dog might be bred).
4
Preventing less valued individuals from
procreating would prevent their weaknesses being passed on to
the next generation and improve the overall stock. At the time,
eugenics was popular on both the political right and left, with
many a notable enthusiast in Europe and in the USA. In Aus-
tralia, the condemnation of ‘breeding’ of indigenous people and
Caucasian settlers, the removal and isolation of mixed race
children and the White Australia policy would all be defended
through eugenics.
5
In these early years, the emphasis of eugenics was on preven-
tion of reproduction, mainly by means of sterilisation, rather
than euthanasia. It would be in post-First World War Germany,
however, that it would be developed to include euthanasia. In
Permission for the Destruction of Life Unworthy of Life,
6
published in
Germany in 1920, the academic lawyer Karl Binding and psy-
chiatrist Alfred Hoche argued that sentimentality over the sanc-
tity of life prevented the necessary task of removing ‘mentally or
intellectually dead’ individuals who contributed nothing. Why,
they asked, should such people be cared for at great cost with
little or no public benefit, when the state had sacrificed a gen-
eration of healthy, productive young men on the battlefield?
The increasingly dire socio-economic predicament of post-First
World War Germany allowed such arguments to gain momen-
tum and set the scene for the rise and seizure of power of Adolf
Hitler and the Nazi Party in 1933.
The Rise of the Nazis and a Chance Letter
The concept of racial and genetic superiority was at the forefront
of Nazi ideology. Before obtaining power, at a Nuremberg Party
Rally in 1929, Hitler introduced a future direction: ‘If Germany
was to get a million children a year and was to remove 700–
800 000 of the weakest people then the final result might even
be an increase in strength’.
1
Although compulsory sterilisation
of people with disabilities commenced early on in Hitler’s dic-
tatorship, a formal euthanasia programme did not occur until
the war began, strangely prompted by a chance letter sent to
Hitler.
The letter came from Richard Kretschmar, the father of a male
infant born with severe disabilities in Germany in late 1938. He
had already approached his local paediatrician, Dr Werner Catel,
asking that his son receive a mercy killing but Catel refused
because it was illegal. Unhappy with this decision, the father
wrote directly to Hitler requesting permission for his child to be
killed. The letter was brought to the attention of Hitler, who sent
his personal physician, Dr Karl Brandt, to investigate further.
Brandt testified on the case at his own trial in 1946: ‘The father
of a deformed child wrote to the Fuhrer with a request to be
allowed to take the life of this child or this creature. Hitler
ordered me to take care of this case. The child had been born
blind, seemed to be idiotic, and a leg and part of the arm were
missing’.
7
After Brandt’s visit, the case went in the favour of the
father and the child was killed.
Motivated by the Kretschmar case, and with the country now
at war, the Nazis seized the opportunity to legislate for a more
consistent approach for similar children. Doctors and midwives
across Germany were mandated to report not only infants born
with congenital illnesses, but also children with existing prob-
lems up to the age of three. The centralised Reich Committee for
the scientific registering of serious hereditary and congenital suffering
would then review notifications. Firstly, two laymen would
choose appropriate cases and then pass them on to three phy-
sicians (including Dr Werner Catel). The physicians would then
mark the cases with a ‘
+’ or a ‘–’, indicating whether the chil-
dren were considered appropriate for euthanasia. Once agree-
ment was secured between the physicians, the children would
be located and taken from their parents to various clinics (some
new and some in existing children’s hospitals and clinics) where
doctors and nurses would organise their demise. Efforts would
be made to take the child to an institution some distance from
their home to discourage parents visiting. Sedating medicines
such as phenobarbitol were used to induce respiratory failure
and arrest or in some cases, the children were reported to have
been left to starve to death.
8
Once the child had died, a fake
illness would be fabricated, commonly measles or ‘weakness’.
The child would be cremated and the parents would be
informed by letter, letters ending with the bold authority of the
salutation: Heil Hitler!
Parents: Cause and Effect
The Kretschmar case illustrates that some parents may have felt
the death of a severely disabled child to be appropriate. Bringing
up a disabled child in wartime Germany would have been
difficult for then, as now, disability carried with it huge stigma.
