Contents
lists
available
at
Resuscitation
j o
u
r n
a l
h o m
e p a g e
:
w w w . e l s e v i e r . c o m / l o c a t e / r e s u s c i t a t i o n
Clinical
Paper
Impact
of
resuscitation
system
errors
on
survival
from
in-hospital
cardiac
arrest
夽
Joseph
P.
Ornato
, Mary
Ann
Peberdy
,
Renee
D.
Reid
,
V.
Ramana
Feeser
,
Harinder
S.
Dhindsa
,
for
the
NRCPR
Investigators
a
Department
of
Emergency
Medicine,
Virginia
Commonwealth
University,
Richmond,
VA,
United
States
b
Department
of
Internal
Medicine
&
Emergency
Medicine,
Virginia
Commonwealth
University,
Richmond,
VA,
United
States
a
r
t
i
c
l
e
i
n
f
o
Article
history:
Received
14
May
2011
Received
in
revised
form
9
September
2011
Accepted
11
September
2011
Keywords:
Inhospital
Resuscitation
Quality
Outcomes
Errors
a
b
s
t
r
a
c
t
Background:
An
estimated
350,000–750,000
adult,
in-hospital
cardiac
arrest
(IHCA)
events
occur
annually
in
the
United
States.
The
impact
of
resuscitation
system
errors
on
survival
during
IHCA
resuscitation
has
not
been
evaluated.
The
purpose
of
this
paper
was
to
evaluate
the
impact
of
resuscitation
system
errors
on
survival
to
hospital
discharge
after
IHCA.
Methods
and
results:
We
evaluated
subjective
and
objective
errors
in
118,387
consecutive,
adult,
index
IHCA
cases
entered
into
the
Get
with
the
Guidelines
National
Registry
of
Cardiopulmonary
Resuscitation
database
from
January
1,
2000
through
August
26,
2008.
Cox
regression
analysis
was
used
to
determine
the
relationship
between
reported
resuscitation
system
errors
and
other
important
clinical
variables
and
the
hazard
ratio
for
death
prior
to
hospital
discharge.
Of
the
108,636
patients
whose
initial
IHCA
rhythm
was
recorded,
resuscitation
system
errors
were
committed
in
9,894/24,467
(40.4%)
of
those
with
an
ini-
tial
rhythm
of
ventricular
fibrillation
or
pulseless
ventricular
tachycardia
(VF/pVT)
and
in
22,599/84,169
(26.8%)
of
those
with
non-VF/pVT.
The
most
frequent
system
errors
related
to
delay
in
medication
admin-
istration
(>5
min
time
from
event
recognition
to
first
dose
of
a
vasoconstrictor),
defibrillation,
airway
management,
and
chest
compression
performance
errors.
The
presence
of
documented
resuscitation
system
errors
on
an
IHCA
event
was
associated
with
decreased
rates
of
return
of
spontaneous
circu-
lation,
survival
to
24
h,
and
survival
to
hospital
discharge.
The
relative
risk
of
death
prior
to
hospital
discharge
based
on
hazard
ratio
analysis
was
9.9%
(95%
CI
7.8,
12.0)
more
likely
for
patients
whose
ini-
tial
documented
rhythm
was
non-VF/pVT
when
resuscitation
system
errors
were
reported
compared
to
when
no
errors
were
reported.
It
was
34.2%
(95%
CI
29.5,
39.1)
more
likely
for
those
with
VF/pVT.
Conclusions:
The
presence
of
resuscitation
system
errors
that
are
evident
from
review
of
the
resuscitation
record
is
associated
with
decreased
survival
from
IHCA
in
adults.
Hospitals
should
target
the
training
of
first
responders
and
code
team
personnel
to
emphasize
the
importance
of
early
defibrillation,
early
use
of
vasoconstrictor
medication,
and
compliance
with
ACLS
protocols.
© 2011 Elsevier Ireland Ltd. All rights reserved.
1.
Introduction
The
Institutes
of
Medicine
(IOM)
landmark
publication
(“To
Err
is
Human”)
estimated
that
at
least
44,000
and
perhaps
as
many
as
98,000
Americans
die
in
hospitals
each
year
as
a
result
of
med-
ical
the
magnitude
of
the
problem
has
been
夽 A
Spanish
translated
version
of
the
abstract
of
this
article
appears
as
Appendix
in
the
final
online
version
at
doi:10.1016/j.resuscitation.2011.09.009
.
∗ Corresponding
author
at:
Department
of
Emergency
Medicine,
Virginia
Com-
monwealth
University,
1250
East
Marshall
Street
–
Main
Hospital
2nd
Floor,
Suite
500,
Richmond,
VA
23298-0401,
United
States.
Tel.:
+1
804
828
5250;
fax:
+1
804
828
8590.
address:
(J.P.
Ornato).
c
For
the
American
Heart
Association’s
Get
With
the
Guidelines
–
Resuscitation
(National
Registry
of
Cardiopulmonary
Resuscitation)
Investigators,
see
questioned,
Canadian
Adverse
Events
(AE)
Study
confirms
an
alarming
frequency
of
in-hospital
AEs
(7.5
per
100
hospital
admissions;
95%
confidence
interval
[CI],
5.7–9.3),
36.9%
(95%
CI,
32.0–41.8%)
of
which
are
potentially
preventable.
Death
occurred
in
20.8%
(95%
CI,
7.8–33.8%)
of
cases.
