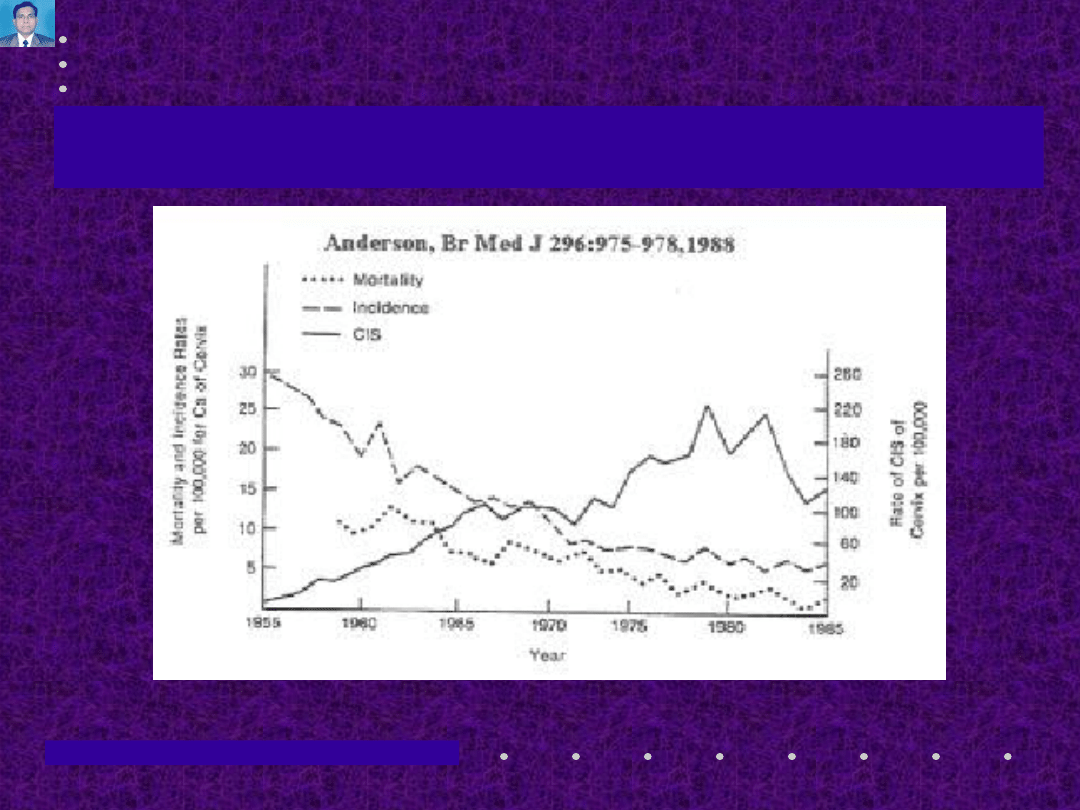
Cervical Cancer
Incidence and Death in relation to
Incidence and Death in relation to
detection of CIS
detection of CIS
*Please see notes
page..
02-11-02
03:24 A
M
Management Dilemmas in Cervical Cancer- Prof. S.N.Panda
4
Cervical Cancer
• Symptoms: -
– Asymptomatic in early cases/ preclinical
stage
– Haemorrhage- Metrorrhagia / Post coital.
• Bleeding is usually severe in cauliflower like
exophytic growths.
– Discharge- watery, offensive, blood
stained
– Cachexia and Pain-In advanced cases.
Clinical Features: -
02-11-02
03:24 A
M
Management Dilemmas in Cervical Cancer- Prof. S.N.Panda
5
Cervical Cancer
• Signs: -
– An obvious growth may or may not be
present
– When an obvious growth is present, it may
be exophytic cauliflower like or endophytic,
ulcerative and scirrhous
– Cervix is usually indurated and hard to
feel, friable, easily bleeds on touch and its
mobility may be restricted or lost.
– In cases of endocervical growths, the Cx is
expanded, firm and feels barrel shaped.
Clinical Features: -
02-11-02
03:24 A
M
Management Dilemmas in Cervical Cancer- Prof. S.N.Panda
6
Cervical Cancer
• PAP smear examination
• Colposcopy
• Biopsy: -
– Excisional biopsy is preferable to punch
biopsy
– Employing Schiller’s test / Acetic acid test
helps in selecting the biopsy site where
the growth is not obvious.