Disability would have been a source of personal guilt and impli-
cation for parents, in particular for mothers. Attitudes would
have been compounded by the propaganda that the Nazis pro-
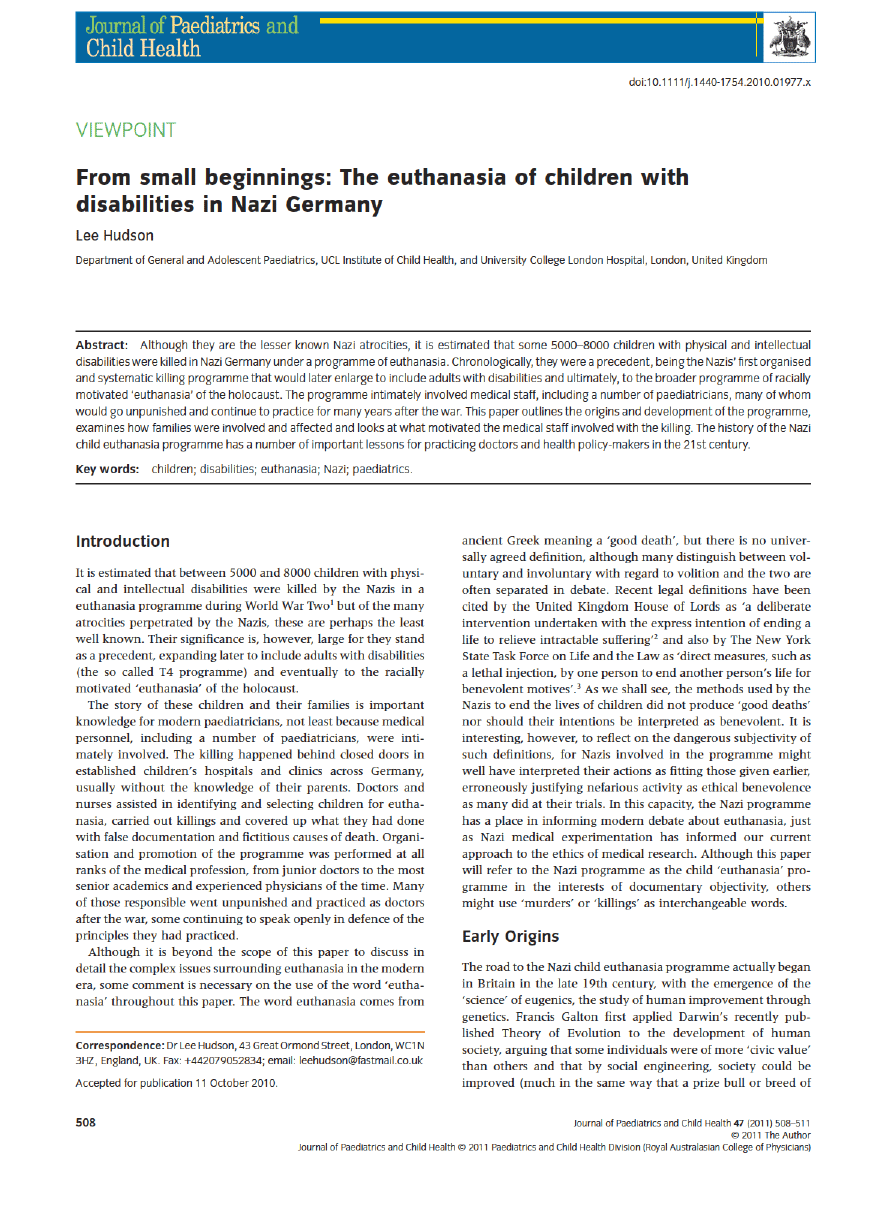
duced about people and children with disabilities. Powerful
films and posters (such as the one in Fig. 1) aimed at invoking
public sympathy for a euthanasia programme. Mathematical
questions on the costs of providing care for people with disabili-
ties versus food for families and wartime supplies appeared in
standard school textbooks.