The
American
Heart
Association
(AHA)
Get
with
the
Guidelines
National
Registry
of
Cardiopulmonary
Resuscitation
(NRCPR)
col-
lects
data
on
adult
and
pediatric
in-hospital
cardiac
arrest
(IHCA)
events
from
approximately
10%
of
hospitals
in
the
United
From
this
registry,
NRCPR
investigators
have
documented
lower
survival
from
adult
in-hospital
cardiac
arrest
(1)
on
nights
and
weekends
likely
due,
at
least
in
part,
to
system
when
defibrillation
is
delayed
greater
than
2
min
in
patients
whose
ini-
tial
IHCA
rhythm
is
ventricular
fibrillation
or
pulseless
ventricular
tachycardia
(3)
in
certain
hospital
locations.
The
purpose
of
this
paper
was
to
determine
whether
the
presence
of
resuscitation
system
errors
reported
to
NRCPR
are
0300-9572/$
–
see
front
matter ©
2011 Elsevier Ireland Ltd. All rights reserved.
doi:

64
J.P.
Ornato
et
al.
/
Resuscitation
83 (2012) 63–
69
associated
with
lower
likelihood
of
survival
in
adult
patients
who
experience
an
IHCA.
2.
Methods
2.1.
Data
collection
and
integrity
NRCPR
is
a
prospective,
observational,
multi-center
perfor-
mance
improvement
registry
of
IHCA
events.
Hospitals
join
voluntarily
and
pay
an
annual
fee
for
data
support
and
report
gen-
eration.
Hospital
medical
records
on
sequential
IHCA
events
are
abstracted
by
trained,
NRCPR-certified,
performance
improvement
personnel
at
each
participating
institution.
All
data
elements
have
standardized
definitions
allowing
aggregate
data
analysis
from
multiple
sites,
and
all
data
transfer
is
in
compliance
with
the
Health
Insurance
Portability
and
Accountability
Act.
Oversight
for
opera-
tions
is
provided
by
the
American
Heart
Association,
a
scientific
advisory
board,
and
an
executive
database
steering
committee.
Multiple
efforts
are
taken
to
assure
data
integrity,
including
data
abstractor
certification
prior
to
allowing
data
entry,
over
300
soft-
ware
checks
and
smart
skips
to
assist
with
accurate
data
entry,
and
ongoing
abstractor
training
with
monthly
user’s
group
calls
and
an
annual
user’s
group
conference.
Even
though
the
most
challeng-
ing
data
points
to
collect
during
resuscitation
are
event
times
and
intervals,
these
are
documented
in
a
high
percentage
of
cases
in
NRCPR
hospitals.
For
example,
in
this
analysis
the
time
intervals
from
IHCA
onset
to
start
of
CPR
and
first
vasopressor
administra-
tion
were
captured
in
89%
and
76%,
respectively.
Further
details
of
the
NRCPR
database
and
data
integrity
can
be
found
in
previous
2.2.
Study
outcomes
The
primary
study
outcome
was
survival
to
hospital
discharge.
Secondary
outcomes
were
return
of
spontaneous
circulation
(ROSC)
and
survival
for
24
h
after
IHCA.
2.3.
Inclusion/exclusion
criteria
The
current
analysis
includes
all
consecutive,
adult
(age
≥18
years),
initial,
pulseless
IHCA
events
entered
from
549
dif-
ferent
hospitals
from
January
1,
2000
through
August
26,
2008.
All
adults
(
≥18
years
of
age)
who
experienced
an
in-hospital
resuscitation
event
and
who
had
documentation
of
initial
heart
rhythm
were
eligible
for
inclusion.
An
event
is
defined
as:
(1)
cardiopulmonary
arrest
requiring
chest
compressions
and/or
defib-
rillation,
or
(2)
acute
respiratory
compromise
requiring
emergency
assisted
ventilation
leading
to
cardiopulmonary
arrest
requiring
chest
compressions
and/or
defibrillation.
All
events
must
also
elicit
a
resuscitation
response
by
facility
personnel
and
have
a
resusci-
tation
record
completed.
Events
are
excluded
if
the
arrest
begins
outside
of
the
hospital,
is
limited
to
a
shock
delivered
by
an
implanted
cardioverter-defibrillator
(ICD),
or
occurs
on
a
patient
with
a
pre-existing
do
not
attempt
resuscitation
order.
For
patients
having
multiple
IHCA
events
during
the
same
hospitalization,
only
the
first
event
was
analyzed.
2.4.
Categorization
and
counting
of
resuscitation
system
error
types
The
NRCPR
database
contains
a
section
for
the
data
abstractor
at
each
hospital
site
to
capture
“self-reported”
system
errors
that
were
noted
during
or
following
the
resuscitation
effort
on
the
code
record
and/or
hospital
chart
or
to
document
errors
reported
by
resuscitation
members.
Types
of
error
categories
included
alert-
ing
hospital-wide
resuscitation
response,
airway
management,
vascular
access,
chest
compression,
defibrillation,
medications,
leadership,
protocol
deviation,
and
equipment
function
issues,
with
specific
subcategories
listed
in
type
of
individual
error
had
a
checkbox
that
was
to
be
filled
in
by
the
data
abstractor
if
supported
by
the
code
record
and/or
hospital
chart
documenta-
tion,
or
conveyed
by
personnel
on
scene.
For
analysis
of
this
data,
one
point
was
assigned
for
each
individual
error
box
checked
on
a
given
IHCA
event.
We
totaled
the
number
of
cases
with
individual
system
errors
and
created
subtotals
for
the
various
types
of
errors
to
calculate
the
number
of
cases
in
which
any
error
occurred
and
to
catalogue
and
quantify
the
specific
types
of
errors
that
occurred.
We
counted
and
added
one
point
on
each
case
for
each
NRCPR
“process
of
care
exception”
error
defined
as:
(1)
delay
of
>5
min
from
IHCA
event
recognition
to
the
first
dose
of
a
vasoconstric-
tor
(epinephrine
or
vasopressin)
on
events
that
had
a
duration
of
>5
min;
or
(2)
delay
of
>2
min
from
IHCA
event
recognition
to
the
first
defibrillation
shock
in
patients
whose
initial
documented
IHCA
rhythm
was
VF/pVT.
