Topics in Medicine and Surgery
Topics in Medicine and Surgery
Current Techniques in Avian Anesthesia
Conny Gunkel, DMV, DrMedVet,
Maud Lafortune, DMV, MSc, Dip. ACZM
Abstract
Birds often require anesthesia for diagnostic or therapeutic purposes. The provi-
sion of anesthesia with a low risk of complications is, in part, associated with a
working knowledge of avian cardiopulmonary physiology. Inhalant anesthesia re-
mains the technique of choice for anesthesia of birds. Anesthetic drugs and
techniques, including air sac cannulation and intraosseous catheterization, for pet
birds (psittacines and passerines) are covered in this review. Copyright 2005
Elsevier Inc. All rights reserved.
Key words: anesthesia; avian; birds; isoflurane; pscittacines
A
nesthesia is an important and challenging
aspect of avian medicine and surgery. Birds
have unique anatomical and physiologic
features that have an important impact on anes-
thesia. A knowledge and understanding of the
characteristics of the cardiorespiratory system of
birds are important for appropriate selection and
administration of anesthetics. Veterinarians in-
volved in the administration of anesthesia to birds
are encouraged to avail themselves of the informa-
tion contained in several comprehensive reviews
of avian cardiorespiratory anatomy and physiolo-
gy.
Cardiorespiratory Physiology
The avian cardiovascular system is considered a
“high performance” system. Compared with mam-
mals, birds have a proportionally larger heart,
larger stroke volume, greater cardiac output,
higher blood pressures, and a lower heart rate.
An increase in the release of endogenous cat-
echolamines, as it occurs during periods of stress,
may have greater impact on birds during anesthe-
sia. Hypoxia, severe hypercapnia, and anesthetic
drugs may produce further depression of the car-
diovascular system.
Differences between the avian and mammalian
respiratory system are marked. Avian tracheas are
typically 2.7 times longer and 1.3 times wider than
their mammalian counterparts.
Dead space of the
respiratory system is also increased (approximately 4
times), but a larger tidal volume and a lower respi-
ratory frequency compensate for this difference. The
trachea has complete tracheal rings and bifurcates at
the syrinx, which is located at the thoracic inlet.
Avian lungs are paired and attached firmly to the
dorsal ribs. Compared with mammals, oxygen and
carbon dioxide exchange is very efficient in birds.
Most birds, including psittacines, have 9 air sacs (4
paired, 1 unpaired).
The air sacs are avascular and
do not contribute to gas exchange, but do contrib-
ute to the effective respiration cycle.
From the Department Anesthesiology, Oregon State University,
College of Veterinary Medicine, 227 Magruder Hall,Corvallis, OR
97331 USA, and Houston Zoo Inc., 1513 North MacGregor,
Houston, TX 77030 USA.
Address correspondence to: Conny Gunkel, DMV, DrMedVet,
Department of Anesthesiology, Oregon State University, College of
Veterinary Medicine, 227 Magruder Hall, Corvallis, OR 97331.
E-mail: conny.gunkel@oregonstate.edu
© 2005 Elsevier Inc. All rights reserved.
1055-937X/05/1404-$30.00
doi:10.1053/j.saep.2005.09.006
Seminars in Avian and Exotic Pet Medicine, Vol 14, No 4 (October), 2005: pp 263–276
263

Selecting a Protocol
Inhaled Anesthetics
Inhalant anesthesia is the preferred method for the
induction and maintenance of anesthesia in birds.
Advantages of using inhaled anesthetics for these
phases include rapid induction and recovery, ability
to make rapid and frequent adjustments in anes-
thetic depth, minimal biotransformation, minimal
cardiorespiratory side effects, or organ toxicity at
clinically useful doses. These qualities make most
inhaled anesthetics ideal for anesthesia of birds with
liver- and/or kidney-altered function.
Inhaled anesthetic requirements in birds are re-
ported as the minimum anesthetic concentration
(MAC) that prevents purposeful movement in re-
sponse to a noxious stimulus in 50% of animals
tested. MAC is similar to the median effective dose
reported for other drugs. Values for MAC are similar
in birds and mammals.
The cardiorespiratory de-
pression of inhaled anesthetics is dose dependent.
Respiratory depression seems to be more significant
in birds than in mammals. A decrease in respiratory
rate and/or apnea is observed earlier in birds than
in mammals. This may reflect the fact that birds rely
more heavily on thoracic musculature for ventila-
tion. During anesthesia, these muscles become re-
laxed, reducing their ability to generate effective
ventilation. This results in a decrease in tidal volume
and less efficient CO
2
elimination. The highly effi-
cient gas exchange mechanism of birds results in
rapid changes in anesthetic depth in response to
changes in the delivered anesthetic concentration.
The concentration of inhalation anesthetics at
which apnea ensues is known as the anesthetic index
(AI).
Because MAC and AI are close, assisted or
controlled ventilation is often recommended. The
similarity between MAC and AI also emphasizes the
need for close monitoring of anesthetic depth to
prevent apnea.
Isoflurane and sevoflurane are the most common
inhaled anesthetics used in avian anesthesia. These
inhalants produce less cardiovascular depression,
are less soluble than halothane or methoxyflurane,
and require minimal biotransformation.
Low sol-
ubility allows for faster inductions and recoveries, as
well as more rapid changes in the depth of anesthe-
sia. In Galahs (Eolophus rosweicapillus), halothane
causes more hypothermia, hypercapnia, and electro-
cardiographic abnormalities than isoflurane.
Simi-
larly, in ducks, increasing MAC multiples of halo-
thane cause more cardiorespiratory depression than
isoflurane.
In pigeons, induction and recovery times with
sevoflurane are shorter than those observed with
isoflurane.
In psittacines, anesthesia with sevoflu-
rane, compared with that achieved with isoflurane, is
associated with an earlier return of alertness and less
ataxia in the recovery period. No differences be-
tween these two inhalants are observed in heart and
respiratory rates during the anesthetic period or in
the time to recovery.
Sevoflurane is less irritating
during mask induction than isoflurane. This charac-
teristic is associated with less breath holding and is
thought to be responsible for faster induction times
in humans, some other mammalian species, and
reptiles. It is not known if this characteristic has any
clinical impact in birds. The more controlled recov-
eries observed after anesthesia with sevoflurane may
make the use of this inhalant more advantageous;
however, practitioners must weigh this advantage
against the cost differential that exists between these
two inhalants.
Desflurane is an isomer of isoflurane. This inhal-
ant is more volatile than the other inhaled anesthet-
ics. As such, it requires a specialized and expensive
vaporizer for its administration.
In mammals, induc-
tion and recovery with desflurane are rapid, and
anesthetic depth can be quickly adjusted.
How-
ever, the cardiorespiratory effects of desflurane in
nonavian species are comparable with those ob-
served with either sevoflurane or isoflurane. To our
knowledge, the use of desflurane has not been eval-
uated in birds.
Injectable Drugs
Injectable anesthetics are preferred in field condi-
tions or other situations where inhalation anesthesia
is not readily available. The advantages of using in-
jectable drugs in birds rarely outweigh their disad-
vantages. These disadvantages include: dose-depen-
dent cardiovascular depression, significant interspe-
cies and intraspecies variability in response, an
inability to reverse the drug, requirement for
significant renal and hepatic biotransformation for
clearance, the potential for prolonged and/or rough
recoveries, the need for an accurate weight for ap-
propriate dosing (which may not be possible to ob-
tain in field settings), and, in most cases, a relatively
narrow margin of safety.
Injectable anesthetics used in birds include
propofol, ketamine, and ketamine combinations
(
). Tiletamine-zolazepam and alphaxalone-
alphadolone have been used in birds but with poor
results.
Propofol is a nonbarbiturate, isopropyl phenol
injectable anesthetic that is used commonly for in-
264
Gunkel and Lafortune
duction of anesthesia in mammals and reptiles.
The advantages of propofol use include rapid induc-
tion, short duration of action, and quick recovery.
Some disadvantages include the potential for apnea
during induction, hypotension, and the need for
intravenous administration.
In mammals, propo-
fol is used for maintenance of anesthesia when ad-
ministered as a constant rate infusion (CRI). Propo-
fol is particularly useful in procedures involving the
upper respiratory tract or in field situations (for
example, with exotic hoofstock).
In mammals,
there is little accumulation of the drug in the body,
and quick recoveries are observed despite extended
infusion periods.
Propofol has been evaluated in pigeons, barn owls,
turkeys, chickens, mallard ducks, canvasback ducks,
ostriches, red-tailed hawks, great horned owls, and His-
paniolan parrots.
Propofol is given intravenously
(IV) at a dosage of 3 to 15 mg/kg, depending on the
species. In these species, the administration of propo-
fol is generally followed by a smooth and rapid induc-
tion of anesthesia. Significant cardiopulmonary de-
pression can occur.
Ventilation is strongly rec-
ommended in birds anesthetized with propofol
because of the significant apnea and respiratory de-
pression that can occur after its administration.
In birds, prolonged and/or stormy recoveries are
frequently reported after the administration of
propofol, particularly if it is administered as a
CRI.
The dosage of propofol during CRI is
higher in birds than that used in mammals (0.8-1
mg/kg/min in Hispaniolan parrots and canvasback
ducks
vs. 0.15-0.4 mg/kg/min in mammals).
The prolonged recovery times suggest that phenolic
clearance rates in birds are significantly less than
those observed in mammals.