There would also have been financial and social pressure for
mothers raising children alone while fathers were posted at the
front. There is evidence that parents handed over their disabled
Fig. 1
“Propaganda slide featuring a disabled infant”. The caption reads
“. . . because God cannot want the sick and ailing to reproduce.” Circa
1934, Germany. United States Holocaust Memorial Museum, courtesy of
Marion Davy. Copyright: United States Holocaust Memorial Museum.
L Hudson
Nazi euthanasia of children
Journal of Paediatrics and Child Health
47 (2011) 508–511
© 2011 The Author
Journal of Paediatrics and Child Health © 2011 Paediatrics and Child Health Division (Royal Australasian College of Physicians)
509

children to the authorities for temporary, respite periods not
knowing what treatment they would receive.
9
One father took
his disabled one-year-old son to an asylum in Scheuern in 1937
after the child’s mother had died as he was unable to bring the
child up alone. After remarrying in 1941, he was refused a
request for the return of his son, told by letter from the asylum
that ‘the child is to a high degree feeble-minded and is a fun-
damental case needing pure nursing care. As a result he is
utterly unsuited to being cared for in the family’. The boy was
sent onto Hadamar two years later where he was killed.
9
In fact, for most families, the planned outcome for their child
was unknown as they handed their children over in good faith.
Maria H, whose daughter was born with abnormal facies in
1939, was persuaded by her family doctor that she would be
best cared for at the paediatric clinic of Egling-Haar, some dis-
tance from her home.
8
Trusting, she consented. She received
written notification a month later that her baby had died of
pneumonia. Four-year-old Friedrich S was taken to a paediatric
clinic in Eichberg after developing neurological complications
secondary to meningitis.
8
His family received a letter from the
clinic doctor after his arrival saying that a course of ‘treatment’
had been commenced. They managed to visit him a month later,
finding him malnourished and bruised, but on trying to take
him home, they were prevented, receiving a letter two weeks
later to tell them he had died.
Despite attempts at secrecy about the programme, suspicion
was ignited, especially in the local populace. Children playing in
the streets near the Hadamar clinic would chant ‘here come the
murder boxes’ in reference to the blackened window buses that
brought new patients for euthanasia to the clinic.
9
Some who
were brave enough would make public protest and some would
be punished as a consequence. Increasing public awareness and
discontent may have contributed to the ending of ‘T4’ (the adult
disability euthanasia programme) in 1941, but the bulk of the
work was probably done by then, and larger, racially motivated
crimes outside Germany in the East may have been considered
of larger priority. The child programme continued, enlarging to
encompass more acquired disabilities and even to children dis-
playing antisocial behaviour.
9
Discarding Hippocrates
The involvement of medical staff in the killing of children espe-
cially those specialising in paediatrics seems surprising and
shocking. It is tempting to explain this away as obedient behav-
iour with fear of punishment upon refusal, but there is much to
counter this explanation.
Although the Nazi party provided political and legal authority
for euthanasia, the medical philosophy and will was already
established in Germany before Hitler came to power. At the
beginning of Hitler’s dictatorship, almost half of paediatricians
in Germany were Jewish.
10
Gradual persecution and profes-
sional exclusion led to many emigrating or eventually being
killed themselves in the holocaust, leaving a large professional
vacuum to be filled by physicians of Nazi persuasion. Indeed,
nearly half of practicing doctors in Nazi Germany were members
of the Nazi Party.
11
Doctors received distinguished professorial
posts for involvement and were more likely to secure research
grants from the government.
12
Medical staff were paid more for
work in euthanasia centres.
13
To understand the mindset of the Nazi doctor involved in
euthanasia, we can look to Dr Werner Catel, the Paediatrician
involved in the original Kretschmar case. Catel, a prominent
Nazi who played a central role in the euthanasia of children
both at a local and national level, was cleared of criminal
charges after the war and would continue to be a proponent for
euthanasia of disabled children. Catel insisted that he had
helped children and their families by killing disabled children:
‘the physician who made the diagnosis must explain the situa-
tion to the parents. He must tell them the truth especially that
this creature cannot be helped anymore, that it will never
becomes a human being’.