– Cone biopsy in early cases
• Endocervical curettage
Diagnosis: -
02-11-02
03:24 A
M
Management Dilemmas in Cervical Cancer- Prof. S.N.Panda
7
Cervical Cancer
• Squamous Cell (>90%)
• Adenocarcinoma (5%)
• Clear Cell
• Mesonephric
Histopathology
02-11-02
03:24 A
M
Management Dilemmas in Cervical Cancer- Prof. S.N.Panda
8
Cervical Cancer
• 0:Carcinoma-in-situ
• Ia:Microinvasive (Ia1, Ia2)
• Ib:Invasive (>5mm FIGO, >3mm SGO)
• IIa:Upper 2/3 of vagina
• IIb:Parametrial involvement (not to PSW)
• IIIa:Lower 1/3 of vagina
• IIIb:PSW or hydronephrosis/nonfunctional
kidney
• IVa:Bladder or rectal mucosa
• IVb:Distant metastases
Staging: -Always Clinical
02-11-02
03:24 A
M
Management Dilemmas in Cervical Cancer- Prof. S.N.Panda
9
• Complete physical Exam, Pelvic Exam ,
Rectal Exam.
– if needed, examination under anaesthesia,
should be done.
• Ultrasonography
• Chest X ray
• IVP
• Cystoscopy
• Proctosigmoidoscopy
Staging: -Techniques
Cervical Cancer
02-11-02
03:24 A
M
Management Dilemmas in Cervical Cancer- Prof. S.N.Panda
10
Cervical Cancer
SURGERY
RADIOTHERAPY
THE TREATMENT DILEMMA
THE TREATMENT DILEMMA
02-11-02
03:24 A
M
Management Dilemmas in Cervical Cancer- Prof. S.N.Panda
11
Treatment of Cervical
Cancer
• Stage I A-I. (<1mm).
– Conization
– Simple Hysterectomy -- vaginal / abdominal
– Type I Hysterectomy (Extra fascial)
• Stage I A-II. (1 – 3mm, Lymph node -
1%).
– Type II Hysterectomy (Modified radical
Hysterectomy-Removal of medial half of
uterosacral and cardinal ligaments and
smaller margin of vagina)
Options: -
02-11-02
03:24 A
M
Management Dilemmas in Cervical Cancer- Prof. S.N.Panda
12
Treatment of Cervical
Cancer
• Stage I B & II A.
– Type III Hysterectomy (Radical
hysterectomy with removal of most of utero
sacral and cardinal ligaments, upper 1/3 rd
of vagina, pelvic lymphadenectomy)
followed by
– Post operative irradiation
• Bulky Lesions & stage II B
– Full irradiation followed 3 - 4 weeks later by
– Type II Hysterectomy
Options: -
02-11-02
03:24 A
M
Management Dilemmas in Cervical Cancer- Prof. S.N.Panda
13
Treatment of Cervical
Cancer
• Recurrent disease: -as per previous
treatment
– RT Exenteration
– Surgery RT
• Stage III & IV: - Radiation / ??Exenteration
• Radiation, as primary treatment is an
option in all stages.