The frequent need for ventilation, and prolonged
and/or excited recoveries, decrease the benefits of
using propofol as the sole drug in an anesthetic
protocol for birds. As in mammals, the excitatory
phase may be reduced by using a balanced anesthe-
sia protocol that includes sedatives and analgesics.
This may provide some drug-sparing effect at induc-
tion and/or with a CRI.
Ketamine is a phencyclidine that causes dissocia-
tive anesthesia. It has also been shown to have some
analgesic properties in mammals by its antagonistic
action at excitatory N-methyl-D-aspartate receptors
in the central nervous system.
In birds, the produc-
tion of anesthesia with ketamine necessitates the use
of a higher dosage rate that is associated with poor
muscle relaxation, muscle tremors, myotonic con-
tractions, opisthotonus, and rough and/or pro-
longed recoveries that may range from 40 to 100
minutes.
In some reports, a surgical plane
of anesthesia was not reached, despite the use of
Table 1. Injectable Anesthetics Used in Avian Anesthesia
Drug
Dosage and Route
Species/Comments
Ketamine
20–50 mg/kg SC, IM, IV
14
Psittacines: poor analgesia. Smaller species require
higher dosage
Ketamine (K)
⫹
Diazepam (D)
10–50 mg/kg K
⫹ 0.5–2mg/kg D IM
14
Psittacines: better muscle relaxation than with
ketamine alone
5–25 mg/kg K
⫹ 2mg/kg D IV
14
Ketamine (K)
⫹
Midazolam (Mz)
10–25 mg/kg K
⫹ 0.5–1 mg/kg Mz IM
14
Psittacines: better muscle relaxation than with
ketamine alone
Ketamine (K)
⫹
Medetomidine (M)
2–5mg/kg K
⫹ 0.05–0.1mg/kg M IV
14
3–7 mg/kg K
⫹ 0.075–0.1mg/kg M
MIM
Psittacines: better muscle relaxation than with
ketamine alone. Atipamezole can be used to
reverse the alpha
2
-agonist (at 5
⫻ dose of
medetomidine)
Propofol
5–15mg/kg IV induction
Psittacines, ducks, raptors
CRI: 0.5–1.0 mg/kg/min
22,25,26
Respiratory depressant, need to ventilate
IM, intramuscular; IV, intravenous; IO, intraosseous; IT, intratracheal.
Avian Anesthesia
265

higher doses of ketamine. For these reasons, the use
of ketamine as the sole anesthetic for birds cannot
be recommended.
Combinations of ketamine and either benzodiaz-
epines or alpha
2
-adrenergic agonists are adminis-
tered in an attempt to improve muscle relaxation,
depth of anesthesia, and quality of recovery.
The use of tiletamine-zolazepam (Telazol; Fort
Dodge Laboratories, Fort Dodge, IA USA) has been
reported in ducks, raptors, and ostriches.
It was
primarily used in zoo and free-ranging birds and in
birds that are difficult to handle. However, because
of prolonged and stormy recoveries (2-4 hours), its
use in birds is rare.
Benzodiazepines, such as midazolam or diaze-
pam, have sedative, anxiolytic, muscle relaxant, and
MAC-sparing effects.
Their minimal cardiovascular
side effects and reversibility make them ideal for
administration in conjunction with either induction
or maintenance drugs. Diazepam is insoluble in wa-
ter, and is best administered IV to avoid the pain or
unreliable absorption observed when it is adminis-
tered intramuscularly (IM). Midazolam, a water-sol-
uble benzodiazepine, is preferred for IM administra-
tion.
Flumazenil is a benzodiazepine antagonist that
can be administered in cases of accidental overdose
or when benzodiazepines are thought to be respon-
sible for a delayed recovery from anesthesia. Fluma-
zenil can be administered as a bolus or titrated to
effect, but the latter is preferred in an attempt to
avoid the reversal of the beneficial anxiolysis, seda-
tion, and muscle relaxation associated with benzodi-
azepines.
Alpha
2
agonists are commonly used in combina-
tion with other anesthetics in mammals and rep-
tiles.
Alpha
2
agonist/ketamine combinations were
commonly used in birds before inhalation anesthesia
was widely available. In birds, xylazine provides un-
reliable anesthesia that is associated with severe car-
diorespiratory depression.
The use of medetomi-
dine, with or without ketamine, has been evaluated
in pigeons and Amazon parrots.
The results of
these evaluations suggest that, in general, alpha
2
agonists cannot be recommended as short-term an-
esthetics in these birds because of their unreliable
sedative effects, their inability to provide immobili-
zation, their profound cardiovascular and respira-
tory side effects, and the fact that general excitement
can effectively override their sedative effects.
Pre-anesthetic Evaluation of Birds
Ideally, in a scheduled anesthetic procedure, a pre-
anesthetic physical examination is completed a day
before the procedure. Body weight, baseline vital
signs, and diagnostic blood tests (complete blood
cell count, hematocrit, total protein, glucose, uric
acid, Aspartate Aminotransferase (AST), calcium,
phosphorus, and creatine phosphokinase) provide
useful information for both drug selection and dos-
ing. In the event that a pre-anesthetic examination is
not possible, data can be obtained during the anes-
thetic period, although this is less than ideal. In this
situation, sample analysis should be performed in a
timely manner so that any indicated auxiliary treat-
ments can be initiated in the anesthetic period.
Blood samples can be obtained from the jugular
vein (right side is larger in psittacines), basilic vein
(located on the ventral aspect of the wing at the level
of the elbow) or the medial metatarsal vein (espe-
cially useful in waterfowl and raptors). The jugular
vein is the common site for phlebotomy in
psittacines, because it is easily visualized under a
featherless area of the skin (apterium). This area is
less prone to the development of hematomas than
areas surrounding the basilic vein. As a general rule,
the volume of blood taken from a bird should not
exceed 1% of their body weight.
This amount is
usually not associated with adverse side effects in a
healthy animal; however, caution is advised in birds
that are anemic, hypovolemic, or dehydrated. In
these situations, it is safer to collect a maximum of
0.5% of the bird’s body weight. The method of blood
collection and sample handling is important for ob-
taining reliable results.
Hemolysis, clotting, and
over-dilution with heparin are the most common
problems when handling avian blood.
Pre-anesthetic Fasting
The optimum time for fasting of birds before anes-
thesia is not unequivocal. Regardless of the varied
opinions, most will agree that the length of the
fasting period, if imposed, will be influenced by
clinical status, size, and species. The main indica-
tions for fasting include an increased risk for regur-
gitation and subsequent aspiration associated with a
full crop. A full gastrointestinal tract will also de-
crease the efficiency of ventilation by impeding the
movement of air through the air sacs. When indi-
cated, a crop flush can be done to decrease the crop
volume. The procedure involves passing a red rub-
ber catheter through the esophagus into the crop for
infusion of warmed saline solution, and subsequent
aspiration of the crop contents as the crop is gently
massaged to soften any food material.
Because birds have a high metabolic rate and
relatively poor hepatic glycogen stores compared
with mammals, there is a higher risk of hypoglycemia
266
Gunkel and Lafortune
when prolonged periods of fasting are imposed. For
these reasons, fasting time should not exceed 6
hours. A fasting time between 2 and 4 hours is often
recommended in medium-sized species, whereas
birds under 200 g may not need fasting at all.
The Anesthetic Period
All phases of anesthesia (premedication, induction,
maintenance, and recovery) are critical components
of the anesthetic period. Complications can occur
during any of these periods, and careful planning
and attention to detail throughout the entire peri-
anesthetic period can lower the risk of occurrence of
critical incidents that may negatively affect outcome.
Premedication
The restraint of birds requires some expertise to
ensure a safe and lower stress experience for the
bird, handler, and clinician. Premedication is rarely
used in avian medicine to avoid repeated episodes of
manual restraint. Nevertheless, the use of premedi-
cants for sedation can be advantageous in anxious,
frightened, or excited birds. In addition, these drugs
may decrease the amount of inhaled anesthetic re-
quired with a consequent dose-dependent reduction
in negative cardiovascular side effects (arrhythmoge-
nicity, hypotension).
Benzodiazepines (midazolam, diazepam) and
opioids (butorphanol) commonly used to premedi-
cate birds. Parasympatholytics (atropine, glycopyrro-
late) are only used in patients with a history of
bradyarrhythmias. The routine use of parasympatho-
lytics may result in thickening of tracheobronchial
secretions and saliva. This may lead to an increased
risk of airway obstruction, particularly in smaller
birds. For this reason, the routine use of anticholin-
ergics as premedicants in birds is not recommended.
presents the dosages of the most commonly
used premedicants.
Induction
In preparation for general anesthesia, anesthetic
equipment and heating devices must be prepared.
Drug doses for emergency drugs should be calcu-
lated before starting the procedure and, in very crit-
ical cases, drawn up in advance. The high level of
excitement associated with restraint during induc-
tion can predispose to cardiac arrhythmias (tachyar-
rhythmias) in this critical period. After drug admin-
istration, bradycardia and apnea can be common
and lead to respiratory arrest and, subsequently, car-
diac arrest.