14
Contrast this with the Jewish female
Paediatrician Dr Lucie Adelsberger. Herself interred in Aus-
chwitz, Adelsberger was doctor for the small (and eventually
exterminated) gypsy population in Auschwitz: ‘The only thing
doctors could do for their patients, emaciated, skeletal or
swollen with edema of starvation and wallowing in feverish
deliriums, was to comfort them. It didn’t make them any better,
they still died like flies’.
10
Care for and comfort them, in other
words, not kill them yourself like Catel.
There were doctors who refused to participate. Dr Friedrich
Hozel, a Nazi, was asked by seniors to head a child euthanasia
programme and refused. He explained: ‘I am reminded of the
difference which exists between a judge and an executioner
. . . lively as my desire is in many cases to improve upon the
natural course of things, it is equally repugnant to me to carry
this out as a systematic policy after cold-blooded deliberation
and according to objective scientific principles, and without any
feeling towards the patient’.
11
There is no evidence that German
doctors and nurses who refused to participate received punish-
ment. Doctors such as Dr Hozel went to work safely elsewhere.
This is in contrast to doctors in Holland who collectively refused
to carry out Nazi orders to collude with the Nazi policy of
euthanasia on their patients during their occupation, some of
whom were sent to concentration camps as a consequence.
15
Conclusions
How can we prevent physicians becoming involved with
medical atrocities in the same way again? To answer this ques-
tion, we should perhaps look to Dr Leo Alexander, the Ameri-
can psychiatrist who gave medical advice at the Nuremberg
Trials, wrote parts of the Nuremberg Code and witnessed
first-hand the individual doctors who were tried for war crimes.
He argued that ‘Science under dictatorship becomes subordi-
nated to the guiding philosophy of the dictatorship’.
15
All gov-
ernments in some way control the health-care system in their
countries, but self-regulatory bodies such as the Royal Colleges
can allow independence from government and provide separate
guidance on complex issues such as withdrawing care. Alex-
ander also warned that in the Nazi state, crimes and atrocities
‘started from small beginnings’.
15
The gradual acceptance of Nazi
State policy by physicians over the unworthiness of some indi-
viduals to deserve life allowed them to first kill severely disabled
children. Once adapted to this, they were able to move on to
older children with existing and lesser disabilities, to adults and
eventually to anyone considered unsuitable of life by the state.
Nazi euthanasia of children
L Hudson
Journal of Paediatrics and Child Health
47 (2011) 508–511
© 2011 The Author
Journal of Paediatrics and Child Health © 2011 Paediatrics and Child Health Division (Royal Australasian College of Physicians)
510

In Nazi society individuals were measured by their civic or
financial value, as well as speculative future worth or potential
danger. Disabled children would grow to become disabled,
unproductive adults who might procreate and pass on their
problems and so were killed; jewish children would become
jewish adults and so were killed. In modern times of financial
difficulty, arguments over the rationalisation of health-care pro-
vision can include focusing on the value or civic return for
investment for an individual rather than upon need. We should
be mindful of where this has led in the past.
The Nazi euthanasia programme should also make us reflect
upon how we as individuals and as a society react to adults and
children with disabilities. The nameless stranger with a disability
in the street can evoke an array of emotional responses includ-
ing pity, anger, frustration and confusion until we know that
person as an individual, as part of our family, as our friend, our
colleague or as our patient. Today, as under the Nazis, children
and adults with disabilities are sometimes considered as outside
of society rather than part of it and in so doing, may be seen as
a burden or apportioned blame. Blame can be a natural
response to disability or any illness that frustrates us (this
patient is not trying, is not complying). Blame alleviates our
frustration, guilt and shame, which ultimately diminishes our
civic or moral responsibility. If we are not careful, this can lead
to their neglect, or in the case of the Nazis, their destruction.
Acknowledgements
The contents of the paper were presented as an oral presenta-
tion for The British Society for the History of Paediatrics and
Child Health (BSHPCH) autumn meeting in Liverpool, UK in
2010.
References
1 Kershaw I. In: Chapter 17: Licensing Barbarism eds. Hitler
(One-Volume Abridgment of Hitler 1889–1936 and Hitler 1936–1945).
