
CME
10.1586/ERN.12.59
1061
ISSN 1473-7175
© 2012 Expert Reviews Ltd
www.expert-reviews.com
Review
Felix Luessi, Volker
Siffrin and Frauke Zipp*
Focus Program Translational
Neuroscience (FTN), Rhine Main
Neuroscience Network (rmn
2
),
Department of Neurology, University
Medical Center Mainz, Johannes
Gutenberg University Mainz,
Langenbeckstr 1, 55131 Mainz,
Germany
*Author for correspondence:
Tel.: +49 6131 17 7156
Fax: +49 6131 17 5697
frauke.zipp@unimedizin-mainz.de
In recent years it has become clear that the neuronal compartment already plays an important
role early in the pathology of multiple sclerosis (MS). Neuronal injury in the course of chronic
neuroinflammation is a key factor in determining long-term disability in patients. Viewing MS
as both inflammatory and neurodegenerative has major implications for therapy, with CNS
protection and repair needed in addition to controlling inflammation. Here, the authors’ review
recently elucidated molecular insights into inflammatory neuronal/axonal pathology in MS and
discuss the resulting options regarding neuroprotective and regenerative treatment strategies.
Neurodegeneration in multiple
sclerosis: novel treatment
strategies
Expert Rev. Neurother. 12(9), 1061–1077 (2012)
K
eywords
:
multiple sclerosis • neurodegeneration • neuronal injury • neuroprotection • treatment
Expert Review of Neurotherapeutics
2012
12
9
1061
1077
© 2012 Expert Reviews Ltd
10.1586/ERN.12.59
1473-7175
1744-8360
Neurodegeneration in multiple sclerosis: novel treatment strategies
Luessi, Siffrin & Zipp
Expert Rev. Neurother.
Review
Medscape: Continuing Medical Education Online
This activity has been planned and implemented in
accordance with the Essential Areas and policies of the
Accreditation Council for Continuing Medical Education through the joint sponsorship of
Medscape, LLC and Expert Reviews Ltd. Medscape, LLC is accredited by the ACCME to provide
continuing medical education for physicians.
Medscape, LLC designates this Journal-based CME activity for a maximum of 1 AMA PRA
Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent
of their participation in the activity.
All other clinicians completing this activity will be issued a certificate of participation. To par-
ticipate in this journal CME activity: (1) review the learning objectives and author disclosures;
(2) study the education content; (3) take the post-test with a 70% minimum passing score and
complete the evaluation at www.medscape.org/journal/expertneurothera; (4) view/print certificate.
Release date: 5 October 2012; Expiration date: 5 October 2013
Learning objectives
Upon completion of this activity, participants will be able to:
• Describe recent insights into inflammatory neuronal injury in multiple sclerosis, based on a review
• Describe methods of quantification of neuronal injury in patients with multiple sclerosis, based on
a review
• Describe applications of these findings to treatment for patients with multiple sclerosis, based on
a review
THeMed ArTICLe
y Demyelinating Diseases
For reprint orders, please contact reprints@expert-reviews.com
CME
Expert Rev. Neurother. 12(9), (2012)
1062
Review
Luessi, Siffrin & Zipp
Introduction
Multiple sclerosis (MS) is the most common chronic inflammatory
demyelinating disorder of the CNS, and the leading cause of non-
traumatic neurological disability in young adults, affecting 0.1% of
the general population in Western countries
[1]
. Approximately 85%
of patients initially experience a relapsing-remitting disease (RR-MS)
course, which is characterized by recurrent episodes of neurological
deficits, such as limb weakness, optic neuritis, ataxia and sensory
disturbances, followed by periods of remission
[2]
. Remission is not
always complete, and after a variable number of years the majority
of these patients develop a secondary progressive disease course. In
15% of patients, MS is progressive from onset without superimposed
relapses, referred to as primary progressive MS
[3]
. The etiology of
this chronic disease has not been completely understood, but epide-
miological and association studies make the interplay between envi-
ronmental factors and susceptibility genes very likely. Consequently,
these factors trigger the infiltration of circulating myelin-specific
autoreactive lymphocytes into the CNS, leading to inflammation,
demyelination and neuronal injury. Relapses are considered to be
the clinical manifestation of acute inflammatory demyelination in
the CNS, and disability progression is thought to reflect chronic
demyelination, gliosis and axonal loss. Viewing MS as both inflam-
matory and neurodegenerative has major implications for therapy,
with CNS protection and repair needed in addition to controlling
inflammation
[4]
. Here, the authors review recently elucidated
molecular insights into inflammatory neuronal/axonal pathology
in MS and discuss the resulting options regarding neuroprotective
and regenerative treatment strategies.
Recent insights into inflammatory neuronal injury
in MS
Although MS was traditionally considered to be an inflammatory
demyelinating disease of the CNS, which leaves the axons
largely intact at least at onset of the disease
[5]
, recent studies
have shown that neurodegenerative processes also play an
important role early in the pathogenesis of MS. Interestingly,
axonal damage has already been in the focus of MS research
between 1880 and 1930
[6]
. State-of-the-art histopathological
analyses of brain tissue and neuroimaging studies demonstrated
significant damage to neuronal structures with axonal loss and
neurodegeneration, which ccurs in early disease stage and most
likely leads to irreversible neurological impairment
[3,7,8]
. Axonal
pathology is particularly pronounced in active and chronic active
MS lesions throughout the disease course and is closely associated
with the presence of immune cells
[8–10]
. In addition to axonal
damage, either immediate or subsequent to acute inflammatory
infiltration, neurodegeneration continues in the progressive
stage of the disease
[4]
. Quantitative morphological studies also
detected neuronal damage within the normal-appearing white
and gray matter, devoid of obvious demyelinating lesions
[11–13]
.
These observations have led to the hypothesis that the destruction
of myelin and neurons might, at least, partially represent an
independent processes.
Quantification of neuronal injury in patients
The clinically-measurable disability progression in MS patients
is very slow in the beginning of the disease, which makes it very
difficult to monitor pathology in the neuronal compartment in
the first years of the disease. However, imaging and histopatho-
logic data clearly show that pathology in the neuronal compart-
ment is widespread and dramatic from onset of the disease
[10,14]
.
This clinicoradiologic and clinicohistopathologic paradox might
be explained by strong compensatory processes of the rather
patchy affection of the CNS in the first years of the disease until
a crucial amount of neuronal tissue is lost and these processes
decompensate.
Financial & competing interests disclosure
E
ditor
Elisa Manzotti
Publisher, Future Science Group, London, UK.
Disclosure: Elisa Manzotti has disclosed no relevant financial relationships.
CME A
uthor
Laurie Barclay
Freelance writer and reviewer, Medscape, LLC.
Disclosure: Laurie Barclay, MD, has disclosed no relevant financial relationships.
A
uthors
And
C
rEdEntiAls
Felix Luessi, MD
Department of Neurology, University Medical Center Mainz, Johannes Gutenberg University Mainz, Germany.
Disclosure: Felix Luessi, MD, has disclosed no relevant financial relationships.
Volker Siffrin
Department of Neurology, University Medical Center Mainz, Johannes Gutenberg University Mainz, Germany.
Disclosure: Volker Siffrin has disclosed no relevant financial relationships.
Frauke Zipp, MD
Department of Neurology, University Medical Center Mainz, Johannes Gutenberg University Mainz, Germany.
Disclosure: Frauke Zipp, MD, has received research grants from Teva, Novartis, Merck Serona and Bayer. She has received consultation funds from
Johnson & Johnson, Novartis, Ono and Octapharma. Her travel compensation has been provided by the aforementioned companies.
Luessi, Siffrin & Zipp
CME
1063
www.expert-reviews.com
Review
Neurodegeneration in multiple sclerosis: novel treatment strategies
To evaluate whether existing and emerging treatments for
MS have neuroprotective effects, it is essential to detect sub-
clinical disease activity. MRI techniques have been extensively
explored in this respect for use in clinical studies. Currently, it
is widely accepted to monitor contrast-enhancing lesions (CELs;
blood–brain barrier leakage) as a sign of acute inflammatory
lesions and numbers/volume of T2-hypointense lesions as a
marker of lesion accumulation over time. This approach has
been widely adopted in clinical trials
[15]
. However, advanced
MRI techniques are needed as the number of CEL is hardly and
the T2 lesion load is only weakly to moderately associated with
later disability progression
[16]
. The most promising alternative
outcome measures to quantitatively assess progressive axonal and
neuronal loss over time include change in brain volume, evo-
lution of persistent hypointense lesions on T1-weighted scans,
magnetic resonance spectroscopy, and retinal nerve fiber layer
(RNFL) thickness on optical coherence tomography (OCT) as
non-MRI technique
[17,18]
.
The assessment of whole-brain volume change with serial MRI is
one of the best-studied imaging outcome measures for MS-related
tissue destruction in the CNS
[19]
. Changes in brain volume are
relatively small, up to 0.5–1% of tissue loss per year, but appear
relatively constant over time and are highly correlated with dis-
ability progression
[20]
. Complex computational paradigms have
been established to quantify the small brain volume changes with
sufficient accuracy. These comprise structured image evaluation
using normalization of atrophy
[21]
and brain parenchymal frac-
tion determination
[22]
. The extent of brain atrophy seems to cor-
relate well with concurrent
[22]
and future disability
[23]
. However,
measurement of global brain atrophy is unspecific for location and
tissue-specific processes, such as increase in glial content and loss
of myelin or axons. Thus, interpretation of brain atrophy data
might be difficult because other factors such as aging, drug use
and comorbidities, as well as ‘pseudoatrophy’ due to absorption
of edema upon anti-inflammatory treatments, may also influence
atrophy rates
[24]
.
The evolution of persistent T1-hypointense lesions (or persis-
tent ‘black holes’ [PBHs]) is a lesion-based MRI measure that
reflects tissue rarefaction following axonal damage
[16]
and cor-
relates with disability
[17]
. A postmortem examination revealed a
strong correlation between the strength of hypointensity of the
PBH and the degree of axonal loss, with a reduction of up to 90%
in axonal density being observed in the most hypointense lesions
[25,26]
. However, similarly as with brain parenchymal fraction
determination, the assessment of PBH evolution depends on the
quality of and adherence to standardized imaging protocols. The
main problem of PBH evolution to measure treatment effects is
the generally low number of events available for analysis in the
usual time frame of clinical trials. Nonetheless, PBH evolution
is already being widely used to demonstrate neuroprotective and
reparative treatments effects
[27]
.
Magnetic resonance spectroscopic imaging is another method
that allows a noninvasive quantification of neuronal dam-
age in patients with MS
[28,29]
. Here the neuronal metabolite
N-acetyl-aspartate (NAA) – a highly specific marker of neuronal
and axonal integrity – is quantified. Abnormally low NAA val-
ues were already observed in the early stages of disease, even
before significant disability was clinically evident
[15]
. In longi-
tudinal studies, the rate of decline of NAA concentration cor-
related strongly with the rate of progression of disability assessed
by the Expanded Disability Status Scale (EDSS) over time
[30]
.
Interestingly, NAA concentration decreased more rapidly with
respect to EDSS at lower EDSS scores than at higher ones,
which is in line with findings of histopathologic studies of early
neuronal damage in MS
[10]
. Accordingly, NAA concentration
is inversely correlated with T1-hypointensity in PBHs
[31]
. These
findings highlight the value of magnetic resonance spectroscopy
for measuring the neuronal damage underlying development of
disability, which is a potential predictor for future disability
[28]
.
Furthermore, NAA is a very good marker for mitochondrial func-
tion and dysfunction, and can thus show pronounced and some-
times rapid improvement of pathological values during plaque
maturation as well as in the whole brain upon treatment with
anti-inflammatory drugs.
Magnetization transfer (MT) imaging is a technique that allows
detection of tissue loss in lesions by quantifying the capacity
of hydrated macromolecules to exchange magnetization with
surrounding free water molecules
[32]
. It is an indirect measure of
the structural integrity of brain tissue. The MT ratio correlates
well with residual axonal density
[26]
. The MT ratio seems to
predict the subsequent accumulation of disability. In a prospective
study in MS patients, the mean change in average lesion
MT ratio over the first 12 months of follow-up was the best
predictor of sustained disability after 8 years
[33]
. In addition,
a robust correlation of MT ratio with myelin content was
demonstrated, which suggests that the measurement of MT
ratios could be used to monitor potential remyelination
treatments
[34]
. All MRI-based techniques for measurement
of neurodegeneration seem to be very valuable for and widely
used under study conditions; however, they have not arrived in
everyday patient care due to the need for a very precise techniques,
and time-consuming extra data analysis.