Table 2. Premedicants Used in Avian Anesthesia
Drug
Dosage and Route
Species/Comments
Butorphanol
0.02–0.04 mg/kg IV
37
Psittacines: Naltrexone or naloxone can be
titratred to effect as reversal
0.4–1.0 mg/kg IM
14,37
Midazolam
0.8–3.0 mg/kg IM
14
Psittacines
0.05–0.15 mg/kg IV
37
or 0.1–0.5mg/kg IM
37
Flumazenil 0.02–0.03 mg/kg IM, 0.05mg/
kg IV
33
titrated to effect or 0.1 mg/kg
IM for reversal
0.1–0.5 mg/kg IM
⫹ 0.4–1 mg/kg
butorphanol
37
Diazepam
0.2–1.0 mg/kg IM, IV
1,14,37
Most species, pigeons. Note that
diazepam should be given IV.
Midazolam is preferred for IM injection.
Flumazenil 0.02–0.03 mg/kg IM,
0.05mg/kg IV
33
titrated to effect or 0.1
mg/kg IM for reversal
Glycopyrrolate
0.01–0.02 mg/kg IM, IV
14, 37
Most species, rarely indicated
Atropine
0.01–0.02 mg/kg SC, IM
1,14
Most species, rarely indicated
0.02–0.08 mg/kg IM
37
IM, intramuscular; IV, intravenous; IO, intraosseous; IT, intratracheal.
Avian Anesthesia
267
Induction should be done in a quiet and light-
subdued environment. Because birds lack a dia-
phragm, respiration should not be compromised by
forceful restraint that prevents normal thoracic ex-
cursions during ventilation. The handler should be
experienced in bird handling. Such experience will
help avoid trauma, bites, and excessive stress on the
bird. Catching the bird with a towel or a net is a
commonly used technique. After capture, the bird
can be held through the towel or with bare hands for
induction. The holder should have control of the
head, wings, and feet at all times.
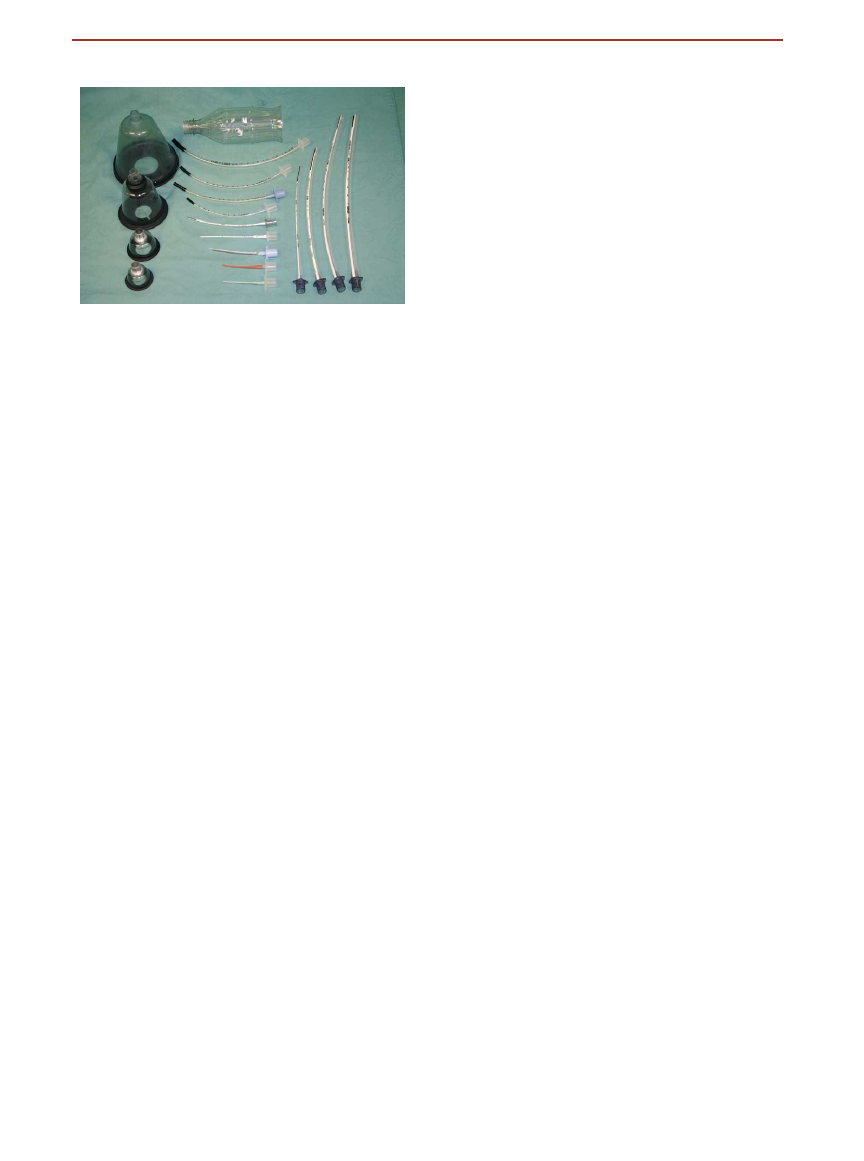
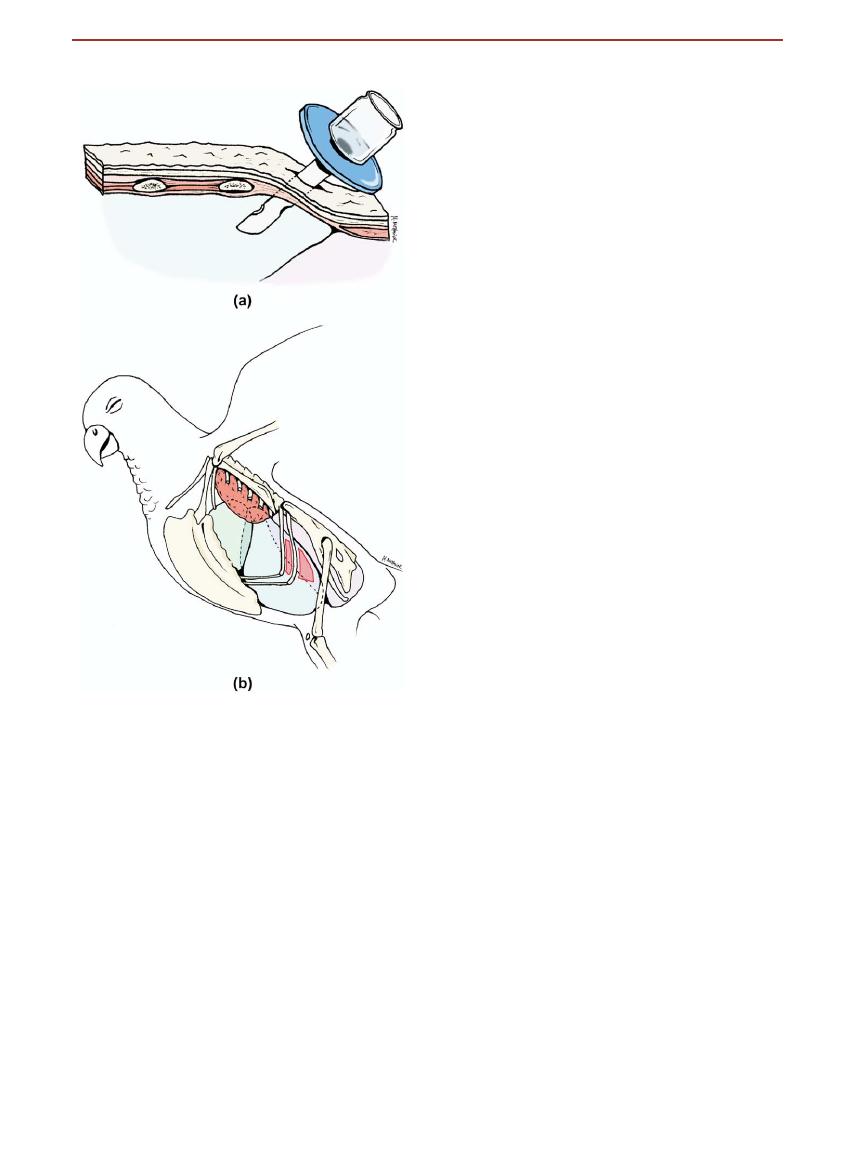
Induction with Inhaled Anesthetics.
If a face
mask induction with inhaled anesthetics is to be
performed, appropriately sized face masks that facil-
itate inductions with inhaled anesthetics and pro-
duce less environmental pollution than ill-fitting
masks that allow for significant leakage of the induc-
ing gas should be used. A selection of mask sizes and
types should be available. This is particularly true
when anesthetizing birds that can have widely diver-
gent beak sizes and shapes (
). Custom masks
can be fabricated from plastic water bottles and sy-
ringe cases. It is important to ensure that the nares
of the bird are covered by the mask. In smaller birds,
the entire head of the bird can be placed inside the
face mask.
Before the induction of anesthesia with a face
mask, a period of preoxygenation is ideal. However,
the risks associated with prolonged periods of phys-
ical restraint and excitement often outweigh the
benefits of preoxygenation. This technique should
be reserved for use in birds whose degree of respi-
ratory embarrassment necessitates the administra-
tion of oxygen before induction of anesthesia.
There are two methods of anesthetic induction
using inhaled anesthetics. One method involves in-
cremental increases of the inhalant over time (low-
This method has the advantage
of a reduced risk of overdose but has the disadvan-
tage of a longer induction and excitement phase,
which can be detrimental in a stressed and debili-
tated bird.
However, a premedicated, sedated bird
may accept this technique well.