• Chemotherapy - as adjunct to RT or for
palliation
Options: -
02-11-02
03:24 A
M
Management Dilemmas in Cervical Cancer- Prof. S.N.Panda
14
Radical Hysterectomy
• Removes corpus, cervix, parametria,
upper third of vagina
• Uterine arteries divided at origin
• Ureters dissected through tunnel
• Uterosacral ligaments divided near
rectum
• Typically combined with LND
• Oophorectomy not mandatory
Key Points: -
02-11-02
03:24 A
M
Management Dilemmas in Cervical Cancer- Prof. S.N.Panda
15
Radical Hysterectomy
• Abdominal exploration
• Assessment of operability
• Ligation and section of ovario pelvic fold
and round ligament
• Dissection of pelvic lymphnodes
• Dissection of ureter
• Separation of bladder
• Ligation of uterine vessels
Technique: -
02-11-02
03:24 A
M
Management Dilemmas in Cervical Cancer- Prof. S.N.Panda
16
Radical Hysterectomy
• Dissection of ureter from cardinal ligament
• Cleaning of paravescial and pararectal
fossa
• Opening of rectovaginal septum
• Clamping and transection of uterosacral
and cardinal ligament
• Transection of vagina
• Hemostasis and drainage
• Reperitonisation
Technique: -
02-11-02
03:24 A
M
Management Dilemmas in Cervical Cancer- Prof. S.N.Panda
17
Radical Hysterectomy
• Acute: Hemorrhage, Trauma, Sepsis,
Thrombophlebitis, Pulmonary Embolism,
Small Bowel obstruction, Febrile
Morbidity, UVF - 1-2%, V V F - < 1%,
• Primary mortality- 1%
• Sub Acute:
Neurogenic bladder
dysfunction
• ChronicLymphocyst, Ureteral stricture
Complications: -
02-11-02
03:24 A
M
Management Dilemmas in Cervical Cancer- Prof. S.N.Panda
18
Radical Hysterectomy
• More thorough assessment of the spread
and type of lesion
• ? Preservation of ovaries if desired
• Retention of more functional vagina
• Less morbidity and less recurrence
• Special conditions like
– Large Adnexal masses
– Fibromyoma
– Radioresistatnt growth
– Unsuitable for intracavitary irradiation
– Central recurrence after radiotherapy
Advantages: -
02-11-02
03:24 A
M
Management Dilemmas in Cervical Cancer- Prof. S.N.Panda
19
Schauta Operation
• Adopted as Mitra’s Operation In India as an
alternative to Wertheim’s Hysterectomy.
• Its an extended Vaginal Hysterectomy.
• Comprises of removal of entire Uterus and
Adenexae with most of the vagina and medial
portion of parametria, by vaginal route
• Though primary mortality is low (<1%)
lymph nodes cannot be removed. So it should
be followed by
– Post operative radiation or
– Taussig’s extra peritoneal Lymphadenectomy
An Alternative surgery: -
02-11-02
03:24 A
M
Management Dilemmas in Cervical Cancer- Prof. S.N.Panda
20
Radiation
Acute: -
• Perforation
• Fever
• Diarrhea
• Bladder spasm
Chronic: -
• Proctitis
• Cystitis-UTI
• Fistula
• Enteritis
• Femoral head
necrosis
• Ureteric stenosis
• Rectal stricture
Complications: -
02-11-02
03:24 A
M
Management Dilemmas in Cervical Cancer- Prof. S.N.Panda
21
Special Category
• Invasive Cancer discovered on Cone
Biopsy
• Cervical Stump Carcinoma
• Invasive Carcinoma found after
simple hysterectomy
• Cervical Cancer in Pregnancy
• Large Barrel shaped lesion
Difficult to deal: -
02-11-02
03:24 A
M
Management Dilemmas in Cervical Cancer- Prof. S.N.Panda
22
Follow Up