London: Penguin Books, 2009; 532.
2 Report of the House of Lords Select Committee on Medical Ethics (HL
Paper 21-I of 1993–4). London: HMSO, 1994; paragraph 20–21.
3 When Death is Sought: Assisted Suicide and Euthanasia in the
Medical Context. New York: New York State Task Force on Life and the
Law, 1994. Executive summary.
4 Galton F. The possible improvement of the human breed under
the existing conditions of law and sentiment. Nature 1901;
64:
659–65.
5 Wyndham D. Eugenics in Australia: Striving for National Fitness.
London: The Galton Institute, 2003.
6 Hoche A, Binding K. Die Freigabe der Vernichtung Lebensunwerten
Lebens. Leipzig: Felix Meiner Verlag, 1920.
7 Schmidt U. Karl Brandt: The Nazi Doctor. London: Hambledon
Continuum, 2007.
8 Burleigh M. In: Chapter 3, ‘Wheels must roll for victory!’ Children’s
‘euthanasia’ and ‘Aktion T-4’. eds. Death and Deliverance:
‘Euthanasia’ in Germany C. 1900–1945. Cambridge: Cambridge
University Press, 1994; 100–7.
9 Stargardt N. In: Chapter 3, Medical murder, eds. Witnesses of War,
Children’s Lives under the Nazis. New York: Alfred A. Knopf
Publishing, 2006; 81–102.
10 Saenger P. Jewish pediatricians in Nazi Germany: victims of
persecution. Isr. Med. Assoc. J. 2006;
8: 324–8.
11 Burleigh M. In: Chapter 5, ‘Eugenics and Euthanasia’ eds. The Third
Reich a New History. London: Pan Books, 2000; 386–88.
12 Friedlander H. In: Chapter 11, ‘Physicians and other killers’ eds. The
Origins of Nazi Genocide: From Euthanasia to the Final Solution.
Chapel Hill, NC: University of North Carolina Press, 1995; 216–45.
13 Benedict S. Nurses’ participation in the Nazi euthanasia programs.
West. J. Nurs. Res. 1999;
21: 246–63.
14 Parent S, Shevell M. The ‘first to perish’. Arch. Pediatr. Adolesc. Med.
1998;
152: 79–86.
15 Alexander L. Medical science under dictatorship. N. Engl. J. Med.
1949;
241: 39–47.
L Hudson
Nazi euthanasia of children
Journal of Paediatrics and Child Health
47 (2011) 508–511
© 2011 The Author
Journal of Paediatrics and Child Health © 2011 Paediatrics and Child Health Division (Royal Australasian College of Physicians)
511
Wyszukiwarka
Podobne podstrony:
Brothers and Sisters of Children with Disabilities Medicine Jessica Kingsley Publishers
The Presentation of Self and Other in Nazi Propaganda
Differences between the gut microflora of children with autistic spectrum disorders and that of heal
Locke and the Rights of Children
APA practice guideline for the treatment of patients with Borderline Personality Disorder
Kosky; Ethics as the End of Metaphysics from Levinas and the Philosophy of Religion
Geoffrey Hinton, Ruslan Salakhutdinov Reducing the dimensionality of data with neural networks
A Propagandist of Extermination, Johann von Leers and the Anti Semitic Formation of Children in Nazi
Wicca Book of Spells and Witchcraft for Beginners The Guide of Shadows for Wiccans, Solitary Witche
Jóźwiak, Małgorzata; Warczakowska, Agnieszka Effect of base–acid properties of the mixtures of wate
Paul Ricoeur From Existentialism to the Philosophy of Language
Shel Leanne, Shelly Leanne Say It Like Obama and WIN!, The Power of Speaking with Purpose and Visio
Latour Pursuing the Discussion of Interobjectivity With a Few Friends
Stories from a Ming Collection The Art of the Chinese Story Teller by Feng Menglong tr by Cyril Bir
Fishea And Robeb The Impact Of Illegal Insider Trading In Dealer And Specialist Markets Evidence Fr
The Keys of Basilus With Commentary
2002 04 Migration the Benefits of Browsing with Konqueror
więcej podobnych podstron