The second method (high-to-low-protocol) is of-
ten the preferred method. This technique involves
the initial administration of a high percentage of
inhalant (4%-5% isoflurane or 6%-8% sevoflurane in
1-2 L/min of oxygen) for induction. This initial high
concentration of inhalant is then followed by a lower
concentration that is used for maintenance of anes-
thesia (2%-3% isoflurane or 4%-5% sevoflurane).
These concentrations will vary somewhat, depending
on the status of the animal and whether any premed-
ication was given before induction.
This technique
requires close attention to the animal during induc-
tion and a timely decrease in anesthetic concentra-
tion to avoid overdosing. Higher concentrations dur-
ing induction reduce the length of any period of
excitement, potentially making this method of in-
duction a safer protocol, even for debilitated
animals.
After the induction of anesthesia with either tech-
nique, the face mask is removed, and intubation with
an endotracheal (ET) tube of an appropriate size
can be performed.
Intubation.
Although some birds can be main-
tained on a face mask for short anesthetic proce-
dures, in most cases intubation is recommended and
is relatively easy to perform in birds. The advantages
of intubation, even for short procedures, include the
ability to provide manual ventilation, better control
of anesthetic depth, and prevention of aspiration
from food reflux. Because respiratory arrest can be
followed quickly by cardiac arrest, it is easier to
ventilate an already intubated bird. Moreover, ET
tubes allow for the use of a capnograph as a moni-
toring tool during anesthesia.
The avian glottis is located at the base of the
tongue and lacks an epiglottal structure, making
visualization of the glottis relatively easy compared
with mammals. During intubation, the beak is care-
fully opened with both hands or with the aid of
gauze strips. A cotton-tip applicator may help exte-
riorize the tongue, providing better access to the
glottis. A mouth gag made of rolled gauzes and tape
can be used to prevent damage to the tube (
Uncuffed ET tubes should be used for avian intu-
bation. The avian trachea has complete tracheal
rings and a fragile mucosa, which is easily damaged
by the excessive pressure that can be imposed by an
Figure 1.
Variety of face masks and ET tubes used in avian patients.
268
Gunkel and Lafortune

over-inflated ET cuff. Such damage may lead to fi-
brosis of the tracheal mucosa which can narrow the
tracheal lumen, leading to respiratory complica-
tions. This complication may not become evident
until 3 to 7 days after intubation.
Uncuffed ET tubes come in a wide variety of sizes,
the smallest having an internal diameter of 1.0 mm
(
) (Global Veterinary Products Inc, New Buf-
falo, MI; Bivona, Inc, Gary, IN; Mallinkrodt Medical,
St. Louis, MO; Rusch, Waiblingen, Germany). Intu-
bation with small tubes may be facilitated with a
stylet placed in the ET tube lumen. Some manufac-
turers produce ET tubes with a metal coil incorpo-
rated into the tube that provides rigidity and pre-
vents kinking. For small birds, a very small ET tube,
a catheter sheath, red rubber feeding tube, or uri-
nary catheter can be used for intubation. Birds
weighing less than 80 g are usually not intubated
because of the risk of occlusion of the small ET
lumen by respiratory tract secretions.
Cuffed ET tubes and a very small amount of cuff
inflation can be used in larger birds in whom an
effective airway seal for assisted or controlled venti-
lation is important, or during procedures involving
crop lavage, which may be associated with a higher
risk of airway contamination.
Air Sac Intubation.
Air sac intubation is used as an
emergency procedure in cases of upper airway ob-
struction that may be produced by a tracheal foreign
body, tracheal masses, or fungal granulomas. It can
also be used during anesthesia as an alternative to
ET intubation when unobstructed access to the head
and upper respiratory tract is required. Avian air sac
cannulas are commercially available (Air sac surgical
catheters, Global Veterinary Products, Inc.). These
short tubes (2.5-3.6 cm long) have multiple ventila-
tion holes and a convenient silicone disk that is used
to fix the cannula to the skin. They also have a
removable proximal fitting that accepts conventional
anesthesia tubing. These cannulae are available in
14F or 20F diameters (3-mm and 4-mm internal
diameter) and are cuffed or uncuffed. Alternatively,
an air sac cannula can be made from an ET tube by
cutting it shorter and creating supplemental holes in
the tube to reduce chances of obstruction.
Air sac cannulation is performed on either side of
the bird in the caudal thoracic, abdominal, or cervi-
cal air sacs. The left caudal thoracic air sac is the
preferred site because of its larger size. The ap-
proach to and location of this air sac is familiar to
most clinicians who perform coelioscopy for gender
determination.
Clavicular air sac cannulation fails
to provide effective ventilation or maintain anesthe-
sia in Sulfur-crested cockatoos and is therefore not
recommended.
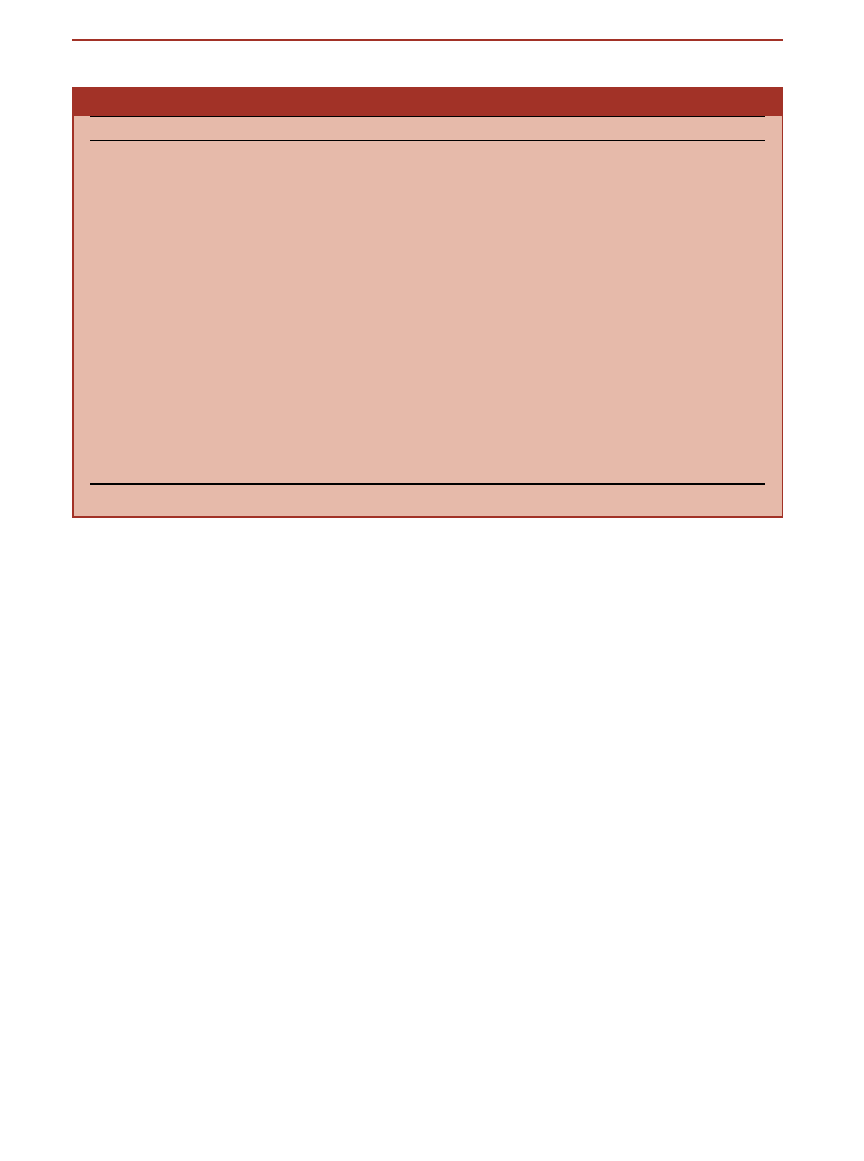
With the exception of emergency situations, air
sac cannulation is best performed in the anesthe-
tized bird. The administration of an analgesic and a
local anesthetic block before cannulation should be
considered. The bird is placed in right lateral recum-
bency, the left leg is pulled caudally, and the wings
are pulled upwards to reveal the left paralumbar
fossa (
). The cannulation area is defined as a
triangular area bordered caudally by the cranial
thigh (femur), cranially by the last 2 ribs, and dor-
sally by the synsacrum. The area is plucked and
prepared aseptically. A small incision (0.5-1.0 cm,
long enough to pass the cannula) is made through
the skin caudally to the last rib (or in certain cases,
between the last 2 ribs). A sterile hemostat is used to
dissect the soft tissue and, with a quick, controlled
stab, the coelomic cavity is bluntly penetrated, in a
technique similar to that used during laparoscopy. A
loud popping noise is often heard when the coelo-
mic cavity is penetrated. The hemostats are opened,
and the cannula is inserted into the underlying ab-
dominal air sac (1-2 cm deep). The short tube is
secured to the skin with nonabsorbable sutures, su-
turing the silicon disk of the commercial air sac
cannulae, or by using butterfly tape and sutures on
cannulae that are fashioned from ET tubes. Purse-
string sutures and a Chinese finger-trap technique
can also be used.
Confirmation of proper place-
ment and function is made by observing vapor con-
densation in the tube during respiration, or by plac-
ing a down feather in front of the tube and looking
for its movement during breathing. The air sac tube
Figure 2.