“Resuscitation
system
errors”
were
defined
as
the
total
number
of
reported
system
errors
plus
the
number
of
“process
of
care
exceptions”
in
each
case.
When
the
process
of
care
exception
matched
a
self
reported
error
(e.g.,
delay
in
time
to
first
shock,
time
to
first
vasoconstrictor
administration),
only
one
point
was
assigned
for
the
error
to
avoid
double
counting.
2.5.
Statistical
analysis
All
data
analyses
were
performed
using
PASW
Statistics
ver-
sion
17.0.2
(SPSS,
Inc.,
Chicago,
IL).
Chi
square
and
95%
confidence
intervals
were
used
for
comparison
of
descriptive
variables.
ANOVA
using
Scheffe’s
test
for
multiple
comparisons
was
used
to
analyze
the
relationship
between
0,
1,
2,
3
or
more
errors
and
outcome
variables.
Cox
regression
analysis
was
used
to
determine
the
rela-
tionship
between
reported
resuscitation
system
errors
as
well
as
other
important
clinical
variables
and
the
hazard
ratio
for
death
prior
to
hospital
discharge.
The
status
of
the
primary
outcome
(i.e.,
life
or
death)
was
ascertained
at
three
time
points
follow-
ing
resuscitation:
(1)
whether
ROSC
occurred;
(2)
24
h
following
the
IHCA
event;
and
(3)
at
hospital
discharge.
Cox
regression
anal-
ysis
was
also
used
to
determine
the
hazard
ratio
for
the
time
of
day
(day/evening
or
7a–11p
vs.
night
or
11p–7a)
and
day
of
week
(weekday
or
M–F,
weekend
or
S–Su)
on
the
reporting
of
resuscita-
tion
system
errors
during
a
IHCA
event.
3.
Results
A
total
of
118,387
in-hospital,
adult,
index
IHCA
cases
were
entered
into
the
NRCPR
database
from
January
1,
2000
through
August
26,
2008.
Of
these,
84,440
(71.3%)
had
no
system
errors
recorded
and
33,947
(28.7%)
had
one
or
more
system
errors
recorded.
Of
the
cases
with
system
errors,
26,919
(22.7%)
had
1
error,
5614
(4.7%)
had
2
system
errors,
and
1414
(1.2%)
had
3
or
more
system
errors.
Of
all
cases
in
which
the
initial
rhythm
was
recorded,
84,169/108,636
(77.5%)
had
non
VF/pVT
and
24,467/108,636
(22.5%)
had
VF/pVT.
Errors
were
committed
in
22,599/84,169
(26.8%)
of
non
VF/pVT,
and
in
9894/24,467
(40.4%)
of
those
with
VF/pVT
as
the
first
documented
rhythm.
The
distribution
of
system
errors
for
all
IHCA
patients
by
cate-
gory
is
noted
in
The
most
frequent
system
errors
related
to
delay
in
medication
administration
(>5
min
time
from
event
recognition
to
first
dose
of
a
vasoconstrictor),
defibrillation,
air-
way
management,
and
chest
compression
performance
errors.
The
5.4%
of
cases
having
a
delay
in
defibrillation
of
>2
min
repre-
sents
the
percentage
of
patients
with
defibrillation
delays
using
all

J.P.
Ornato
et
al.
/
Resuscitation
83 (2012) 63–
69
65
Table
1
Distribution
of
resuscitation
system
errors.
Error
category
N
%
of
cases
%
of
reported
resuscitation
system
errors
Alerting
Delay
in
alerting
code
team
232
0.2
1.1
Pager
issue
66
0.1
Other
266
0.2
Airway
Aspiration
related
to
provision
of
airway
225
0.2
17.0
Airway
insertion
delay
2672
2.3
Delayed
recognition
of
airway
misplacement
328
0.3
Intubation
attempted,
not
achieved
319
0.3
Multiple
intubation
attempts
3314
2.8
Other
1939
1.6
Vascular
access
Delay
in
obtaining
access
846
0.7
3.4
Inadvertent
arterial
cannulation
37
<0.1
Infiltration
or
inadvertent
disconnection
of
IV
line
415
0.4
Other
480
0.4
Chest
compression
Compression
rate
of
∼100/min
not
maintained
2530
2.1
7.2
Interruption
of
compressions
>10
s
at
any
time
177
0.1
Delay
in
starting
chest
compressions
155
0.1
No
board
used
beneath
patient
during
compressions
758
0.6
Other
120
0.1
Defibrillation
Defibrillation
delay
>2
min
from
event
recognition
in
patients
with
an
initial
CA
rhythm
of
VF/pVT
due
to
insufficient
trained
personnel
or
defibrillator
not
immediately
available
6364
5.4
19.0
Energy
level
too
high/low
based
on
AHA
guidelines
485
0.4
Incorrect
defibrillator
paddle/pad
placement
32
<0.1
Defibrillator
malfunction
131
0.1
Shock
given,
not
indicated
957
0.8
Shock
indicated,
not
given
607
0.5
Other
1068
0.9
Medications
First
vasopressor
(epinephrine
or
vasopressin)
delay
>5
min
from
event
recognition
in
cases
with
event
duration
>5
min
20,035
16.9
42.5
Wrong
route
of
administration
202
0.2
Wrong
dosage
575
0.5
Wrong
medication
selection
1190
1.0
Code
team
leadership
Delay
in
identifying
team
leader
276
0.2
2.8
Knowledge
of
equipment
107
0.1
Knowledge
of
medications/protocols
539
0.5
Knowledge
of
team
member
roles
223
0.2
Code
team
oversight
196
0.2
Too
many
individuals
present
in
room
105
0.1
Protocol
deviation
from
AHA
Guidelines
Deviation
from
AHA
ACLS
guideline
recommendations
1521
1.3
3.1
Other
84
0.1
Equipment
issues
Availability
1100
0.9
3.9
Malfunction
540
0.5
Other
387
0.3
patients
as
the
denominator
including
those
without
initial
shock-
able
rhythms.