OCT has gained a lot of interest in the field of neuroimmu-
nology. This technique uses the reflection patterns of infrared
light off the retinal layers to quantify RNFL thickness
[18]
. The
evaluation of RNFL thickness measures the unmyelinated axons
of retinal ganglion cells before their entry into the optic nerve.
In MS, and following optic neuritis, RNFL thickness corre-
lates with visual acuity, EDSS score and brain atrophy
[35–38]
.
Already 1 month after acute optic neuritis, loss of retinal nerve
fibers begins and goes on for half a year. Thus, OCT seems
to be a promising and easy to use tool for quantifying nerve
injury after clinical or subclinical acute optic neuritis. It has
been reported that the eyes of patients with MS who have no
clinical history of optic neuritis often have subclinical RNFL
thinning
[36]
, and longitudinal studies have shown that even in
the absence of an optic neuritis episode, a subset of patients will
have detectable thinning over a 2-year period
[16]
. However, one
study failed to detect significant RNFL changes over a period
of 22 months
[39]
, which might be because of the differences in

CME
Expert Rev. Neurother. 12(9), (2012)
1064
Review
Luessi, Siffrin & Zipp
machinery and precision of the technique. Hence, the value of
OCT for monitoring global CNS neurodegeneration in MS is
highly controversial and its role in everyday patient care has to
be evaluated.
In summary, quantification of neurodegeneration by imaging is
feasible in MS. Combining currently available methods seems to
be the optimal strategy to evaluate the neuroprotective capacity of
a novel treatment. New long-term studies are needed to validate
imaging markers in relation to clinical outcomes.
Mechanisms of neuronal injury
Improving the understanding of the mechanisms underlying
neurodegeneration in MS is a major challenge in experimen-
tal neuroimmunology. The underlying disease pathophysi-
ology is complex and involves the key features of the disease,
which include demyelination, inflammation, astrogliosis and
neurodegeneration. The potential causes of acute and chronic
neuronal and axonal injury are bystander damage by pro-
inflammatory neurotoxic substances; direct damage processes,
which involve cell contact-dependent mechanisms; and demy-
elination-dependent metabolic disturbances in the denuded
axons. A recently published genome-wide association study
showed that polymorphisms of immunologically relevant genes
rather than genes likely to be involved more directly in neuro-
degeneration are associated with MS
[40]
. This lends weight to
the idea that inflammation might be a relevant factor for neuro-
degeneration in MS and not a certain disposition of the neuronal
compartment itself.
Immune cell-mediated axonal injury
The inflammatory infiltrates of active and chronic active MS
lesions consist predominantly of CD4
+
T cells, CD8
+
T cells and
activated microglia/macrophages
[8,41]
. Because of the correla-
tion between the degree of inflammation and neurodegeneration
[42]
, exposure to the inflammatory milieu has been proposed as a
trigger of neurodegeneration
[43]
. However, direct cell-mediated
mechanisms have also been postulated as a cause of neuronal
pathology.
Endogenous microglia cells in the CNS are dynamic sur-
veillants of brain parenchyma integrity and rapidly react to
potential threats by encapsulation of dangerous foci, removal
of apoptotic cells and assistance with tissue regeneration in
toxin-induced demyelination
[44,45]
. In the context of nonauto-
immune pathogen-associated inflammation, the microglia
protects the neuronal compartment
[46]
. Contrarily, in MS,
microglia and macrophages are shifted toward a strongly pro-
inflammatory phenotype and may potentiate neuronal damage
by releasing proinflammatory cytokines (i.e., TNF-
α, IL-1β,
IL-6) and proinflammatory molecules such as nitric oxide,
proteolytic enzymes and free radicals
[47–49]
. In a MS animal
model of experimental autoimmune encephalomyelitis (EAE),
paralysis of microglia in vivo, resulted in substantial ameliora-
tion of the clinical signs and in strong reduction of CNS inflam-
mation, demonstrating their active involvement in damage pro-
cesses
[50]
. However, it is doubtful whether monocyte-derived
macrophages and microglia actually have the potential to influ-
ence their fate. The adaptive immune system is more likely to
direct the attack against CNS cells.
Clonally expanded CD8
+
T cells have been shown within MS
lesions as well as in the cerebrospinal fluid of MS patients
[51,52]
.
However, the significance of these CD8
+
T cells in MS patho-
genesis is controversial since there is evidence for a suppressor
function that inhibits pathogenic autoreactive CD4
+
T cells
[53–55]
and evidence for a tissue-damaging role because a signifi-
cant correlation between the extent of axonal damage and the
number of CD8
+
T cells has been reported
[10,42]
. In accordance
with the latter observation, MHC class I-restricted CD8
+
T cells
were found to induce neuronal cell death in certain immu-
nological constellations in cultured neurons and hippocam-
pal brain slices
[56,57]
. In addition, the transsection of MHC
class I-induced neurites by CD8
+
T cells has been described
[58]
,
a process that might also contribute to pathology in human dis-
ease. In contrast, a study in EAE has shown enhanced neuronal
damage in the absence of MHC class I molecules in vivo
[59]
,
supporting earlier reports on pronounced immunoregulatory
functions of CD8
+
T cells
[55,60,61]
. Up until now, direct CD8
+
T-cell-mediated neuronal damage has not been demonstrated
with sufficient evidence and a specific neuronal epitope trig-
gering CD8
+
T-cell-mediated neuronal damage in MS has not
yet been found.
Current evidence on the induction and, most likely, in the
perpetuation of MS still favors CNS-reactive CD4
+
T cells as
the single most important component in the induction of an
autoimmune response against the myelin sheath. Nevertheless,
the contribution of CD4
+
T cells to neurodegeneration is a matter
of debate. Doubts arise from the fact that CD4
+
T cells seem to
be quite rare in the lesions of MS patients – at least in later disease
stages – and that treatments with antibodies directed against
T cells and their differentiation – for example, ustekinumab
(IL-12/23 p40 neutral antibody) – did not show therapeutic
efficacy in MS patients
[62]
. However, the genetic risk of MS and
EAE is, to a substantial degree, conferred by MHC class II alleles
and to other genes involved in T-cell phenotype expression in
both the human disease and the murine disease model
[63,64]
. An
affinity between invading activated CD4
+
T cells and neurons
had not seriously been considered to date as neurons do not
express MHC class II molecules, which are required to make
target T cells accessible for this immune cell subset, and CD4
+
T cells invading the CNS in the course of neuroinflammatory
diseases are usually not specific for neuronal antigens. However,
due to recent advances in deep-tissue imaging using two-photon
microscopy, interactions between neurons and immune cells can
be investigated in vivo and in organotypic microenvironments.
These have revealed that encephalitogenic CD4
+
T cells possess
marked migratory capacities within the CNS parenchyma and
directly interact with the soma and processes of neurons, partially
leading to cell death
[65]
. Among others, the death ligand TNF-
related apoptosis-inducing ligand as a T-cell-associated effector
molecule contributes to the induction of neuronal apoptosis. It
has been shown that TNF-related apoptosis-inducing ligand
Luessi, Siffrin & Zipp
CME
1065
www.expert-reviews.com
Review
Neurodegeneration in multiple sclerosis: novel treatment strategies
expressed by CD4
+
T cells induces collateral death of neurons
in the inflamed brain and promotes EAE
[66,67]
. Importantly, by
using in vivo live imaging in EAE, a direct contact between CD4
+
T cells, particularly T helper (Th17) cells, and neurons has been
confirmed that leads to neuronal dysfunction and subsequently
cell death
[68]
. This neuronal injury mediated by Th17 cells was
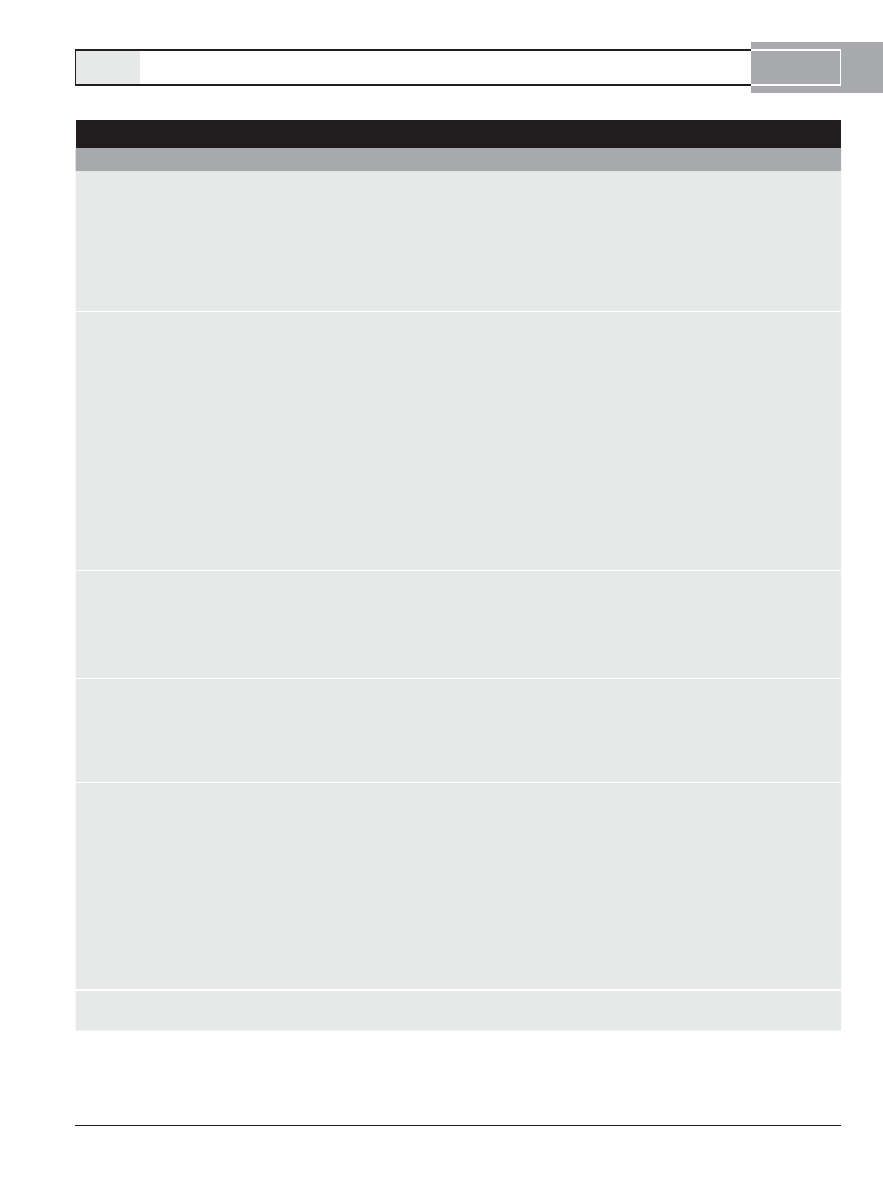
Table 1. Approved therapies in multiple sclerosis.
Compound
Proposed mechanisms
Indication
Clinical outcome
MRI outcome
Ref.
GA
Secretion of BDNF by
GA-reactive T cells
CIS
Reduces disability rate
Reduces proportion of
new lesions evolving to
black holes
[89,96,97,143]
Modulation of T-cell
activation and proliferation
RR-MS
Reduces relapse rate
Reduces gadolinium-
enhancing lesions
Augmentation of the ratio
of anti-inflammatory to
proinflammatory cytokines
Increases
N-acetyl-aspartate/creatine
ratio
IFN-
β
1a
and -
β
1b
Inhibition of T-cell
activation and
costimulation
CIS
Delay to Poser MS in
CIS patients
Reduces gadolinium-
enhancing lesions
[101,144–146]
Modulation of anti-
inflammatory and
proinflammatory cytokines
RR-MS
Reduces relapse rate
Reduces T2 lesions
Downregulation of T-cell
migration
SP-MS
(IFN-
β
1b
)
Increased time to
confirmed progression
in SP-MS
Reduces the mean
T2 lesion volume
Suppression of Th17 cell
differentiation
Reduces development of
permanent black holes
(IFN-
β
1b
)
Stimulates the production
of NGF in early stages of
the disease
Slows progressive loss of
brain tissue in CIS
patients (IFN-
β
1a
)
Mitoxantrone
B- and T-cell suppression
Active
RR-MS
Reduces relapse rate
Reduces the T2 lesion
load
[147,148]
Eliminates and deactivates
monocytes and
macrophages
SP-MS
Reduces progression of
disability
Reduces gadolinium-
enhancing lesions
Inhibits T-cell migration
Natalizumab
Inhibits transendothelial
migration of leukocytes
across the blood–brain
barrier
Active
RR-MS
Reduces relapse rate
Reduces gadolinium-
enhancing lesions
[149]
Reduces progression of
disability
Reduces T2 lesions
Fingolimod
(FTY720)
Modulates activation of
S1P receptors 1, 3–5
Active
RR-MS
Reduces relapse rate
Reduces the rate of brain
atrophy
[104]
Prevents egress of
lymphcytes from second-
ary lymphoid tissue to sites
of inflammation
Reduces risk of disability
progression
Reduces gadolinium-
enhancing lesions
Differentially retains
effector memory cells and
Th17 cells
Reduces the number of
new or enlarging
T2-hyper-intense lesions
Might promote remyelina-
tion by acting on oligo-
dendrocyte S1P5 receptors
BDNF: Brain-derived neurotrophic factor; CIS: Clinically isolated syndrome; GA: Glatiramer acetate; MS: Multiple sclerosis; RR-MS: Relapsing-remitting MS;
S1P: Sphingosine-1-phosphate; SP-MS: Secondary progressive MS; Th: T helper.