An anesthetized blue and gold macaw. Note the ET tube
and Ayre’s T-Piece system (A), the mouth gag made of rolled gauzes
(B), intravenous catheter (C) and continuous fluid infusion via a fluid
pump (D), and pulse oximeter probe (E). A Doppler flow detector is
also commonly used in birds but is not shown in this picture.
Avian Anesthesia
269
can be used for maintenance of inhalant anesthesia
when positive pressure ventilation is used. Because
of the unusual location of the ET tube, chest excur-
sions are more difficult to observe in a bird with an
air sac cannula in place.
After recovery from anesthesia, the tube may be
left for several days, but it must be monitored for
continuing patency. Before removing the tube, it is
wise to first obliterate it and verify that the bird can
still breathe well. Most birds do not tolerate their air
sac cannulas and require an Elizabethan collar to
prevent destruction or removal of the tube.
Maintenance of Anesthesia
During the maintenance period, it is important to
position the bird in a manner that facilitates the
surgical or diagnostic procedure, avoids impairing
cardiorespiratory function, and facilitates monitor-
ing. Normothermia should be maintained to avoid
hypothermia-induced bradycardia and hypotension,
and prolonged drug metabolism and clearance. In
the authors’ experiences, most anesthetic complica-
tions occur after prolonged anesthetic times. Thus,
every effort should be made to ensure a well-
planned, efficient procedure that minimizes the an-
esthetic time.
Maintenance of anesthesia is usually accom-
plished with inhaled anesthetics. For short proce-
dures, anesthesia may be maintained with injectable
drugs such as additional doses of the drug or drugs
that were used for the induction of anesthesia. How-
ever, concerns about drug accumulation and
rougher recoveries make inhalation anesthetics the
preferred method of anesthesia, even for short pro-
cedures. For some injectable drugs, the use of antag-
onists may facilitate a smooth recovery. Anesthetic
monitoring and pain management are discussed
elsewhere in this issue.
Breathing Circuits and Ventilation during Anes-
thesia.
Some form of assisted or controlled ventila-
tion to counteract the respiratory depression of
inhaled anesthetics is recommended during avian
anesthesia. Respiratory rates of 10 to 25 breaths/min
in larger species and 30 to 40 breaths/min for
smaller birds are recommended.
The efficacy of
ventilation is determined by direct visualization of
chest excursions. The peak inspiratory pressure dur-
ing assisted or controlled ventilation should not ex-
ceed 5 to 15 cm of H
2
O, depending on the size of the
bird. Excessive airway pressures can lead to air sac
trauma. Pediatric ventilators can be used in birds,
but an alarm system that signals excessive airway
pressures is mandatory.
Non-rebreathing circuits such as the Ayre’s T-
piece or Bain’s coaxial circuit are most commonly
used in birds weighing less than 7 kg. The recom-
mended fresh gas flow for the Bain system is 150 to
200 mL/kg/min with a minimum flow of 500 mL/
min, whereas for an Ayre’s T-piece, the flow should
be about 400 mL/kg/min.
The advantages of using
these systems compared with circle-breathing cir-
cuits include faster changes in the anesthetic gas
concentration and anesthetic depth, reduced dead
space, less resistance, and convenient handling. Dis-
advantages include higher gas consumption rates
and cooling and dehumidification associated with
Figure 3.
(a) is representing the two sites of insertion for placement
of an air sac canula into the caudal thoracic air sac. The incision is
made just cranially or most commonly caudally to the last rib. (b) is
a schematic close up view of the air sac canula in place. The canula
penetrates the skin and the thin muscle layers and is opening into
the caudal thoracic air sac. After placement the air sac canula has
to be secured with suture material to the skin and can be connected
to oxygen or inhalant agents.
270
Gunkel and Lafortune

these higher gas flow rates. The placement of the
rebreathing bag and pop-off valve on the Ayre’s
T-piece can be inconvenient. High gas flow rates and
a lack of distensibility of the breathing circuit can
quickly lead to barotrauma, decreased venous re-
turn, and cardiac arrest, should the pop-off valve be
inadvertently closed.
A pediatric rebreathing circle system may be used
in birds weighing over 7 kg. Use of this type of circuit
may have the associated advantage of better heat
preservation compared with a non-rebreathing cir-
cuit, especially when lower gas flow rates are used.
Lower gas flow rates have the advantages of reduced
gas consumption, less environmental pollution, and
the potential for heat preservation.
Ventilation in anesthetized birds can be de-
pressed significantly. This depression can occur be-
cause of the respiratory depression associated with
the administration of inhaled anesthetics, respira-
tory muscle relaxation, an increase in dead-space
ventilation due to airway apparatus, and inhibition
of ventilation due to positioning. The lack of a
diaphragm, an enlarged gastrointestinal tract, or
physical pressure from the surgeon’s hand can all
impede ventilation during anesthesia.
Optimum
positioning will be dictated by the procedure but,
when possible, birds should be placed in lateral re-
cumbency. Dorsal or ventral recumbency can restrict
the movement of the sternum and compress the
abdominal air sacs leading to a decrease in effective
ventilation.
Recovery
Recovery is a critical period in avian anesthesia. As
with induction and maintenance, monitoring for
cardiorespiratory depression, particularly from re-
straint, is very important. Supplemental oxygen may
be given during recovery either through the ET
tube, if the bird is still intubated, or by placing a face
mask directly in front of the bird’s face. Positioning
is very important, and the clinician must verify that
the bird’s ventilation is not impeded during recov-
ery. It is common practice for some practitioners to
hasten recovery by side-to-side rocking; however,
these fast turns may lead to detrimental hemody-
namic changes. As such, this procedure is not rec-
ommended. Extubation should occur when the bird
is fully awake, breathing well, and able to swallow.
Before, and immediately after extubation, examina-
tion of the glottis for secretions that may obstruct the
airway is crucial. In the event of regurgitation, the
bird’s head should be lowered while the secretions
are removed with cotton-tip applicators or gauze
sponges. Use of suction is rarely necessary. The bird
should be held until it is only mildly sedate. At this
point it can be returned to a cage or kennel in a
quiet and warm environment. Small padded cages or
an incubator with the bird wrapped in towels
facilitate a smooth recovery. Continuing hypother-
mia or rewarming-induced hyperthermia should be
avoided. Rewarming of a hypothermic bird should
be accomplished gradually.
Because of the risk of hypoglycemia, it is impor-
tant that birds eat soon after recovery from anesthe-
sia. This is of particular concern in smaller birds.
Oral administration of a few drops of 50% dextrose
can be performed during recovery if hypoglycemia is
suspected. Pain management may aid in a smooth
recovery; this important topic is presented elsewhere
in this issue.
Supportive Therapy during Anesthesia
Fluid Therapy
Fluid Choice.
The choice of fluid type is deter-
mined by the status of the patient (packed cell vol-
ume (PCV), total protein (TP), dehydration status)
and any anticipated or calculated surgical blood loss.
Because of the bird’s high metabolic rate and low
glycogen-storage capacity, a regular assessment of
blood glucose concentration is recommended. This
is rarely performed in clinical settings in smaller
birds because of their small blood volume. However,
glucometers require a very small amount of blood; a
volume that should be obtained easily in small birds.
Intraoperative measurement of glucose with a glu-
cometer should become part of routine monitoring
during prolonged procedures. Lactated Ringer’s so-
lution with 2.5% to 5% dextrose is commonly admin-
istered to prevent hypoglycemia.
Reference to species-specific biochemistry values
is essential in selecting a fluid appropriate in its
tonicity and electrolyte composition. Interspecies
differences in normal serum electrolyte concentra-
tions exist. Birds generally have lower potassium and
higher sodium serum concentrations compared with
mammals.
These differences may have an impact
on body fluid dynamics and physiologic processes
such as cardiac contractility when isotonic fluids for-
mulated for mammals are administered to birds.
Such differences need to be considered when mak-
ing decisions concerning appropriate fluid therapy
for birds. Clearly, routine determinations of serum
electrolyte concentrations would be ideal; however,
this may not be practical in the clinical setting.
Crystalloids.
All birds that undergo a prolonged an-
esthetic procedure should receive some form of
Avian Anesthesia
271

fluid therapy. Replacement balanced electrolyte so-
lutions such as Lactated Ringer’s solution, Plasma-
lyte 148 (Baxter Laboratories, Deerfield, IL), and
Normosol R (Sanofi Animal Health, Overland Park,
KS) can be administered IV or intraosseously (see
below) at 10 to 20 mL/kg/hr. This small amount of
fluid can be given continuously with a syringe pump
or titrated manually. Alternatively, a bolus of fluids
(30 mL/kg) can be administered subcutaneously.
Generally, this is a quick and easy method of fluid
administration that appears to be quite effective,
even in debilitated birds. Before administration, flu-
ids should be warmed to body temperature.
Blood Transfusion, Colloids, and Hemoglobin-
Based Solutions.
The administration of whole
blood, colloidal solutions, or hemoglobin-based
products should be considered in the event of sig-
nificant blood loss during surgery and anesthesia.
Although the pathophysiology of hemorrhagic shock
in birds has not been fully described, hypotension
and tachycardia are known signs of acute blood
loss.
Compared with mammals, birds seem to be
more tolerant to acute blood loss than mammals, in
part because of their tolerance of prolonged he-
modilution.
The estimated circulating blood vol-
umes in different avian species vary considerably
from 5% of body weight in ring-necked pheasants up
to 20% in racing pigeons.