There
were
6364
patients
with
defibrillation
delays
of
>2
min
out
of
20,125
patients
with
an
initial
shock-able
rhythm
documented,
yielding
a
delay
in
defibrillation
in
31.6%
of
patients
in
whom
defibrillation
was
indicated.
the
demographic
characteristics
of
IHCA
events
with
and
without
reported
resuscitation
system
errors.
Cases
in
which
system
errors
were
documented
were
more
likely
to
be
male,
not
witnessed/monitored
at
the
time
of
arrest,
during
the
night
(11p–7a),
on
weekends
(S–Su),
initially
in
VF/pVT,
medical
(vs.
sur-
gical
or
cardiac)
type
admissions,
or
non-ICU
patients
(vs.
ICU,
ED,
or
OR/PACU
patients)
than
cases
in
which
no
system
errors
were
documented.
Resuscitation
system
errors
occurred
in
the
highest
percentage
of
IHCA
events
in
non-ICU
inpatient
areas
(9838/24,378,
40.4%);
they
were
least
frequently
noted
on
IHCA
events
occurring
in
ICU/stepdown
units
(17,692/69,643,
25.8%),
EDs
(3491/12,830,
27.2%),
or
Operating
Room/Post-Anesthesia
Care
Units
(685/2913,
23.5%)
(p
=
.0001).
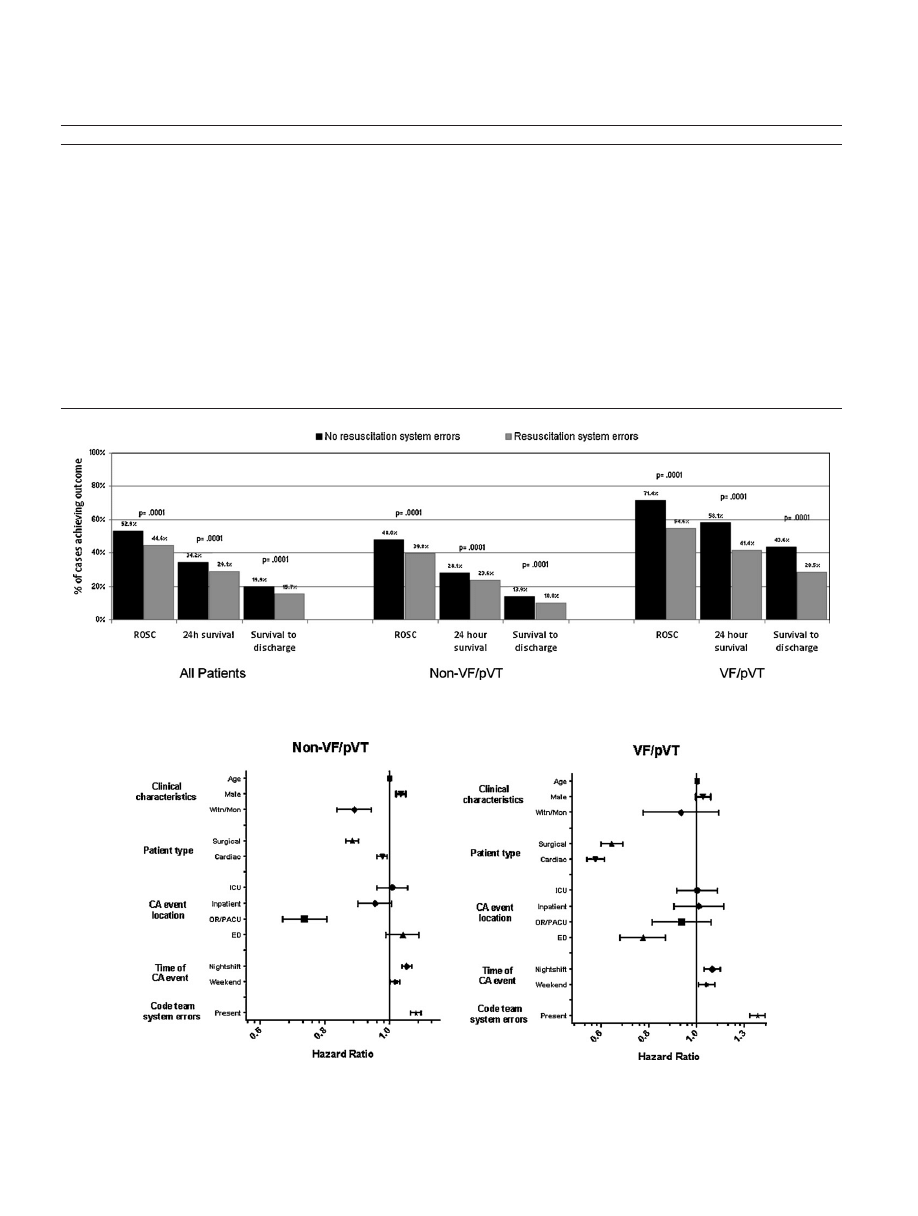
The
presence
of
documented
resuscitation
system
errors
on
an
IHCA
event
was
associated
with
decreased
rates
of
ROSC,
survival
to
24
h,
and
survival
to
hospital
discharge
(
all
patients
as
a
group
and
in
those
whose
initial
documented
IHCA
rhythm
was
separated
into
VF/pVT
or
non-VF/pVT
categories.