Adapted with permission from
[150].

CME
Expert Rev. Neurother. 12(9), (2012)
1066
Review
Luessi, Siffrin & Zipp
found to be lymphocyte function-associated antigen 1-dependent
and potentially reversible. These results suggest that once they
reach the CNS, CD4
+
T cells are directly involved in local
neuronal damage processes in EAE. However, these findings
based on experiences in animal models need to be confirmed in
MS patients.
Axonal degeneration as a consequence of demyelination
Although irreversible neurological disability in MS patients
results from axonal degeneration
[30,69]
, knowledge of the
mechanisms by which demyelinated axons degenerate is far
from complete. The ‘virtual hypoxia hypothesis’ postulates that
demyelination increases the energy demand in denuded axons
[43]
. To safeguard nerve conduction, since the voltage-gated Na
+
channels are usually concentrated in axons that have incom-
plete myelination, larger numbers of Na
+
channels are needed
to compensate for loss of saltatory axon potential propagation
[70,71]
. However, higher numbers of Na
+
channels necessitate an
increased energy supply to restore transaxolemmal Na
+
and K
+
gradients. In addition, an impaired axoplasmatic ATP produc-
tion in chronically demyelinated axons due to mitochondrial
dysfunction has been described
[72]
. The function of mitochon-
drial respiratory chain complex I and III was reduced by 40–50%
in mitochondrial-enriched preparations from the motor cortex of
MS patients
[73]
. Furthermore, defects of mitochondrial respira-
tory chain complex IV have been reported
[74,75]
, and have been
associated with hypoxia-like tissue injury
[76]
and reduced brain
NAA concentration
[77]
. The combination of increased energy
requirements and compromised ATP production as a result of
demyelination leads to a vicious circle by the loss of Na
+
/K
+
ATPase
[78]
, which contributes to an increased intracellular Na
+
.
Consequently, Ca
2+
is released from intracellular stores
[79]
and
the direction of the Na
+
/Ca
2+
exchanger is reversed, resulting
in additional extracellular Ca
2+
influx
[80]
. That in turn leads
to Ca
2+
-mediated degenerative responses such as cytoskeleton
disruption and cell death
[81,82]
.
Aside from the summarized dramatic ion and energy imbal-
ances following demyelination, the lack of structural as well as
trophic support to axons provided by myelin and oligodendro-
cytes also contributes to neurodegeneration
[83,84]
. In vitro evi-
dence suggests that oligodendrocytes produce trophic factors such
as IGF-1 and neuregulin that promote normal axon function and
survival
[85,86]
. Moreover, mice lacking structural components of
compact myelin such as proteolipid protein demonstrated a late
onset, slowly progressing axonopathy
[87]
. However, oligoden-
drocyte dysfunction independent of and prior to inflammation
in classic MS still lacks direct evidence.
Therapeutic approaches to neuronal degeneration
in MS
All currently approved MS therapeutics primarily target inflam-
mation. However, recent insights into inflammatory neurodegen-
eration in MS indicate that an optimized therapeutic approach
should specifically tackle the promotion of neuroprotection and
repair to prevent chronic disability. This is even more important
as serious side effects of the highly effective anti-inflammatory
therapy regimen in MS and the need for a life-long treatment for
the authors’ MS patients preclude the majority of patients from
high-efficiency therapeutics, as risk–benefit evaluations are in
favour of the basic therapeutics.
The potentially neuroprotective effects of approved and novel
treatment strategies and most importantly direct neuroprotec-
tives, which might be used as an add-on to established basic
anti-inflammatory therapeutics, will be discussed below.
Current therapeutic concepts
At present, five disease-modifying drugs have been approved for
MS therapy
(t
ablE
1)
. Glatiramer acetate (GA) and the IFN-
β
preparations have been established as first-line disease-modifying
immune-modulatory treatments that reduce the relapse rate and
ameliorate relapse severity
[88]
, but also slow the progression of
disability in patients with RR-MS
[89,90]
. Through binding to a
specific receptor, IFN-
β exerts a variety of immunological effects.
Presumed mechanisms of action include inhibition of T-cell
activation and co-stimulation, modulation of anti-inflammatory
and proinflammatory cytokines, and downregulation of T-cell
migration
[91,92]
. GA is a synthetic peptide composed of a random
mix of four amino acids resembling myelin basic protein that
leads to a shift in immune response from Th1 to a more anti-
inflammatory Th2-profile
[93]
. GA also takes effect by limiting
T cells through downregulating proliferation, activation
and induction of apoptosis
[88,94]
. There is evidence that in
addition to their immune-modulatory effects, GA and IFN-
β
also appear to have neuroprotective effects. GA-specific T cells
have demonstrated an increased production of brain-derived
neurotrophic factor (BDNF), which propagates neuronal survival
[95]
. Furthermore, GA treatment was associated with a reduction
of PBHs in patients
[96]
and increased the NAA concentration
in magnetic resonance spectroscopy
[97]
, which implies that this
treatment may reduce axonal injury in developing lesions and
maintain axonal metabolic function. It has been shown that
IFN-
β stimulates the production of NGF in early stages of disease
and inhibits microglia and gliosis
[98,99]
. In MRI-based studies,
treatment with IFN-
β was associated with a reduced development
of PBH as well as a decrease in brain atrophy rate
[22,100,101]
.
Whether these findings are mediated by direct neuroprotective
effects of GA and IFN-
β or result from their anti-inflammatory
properties remains to be established.
The newly approved immune-modulatory treatment with
Fingolimod (FTY720) is also supposed to have neuroprotective
properties. Following in vivo phosphorylation, it acts as a modula-
tor of the activity of sphingosine 1-phosphate receptors, thus pre-
venting lymphocyte egress from secondary lymphatic organs and
subsequent migration to sites of inflammation
[102]
. It might also
diminish astrogliosis and promote remyelination via sphingosine
1-phosphate receptors on astrocytes and oligodendrocytes
[103]
.
In a recent 2-year Phase III trial, fingolimod-treated patients had
a reduced rate of disability progression and brain volume loss as
well as a smaller increase in T1-hypointense lesion volume than
patients who were given placebo
[104]
.
Luessi, Siffrin & Zipp
CME
1067
www.expert-reviews.com
Review
Neurodegeneration in multiple sclerosis: novel treatment strategies
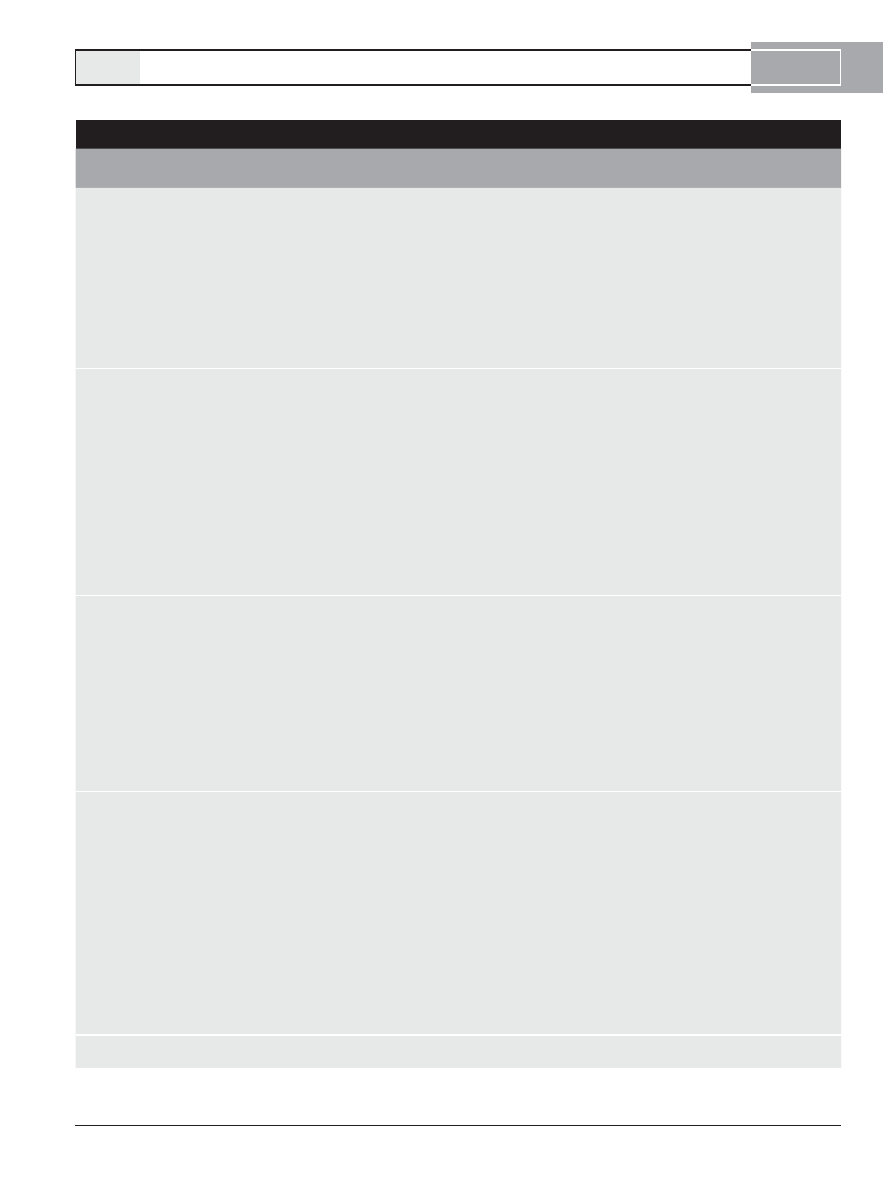
Table 2. Novel therapies in multiple sclerosis currently undergoing clinical development.
Compound Proposed mechanisms
Phase
Indication n
Study design
Duration
(months)
Outcome
Ref.
Alemtuzumab • mAb to CD52, a surface
antigen of unknown function
on lymphocytes, monocytes
and dendritic cells
• Induces a sustained T-cell
depletion and a transient
B-cell depletion
• Increases levels of BAFF
and regulatory T cells
• Increases secretion of BDNF
by lymphocytes
II
RR-MS
334
12 mg alemtuzumab/
day, eight times
a year
versus
24 mg alemtuzumab/
day, eight times a
year
versus
44 μg IFN-
β
1a
three
times a week
36
• Improves mean
disability score
• Reduces
relapse rate
• Reduces
gadolinium-
enhancing
lesions
• Reduces brain
atrophy rate
[115,116]
Daclizumab
• mAB to CD25, a
component of the high-
affinity IL-2 receptor on
T cells
• Inhibition of early IL-2
receptor signal transduction
events
• Blocks T-cell activation and
expansion
• Causes expansion of
regulatory CD56 bright
natural killer cells
• Decreases the number of
CD8
+
T cells
II
RR-MS
230
2 mg daclizumab/kg
bodyweight every
2 weeks
versus
1 mg daclizumab/kg
bodyweight every
4 weeks
versus
placebo as add-on to
IFN-
β
18
• Trend toward
reducing relapse
rate
• Reduces
number of new
or enlarging
T2-hyperintense
lesions
• Reduces
gadolinium-
enhancing
lesions
[119]
Fumarate
(BG00012)
• Activation of transcription
factor Nrf2
• Induction of Th2-like
cytokines
• Induction of apoptosis in
activated T cells
• Downregulation of
intracellular adhesion
molecules and vascular
adhesion molecules
• Upregulation of antioxidant
response elements
II
RR-MS
257
120 mg fumarate/day
versus
360 mg fumarate/day
versus
720 mg fumarate/day
versus
placebo
12
• Trend toward
reducing relapse
rate
• Reduces
gadolinium-
enhancing
lesions
• Reduces
number of new
or enlarging
T2-hyperintense
lesions
[108]
Laquinimod
• Immunmodulator related to
linomide with unknown
molecular target
• Anti-inflammatory activity
via Th1–Th2 shift
• Modulation of BDNF
secretion
III
RR-MS
1106
0.6 mg laquinimod/
day
versus
placebo
24
• Reduces
relapse rate
• Lowers risk of
sustained
progression of
disability
• Reduces
gadolinium-
enhancing
lesions
• Reduces
number of new
or enlarging
T2-hyperintense
lesions
[110]
BAFF: B-cell-activating factor of the tumor necrosis factor family; BDNF: Brain-derived neurotrophic factor; mAb: Monoclonal antibody; Nef2: Nuclear factor
E2-related factor 2; RR-MS: Relapsing-remitting multiple sclerosis; SP-MS: Secondary progressive multiple sclerosis; Th: T helper.