Acute blood loss of 60%
of the calculated total blood volume in ducks has
been described as the median lethal dose (50% mor-
tality), compared with mammals, in whom the me-
dian lethal dose is 40% to 50% of the total blood
volume.
Blood Transfusion.
In the face of significant blood
loss, the administration of whole blood most ade-
quately restores tissue perfusion and oxygen deliv-
ery. Clearly, in avian medicine and surgery, whole
blood transfusion is limited because of the availabil-
ity of donors. At the present time, blood types have
not been described in birds, which limits the appli-
cation of crossmatching before transfusion.
Ho-
mologous (of the same species) transfusions are as-
sociated with the longest erythrocyte survival time,
but heterologous (between different species) blood
transfusions in birds are often more feasible and
have been performed without any significant side
effects.
Anticoagulants include acid citrate dex-
trose, sodium citrate, or citrate phosphate dextrose
at 1 to 1.5 mL per 10 mL of blood. Heparin can also
be used at 0.25 mL/10 mL of blood.
In avian
medicine and surgery, the volume of blood given
during transfusion is often dictated by the amount of
blood that can be safely harvested from the donor
bird rather than the amount required by the recip-
ient. Blood for transfusion can be administered IV or
intraosseously through a blood filter at a continuous
rate of 2 mL/min or as intermittent boluses over a
few hours.
Colloids.
Because of the limited availability of avian
blood products, the use of colloids is often the only
real option for treating acute hemorrhagic shock.
Compared with mammalian blood, the total protein
concentration of avian blood is substantially lower
(21-45 g/L [2.1-4.5 g/dL]).
Proteins are the major
determinant of colloid osmotic pressure (COP) and
may indirectly influence blood pressure. COP in
birds is substantially lower than mammalian COP (11
mm Hg for chickens and 8.1 mm Hg in doves, com-
pared with 25 mm Hg in mammals),
but the ratio
of protein concentration in the interstitial fluid to
that in the blood is much lower as well.
This lower
ratio may be correlated with the higher arterial
blood pressures observed in birds. Mean arterial
blood pressure may exceed 150 mm Hg in some
species of birds.
Lower total protein concentrations
in avian blood are a consideration when choosing a
colloidal solution, because the COP of most colloidal
solutions is 20 to 25 mm Hg. This may exceed the
avian COP and may lead to fluid movement from the
extravascular space to the intravascular space, result-
ing in excessive volume expansion and dehydration
of the interstitial space.
The use of hetastarch (HES; Abbott Laboratories,
North Chicago, IL USA) for the management of
hypoproteinemia and hypovolemia in birds has been
described.
Although IV boluses of 10 mL/kg have
been given to birds, the authors recommend admin-
istering colloids, in conjunction with crystalloids,
with a syringe pump over a period of minutes to
hours, giving the colloids over several minutes to
hours. In a study on cockatiels, hetastarch was given
as an IV bolus with crystalloids between 1 and 15
mL/kg.
The effect of hetastarch on platelet aggre-
gation in birds has not been investigated.
Hemoglobin Solutions.
Oxyglobin (Biopure Corpora-
tion, Cambridge, MA) is a purified polymerized bo-
vine hemoglobin. This solution has both colloidal
properties and an ability to carry oxygen. Because it
has no significant antigens, crossmatching is not re-
quired, nor do filters need to be used during admin-
istration.
In birds, oxyglobin has been given as a
rapid bolus over a few minutes, with crystalloids at
dosages between 1 and 15 mL/kg.
Unfortu-
nately, at the time of writing, oxyglobin is no longer
available in the United States.
272
Gunkel and Lafortune
Intraosseous Catheterization.
The placement of
an intraosseous (IO) catheter for fluid administra-
tion should be considered in dehydrated or hypovo-
lemic birds, when establishing a venous access is
difficult.
Any fluid type, medication, or emer-
gency drug that can be administered IV can also be
administered intraosseously. Solutions injected into
the IO space are absorbed by sinusoids and drain
into veins that connect into the systemic circula-
tion.
Therefore, IO administration provides the
same access to the vascular system as IV administra-
tion.
The most common sites for IO catheter
placement are the proximal and distal ulna and the
proximal tibiotarsus. The avian humerus and femur
are often pneumatized and connected to the respi-
ratory system; thus, these bones are contraindicated
as sites for an IO catheter.
IO catheters are commercially available (Global
Veterinary Products, Inc.). They range from 14 to
20-gauge and are 3 cm in length. These catheters
have a metal stylet, a convenient handle to facilitate
the introduction of the needle into the bone, and a
plastic fixation device that can be sutured to the skin
and to stabilize the IO catheter. Alternatively, regu-
lar needles or spinal needles can be used. A gauge
and length of needle appropriate for the size of the
bird should be used. A disadvantage of using regular
needles is the possibility of being blocked by a bone
plug, but in the authors’ experience this problem is
rarely encountered. In small patients, regular nee-
dles are easier to use and more versatile than an IO
catheter, which, because of its larger size, can easily
penetrate the thin cortex of avian bones.
To place an IO catheter in the distal ulna, the
dorsal aspect of the ulna is plucked and the area is
aseptically prepared. The ulna is held in one hand
(usually the left for a right-handed person), and
the needle is held in the other hand and posi-
tioned ventral to the condylar ridge of the distal
ulna.
With a firm and slight rotating movement
similar to that of a retrograde pin placement, the
needle is gently driven into the ulnar bone at a 45°
to 70° angle. When the ulna is penetrated, a
marked reduction in resistance will be felt. At that
point, the needle angle is reduced so that it is as
parallel to the bone as possible. With a gentle
rotating movement, the needle is completely
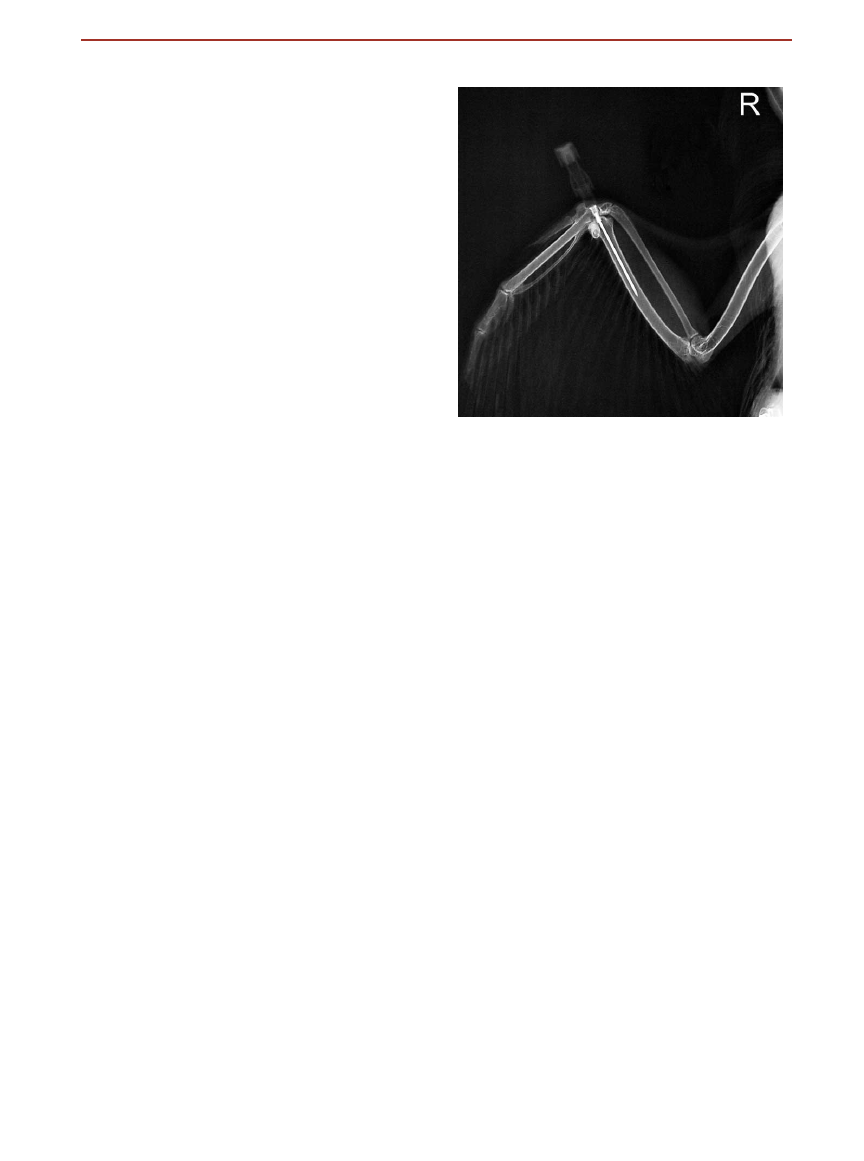
driven into the medullary cavity of the ulna. Cor-
rect placement of the IO catheter can be con-
firmed radiographically (
). If the needle is
properly positioned, fluids will easily flow through
the catheter and can be seen passing through the
ulnar vein.
The catheter is capped with a luer-lock
injection port and secured to the wing with tape
and/or sutures. Gauze squares may be used to
protect the injection port, and the wing wrapped
with a standard figure-of-8 bandage.
When placing a proximal ulnar catheter, the
point of entry should be 3 to 4 flight feathers prox-
imal to the elbow.