Characteristics
that
increased
the
likelihood
of
death
prior
to
hospital
discharge
in
patients
whose
initial
rhythm
was
non-VF/pVT
included:
male
gender,
when
the
event
occurred
at
night
or
on
a
weekend,
or
when
there
were
documented
resuscitation
system
errors
(
There
was
a
lower
likelihood
of
death
prior
to
hospital
discharge
if
the
event
was
witnessed
or
monitored,
if
the
type
of
patient
was
car-
diac
or
surgical
(as
opposed
to
general
medical),
and
if
the
patient
location
was
OR/PACU.
66
J.P.
Ornato
et
al.
/
Resuscitation
83 (2012) 63–
69
Table
2
Demographic
characteristics
of
in-hospital
CA
events
with
and
without
resuscitation
system
errors.
No
resuscitation
system
errors
Resuscitation
system
errors
p
N
(total
=
118,387)
84,440
(71.3%)
33,947
(28.7%)
–
Age
[mean,
95%
CI]
66.07
[65.96,
66.18]
66.36
[66.20,
66.53]
.008
Male
48,428/84,440
(57.4%)
19,951/33,947
(58.8%)
.0001
Witnessed
or
monitored
arrest
69,361/70,152
(98.9%)
25,729/26,636
(96.6%)
.0001
Initial
documented
CA
rhythm
VF/pVT
14,573/76,143
(19.1%)
9894/32,493
(30.4%)
.0001
Patient
type
Cardiac
29,329/81,750
(35.9%)
11,487/33,757
(34.0%)
.0001
Medical
34,777/81,750
(42.5%)
15,483/33,757
(45.9%)
Surgical
17,644/81,750
(21.6%)
6787/33,757
(20.1%)
CA
event
location
ICU
or
stepdown/telemetry
area
50,951/77,057
(66.1%)
17,692/31,707
(55.8%)
.0001
Non-ICU
inpatient
area
14,539/77,057
(18.9%)
9838/31,707
(31.0%)
Emergency
department
9339/77,057
(12.1%)
3491/31,707
(11.0%)
Operating
room
or
PACU
2228/77,057
(2.9%)
685/31,707
(2.2%)
Time
of
day
Day-evening
(7a–11p)
54,888/80,480
(68.2%)
22,387/33,777
(66.3%)
.0001
Night
(11p–7a)
25,592/80,480
(31.8%)
11,390/33,777
(33.7%)
Day
of
week
Weekday
(M–F)
56,783/81,970
(69.3%)
23,236/10.711
(68.4%)
.003
Weekend
(S–Su)
25,187/81,970
(30.7%)
10,711/33,947
(31.6%)
Fig.
1.
Effect
of
any
resuscitation
system
errors
on
an
IHCA
event
and
the
rate
of
ROSC,
survival
for
24
h,
and
survival
to
hospital
discharge
for
all
patients
and
those
with
an
initial
documented
IHCA
rhythm
of
non-VF/pVT
and
VF/pVT.
Fig.
2.
Association
between
the
number
of
resuscitation
system
errors
during
an
IHCA
event
and
a
significantly
increased
hazard
ratio
for
death
prior
to
hospital
discharge
stratified
by
patients
with
an
initial
IHCA
rhythm
of
non-VF/pVT
or
VF/pVT.

J.P.
Ornato
et
al.
/
Resuscitation
83 (2012) 63–
69
67
Characteristics
that
increased
the
likelihood
of
death
prior
to
hospital
discharge
in
patients
whose
initial
rhythm
was
VF/pVT
included:
when
the
event
occurred
at
night
or
on
a
weekend,
or
when
there
were
documented
resuscitation
system
errors
(
There
was
a
lower
likelihood
of
death
prior
to
hospital
discharge
if
the
type
of
patient
was
cardiac
or
surgical
(as
opposed
to
gen-
eral
medical)
or
if
the
patient
location
was
ED.
The
relative
risk
of
death
prior
to
hospital
discharge
based
on
hazard
ratio
analysis
was
9.9%
(95%
CI
7.8,
12.0)
more
likely
for
patients
whose
initial
docu-
mented
rhythm
was
non-VF/pVT
when
resuscitation
system
errors
were
reported
compared
to
when
no
errors
were
reported.
It
was
34.2%
(95%
CI
29.5,
39.1)
more
likely
for
those
with
VF/pVT.