• At 2-3 Months interval ---- 2year
• At 3-4 Months interval ---- Next 2- 4
year
• At 6 Monthly interval ----- Rest of the
life
• ?Tumour markers
02-11-02
03:24 A
M
Management Dilemmas in Cervical Cancer- Prof. S.N.Panda
23
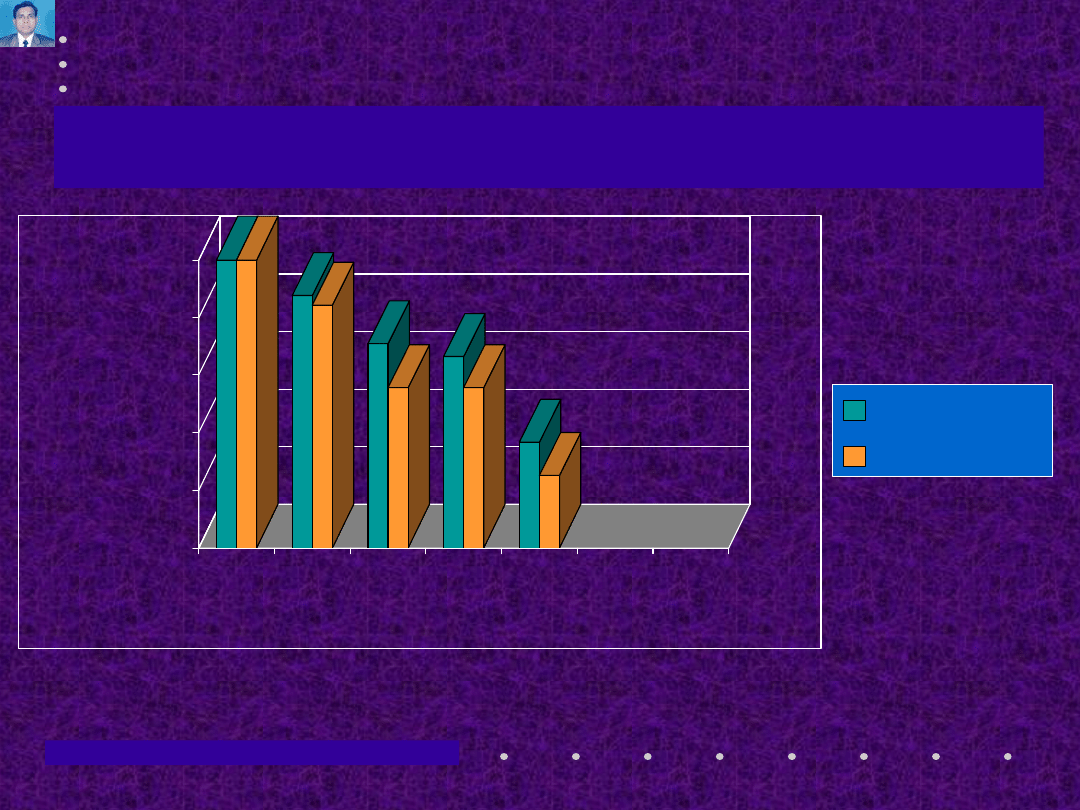
Cervical Cancer
0
20
40
60
80
100
%
IA
IB
IIA
IIB
III
Stage
SCCA
AdenoCA
from Grigsby, P.W., et.al Radiother Oncol 12:289, 1988
from Grigsby, P.W., et.al Radiother Oncol 12:289, 1988
Five-Year Survival: -
Please see notes
page.
02-11-02
03:24 A
M
Management Dilemmas in Cervical Cancer- Prof. S.N.Panda
24
Conclusion
• “Prophylaxis - better than cure” - Never more
True
• Pre treatment evaluation and Proper staging is a
must.
• Surgery and radiation are complimentary. So
proper team is essential- Surgeon and
Radiotherapist should join hands.
• Stage for stage, little progress has been made in
lowering mortality rates.
• However, the overall mortality rate is decreasing
because more patients are having their cancers
diagnosed in early states of disease.
02-11-02
03:24 A
M
Management Dilemmas in Cervical Cancer- Prof. S.N.Panda
25
Conclusion
•
Five year survival - stage IA – 100 %, IB - 85 - 90
% , stage IIA- 70 - 75 %
•
Many physicians are discouraged with the
results of cancer therapy.
•
However, the opportunity is there for all
physicians to make an early diagnosis in Ca Cx
and to protect the women from this dreadful
disease.
•
Those women saved from the ravages of cervical
cancer shall call their physicians blessed.
02-11-02
03:24 A
M
Management Dilemmas in Cervical Cancer- Prof. S.N.Panda
26
Conclusion
“Days are gone when a patient with
gynaecological malignancy could be
treated by a surgeon or a radiotherapist
in isolation”. -Stallworthy
02-11-02
03:24 A
M
Management Dilemmas in Cervical Cancer- Prof. S.N.Panda
27
Thank You
Thank You
At the service of
women
Document Outline
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
Wyszukiwarka
Podobne podstrony:
Trend in cervical cancer screening in Spain
Filling a gap in cervical cancer screening programmes
Increasing participation in cervical cancer screenin Telephone contact
Morbidity and mortality due to cervical cancer in Poland
Lower utilization of cervical cancer screening by nurses in Taiwan
The present ways in prevention of cervical cancer
Knowledge of cervical cancer and screening practices of nurses at a regional hospital in tanzania
New technologies for cervical cancer screening
Human Papillomavirus and Cervical Cancer Knowledge health beliefs and preventive practicies
Alternative approaches to cervical cancer screening — kopia
New technologies for cervical cancer screening
European transnational ecological deprivation index and index and participation in beast cancer scre
Cervical Cancer Prevention and Early american cancer society
What do British women know about cervical cancer symptoms and the risks
Quality of life and disparities among long term cervical cancer suvarviors
Women s knowledge about cervical cancer
health behaviors and quality of life among cervical cancer s
ATM POLYMORPHISM IVS6260GA IS NOT ASSOCIATED WITH DISEASE AGGRESSIVENESS IN PROSTATE CANCER
więcej podobnych podstron