The ulna is penetrated at an
acute angle with a rotating motion. Once the needle
is inserted into the bone, the angle is reduced, and
the needle is fully inserted into the ulnar medullary
cavity with a gentle rotating movement.
If placing a
proximal tibiotarsus IO catheter, the stifle is flexed
and the needle is inserted into the trochanteric
fossa.
If an IV catheter is used, fluids can be given
continuously or with intermittent bolus injections.
The catheter can be left in place for several days.
Anesthetic Complications
During the anesthesia of birds, it is prudent to have
the more commonly used emergency drugs, such as
atropine and epinephrine, drawn up and ready for
injection (
Respiratory arrest, closely followed by cardiac ar-
rest, is not an infrequent complication associated
with avian anesthesia. Respiratory arrest is often re-
versible when detected early. After recognition of
respiratory arrest, the first step in treatment should
be either reducing or turning off the inhaled anes-
thetic and/or administering any antagonists for
Figure 4.
Dorsoventral radiograph of an IO cathether (20-gauge,
2.7-cm needle and luer-lock injection cap) placed in the distal ulna
of a mallard duck.
Avian Anesthesia
273
drugs that have been given. Manual ventilation
should be provided until spontaneous respiration
returns. It is important that assisted ventilation not
be overly aggressive, because the decrease in cardiac
output associated with aggressive ventilation can
lead to further complications. The use of doxapram
as a treatment for apnea is controversial and not
recommended by the authors, particularly in
hypoxemic birds. Doxapram is a central stimulant
that increases tidal volume but not respiratory fre-
quency.
In infants, the effectiveness of doxapram
is profoundly diminished when the brain is already
hypoxic. It increases the oxygen consumption as well
as the cerebral metabolic requirements, and there-
fore can cause perfusion injury to the white matter
that is in a hypoxic state.
The generally accepted
opinion on the use of doxapram is that it is unlikely
to be of much benefit in the apneic, hypoxic new-
born, and its routine use as a respiratory stimulant is
not warranted.
The American Heart Association
does not recognize the routine use of doxapram as a
treatment for respiratory arrest,
and the authors do
not recommend using it in birds with respiratory
arrest. Assisted ventilation via the ET tube is pre-
ferred.
In the event that respiratory arrest progresses to
cardiac arrest, cardiac compressions can be at-
tempted, but are difficult to perform in birds be-
cause of the location of the heart in relation to the
sternum.
Epinephrine can be given IV, intraosse-
ously, or intratracheally. Unfortunately, the success
rate for the return of cardiac function in birds after
arrest is low.
Arrhythmias may arise during anesthesia in re-
sponse to many different causes. These include pain,
inappropriate depth of anesthesia, hypoglycemia,
hypothermia, aberrations in acid base status or elec-
trolyte concentrations, and blood loss. Hypothermia
is a frequent, reversible, and even preventable com-
plication of anesthesia in most species. Hypothermia
can lead to bradyarrythmias that may be resistant to
treatment with glycopyrrolate or atropine. As with
many complications, prevention is easier than treat-
ment. Warm-forced air blankets are the most success-
ful heating devices for preventing hypothermia in
very small animals.
Summary
Despite considerable research into the identification
of the ideal injectable anesthetic for birds, inhaled
anesthetics remain the most frequently administered
drugs for general anesthesia. Inhaled anesthetics are
Table 3. Emergency Drugs and Dosages
Drug
Dosage and Route
Species/Comments
Atropine
0.02–0.5 mg/kg IM, IV, IO, IT
1,14,37
Bradycardia, CPR
Glycopyrrolate
0.01–0.02 mg/kg IM, IV
14,36
Bradycardia
Epinephrine
0.5–1.0 mg/kg IM, IV, IO, IT
14
Asystole, CPR
Calcium
gluconate
50–100 mg/kg IV slow, IM
1,14
Hypocalcemia
Sodium
bicarbonate
1–5 mEq/kg IV, IO
1,14
Metabolic acidosis, CPR
Dextrose 50%
500mg/kg IV slow
14
Most species for hypoglycemia. Should never be
given IM or SC.
Doxapram
5–20mg/kg IM, IV, IO
1,14
Authors do not recommend use of doxapram
during respiratory arrest (see text).
IM, intramuscular; IV, intravenous; IO, intraosseous; IT, intratracheal; CPR, cardiopulmonary resuscitation; SC, subcutaneously.
274
Gunkel and Lafortune

favored because of their relative safety, short onset
and duration of action, and comparably smooth and
quick recoveries. However, inhalant drugs have no
analgesic properties, and appropriate analgesics
must be given. Options for pain management are
discussed in a separate article in this issue.
The trend in anesthesia and analgesia in mam-
mals is toward a multimodal, balanced approach that
involves the administration of smaller doses of sev-
eral drugs targeted at specific needs associated with
the anesthetic process. This is in contrast to the
practice of administering a large dose of a single
drug to achieve the desired effects. Balanced anes-
thesia typically involves the administration of a sed-
ative or analgesic before anesthesia, allowing for the
administration of lower doses of inhaled anesthetics.
The ideal adjuncts to inhaled anesthesia have no to
minimal cardiopulmonary side effects and are short-
acting and reversible.
The progressive practice of balanced anesthesia is
being adopted by the providers of avian anesthesia,
and continued expansion of this approach in the
realm of avian and exotic animal anesthesia will
serve to reduce anesthesia-related morbidity and
mortality.
Acknowledgments
The authors would like to thank Alex Valverde, Jim
Wellehan, and Jessica Siegal-Willet for their help
with this manuscript and Michelle Mehalick for pro-
viding
References
1.
Ritchie BW, Harrison GJ, Harrison LR (eds): Avian
Medicine, Principles and Application. Philadelphia,
PA, Saunders, 1997
2.
Altman RB, Clubb SL, Dorrestein GM, et al (eds):
Avian Medicine and Surgery. Philadelphia, PA,
Saunders, 1997
3.
Whittow GC (ed): Sturkie’s Avian Physiology (ed 5).
San Diego, CA, Academic Press, 2000
4.
Gleed RD, Ludders JW (eds): Recent Advances in
Veterinary Anesthesia and Analgesia: Companion
Animals. Ithaca, NY, International Veterinary Infor-
mation Service, 2001
5.
Thurmon JC, Tranquilli WJ, Benson GJ: Lumb &
Jones’ Veterinary Anesthesia (ed 3). Baltimore, MD,
Williams and Wilkins, 1996
6.
Miller RD (ed): Anesthesia (ed 5). Philadelphia, PA,
Churchill Livingstone, 2000
7.
Jaensch SM, Cullen L, Raidal SR: Comparative car-
diopulmonary effects of halothane and isoflurane in
Galahs (Eolophus rosweicapillus). J Avian Med Surg
13:15-55, 1999
8.
Ludder JW, Mitchel JS, Rode J: Minimal anesthetic
concentration and cardiopulmonary dose response
of isoflurane in ducks. Vet Surg 19:304-307, 1990
9.
Ludder JW: Minimal anesthetic concentration and
cardiopulmonary dose response of halothane in
ducks. Vet Surg 21:319-324, 1992
10.
Korbel R: Comparative investigations on inhalation
anesthesia with isoflurane (Forene) and sevoflurane
(SEVOrane) in racing pigeons (Columba livia, 1789,
var. domestica) and presentation of a reference an-
esthesia protocol for birds Tierarztl Prax Ausg K
Klientiere Heimtiere 26:211-223, 1998
11.
Quandt JE, Greenacre CB: Sevoflurane anesthesia in
psittacines. J Zoo Wildl Med 30:308-309, 1999
12.
Barter LS, Ilkiw JE, Pypendop BH, et al: Evaluation of
the induction and recovery characteristics of anes-
thesia with desflurane in cats. Am J Vet Res 65:748-
751, 2004
13.
Samour JH, Jones DM, Knight JA: Comparative stud-
ies of the use of some injectable anesthetic agents in
birds. Vet Rec 115:6-11, 1984
14.
Carpenter JW, Mashima TY, Rupiper DJ (eds): Exotic
Animal
Formulary
(ed
2).
Philadelphia,
PA,
Saunders, 2001
15.
Fowler ME, Miller RE (eds): Zoo and Wild Animal
Medicine (ed 5). Philadelphia, PA, Saunders, 2003
16.
Langley M, Heel R: Propofol: a review of its pharma-
codynamic and pharmacokinetic properties and use
and an intravenous anaesthetic. Drugs 35:334-372,
1988
17.
Fitzgerald G, Cooper JE: Prelimiary studies on the
use of propofol in the domestic pigeon (Columbia
livia). Res Vet Sci 49:334-338, 1990
18.
Mama KR, Phillips LG, Pascoe PJ: Use of propofol for
induction and maintenance of anesthesia in a barn
owl (Tyto alba) undergoing tracheal resection. J Zoo
Wildl Med 27:397-401, 1996
19.
Schumacher J, Citino SC, Kernandez K, et al: Car-
diopulmonary and anesthetic effects of propofol in
wild turkeys. Am J Vet Res 58:1014-1017, 1997
20.
Lukasik VM, Gentz EJ, Erb HN, et al: Cardiopulmo-
nary effects of propofol anesthesia in chickens (Gal-
lus gallus domesticus). J Avian Med Surg 11:93-97, 1997
21.
Machin KL, Caulkett NA: Cardiopulmonary effects of
propofol and a medetomidine-midazolam-ketamine
combination in mallard ducks. Am J Vet Res 59:598-
602, 1998
22.