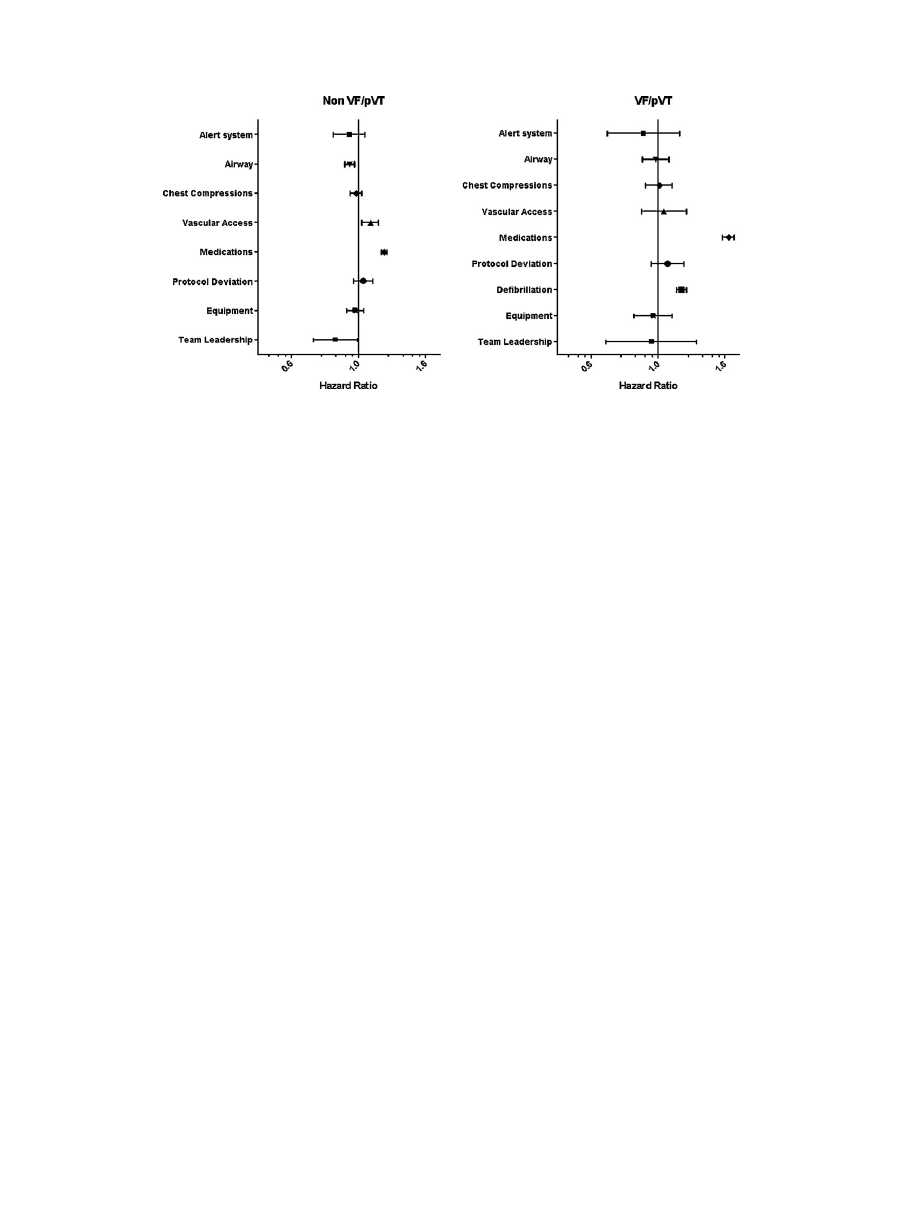
Only
certain
types
of
resuscitation
system
errors
were
asso-
ciated
with
an
increased
hazard
ratio
for
death
prior
to
hospital
discharge.
For
patients
whose
initial
rhythm
was
non-VF/pVT,
delays
in
obtaining
vascular
access
(i.e.,
an
intravenous
line)
and
medication
errors
increased
the
hazard
ratio
for
death
prior
to
hospital
discharge
For
patients
whose
initial
rhythm
was
VF/pVT,
defibrillation
problems
and
medication
errors
increased
the
hazard
ratio
for
death
prior
to
hospital
discharge.
4.
Discussion
The
principal
finding
in
this
study
is
that
the
presence
of
resus-
citation
system
errors
is
associated
with
decreased
survival
from
IHCA
in
adults.
More
errors
were
noted
in
patients
whose
initial
documented
IHCA
rhythm
was
VF/pVT
as
opposed
to
those
with
non-shock-able
rhythms.
This
finding
is
particularly
relevant
clin-
ically,
given
that
the
majority
of
survivors
of
IHCA
are
those
with
initial
VF/pVT.
Our
findings,
although
much
broader,
support
those
reported
by
Chan
et
evaluated
6789
sequential
patients
with
VF
as
the
first
documented
rhythm
in
the
NRCPR
database
and
found
that
30.1%
of
this
cohort
underwent
defibrillation
more
than
2
min
after
initial
recognition
of
their
IHCA.
Patients
with
delayed
defib-
rillation
had
a
significantly
lower
likelihood
of
ROSC
(adjusted
odds
ratio,
0.55;
95%
CI,
0.49–0.62;
p
<
0.001)
and
survival
at
24
h
after
the
cardiac
arrest
(adjusted
odds
ratio,
0.52;
95%
CI,
0.46–0.58;
p
<
0.001).
The
Chan
study
was
the
first
large
scale
analysis
of
data
in
IHCA
patients
identifying
a
specific
defibrillation
delay
time
cut-
off
(2
min
or
less
after
event
recognition)
that
negatively
impacts
survival.
Our
analysis,
in
a
larger
sample
size
from
the
same
reg-
istry,
confirms
that
defibrillation
system
errors,
including
a
>2
min
delay
from
IHCA
recognition
to
initial
defibrillation
accounts
for
higher
mortality
in
the
initial
VF/pVT
group,
but
it
also
found
an
association
between
medication
errors
and
a
lower
likelihood
of
survival.
Peberdy
et
that
survival
to
discharge
following
in-
hospital
cardiac
arrest
is
lower
during
nights
(14.7%
[95%
CI,
14.3–15.1%]
vs.
19.8%
[95%
CI,
19.5–20.1%])
or
weekends
(20.6%
[95%
CI,
20.3–21%]
vs.
17.4%
[95%
CI,
16.8–18%])
compared
with
day/evening
or
weekdays,
even
after
accounting
for
many
poten-
tially
confounding
IHCA
event
and
hospital
factors.
Our
current
study
confirms
that
nights
and
weekends
are
associated
with
an
increased
hazard
ratio
for
death
prior
to
hospital
discharge
in
patients
regardless
of
the
initial
documented
IHCA
rhythm
and
goes
a
step
beyond
the
previously
reported
data
in
demonstrating
an
increased
hazard
ratio
for
death
during
those
times
in
which
there
is
an
increase
in
resuscitation
system
errors,
thus
suggesting
a
link
between
increased
error
on
nights
and
weekends
and
decreased
survival
during
those
times.