CME
Expert Rev. Neurother. 12(9), (2012)
1068
Review
Luessi, Siffrin & Zipp
Novel therapies undergoing clinical development
Several new compounds are currently undergoing clinical devel-
opment for MS therapy, including immunomodulatory as well
as nonselective and selective immunosuppressive drugs
(t
ablE
2)
.
The mechanism of action of some of these therapies under
development is not well understood. Agents such as cladribine
and teriflunomide are antiproliferative agents that take effect
by interfering with DNA synthesis, nucleotide metabolism and
signaling pathways of activated immune cells
[105,106]
. In a 2-year
Phase III trial, treatment with cladribine tablets significantly
reduced relapse rates, the risk of disability progression and MRI
measures of disease activity
[107]
. Despite these promising results,
the European Medicines Agency did not approve cladribine for
the treatment of MS because of safety concerns in the context of
an increased number of patients with cancer observed in trials
with cladribine.
A more specific immune-modulatory mode of action has been
proposed for two compounds currently in advanced clinical tri-
als, dimethylfumarate (BG00012) and laquinimod. A 24-week
Phase II trial demonstrated that dimethylfumarate treatment
led to a significant reduction of CEL and PBHs
[108]
, likely as
a result of the activation of the neuroprotective nuclear factor
E2-related factor 2 transcription pathway
[109]
. Laquinimod
showed a modest reduction of the annualized relapse rate and
a reduction in the risk of confirmed disability progression in a
24-month Phase III trail with RR-MS patients
[110]
. In this study,
treatment with laquinimod was also associated with reduced
MRI-measured disease activity. The effect by which laquinimod
exerts its anti-inflammatory activity may be due to its impact
on the dendritic cell compartment and a Th1–Th2 shift
[111,112]
.
Furthermore, laquinimod ameliorated EAE via BDNF-dependent
mechanisms, which may contribute to neuroprotection
[113]
.
Targeting mechanisms of the immune system with biologics
such as recombinant antibodies might provide additional selective
treatment strategies for MS. A possible candidate is alemtuzumab,
a humanized monoclonal antibody targeting the CD52 antigen,
which is a protein of unknown function expressed on the surface
of T and B cells, natural killer (NK) cells, a majority of monocytes
and macrophages and some dendritic cells
[114]
. The binding of
alemtuzumab results in rapid and prolonged depletion of targeted
cells by complement-dependent and antibody-dependent T cellu-
lar toxicity. In a recent 3-year Phase II trial, alemtuzumab signifi-
cantly reduced the risk of relapse, brain volume loss and accumu-
lation of disability in early RR-MS compared with IFN-
β
1a
[115]
.
Patients treated with alemtuzumab experienced an improvement
in disability at 6 months that was sustained in the 5-year follow-
up study
[116]
. These findings for alemtuzumab treatment might
result, in part, from neuroprotection associated with increased
lymphocytic delivery of BDNF to the CNS
[117]
. Alemtuzumab
is now being investigated in Phase III trials, which will determine
the risk–benefit ratio of this potent agent, since alemtuzumab led
to significant side effects including autoimmune thyroid disorders
(>10%) and idiopathic thrombocytopenic purpura (2.8%).
This incidence of rare but severe side effects highlights the need
for further strategies preserving the high efficacy but minimiz-
ing the risk. Daclizumab – a humanized anti-CD25 monoclonal
antibody – appears to be an alternative with a favorable risk profile
thus far. It is directed against the IL-2 receptor (IL-2R), which is
upregulated on activated T cells. In EAE, IL-2R antibody therapy
has been shown to induce the expansion of an immunoregulatory
subset of NK cells, most likely by increasing free IL-2 levels, which
express high levels of CD56
[118]
. Data from a recent Phase II
trial showed that add-on treatment with daclizumab reduced the
number of new or enlarged CEL compared with IFN-
β alone
[119]
.
Table 2. Novel therapies in multiple sclerosis currently undergoing clinical development (cont.).
Compound Proposed mechanisms
Phase
Indication n
Study design
Duration
(months)
Outcome
Ref.
Rituximab
• mAB to CD20, a surface
antigen expressed on
B cells, but not on
plasma cells
• Causes rapid depletion of
B cells
II
RR-MS
104
1000 mg rituximab
on days 1 and 15
versus
placebo
12
• Reduces
relapse rate
• Reduces
gadolinium-
enhancing
lesions
[151]
Teriflunomide • Active metabolite of
leflunomide used for
rheumtoid arthritis
Impairs cellular nucleotide
metabolism by inhibiting
the dihydroorotate
dehydrogenase
• Suppresses tyrosine
kinases involved in signal
transduction pathways
II
RR-MS
SP-MS
179
7 mg teriflunomide/
day versus
14 mg teriflunomide/
day versus
placebo
9
• Trend toward
reducing relapse
rate
• Reduces
gadolinium-
enhancing
lesions
• Reduces
number of new
or enlarging
T2-hyperintense
lesions
[142]
BAFF: B-cell-activating factor of the tumor necrosis factor family; BDNF: Brain-derived neurotrophic factor; mAb: Monoclonal antibody; Nef2: Nuclear factor
E2-related factor 2; RR-MS: Relapsing-remitting multiple sclerosis; SP-MS: Secondary progressive multiple sclerosis; Th: T helper.
Luessi, Siffrin & Zipp

CME
1069
www.expert-reviews.com
Review
Neurodegeneration in multiple sclerosis: novel treatment strategies
Promising therapeutic concepts with putative
neuroprotective effects
New therapeutic strategies have evolved that specifically tar-
get the neurodegenerative aspect of MS
(t
ablE
3)
. Following up
on the findings that demyelination leads to an altered energy
demand and changes in intracellular ion homeostasis in neurons,
several ion channel blockers already in use for other medical
conditions are now being investigated in CNS autoimmun-
ity. Evidence from animal studies has shown beneficial effects
in rats with chronic EAE for up to 180 days after treatment
with phenytoin
[120]
, a Na
+
channel blocker commonly used
for epilepsy. Interestingly, when the study was repeated using
either phenytoin or carbamazepine, another antiepileptic with
Na
+
channel blocker capacities, the animals became acutely
worse after the withdrawal of either drug
[121]
, indicating that
more work needs to be done to understand the consequences
of the long-term effects of Na
+
channel blockers and of their
withdrawal in MS. Two other Na
+
-blocking agents, the anti-
arrhythmic agent flecainide and the antiepileptic lamotrigine,
have now been shown to improve axonal survival and decrease
disability in EAE-affected rats
[122,123]
. However, in a Phase II
study in patients with secondary progressive disease course,
lamotrigine showed an increase of cerebral volume loss which
was not clinically relevant, but could not be explained
[123]
.
This ‘pseudoatrophy’, seen in the early stages of this trial under
lamotrigine treatment, indicates that the choice of this trial end
point was not adequate. It highlights the importance of clini-
cal design and selection of paraclinical markers to develop trial
protocols that are adequate to detect neuroprotective effects.
Another clinical study of the antiepileptic drug topiramate,
which has partial Na
+
channel-blocking capabilities, in combi-
nation with IFN-
β in patients with RR-MS is currently under-
way. A direct neuroprotective effect of Na
+
channel blockers
remains to be demonstrated. In addition, anti-inflammatory
mechanisms on microglia and macrophages have been suggested
[124]
, which might lead to the rebound of disease after treatment
termination
[121]
.
In light of the ‘virtual hypoxia hypothesis’, promoting remy-
elination by blocking the transmembrane protein Lingo-1 is
another promising strategy to prevent neuronal damage
[43]
.
Treatment with an antibody of Lingo-1 has been demonstrated
to prevent and therapeutically improve EAE symptoms
[125]
.
This is reflected biologically through improved axonal integrity,
as confirmed by magnetic resonance diffusion tensor imaging
and by newly formed myelin sheaths, as determined by elec-
tron microscopy. The anti-Lingo-1 antibody BIIB033 is cur-
rently being i nvestigated in a Phase I study with MS patients
(ClinicalTrials.gov identifier: NCT01244139).
The blockade of voltage-gated Ca
2+
channels (VGCC) is a
potentially promising target, as the elevated intracellular Ca
2+
lev-
els lead to axonal damage through activation of different enzymes,
in particular proteases. In a study of EAE-affected rats, the effect
of bepridil, a broad-spectrum Ca
2+
channel blocker, was com-
pared with nitrendipine, which is a blocker of
l
-type VGCCs.
Both drugs prevented axonal loss and disablity in treated animals
[126]
. However, clinical trials in MS patients are not available at
the moment.
Intracellular Ca
2+
is also increased by the excitatory neuro-
transmitter glutamate via
α-amino-3-hydroxy-5-methyl-4-
isoxazolepropionic acid (AMPA)/kainate receptors. Antagonism
of AMPA/kainate receptors in EAE models resulted in improved
disability and decreased apoptosis of spinal cord neurons
[127,128]
.
With respect to MS and EAE, the detailed underlying mechanism
of action remains to be elucidated to further explain the treat-
ment effects. In addition, the unexpected rebound of disease after
withdrawal of AMPA/kainate receptor antagonists in EAE needs
further investigation
[128]
.
Among potential candidate compounds for neuroprotection,
erythropoietin – a hemapoietic growth factor commonly used to
treat anaemia – is another promising agent. Erythropoietin and
its receptor are widely expressed in the CNS and appear to have a
beneficial effect on several models of neurological injury including
ischemia, trauma and epilepsy
[129,130]
. EAE studies have indi-
cated benefits in inflammatory demyelination through inhibition
of proinflammatory cytokines
[131]
. An early trial in MS demon-
strated clinical and electrophysiological improvement upon high-
dose erythropoietin treatment for half a year
[132]
. However, MRI
volumetric analysis of total brain and ventricles did not uncover
changes compared with baseline upon treatment with erythro-
poietin. Results of a larger, randomized controlled study are now
awaited.
Cannabis is used by MS patients for relief from a variety of
symptoms
[133]
, despite the equivocal results of several clinical trials
[134]
. Improved knowledge about the major psychoactive ingredi-
ent of cannabis,
δ-9-tetrahydrocannabinol, and its CB1 and CB2
receptors has resulted in an increase of experimental data from
MS animal models. In vitro evidence suggests that cannabinoids
have an effect on several potential mechanisms of axonal injury,
including glutamate release
[135]
, oxidative free radicals as well as
damaging Ca
2+
influx
[136]
. Furthermore, exogenous agonists of the
cannabinoid CB1 receptor have possible neuroprotective effects in
EAE animal models
[137]
, and strategies to increase the endogenous
cannabinoid anandamide also appear to attenuate the clinico-
pathological features of EAE
[138]
. Despite these promising results,
neuroprotective effects in MS by canna binoids and the modulation
of the endocannabinoid system must still be established.
Statins, primarily used as effective cholesterol-lowering agents,
are now recognized to have unexpected neuroprotective effects,
which have been shown in animal models of MS
[139]
. In an MRI-
based study in patients with RR-MS, treatment with atorva statin,
alone or in combination with IFN-
β, led to a substantial reduction
in the number and volume of CEL
[139]
. Moreover, a clinical study
in RR-MS suggested that adding statins to IFN-
β may reduce the
relapse rate compared with IFN-
β alone
[140]
. However, it has been
shown that statins impair remyelination in vitro and in vivo
[141]
.