Machin KL, Caulkett NA: Cardiopulmonary effects of
propofol infusion in canvasback ducks (Aythya val-
isineria). J Avian Med Surg 13:167-172, 1999
23.
Machin KL, Caulkett NA: Evaluation of isoflurane
and propofol anesthesia for intraabdominal trans-
mitter placement in nesting female canvasback
ducks. J Wild Dis 36:324-334, 2000
24.
Langlan JN, Ramsay EC, Blackford JT, et al: Cardio-
pulmonary and sedative effects of intramuscular me-
detomidine-ketamine and intravenous propofol in
ostriches (Strutio camelus). J Avian Med Surg 14:2-7,
2000
25.
Hawkins MG, Wright BD, Pascoe PJ: Pharmacokinet-
ics and anesthetic and cardiopulmonary effects of
propofol in red-tailed hawks (Buteo jamaicensis) and
great horned owls (Bubo virginianus). Am J Vet Res
64:677-683, 2003
26.
Langlois I, Harvey CR, Jones MP, et al: Cardiopul-
monary and anesthetic effects of isoflurane and
Avian Anesthesia
275

propofol in Hispaniolan Amazon Parrots (Amazona
ventralis). J Avian Med Surg 17:4-10, 2003
27.
Christensen J, Fosse RT, Halvorsen OJ, et al: Com-
parison of various anesthetic regimens in the domes-
tic fowl. Am J Vet Res 48:1649-1657, 1987
28.
Valverde A, Bienzle D, Smith DA, et al: Intraosseous
cannulation and drug administration for induction
of anesthesia in chickens. Vet Surg 22:240-244, 1993
29.
Varner J, Clifton KR, Poulos S, et al: Lack of efficacy
of injectable ketamine with xylazine or diazepam for
anesthesia in chickens. Lab Anim 33:36-39, 2004
30.
Rosskopf WJ, Woerpel RW, Reed S, et al: Avian an-
esthesia administration, in: 1989 Proceedings of the
American Animal Hospital Association, St. Louis,
MO, 1989, pp 449-457
31.
Carp NZ, Saputelli J, Halbherr TC, et al: Technique
for liver biopsy performed in Pekin ducks using an-
esthesia with Telazol. Lab Anim Sci 41:474-475, 1991
32.
Kreeger TJ, Degernes LA, Kreeger JS, et al: Immobi-
lization of raptors with tiletamine and zolazepam
(telazol), in: Redig PT, Cooper JE, Remple JD, et al
(eds): Raptor Biomedicine. Minneapolis, MN, ; pp
141-144University of Minnesota Press, 1993
33.
Sandmeier P: Evaluation of medetomidine for short-
term immobilization of domestic pigeons (Columba
livia) and Amazon parrots (Amazona species). J Avian
Med Surg 14:8-14, 2000
34.
Pollock CG, Schumacher J, Orosz SE: Sedative effects
of medetomidine in pigeons (Columba livia). J Avian
Med Surg 15:95-100, 2001
35.
Atalan G, Uzun M, Demerkan I, et al: Effect of me-
detomidine-butorphanol-ketamine anaesthesia and
atipamezole on heart and respiratory rate and cloa-
cal temperature of domestic pigeons. J Vet Med As-
soc 49:281-285, 2002
36.
Harr KE: Clinical chemistry of companion avian spe-
cies: a review. Vet Clin Path 31:140-151, 2002
37.
Abou-Madi N: Avian anesthesia. Vet Clin North Am
Exot Anim Pract 4:147-167, 2001
38.
Curro TG: Anesthesia of pet birds. Sem Avian Exot
Pet Med 7:10-21, 1998
39.
Heatley JJ, Marks S, Mitchell M, et al: Raptor emer-
gency and critical care: therapy and techniques.
Compendium 23:561-570, 2001
40.
Jaensch SM, Cullen L, Raidal SR: Comparison of
endotracheal, caudal thoracic air sac and clavicular
air sac administration of isoflurane in Sulfur-crested
cockatoos (Cacatua galerita). J Avian Med Surg 15:
170-171, 2001
41.
Rode JA, Bartholow S, Ludders JW: Ventilation
through air sac canula during tracheal obstruction in
ducks. J Avian Assoc Vet 4:98-102, 1990
42.
Lichtenberger M, Orcutt C, DeBehnke D, et al: Mor-
tality and response to fluid resuscitation after acute
blood loss in mallard ducks (Anas platyrhynchos), in:
2002 Scientific Proceedings, 23rd Annual Meeting of
Association of Avian Veterinarians. Monterey, CA,
2002, pp 65-67
43.
Lichtenberger MK, Chavez W, Cray C, et al: Mortality
and response to fluid resuscitation after acute blood
loss
in
mallard
ducks,
in:
2003
Scientific
Proceedings, 24th Annual Meeting of Association of
Avian Veterinarians. Pittsburgh, PA, 2003, pp 7-10
44.
Campbell TW: Avian hematology, in: Campbell TW
(ed): Avian Hematology and Cytology. Ames, IA,
Iowa State University Press, 1995, pp 54-59
45.
Morissey J: Avian transfusion medicine. Exot Pet
Pract 4:65-66, 1999
46.
Degernes LA, Crosier ML, Harrison LD, et al: Autol-
ogous, homologous, and heterologous red blood cell
transfusions in cockatiels (Nymphicus hollandicus). J
Avian Med Surg 13:2-9, 1999
47.
Degernes LA, Harrison LD, Smith DW, et al: Autol-
ogous, homologous, and heterologous red blood cell
transfusions in conures of the genus Aratinga. J Avian
Med Surg 13:10-14, 1999
48.
Lichtenberger MK, Rosenthal K, Brue R, et al: Ad-
ministration of oxyglobin and 6% hetastarch after
acute blood loss in psittacines birds, in: 2001 Scien-
tific Proceedings, 22nd Annual meeting of the Asso-
ciation of Avian Veterinarians. Orlando, FL, 2001, pp
15-18
49.
Altman PL, Dittmer DS (eds): Biology Data Book. In:
Biological Handbooks. Bethesda, MD, Federation of
American Societies for Experimental Biology, 1974
50.
Hargens AR, Millard RW, Johansen K: High capillary
permeability in fishes. Comp Biochem Physiol A,
48:675-680, 1974
51.
Altman PL, Dittmer DS (eds): Biological Handbooks:
Respiration
and
Circulation.
Bethesda,
MD,
Federation of American Societies for Experimental
Biology, 1971
52.
Stone EG, Redig PT: Preliminary evaluation of
hetastarch for the management of hypoproteinemia
and hypovolemia, in: 1994 Proceedings of the Asso-
ciation of Avian Veterinarians. Lake Worth, FL, 1994,
pp 197-199
53.
Lichtenberger M: Transfusion medicine in exotic
pets. Clin Tech Small Anim Pract 19:88-95, 2004
54.
Costello MF: Principles of cardiopulmonary cerebral
resuscitation in special species. Sem Avian Exot Pet
Med 13:132-141, 2004
55.
Bamford OS, Dawes GS, Hanson MA, et al: The
effects of doxapram on breathing, heart rate and
blood pressure in fetal lambs. Respir Physiol 66:387-
396, 1986
56.
Moon PF, Massat BJ, Pascoe PJ: Neonatal critical
care. Vet Clin North Am Small Anim Pract 31:343-
365, 2001
57.
Roll C, Horsch S: Effect of doxapram on cerebral
blood flow velocity in preterm infants. Neuropediat-
rics 35:126-129, 2004
58.
American Heart Association: Guidelines 2000 for car-
diopulmonary resuscitation and emergency cardio-
vascular care. Circulation 102:I1-I384, 2000
59.
Rembert MS, Smith JA, Hosgood G, et al: Compari-
son of traditional thermal support devices with the
forced-air warmer system in anesthetized Hispani-
olan amazon parrots (Amazona ventralis). J Avian Med
Surg 15:187-193, 2001
276
Gunkel and Lafortune
Document Outline
- Current Techniques in Avian Anesthesia
Wyszukiwarka
Podobne podstrony:
Tully Jr 2005 Seminars in Avian and Exotic Pet Medicine
[first author] 2005 Seminars in Avian and Exotic Pet Medicine
Nevarez 2005 Seminars in Avian and Exotic Pet Medicine
[first author] 2005 Seminars in Avian and Exotic Pet Medicine 4
Pokras 2005 Seminars in Avian and Exotic Pet Medicine
Myers 2005 Seminars in Avian and Exotic Pet Medicine
Johnston 2005 Seminars in Avian and Exotic Pet Medicine
Pettifer 2005 Seminars in Avian and Exotic Pet Medicine
[first author] 2005 Seminars in Avian and Exotic Pet Medicine 1
Mosley 2005 Seminars in Avian and Exotic Pet Medicine
[first author] 2005 Seminars in Avian and Exotic Pet Medicine 2
[first author] 2005 Seminars in Avian and Exotic Pet Medicine 3
Suture Materials and Suture Selection for Use in Exotic Pet Surgical
2005 Diet and Age Affect Intestinal Morphology and Large Bowel Fermentative End Product Concentratio
Estimation of Dietary Pb and Cd Intake from Pb and Cd in blood and urine
automating with step 7 in lad and fbd simatic (1)
Key Concepts in Language and Linguistics
Guide to the properties and uses of detergents in biology and biochemistry
więcej podobnych podstron