Kayser
et
al.,
that
ED
location
was
an
inde-
pendent
predictor
of
improved
survival,
speculating
that
this
was
due
to
both
the
requirement
for
ED
staff
to
receive
basic
and
the
advanced
cardiac
life
support
training,
and
their
frequent
experience
in
performing
resuscitation
compared
to
clinicians
working
on
general
hospital
floors.
Our
paper
supports
this
hypoth-
esis
by
confirming
that
IHCA
events
occurring
in
the
ED
have
a
relatively
low
percentage
of
cases
with
resuscitation
system
errors.
Not
all
types
of
errors
were
associated
with
an
increased
hazard
ratio
for
death
prior
to
hospital
discharge
in
our
study.
Olasveen-
gen
et
out-of-hospital
cardiac
arrest
patients
to
receive
ACLS
treatment
with
and
without
intravenous
drug
admin-
istration
and
determined
that
survival
to
discharge
was
the
same
in
both
groups.
However,
they
were
not
able
to
identify
the
timeframe
in
which
the
drug
therapy
was
given
in
the
group
that
received
an
intravenous
line
and
medication.
In
our
IHCA
population,
we
were
able
to
demonstrate
decreased
survival
when
the
first
vaso-
constrictor
was
administered
>5
min
after
IHCA
onset
in
patients
whose
arrest
lasted
for
at
least
5
min.
The
difference
in
our
find-
ings
is
likely
due
to
the
fact
that
the
time
from
event
onset
to
first
drug
administration
is
usually
much
shorter
in-
vs.
out-of-hospital.
In
our
study,
the
mean
time
from
event
onset
to
first
epinephrine
was
2.4
(95%
CI,
2.3,
2.4)
min.
In
contrast,
the
time
interval
from
collapse
to
first
epinephrine
in
standard
vs.
high
dose
epinephrine
pre-hospital
trials
is
approximately
20
Much
of
the
focus
on
patient
safety
and
error
prevention
in
hos-
pitals
focuses
on
interventions
that
relate
to
patient
interactions
that
are
of
higher
volume
and
lower
acuity
compared
to
resus-
citation.
In
our
study,
the
impact
of
resuscitation
team
errors
on
survival
varied
widely
by
both
error
type
and
the
initial
docu-
mented
heart
rhythm,
with
some
errors
causing
little
or
no
impact
and
others
being
associated
with
a
significantly
lower
survival,
par-
ticularly
in
the
group
of
patients
with
initial
VF/pVT.
Given
that
resuscitation
practices
need
to
occur
consistently
well
throughout
all
areas
of
the
hospital
and
that
responders
will
always
have
vary-
ing
degrees
of
expertise
and
experience,
our
findings
suggest
that
resuscitation
training
should
be
targeted
to
emphasize
avoiding
the
types
of
errors
having
the
greatest
impact
on
survival
(e.g.,
delays
in
initial
defibrillation
and
medication
administration
and
adherence
to
ACLS
protocols).
An
increasing
body
of
evidence
indicates
that
effective
lead-
ership
and
team
work
rather
than
just
individual
knowledge,
skills,
and
attitudes
are
required
to
optimize
outcomes
and
min-
imize
errors
in
a
variety
of
medical
emergencies.
behaviors
have
been
identified
that
contribute
to
effective
leader-
ship
including
providing
orienting
remarks,
inviting
team
member
contributions,
promoting
exchange
of
information
and
clear
com-
munication,
and
avoiding
performing
physical
tasks
that
can
be
assigned
to
others
during
the
emergency.
addition,
there
are
four
teamwork
behavior
principles
that
can
help
to
avoid
medi-
cal
errors:
(1)
the
leader
should
voice
specific
findings
rather
than
diagnosing
the
problem
prematurely;
(2)
all
members
of
the
team
should
“think
out
loud”
and
“talk
to
the
room”
as
the
case
unfolds;
(3)
the
leader
should
direct
period
reviews
of
quantitative
infor-
mation
(e.g.,
drug
dose,
time,
response);
and
(4)
all
members
of
the
team
should
double-check
crucial
data.
Unfortunately,
the
majority
of
these
leadership
and
team
behav-
iors
could
not
be
measured
in
this
study.
This
is
the
likely
explanation
for
why
we
were
unable
to
demonstrate
an
association
with
reported
“poor
team
leadership”
and
survival
in
our
study.
The
definition
of
“good
team
leadership”
is
subjective
and
may
not
be
reported
consistently
among
institutions
or
that
that
magnitude
of
the
effect
on
survival
of
other
resuscitation
errors
drowns
out
the
impact
of
poor
team
leadership.
Our
observations
confirm
the
association
between
the
presence
of
resuscitation
system
errors
that
are
evident
from
review
of
the
resuscitation
record
and
decreased
survival
from
IHCA
in
adults.
However,
they
do
not
point
to
a
specific
solution
to
the
problem.
A
number
of
recent
simulator-based
studies
have
identified
qualitatively
and
quantitatively
similar
problems
to
those
noted
68
J.P.
Ornato
et
al.
/
Resuscitation
83 (2012) 63–
69
Fig.
3.
Association
between
various
types
of
resuscitation
system
errors
and
the
hazard
ratio
for
death
prior
to
hospital
discharge
in
patients
whose
initial
IHCA
rhythm
was
non-VF/pVT
and
VF/pVT.
during
clinical
training
can
improve
per-
formance
during
simulation
of
medical
not
all
training
is
equal
or
et
al.,
iden-
tified
specific
elements
required
to
improve
outcome,
including
multi-professional
training
of
all
healthcare
providers
who
man-
age
an
emergency
in
a
realistic
simulation
setting.
These
elements
need
to
be
incorporated
into
team
and
leadership
training,
which
are
now
recommended
in
the
2010
American
Heart
Association
Guidelines
for
Adult
and
Pediatric
Advanced
Cardiovascular
Life
4.1.