The clinical implication of this finding for statin treatment in
MS patients remains to be elucidated.
Combining anti-inflammatory and neuroprotective effects
should result in more efficient therapy. In light of this, the authors
are currently conducting a clinical controlled treatment trial in
CME
Expert Rev. Neurother. 12(9), (2012)
1070
Review
Luessi, Siffrin & Zipp
Table 3. Promising therapeutic approaches with putative neuroprotective effects in multiple sclerosis.
Compound
Proposed mechanisms
Phase
Indication
n
Study
design
Duration
(months)
Outcome
Ref.
Amiloride
• Blocks ASIC1
• Inhibits influx of sodium
and calcium into axons
and oligodendrocytes
• Protects both neurons
and myelin from damage
in EAE
II
(planned)
RR-MS
[152,153]
Cannabinoids
(
Δ9-THC)
• Modulation of
cannabinoid receptor
activation
• Reduces leukocyte
rolling and adhesion to
cerebral microvessels via
CB(2) receptor
• Reduces immune cell
invasion into CNS
II
RR-MS
SP-MS
PP-MS
657
Body-
weight-
adjusted
dose of
Δ9-THC
(maximum
25 mg/day)
versus
placebo
4
[154,155]
Epigallocatechin-
3-gallate
• Limits brain
inflammation and
neuronal damage in EAE
• Abrogates proliferation
and TNF-
α production of
encephalitogenic T cells
Protects against neuronal
injury induced by
N-methyl-
d
-aspartate or
TRAIL
• Directly blocks the
formation of neurotoxic
reactive oxygen species
in neurons
II
(ongoing)
RR-MS
800 mg
EGCG/day
versus
placebo
18
[156,157]
Erythropoietin
• Ameliorates the clinical
course in EAE
Reduces proinflammatory
cytokines
• Stabilizes blood–brain
barrier integrity
• Increases BDNF-positive
cells
• Stimulating oligoden-
drogenesis
II
PP-MS
SP-MS
10
48,000 IU
rhEPO
bi-weekly
versus
8000 IU
rhEPO
bi-weekly
12
• Reduces
disability
score
• Improves
cognitive
performance
• Trend
toward
improving
maximum
walking
distance
[130–132]
Flupirtine
• Centrally acting
nonopioid analgesic drug
• Neuroprotective via
activation of inwardly
rectifying potassium
channels
• Inhibits TRAIL-mediated
death of neurons
• Increases neuronal
survival by Bcl-2
upregulation
II
(ongoing)
RR-MS
300 mg
flupirtine/day
versus
placebo
12
[158,159]
AMPA:
α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid; ASIC1: Acid-sensing ion channel-1; BDNF: Brain-derived neurotrophic factor; EAE: Experimental
autoimmune encephalomyelitis; EGCG: Epigallocatechin gallate; PP-MS: Primary-progressive multiple sclerosis; rhEPO: Recombinant human erythropoietin;
RR-MS: Relapsing-remitting multiple sclerosis; SP-MS: Secondary progressive multiple sclerosis; THC: Tetrahydrocannabinol; TRAIL: TNF-related apoptosis-inducing ligand.
Luessi, Siffrin & Zipp
CME
1071
www.expert-reviews.com
Review
Neurodegeneration in multiple sclerosis: novel treatment strategies
RR-MS to investigate the efficacy of epigallocatechin-3-gallate.
In experimental studies, this flavonoid exhibited antioxidant and
proteasome inhibitory capacities, and thus anti-inflammatory as
well as neuroprotective effects in chronic neuroinflammation
[142]
.
Expert commentary & five-year view
Over the last decades, the immunological aspects of MS have
been extensively investigated, focusing on the immune system’s
contribution in the pathogenesis of the myelin-targeted inflam-
matory attack. The rediscovery of the importance of neuronal
damage in MS has now drawn attention to the neurobiologi-
cal consequences of autoimmune demyelination. As outlined
here, deeper molecular insights into the mechanisms of inflam-
matory neurodegeneration in MS will be necessary to further
identify molecular targets for the development of more efficient
treatment strategies.
Table 3. Promising therapeutic approaches with putative neuroprotective effects in multiple sclerosis (cont.).
Compound
Proposed mechanisms
Phase
Indication
n
Study
design
Duration
(months)
Outcome
Ref.
Lamotrigine
• Blocks voltage-sensitive
Na
+
channels
• Prevents from intracel-
lular calcium accumulation
via Na
+
/Ca
2+
exchanger
Neuroprotective in EAE
II
SP-MS
120
40 mg
lamotrigine/
day
versus
placebo
24
• Reduces the
deterioration
of the
timed 25-foot
walk
• No beneficial
effect on
cerebral
volume loss
[123]
Riluzole
• Modulates glutamate
receptors
• Inhibits the release of
glutamate from nerve
terminals
• Suppression of disease
activity and reduction of
axonal damage in EAE
II
PP-MS
15
100 mg
riluzole/day
24
• Reduces the
development
of T1-hypo-
intense
lesions
• Reduces
the rate of
cervical cord
atrophy
• Only slightly
decreases
the rate
of brain
atrophy
[160]
Statins
• Attenuates immune
response by modulation
of dendritic cell
function
• Inhibition of rho family
functions promotes myelin
repair in EAE
• Increases serum levels of
the regulatory cytokine
IL-10
II
RR-MS
85
40 mg
simvastatin/
day
versus
placebo as
add-on to
30 μg IFN-
β
1a
once weekly
12
• Reduces
relapse rate
• Trend toward
reducing
disability
progression
• Trend toward
reducing
gadolinium-
enhancing
lesions
[140]
Topiramate
• Blocks voltage-sensitive
Na
+
channels
• Inhibits excitatory
neurotransmission
• Enhances GABA-
activated chloride
channels
• Modulates kainate and
AMPA receptors
II (ongoing) RR-MS
Topiramate
versus
placebo as
add-on to
30 μg IFN-
β
1a
once weekly
[161]
AMPA:
α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid; ASIC1: Acid-sensing ion channel-1; BDNF: Brain-derived neurotrophic factor; EAE: Experimental
autoimmune encephalomyelitis; EGCG: Epigallocatechin gallate; PP-MS: Primary-progressive multiple sclerosis; rhEPO: Recombinant human erythropoietin;
RR-MS: Relapsing-remitting multiple sclerosis; SP-MS: Secondary progressive multiple sclerosis; THC: Tetrahydrocannabinol; TRAIL: TNF-related apoptosis-inducing ligand.
CME
Expert Rev. Neurother. 12(9), (2012)
1072
Review
Luessi, Siffrin & Zipp
Key issues
• Damage to the neuronal compartment already plays an important role early in the pathology of multiple sclerosis.
• The neuronal injury in the course of chronic neuroinflammation is a key factor determining long-term disability in patients.
• Quantification of neurodegeneration by modern imaging techniques is necessary to evaluate the neuroprotective capacity of novel
treatments.
• Viewing multiple sclerosis as both inflammatory and neurodegenerative has major implications for therapy, with CNS protection and
repair being needed in addition to controlling inflammation.
• Deeper molecular insights into the mechanisms of inflammatory neurodegeneration in multiple sclerosis will be necessary to further
identify potential drug targets.
References
Papers of special note have been highlighted as:
• of interest
•• of considerable interest
1
Noseworthy JH, Lucchinetti C, Rodriguez
M, Weinshenker BG. Multiple sclerosis.
N. Engl. J. Med. 343(13), 938–952
(2000).
2
O’Connor P; Canadian Multiple Sclerosis
Working Group. Key issues in the diagnosis
and treatment of multiple sclerosis. An
overview. Neurology 59(6 Suppl. 3), S1–33
(2002).
3
Lublin FD, Reingold SC. Defining the
clinical course of multiple sclerosis: results
of an international survey. National
Multiple Sclerosis Society (USA) Advisory
Committee on Clinical Trials of New
Agents in Multiple Sclerosis. Neurology
46(4), 907–911 (1996).
4
Siffrin V, Vogt J, Radbruch H, Nitsch R,
Zipp F. Multiple sclerosis – candidate
mechanisms underlying CNS atrophy.
Trends Neurosci. 33(4), 202–210 (2010).
5
Charcot JM. [Clinical Lectures on the
Diseases of the Nervous System from
Salpetrière Hospital (4th Edition).] New
Sydenham Society, Bourneville, Paris
(1880).
6
Kornek B, Lassmann H. Axonal pathology
in multiple sclerosis. A historical note.
Brain Pathol. 9(4), 651–656 (1999).
7
Inglese M, Ge Y, Filippi M, Falini A,
Grossman RI, Gonen O. Indirect evidence
for early widespread gray matter
involvement in relapsing-remitting multiple
sclerosis. Neuroimage 21(4), 1825–1829
(2004).
8
Ferguson B, Matyszak MK, Esiri MM,
Perry VH. Axonal damage in acute
multiple sclerosis lesions. Brain 120(Pt 3),
393–399 (1997).
9
Trapp BD, Peterson J, Ransohoff RM,
Rudick R, Mörk S, Bö L. Axonal
transection in the lesions of multiple
sclerosis. N. Engl. J. Med. 338(5), 278–285
(1998).
•
Presents transected axons as common
findings in lesions of multiple sclerosis.
10
Kuhlmann T, Lingfeld G, Bitsch A,
Schuchardt J, Brück W. Acute axonal
damage in multiple sclerosis is most
extensive in early disease stages and
decreases over time. Brain 125(Pt 10),
2202–2212 (2002).
11
Bø L, Vedeler CA, Nyland H, Trapp BD,
Mørk SJ. Intracortical multiple sclerosis
lesions are not associated with increased
lymphocyte infiltration. Mult. Scler. 9(4),
323–331 (2003).
12
Kutzelnigg A, Lucchinetti CF, Stadelmann C
et al. Cortical demyelination and diffuse
white matter injury in multiple sclerosis.
Brain 128(Pt 11), 2705–2712 (2005).
13
Bjartmar C, Kinkel RP, Kidd G,
Rudick RA, Trapp BD. Axonal loss in
normal-appearing white matter in a
patient with acute MS. Neurology 57(7),
1248–1252 (2001).
14
De Stefano N, Narayanan S, Francis GS
et al. Evidence of axonal damage in the
early stages of multiple sclerosis and its
relevance to disability. Arch. Neurol. 58(1),
65–70 (2001).
15
Barkhof F, Calabresi PA, Miller DH,
Reingold SC. Imaging outcomes for
neuroprotection and repair in multiple
sclerosis trials. Nat. Rev. Neurol. 5(5),
256–266 (2009).
•• Comprehensive review emphasizing the
importance of new outcome measures in
multiple sclerosis treatment.
16
Barkhof F. MRI in multiple sclerosis:
correlation with expanded disability status
scale (EDSS). Mult. Scler. 5(4), 283–286
(1999).
17
Zipp F. A new window in multiple sclerosis
pathology: non-conventional quantitative
magnetic resonance imaging outcomes.
J. Neurol. Sci. 287(Suppl. 1), S24–S29
(2009).
18
Bock M, Brandt AU, Dörr J et al. Time
domain and spectral domain optical
coherence tomography in multiple
sclerosis: a comparative cross-sectional
study. Mult. Scler. 16(7), 893–896
(2010).
19
Zivadinov R, Reder AT, Filippi M et al.
Mechanisms of action of disease-modifying
agents and brain volume changes in
multiple sclerosis. Neurology 71(2),
136–144 (2008).
20
Simon JH. Brain atrophy in multiple
sclerosis: what we know and would
like to know. Mult. Scler. 12(6), 679–687
(2006).
21
Smith SM, De Stefano N, Jenkinson M,
Matthews PM. Normalized accurate
measurement of longitudinal brain change.
J. Comput. Assist. Tomogr. 25(3), 466–475
(2001).
22.
Rudick RA, Fisher E, Lee JC, Simon J,
Jacobs L. Use of the brain parenchymal
fraction to measure whole-brain atrophy in
relapsing-remitting MS. Multiple Sclerosis
Collaborative Research Group. Neurology
53(8), 1698–1704 (1999).
23
Fisher E, Rudick RA, Simon JH et al.
Eight-year follow-up study of brain atrophy
in patients with MS. Neurology 59(9),
1412–1420 (2002).
24
Zivadinov R, Stosic M, Cox JL, Ramasamy
DP, Dwyer MG. The place of conventional
MRI and newly emerging MRI techniques
in monitoring different aspects of treatment
outcome. J. Neurol. 255(Suppl. 1), 61–74
(2008).
25
van Walderveen MA, Kamphorst W,
Scheltens P et al. Histopathologic correlate
of hypointense lesions on T1-weighted
spin-echo MRI in multiple sclerosis.
Neurology 50(5), 1282–1288 (1998).
26
van Waesberghe JH, Kamphorst W,
De Groot CJ et al. Axonal loss in multiple
sclerosis lesions: magnetic resonance
imaging insights into substrates of
disability. Ann. Neurol. 46(5), 747–754
(1999).
27
Giacomini PS, Arnold DL. Non-
conventional MRI techniques for
measuring neuroprotection, repair and
Luessi, Siffrin & Zipp

CME
1073
www.expert-reviews.com
Review
Neurodegeneration in multiple sclerosis: novel treatment strategies
plasticity in multiple sclerosis. Curr. Opin.
Neurol. 21(3), 272–277 (2008).
28
De Stefano N, Filippi M. MR spectroscopy
in multiple sclerosis. J. Neuroimaging
17(Suppl. 1), 31S–35S (2007).
29
Bjartmar C, Kidd G, Mörk S, Rudick R,
Trapp BD. Neurological disability
correlates with spinal cord axonal loss and
reduced N-acetyl aspartate in chronic
multiple sclerosis patients. Ann. Neurol.
48(6), 893–901 (2000).
30
De Stefano N, Matthews PM, Fu L et al.
Axonal damage correlates with disability in
patients with relapsing-remitting multiple
sclerosis. Results of a longitudinal magnetic
resonance spectroscopy study. Brain
121(Pt 8), 1469–1477 (1998).
31
van Walderveen MA, Barkhof F, Pouwels
PJ, van Schijndel RA, Polman CH,
Castelijns JA. Neuronal damage in
T1-hypointense multiple sclerosis lesions
demonstrated in vivo using proton
magnetic resonance spectroscopy.
Ann. Neurol. 46(1), 79–87 (1999).
32
Filippi M, Rocca MA. Magnetization
transfer magnetic resonance imaging in the
assessment of neurological diseases.
J. Neuroimaging 14(4), 303–313 (2004).
33
Agosta F, Rovaris M, Pagani E et al.
Magnetization transfer MRI metrics
predict the accumulation of disability
8 years later in patients with multiple
sclerosis. Ann. Neurol. 46, 747–754
(1999).
34
Schmierer K, Scaravilli F, Altmann DR,
Barker GJ, Miller DH. Magnetization
transfer ratio and myelin in postmortem
multiple sclerosis brain. Ann. Neurol.
56(3), 407–415 (2004).
35
Trip SA, Schlottmann PG, Jones SJ et al.
Retinal nerve fiber layer axonal loss and
visual dysfunction in optic neuritis. Ann.
Neurol. 58(3), 383–391 (2005).
36
Fisher JB, Jacobs DA, Markowitz CE et al.
Relation of visual function to retinal nerve
fiber layer thickness in multiple sclerosis.
Ophthalmology 113(2), 324–332 (2006).
37
Pulicken M, Gordon-Lipkin E, Balcer LJ,
Frohman E, Cutter G, Calabresi PA.
Optical coherence tomography and disease
subtype in multiple sclerosis. Neurology
69(22), 2085–2092 (2007).
38
Gordon-Lipkin E, Chodkowski B, Reich
DS et al. Retinal nerve fiber layer is
associated with brain atrophy in multiple
sclerosis. Neurology 69(16), 1603–1609
(2007).
39
Serbecic N, Aboul-Enein F, Beutelspacher
SC et al. High resolution spectral domain
optical coherence tomography (SD-OCT)
in multiple sclerosis: the first follow-up
study over two years. PLoS ONE 6(5),
e19843 (2011).
40
Sawcer S, Hellenthal G, Pirinen M et al.;
International Multiple Sclerosis Genetics
Consortium; Wellcome Trust Case Control
Consortium 2. Genetic risk and a primary
role for cell-mediated immune mechanisms
in multiple sclerosis. Nature 476(7359),
214–219 (2011).
41
Traugott U, Reinherz EL, Raine CS.
Multiple sclerosis. Distribution of T cells,
T cell subsets and Ia-positive macrophages
in lesions of different ages.
J. Neuroimmunol. 4(3), 201–221 (1983).
42
Bitsch A, Schuchardt J, Bunkowski S,
Kuhlmann T, Brück W. Acute axonal
injury in multiple sclerosis. Correlation
with demyelination and inflammation.
Brain 123(Pt 6), 1174–1183 (2000).
43
Trapp BD, Stys PK. Virtual hypoxia and
chronic necrosis of demyelinated axons in
multiple sclerosis. Lancet Neurol. 8(3),
280–291 (2009).
•• Comprehensive review on the mechanisms
of axonal injury.
44
Nimmerjahn A, Kirchhoff F, Helmchen F.
Resting microglial cells are highly dynamic
surveillants of brain parenchyma in vivo.
Science 308(5726), 1314–1318 (2005).
45
Remington LT, Babcock AA, Zehntner SP,
Owens T. Microglial recruitment,
activation, and proliferation in response to
primary demyelination. Am. J. Pathol.
170(5), 1713–1724 (2007).
46
Trapp BD, Wujek JR, Criste GA et al.
Evidence for synaptic stripping by cortical
microglia. Glia 55(4), 360–368 (2007).
47
Ransohoff RM, Perry VH. Microglial
physiology: unique stimuli, specialized
responses. Annu. Rev. Immunol. 27,
119–145 (2009).
48
Vogt J, Paul F, Aktas O et al. Lower motor
neuron loss in multiple sclerosis and
experimental autoimmune
encephalomyelitis. Ann. Neurol. 66(3),
310–322 (2009).
49
Hohlfeld R. Biotechnological agents for the
immunotherapy of multiple sclerosis.
Principles, problems and perspectives.
Brain 120(Pt 5), 865–916 (1997).
50
Heppner FL, Greter M, Marino D et al.
Experimental autoimmune
encephalomyelitis repressed by microglial
paralysis. Nat. Med. 11(2), 146–152
(2005).
51
Babbe H, Roers A, Waisman A et al. Clonal
expansions of CD8(
+
) T cells dominate the
T cell infiltrate in active multiple sclerosis
lesions as shown by micromanipulation and
single cell polymerase chain reaction.
J. Exp. Med. 192(3), 393–404 (2000).
52
Jacobsen M, Cepok S, Quak E et al.
Oligoclonal expansion of memory CD8
+
T cells in cerebrospinal fluid from multiple
sclerosis patients. Brain 125(Pt 3), 538–550
(2002).
53
Hu D, Ikizawa K, Lu L, Sanchirico ME,
Shinohara ML, Cantor H. Analysis of
regulatory CD8 T cells in Qa-1-deficient
mice. Nat. Immunol. 5(5), 516–523
(2004).
54
Lu L, Ikizawa K, Hu D, Werneck MB,
Wucherpfennig KW, Cantor H. Regulation
of activated CD4
+
T cells by NK cells via
the Qa-1-NKG2A inhibitory pathway.
Immunity 26(5), 593–604 (2007).
55
Jiang H, Curran S, Ruiz-Vazquez E, Liang
B, Winchester R, Chess L. Regulatory
CD8
+
T cells fine-tune the myelin basic
protein-reactive T cell receptor V
β
repertoire during experimental
autoimmune encephalomyelitis. Proc. Natl
Acad. Sci. USA 100(14), 8378–8383
(2003).
56
Meuth SG, Herrmann AM, Simon OJ
et al. Cytotoxic CD8
+
T cell–neuron
interactions: perforin-dependent electrical
silencing precedes but is not causally linked
to neuronal cell death. J. Neurosci. 29(49),
15397–15409 (2009).
57
Medana IM, Gallimore A, Oxenius A,
Martinic MM, Wekerle H, Neumann H.
MHC class I-restricted killing of neurons
by virus-specific CD8
+
T lymphocytes is
effected through the Fas/FasL, but not the
perforin pathway. Eur. J. Immunol. 30(12),
3623–3633 (2000).
58
Medana I, Martinic MA, Wekerle H,
Neumann H. Transection of major
histocompatibility complex class I-induced
neurites by cytotoxic T lymphocytes.
Am. J. Pathol. 159(3), 809–815 (2001).
59
Linker RA, Sendtner M, Gold R.
Mechanisms of axonal degeneration in
EAE – lessons from CNTF and MHC I
knockout mice. J. Neurol. Sci. 233(1–2),
167–172 (2005).
60
Koh DR, Fung-Leung WP, Ho A, Gray D,
Acha-Orbea H, Mak TW. Less mortality
but more relapses in experimental allergic
encephalomyelitis in CD8
−/−
mice. Science
256(5060), 1210–1213 (1992).
61
Sun D, Qin Y, Chluba J, Epplen JT,
Wekerle H. Suppression of experimentally
induced autoimmune encephalomyelitis by
cytolytic T–T cell interactions. Nature
332(6167), 843–845 (1988).

CME
Expert Rev. Neurother. 12(9), (2012)
1074
Review
Luessi, Siffrin & Zipp
62
Segal BM, Constantinescu CS,
Raychaudhuri A, Kim L, Fidelus-Gort R,
Kasper LH; Ustekinumab MS
Investigators. Repeated subcutaneous
injections of IL12/23 p40 neutralising
antibody, ustekinumab, in patients with
relapsing-remitting multiple sclerosis: a
Phase II, double-blind, placebo-controlled,
randomised, dose-ranging study. Lancet
Neurol. 7(9), 796–804 (2008).
63
Oksenberg JR, Barcellos LF, Cree BA et al.
Mapping multiple sclerosis susceptibility to
the HLA-DR locus in African Americans.
Am. J. Hum. Genet. 74(1), 160–167 (2004).
64
Mangalam A, Luckey D, Basal E et al.
HLA-DQ8 (DQB1*0302)-restricted Th17
cells exacerbate experimental autoimmune
encephalomyelitis in HLA-DR3-transgenic
mice. J. Immunol. 182(8), 5131–5139
(2009).
65
Nitsch R, Pohl EE, Smorodchenko A,
Infante-Duarte C, Aktas O, Zipp F. Direct
impact of T cells on neurons revealed by
two-photon microscopy in living brain
tissue. J. Neurosci. 24(10), 2458–2464
(2004).
66
Aktas O, Smorodchenko A, Brocke S et al.
Neuronal damage in autoimmune
neuroinflammation mediated by the death
ligand TRAIL. Neuron 46(3), 421–432
(2005).
67
Nitsch R, Bechmann I, Deisz RA et al.
Human brain-cell death induced by
tumour-necrosis-factor-related
apoptosis-inducing ligand (TRAIL).
Lancet 356(9232), 827–828 (2000).
68
Siffrin V, Radbruch H, Glumm R et al.
In vivo imaging of partially reversible Th17
cell-induced neuronal dysfunction in the
course of encephalomyelitis. Immunity
33(3), 424–436 (2010).
•
Provides new insights into T-cell-induced
neuronal dysfunction.
69
Arnold DL, Riess GT, Matthews PM et al.
Use of proton magnetic resonance
spectroscopy for monitoring disease
progression in multiple sclerosis.
Ann. Neurol. 36(1), 76–82 (1994).
70
Bostock H, Sears TA. The internodal axon
membrane: electrical excitability and
continuous conduction in segmental
demyelination. J. Physiol. (Lond.) 280,
273–301 (1978).
71
Felts PA, Baker TA, Smith KJ. Conduction
in segmentally demyelinated mammalian
central axons. J. Neurosci. 17(19),
7267–7277 (1997).
72
Dutta R, McDonough J, Yin X et al.
Mitochondrial dysfunction as a cause of
axonal degeneration in multiple sclerosis
patients. Ann. Neurol. 59(3), 478–489
(2006).
73
Su KG, Banker G, Bourdette D, Forte M.
Axonal degeneration in multiple sclerosis:
the mitochondrial hypothesis. Curr. Neurol.
Neurosci. Rep. 9(5), 411–417 (2009).
74
Mahad D, Ziabreva I, Lassmann H,
Turnbull D. Mitochondrial defects in acute
multiple sclerosis lesions. Brain 131(Pt 7),
1722–1735 (2008).
75
Mahad DJ, Ziabreva I, Campbell G et al.
Mitochondrial changes within axons in
multiple sclerosis. Brain 132(Pt 5),
1161–1174 (2009).
76
Lucchinetti C, Brück W, Parisi J,
Scheithauer B, Rodriguez M, Lassmann H.
Heterogeneity of multiple sclerosis lesions:
implications for the pathogenesis of
demyelination. Ann. Neurol. 47(6),
707–717 (2000).
77
Lindquist S, Bodammer N, Kaufmann J
et al. Histopathology and serial,
multimodal magnetic resonance imaging
in a multiple sclerosis variant. Mult. Scler.
13(4), 471–482 (2007).
78
Yang XO, Nurieva R, Martinez GJ et al.
Molecular antagonism and plasticity of
regulatory and inflammatory T-cell
programs. Immunity 29(1), 44–56 (2008).
79
Nikolaeva MA, Mukherjee B, Stys PK.
Na
+
-dependent sources of intra-axonal Ca
2+
release in rat optic nerve during in vitro
chemical ischemia. J. Neurosci. 25(43),
9960–9967 (2005).
80
Stys PK, Waxman SG, Ransom BR. Ionic
mechanisms of anoxic injury in
mammalian CNS white matter: role of Na
+
channels and Na(
+
)-Ca
2+
exchanger.
J. Neurosci. 12(2), 430–439 (1992).
81
Stys PK, Ransom BR, Waxman SG,
Davis PK. Role of extracellular calcium in
anoxic injury of mammalian central white
matter. Proc. Natl Acad. Sci. USA 87(11),
4212–4216 (1990).
82
Stys PK, Jiang Q. Calpain-dependent
neurofilament breakdown in anoxic and
ischemic rat central axons. Neurosci. Lett.
328(2), 150–154 (2002).
83
Nave KA, Trapp BD. Axon–glial signaling
and the glial support of axon function.
Annu. Rev. Neurosci. 31, 535–561 (2008).
84
Trapp BD, Nave KA. Multiple sclerosis:
an immune or neurodegenerative
disorder? Annu. Rev. Neurosci. 31,
247–269 (2008).
85
Wilkins A, Chandran S, Compston A.
A role for oligodendrocyte-derived IGF-1
in trophic support of cortical neurons.
Glia 36, 48–57 (2001).
86
Wilkins A, Majed H, Layfield R et al.
Oligodendrocytes promote neuronal
survival and axonal length by distinct
intracellular mechanisms: a novel role for
oligodendrocyte-derived glial cell
line-derived neurotrophic factor. J. Neuosci.
23, 4967–4974 (2003).
87
Griffiths I, Klugmann M, Anderson T
et al. Axonal swellings and degeneration in
mice lacking the major proteolipid of
myelin. Science 280(5369), 1610–1613
(1998).
88
Aharoni R, Teitelbaum D, Sela M, Arnon
R. Copolymer 1 induces T cells of the
T-helper type 2 that crossreact with myelin
basic protein and suppress experimental
autoimmune encephalomyelitis. Proc. Natl
Acad. Sci. USA 94(20), 10821–10826
(1997).
89
Johnson KP, Brooks BR, Cohen JA et al.
Copolymer 1 reduces relapse rate and
improves disability in relapsing-remitting
multiple sclerosis: results of a Phase III
multicenter, double-blind placebo-
controlled trial. The Copolymer 1 Multiple
Sclerosis Study Group. Neurology 45(7),
1268–1276 (1995).
90
Trojano M, Pellegrini F, Fuiani A et al.
New natural history of interferon-
β-treated
relapsing multiple sclerosis. Ann. Neurol.
61(4), 300–306 (2007).
91
Yong VW. Differential mechanisms of
action of interferon-
β and glatiramer
aetate in MS. Neurology 59(6), 802–808
(2002).
92
Kieseier BC, Hartung HP. Interferon-
β
and neuroprotection in multiple sclerosis
– facts, hopes and phantasies. Exp. Neurol.
203(1), 1–4 (2007).
93
Neuhaus O, Farina C, Yassouridis A et al.
Multiple sclerosis: comparison of
copolymer-1-reactive T cell lines from
treated and untreated subjects reveals
cytokine shift from T helper 1 to
T helper–2 cells. Proc. Natl Acad. Sci. USA
97(13), 7452–7457 (2000).
94
Arnon R, Aharoni R. Mechanism of action
of glatiramer acetate in multiple sclerosis
and its potential for the development of
new applications. Proc. Natl Acad. Sci. USA
101(Suppl. 2), 14593–14598 (2004).
95
Ziemssen T, Kümpfel T, Klinkert WE,
Neuhaus O, Hohlfeld R. Glatiramer
acetate-specific T-helper 1- and 2-type cell
lines produce BDNF: implications for
multiple sclerosis therapy. Brain-derived
neurotrophic factor. Brain 125(Pt 11),
2381–2391 (2002).
Luessi, Siffrin & Zipp

CME
1075
www.expert-reviews.com
Review
Neurodegeneration in multiple sclerosis: novel treatment strategies
96
Filippi M, Rovaris M, Rocca MA,
Sormani MP, Wolinsky JS, Comi G;
European/Canadian Glatiramer Acetate
Study Group. Glatiramer acetate reduces
the proportion of new MS lesions evolving
into ‘black holes’. Neurology 57(4), 731–733
(2001).
97
Khan O, Shen Y, Bao F et al. Long-term
study of brain 1H-MRS study in multiple
sclerosis: effect of glatiramer acetate
therapy on axonal metabolic function and
feasibility of long-term H-MRS monitoring
in multiple sclerosis.
J. Neuroimaging 18(3), 314–319 (2008).
98
Sättler MB, Demmer I, Williams SK et al.
Effects of interferon-
β-1a on neuronal
survival under autoimmune inflammatory
conditions. Exp. Neurol. 201(1), 172–181
(2006).
99
Malik O, Compston DA, Scolding NJ.
Interferon-
β inhibits mitogen induced
astrocyte proliferation in vitro.
J. Neuroimmunol. 86(2), 155–162 (1998).
100
Bagnato F, Gupta S, Richert ND et al.
Effects of interferon-
β-1b on black holes in
multiple sclerosis over a 6-year period with
monthly evaluations. Arch. Neurol. 62(11),
1684–1688 (2005).
101
Filippi M, Rovaris M, Inglese M et al.
Interferon-
β-1a for brain tissue loss in
patients at presentation with syndromes
suggestive of multiple sclerosis: a
randomised, double-blind,
placebo-controlled trial. Lancet
364(9444), 1489–1496 (2004).
102
Rosen H, Goetzl EJ. Sphingosine
1-phosphate and its receptors: an autocrine
and paracrine network. Nat. Rev. Immunol.
5(7), 560–570 (2005).
103
Miron VE, Ludwin SK, Darlington PJ
et al. Fingolimod (FTY720) enhances
remyelination following demyelination of
organotypic cerebellar slices. Am. J. Pathol.
176(6), 2682–2694 (2010).
104
Kappos L, Radue EW, O’Connor P et al.;
FREEDOMS Study Group.
A placebo-controlled trial of oral
fingolimod in relapsing multiple sclerosis.
N. Engl. J. Med. 362(5), 387–401 (2010).
105
Beutler E. Cladribine
(2-chlorodeoxyadenosine). Lancet
340(8825), 952–956 (1992).
106
Claussen MC, Korn T. Immune
mechanisms of new therapeutic strategies
in MS: teriflunomide. Clin. Immunol.
142(1), 49–56 (2012).
107
Giovannoni G, Comi G, Cook S et al.;
CLARITY Study Group. A placebo-
controlled trial of oral cladribine for
relapsing multiple sclerosis. N. Engl.
J. Med. 362(5), 416–426 (2010).
108
Kappos L, Gold R, Miller DH et al.;
BG-12 Phase IIb Study Investigators.
Efficacy and safety of oral fumarate in
patients with relapsing-remitting multiple
sclerosis: a multicentre, randomised,
double-blind, placebo-controlled Phase IIb
study. Lancet 372(9648), 1463–1472
(2008).
109
Nguyen T, Nioi P, Pickett CB. The
Nrf2-antioxidant response element
signaling pathway and its activation by
oxidative stress. J. Biol. Chem. 284(20),
13291–13295 (2009).
110
Comi G, Jeffery D, Kappos L et al.
ALLEGRO Study Group.
Placebo-controlled trial of oral
laquinimod for multiple sclerosis. N. Engl.
J. Med. 366(11), 1000–1009 (2012).
111
Birnberg T, Jung S. Effect of laquinimod
on the dendritic cell compartment.
Neurology 72(Suppl. 3), A36 (2009).
112
Zou LP, Abbas N, Volkmann I et al.
Suppression of experimental autoimmune
neuritis by ABR-215062 is associated with
altered Th1/Th2 balance and inhibited
migration of inflammatory cells into the
peripheral nerve tissue. Neuropharmacology
42(5), 731–739 (2002).
113
Thöne J, Lee D, Seubert S et al.
Laquinimod ameliorates experimental
autoimmune encephalomyelitis via
BDNF-dependent mechanisms.
Mult. Scler. 16 (Suppl. 7), S310 (2010).
114
Moreau T, Coles A, Wing M et al.
CAMPATH-IH in multiple sclerosis.
Mult. Scler. 1(6), 357–365 (1996).
115
Coles AJ, Compston DA, Selmaj KW et al.
CAMMS223 Trial Investigators.
Alemtuzumab versus interferon-
β-1a in
early multiple sclerosis. N. Engl. J. Med.
359(17), 1786–1801 (2008).
116
Coles AJ. Alemtuzumab long-term safety
and efficacy: five years of the
CAMMS223 trial. Mult. Scler. 16,
S134–S135 (2010).
117
Jones JL, Anderson JM, Phuah CL et al.
Improvement in disability after
alemtuzumab treatment of multiple
sclerosis is associated with neuroprotective
autoimmunity. Brain 133(Pt 8),
2232–2247 (2010).
118
Hao J, Campagnolo D, Liu R et al.
Interleukin-2/interleukin-2 antibody
therapy induces target organ natural killer
cells that inhibit central nervous system
inflammation. Ann. Neurol. 69(4),
721–734 (2011).
119
Wynn D, Kaufman M, Montalban X et al.;
CHOICE investigators. Daclizumab in
active relapsing multiple sclerosis
(CHOICE study): a Phase 2, randomised,
double-blind, placebo-controlled, add-on
trial with interferon-
β. Lancet Neurol. 9(4),
381–390 (2010).
120
Black JA, Liu S, Hains BC, Saab CY,
Waxman SG. Long-term protection of
central axons with phenytoin in
monophasic and chronic-relapsing EAE.
Brain 129(Pt 12), 3196–3208 (2006).
121
Black JA, Liu S, Carrithers M, Carrithers
LM, Waxman SG. Exacerbation of
experimental autoimmune
encephalomyelitis after withdrawal of
phenytoin and carbamazepine.
Ann. Neurol. 62(1), 21–33 (2007).
122
Bechtold DA, Kapoor R, Smith KJ. Axonal
protection using flecainide in experimental
autoimmune encephalomyelitis.
Ann. Neurol. 55(5), 607–616 (2004).
123
Kapoor R, Furby J, Hayton T et al.
Lamotrigine for neuroprotection in
secondary progressive multiple sclerosis:
a randomised, double-blind,
placebo-controlled, parallel-group trial.
Lancet Neurol. 9(7), 681–688 (2010).
124
Craner MJ, Damarjian TG, Liu S et al.
Sodium channels contribute to
microglia/macrophage activation and
function in EAE and MS. Glia 49(2),
220–229 (2005).
125
Mi S, Hu B, Hahm K et al. LINGO-1
antagonist promotes spinal cord
remyelination and axonal integrity in
MOG-induced experimental autoimmune
encephalomyelitis. Nat. Med. 13(10),
1228–1233 (2007).
126
Brand-Schieber E, Werner P. Calcium
channel blockers ameliorate disease in a
mouse model of multiple sclerosis.
Exp. Neurol. 189(1), 5–9 (2004).
127
Werner P, Pitt D, Raine CS. Glutamate
excitotoxicity – a mechanism for axonal
damage and oligodendrocyte death in
multiple sclerosis? J. Neural Transm. (60),
375–385 (2000).
128
Waxman SG. Mechanisms of disease:
sodium channels and neuroprotection in
multiple sclerosis – current status. Nat. Clin.
Pract. Neurol. 4(3), 159–169 (2008).
129
Brines ML, Ghezzi P, Keenan S et al.
Erythropoietin crosses the blood–brain
barrier to protect against experimental
brain injury. Proc. Natl Acad. Sci. USA
97(19), 10526–10531 (2000).
130
Buemi M, Cavallaro E, Floccari F et al.
The pleiotropic effects of erythropoietin in

CME
Expert Rev. Neurother. 12(9), (2012)
1076
Review
Luessi, Siffrin & Zipp
the central nervous system. J. Neuropathol.
Exp. Neurol. 62(3), 228–236 (2003).
131
Sättler MB, Merkler D, Maier K et al.
Neuroprotective effects and intracellular
signaling pathways of erythropoietin
in a rat model of multiple sclerosis. Cell
Death Differ. 11(Suppl. 2), S181–S192
(2004).
132
Ehrenreich H, Fischer B, Norra C et al.
Exploring recombinant human
erythropoietin in chronic progressive
multiple sclerosis. Brain 130(Pt 10),
2577–2588 (2007).
133
Clark AJ, Ware MA, Yazer E, Murray TJ,
Lynch ME. Patterns of cannabis use among
patients with multiple sclerosis. Neurology
62(11), 2098–2100 (2004).
134
Pryce G, Baker D. Emerging properties of
cannabinoid medicines in management of
multiple sclerosis. Trends Neurosci. 28(5),
272–276 (2005).
135
Fujiwara M, Egashira N. New perspectives
in the studies on endocannabinoid and
cannabis: abnormal behaviors associate
with CB1 cannabinoid receptor and
development of therapeutic application.
J. Pharmacol. Sci. 96(4), 362–366 (2004).
136
Kreitzer AC, Regehr WG. Cerebellar
depolarization-induced suppression of
inhibition is mediated by endogenous
cannabinoids. J. Neurosci. 21(20), RC174
(2001).
137
Pryce G, Ahmed Z, Hankey DJ et al.
Cannabinoids inhibit neurodegeneration
in models of multiple sclerosis. Brain
126(Pt 10), 2191–2202 (2003).
138
Ligresti A, Cascio MG, Pryce G et al.
New potent and selective inhibitors of
anandamide reuptake with antispastic
activity in a mouse model of multiple
sclerosis. Br. J. Pharmacol. 147(1), 83–91
(2006).
139
Neuhaus O, Stüve O, Zamvil SS, Hartung
HP. Are statins a treatment option for
multiple sclerosis? Lancet Neurol. 3(6),
369–371 (2004).
140
Togha M, Karvigh SA, Nabavi M et al.
Simvastatin treatment in patients with
relapsing-remitting multiple sclerosis
receiving interferon-
β 1a: a double-blind
randomized-controlled trial. Mult. Scler.
16(7), 848–854 (2010).
141
Klopfleisch S, Merkler D, Schmitz M et al.
Negative impact of statins on
oligodendrocytes and myelin formation
in vitro and in vivo. J. Neurosci. 28(50),
13609–13614 (2008).
142
O’Connor PW, Li D, Freedman MS et al.;
Teriflunomide Multiple Sclerosis Trial
Group; University of British Columbia
MS/MRI Research Group. A Phase II
study of the safety and efficacy of
teriflunomide in multiple sclerosis with
relapses. Neurology 66(6), 894–900
(2006).
143
Comi G, Filippi M, Wolinsky JS.
European/Canadian multicenter,
double-blind, randomized,
placebo-controlled study of the effects of
glatiramer acetate on magnetic resonance
imaging – measured disease activity and
burden in patients with relapsing multiple
sclerosis. European/Canadian Glatiramer
Acetate Study Group. Ann. Neurol. 49(3),
290–297 (2001).
144
Jacobs L, Rudick R, Simon J. Extended
observations on MS patients treated with
IM interferon-
β-1a (Avonex): implications
for modern MS trials and therapeutics.
J. Neuroimmunol. 107(2), 167–173 (2000).
145
Kappos L, Freedman MS, Polman CH
et al.; BENEFIT Study Group. Effect of
early versus delayed interferon-
β-1b
treatment on disability after a first clinical
event suggestive of multiple sclerosis:
a 3-year follow-up analysis of the
BENEFIT study. Lancet 370(9585),
389–397 (2007).
146
Jacobs LD, Cookfair DL, Rudick RA et al.
Intramuscular interferon-
β-1a for disease
progression in relapsing multiple sclerosis.
The Multiple Sclerosis Collaborative
Research Group (MSCRG). Ann. Neurol.
39(3), 285–294 (1996).
147
Hartung HP, Gonsette R, König N et al.;
Mitoxantrone in Multiple Sclerosis Study
Group (MIMS). Mitoxantrone in
progressive multiple sclerosis: a placebo-
controlled, double-blind, randomised,
multicentre trial. Lancet 360(9350),
2018–2025 (2002).
148
Edan F, Comi G, Le Page E et al.
Mitoxantrone prior to interferon
β-1b in
aggressive relapsing multiple sclerosis:
a 3-year randomised trial. J. Neurol.
Neurosurg. Psychiatr. 2018–2025 (2002).
149
Polman CH, O’Connor PW, Havrdova E
et al.; AFFIRM Investigators.
A randomized, placebo-controlled trial of
natalizumab for relapsing multiple
sclerosis. N. Engl. J. Med. 354(9), 899–910
(2006).
150
Luessi F, Zipp F. Neuro aktuell 7/2011,
Westermayer Verlag GmbH, p. 28.
151
Hauser SL, Waubant E, Arnold DL et al.;
HERMES Trial Group. B-cell depletion
with rituximab in relapsing-remitting
multiple sclerosis. N. Engl. J. Med. 358(7),
676–688 (2008).
152
Friese MA, Craner MJ, Etzensperger R
et al. Acid-sensing ion channel-1
contributes to axonal degeneration in
autoimmune inflammation of the central
nervous system. Nat. Med. 13(12),
1483–1489 (2007).
153
Vergo S, Craner MJ, Etzensperger R et al.
Acid-sensing ion channel-1 is involved in
both axonal injury and demyelination in
multiple sclerosis and its animal model.
Brain 134(Pt 2), 571–584 (2011).
154
Zajicek J, Fox P, Sanders H et al.; UK MS
Research Group. Cannabinoids for
treatment of spasticity and other symptoms
related to multiple sclerosis (CAMS study):
multicentre randomised placebo-controlled
trial. Lancet 362(9395), 1517–1526
(2003).
155
Maresz K, Pryce G, Ponomarev ED et al.
Direct suppression of CNS autoimmune
inflammation via the cannabinoid receptor
CB1 on neurons and CB2 on autoreactive
T cells. Nat. Med. 13(4), 492–497 (2007).
156
Aktas O, Prozorovski T, Smorodchenko A
et al. Green tea epigallocatechin-3-gallate
mediates T cellular NF-kappa B inhibition
and exerts neuroprotection in autoimmune
encephalomyelitis. J. Immunol. 173(9),
5794–5800 (2004).
157
Schroeder EK, Kelsey NA, Doyle J et al.
Green tea epigallocatechin 3-gallate
accumulates in mitochondria and displays a
selective antiapoptotic effect against
inducers of mitochondrial oxidative stress
in neurons. Antioxid. Redox Signal. 11(3),
469–480 (2009).
158
Dörr J, Roth K, Zurbuchen U et al.
Tumor-necrosis-factor-related apoptosis-
inducing-ligand (TRAIL)-mediated death
of neurons in living human brain tissue is
inhibited by flupirtine–maleate.
J. Neuroimmunol. 167(1–2), 204–209
(2005).
159
Sättler MB, Williams SK, Neusch C et al.
Flupirtine as neuroprotective
add-on therapy in autoimmune optic
neuritis. Am. J. Pathol. 173(5),
1496–1507 (2008).
160
Kalkers NF, Barkhof F, Bergers E,
van Schijndel R, Polman CH. The effect of
the neuroprotective agent riluzole on MRI
parameters in primary progressive multiple
sclerosis: a pilot study. Mult. Scler. 8(6),
532–533 (2002).
161
Angehagen M, Ben-Menachem E,
Rönnbäck L, Hansson E. Topiramate
protects against glutamate- and
kainate-induced neurotoxicity in primary
neuronal-astroglial cultures. Epilepsy Res.
54(1), 63–71 (2003).
Luessi, Siffrin & Zipp
CME
1077
www.expert-reviews.com
Review
Neurodegeneration in multiple sclerosis: novel treatment strategies
Neurodegeneration in multiple sclerosis: novel treatment strategies
To obtain credit, you should first read the journal article. After
reading the article, you should be able to answer the following,
related, multiple-choice questions. To complete the questions
(with a minimum 70% passing score) and earn continuing medi-
cal education (CME) credit, please go to www.medscape.org/
journal/expertneurothera. Credit cannot be obtained for tests
completed on paper, although you may use the worksheet below
to keep a record of your answers. You must be a registered user on
Medscape.org. If you are not registered on Medscape.org, please
click on the New Users: Free Registration link on the left hand
side of the website to register. Only one answer is correct for each
question. Once you successfully answer all post-test questions
you will be able to view and/or print your certificate. For ques-
tions regarding the content of this activity, contact the accredited
provider, CME@medscape.net. For technical assistance, contact
CME@webmd.net. American Medical Association’s Physician’s
Recognition Award (AMA PRA) credits are accepted in the
US as evidence of participation in CME activities. For further
information on this award, please refer to http://www.ama-assn.
org/ama/pub/category/2922.html. The AMA has determined
that physicians not licensed in the US who participate in this
CME activity are eligible for AMA PRA Category 1 Credits™.
Through agreements that the AMA has made with agencies in
some countries, AMA PRA credit may be acceptable as evidence
of participation in CME activities. If you are not licensed in the
US, please complete the questions online, print the AMA PRA
CME credit certificate and present it to your national medical
association for review.
Activity Evaluation
Where 1 is strongly disagree and 5 is strongly agree
1 2 3 4 5
1. The activity supported the learning objectives.
2. The material was organized clearly for
learning to occur.
3. The content learned from this activity will
impact my practice.
4. The activity was presented objectively and
free of commercial bias.
1. Your patient is a 34-year-old woman recently diagnosed with relapsing-remitting multiple sclerosis (MS). Based on
the review by Dr. Luessi and colleagues, which of the following statements about the role of inflammatory
neuronal injury in this patient’s disease is most likely correct?
£
A
At this stage, the pathophysiology is exclusively inflammatory demyelination
£
B
Neuronal damage does not occur in the absence of demyelination
£
C
Axonal pathology is particularly evident in active and chronic active MS lesions throughout the disease course and is
closely associated with inflammatory infiltration
£
D
CD8
+
T cells within multiple sclerosis lesions activate pathogenic autoreactive CD4
+
T cells
2. Based on the review by Dr. Luessi and colleagues, which of the following statements about methods of
quantification of neuronal injury for the patient described in question 1 is most likely correct?
£
A
Monitoring contrast-enhancing lesions (CEL) on routine MRI is sufficient
£
B
T2 lesion load on MRI is an excellent predictor of later disability progression
£
C
Change in brain volume on MRI is not helpful, but evolution of persistent hyperintense lesions on T2-weighted scans
may be helpful
£
D
Magnetic resonance spectroscopy and retinal nerve fiber layer thickness on optical coherence tomography are useful
techniques
3. Based on the review by Dr. Luessi and colleagues, which of the following statements about therapeutic
approaches to neuronal degeneration in multiple sclerosis would most likely be correct?
£
A
Many currently approved agents for multiple sclerosis do not primarily target inflammation
£
B
To prevent chronic disability, an optimized therapeutic approach should target inflammation alone
£
C
Glatiramer acetate (GA) and interferon-
β (IFN-β) are first-line disease-modifying immune-modulatory treatments that
reduce relapses and slow the progression of disability
£
D
Fingolimod (FTY720) has no neuroprotective properties
Wyszukiwarka
Podobne podstrony:
Study of the temperature?pendence of the?initic transformation rate in a multiphase TRIP assi
The Role of Vitamin A in Prevention and Corrective Treatments
Dracula s Women The Representation of Female Characters in a Nineteenth Century Novel and a Twentie
Mettern S P Rome and the Enemy Imperial Strategy in the Principate
Functional Origins of Religious Concepts Ontological and Strategic Selection in Evolved Minds
Multiple Intelligences in the Elementary Classroom
Logistyka Strategia J in T
antinoceptive activity of the novel fentanyl analogue iso carfentanil in rats jpn j pharmacol 84 188
Session 7 in Strategic Management
Kopelmann, Rosette Cultural variation in response to strategic emotions
Advanced Diploma in Business Management Strategic Human Resource Management
Illiad, The Role of Greek Gods in the Novel
Great Expectations Powerful Themes in the Novel
KULT ADAPTACJI STRATEGIA IN, Zarządzanie projektami, Zarządzanie(1)
Flashback to the 1960s LSD in the treatment of autism
New Developments in HBV Treatment
więcej podobnych podstron