Limitations
General
limitations
of
NRCPR
include:
(1)
registry
hospitals
may
not
be
representative
of
all
hospitals;
(2)
there
is
no
on-site
valida-
tion
of
data
collection;
(3)
and
there
is
no
follow-up
after
hospital
discharge.
In
addition,
although
medication
use
is
tracked,
NRCPR
does
not
attempt
to
assess
clinical
eligibility
for
each
medication.
These
limitations
are
similar
to
those
of
other
contemporary
in-
hospital
registries.
The
specific
limitation
pertinent
to
this
analysis
is
that
NRCPR
data
is
self-reported
by
having
a
trained
abstractor
review
hospi-
tal
charts
and
code
records.
The
Get
with
the
Guidelines
NRCPR
is
a
voluntary
data
collection/analysis
quality
improvement
project.
Participating
hospitals
pay
a
fee
to
the
American
Heart
Associa-
tion
to
have
the
data
analyzed,
benchmarked,
and
reported
back
to
them
quarterly.
With
hundreds
of
hospitals
involved
through-
out
the
entire
United
States
and
very
minimal
hospital
user
fees,
it
has
not
been
feasible
to
provide
independent
data
validation
at
the
hospital
level.
The
abstractors
work
with
uniform
definitions
and
uniform
methods
of
data
acquisition.
The
abstractors
review
the
physi-
cian
and
nurse
narrative
notes
in
the
hospital
chart
and
the
“code
record”
on
each
event.
Thus,
all
of
the
errors
identified
came
from
a
review
of
documentation
in
the
patient
charts.
The
abstractors
do
not
capture
whether
the
errors
were
“recognized”
in
the
narrative
notes
by
the
doctors
and
nurses
running
the
code
or
are
evident
from
the
documentation
of
events
themselves
(which
is
the
case
for
the
majority
of
errors
that
we
looked
at).
There
is
no
way
for
the
abstractor
to
verify
whether
errors
may
have
occurred
but
were
not
documented.
This
may
have
resulted
in
an
under-reporting
of
resuscitation
team
errors.
If
this
occurred,
if
anything,
it
would
increase
the
potential
importance
of
our
findings.
Finally,
we
cannot
exclude
the
possibility
that
individu-
als
completing
the
code
sheets
could
have
checked
off
more
“error
boxes”
in
patients
who
did
not
achieve
ROSC
than
the
boxes
they
would
have
checked
had
the
patient
been
resuscitated.
4.2.
Public
health
importance
The
public
health
importance
of
these
findings
is
con-
siderable.
Eisenberg
and
Mengert,
that
there
are
350,000–750,000
adult,
IHCA
events
per
year
in
the
United
States.
Eliminating
resuscitation
system
errors
has
the
potential
to
save
21,000–44,000
additional
lives
per
year
in
the
United
States
from
IHCA.
This
figure
is
ten
times
larger
than
the
estimated
2000–4000
additional
lives
saved
per
year
from
out-of-hospital
cardiac
arrest
that
drove
widespread
deployment
of
public
access
defibrillation
programs
throughout
the
country.
5.
Conclusions
We
conclude
that
the
presence
of
resuscitation
system
errors
that
are
evident
from
review
of
the
resuscitation
record
is
associ-
ated
with
decreased
survival
from
IHCA
in
adults.
Hospitals
should
target
their
training
of
first
responders
and
code
team
personnel
to
emphasize
the
importance
of
early
defibrillation
when
indi-
cated,
early
use
of
vasoconstrictor
medication,
and
compliance
with
established
AHA
ACLS
resuscitation
protocols.
Conflict
of
interest
statement
None
of
the
authors
have
any
relevant
conflicts.
Funding
sources
None.
Acknowledgement
None.
Appendix
A.
Get
with
the
Guidelines
– National
Registry
of
Cardiopulmonary
Resuscitation
(NRCPR)
investigators:

J.P.
Ornato
et
al.
/
Resuscitation
83 (2012) 63–
69
69
Mary
E.
Mancini,
Robert
A.
Berg,
Emilie
Allen,
Elizabeth
A.
Hunt,
Vinay
M.
Nadkarni,
Scott
Braithwaite,
Graham
Nichol,
Kathy
Dun-
can,
Tanya
Lane
Truitt,
Melinda
Smyth,
Brian
Eigel,
Paul
S.
Chan,
Tim
Mader,
Karl
B.
Kern,
Sam
Warren,
Thomas
Noel,
Romergryko
Geocadin,
Dana
Edelson,
Vince
Mosesso
and
Comilla
Sasson.
References
1. Institute
of
Medicine.
To
err
is
human:
building
a
safer
health
system.
Washing-
ton,
DC:
National
Academy
Press;
2000.
2. University
study
identifies
problems
with
IOM
report.
Hosp
Case
Manag
2000;8(Suppl.
3–4):146.
3. Peberdy
MA,
Ornato
JP,
Larkin
GL,
et
al.
Survival
from
in-hospital
cardiac
arrest
during
nights
and
weekends.
JAMA
2008;299:785–92.
4. Chan
PS,
Krumholz
HM,
Nichol
G,
Nallamothu
BK.
Delayed
time
to
defibrillation
after
in-hospital
cardiac
arrest.
N
Engl
J
Med
2008;358:9–17.
5.
Kayser
RG,
Ornato
JP,
Peberdy
MA.
Cardiac
arrest
in
the
emergency
depart-
ment:
a
report
from
the
National
Registry
of
Cardiopulmonary
Resuscitation.
Resuscitation
2008;78:151–60.
6. Nadkarni
VM,
Larkin
GL,
Peberdy
MA,
et
al.
First
documented
rhythm
and
clin-
ical
outcome
from
in-hospital
cardiac
arrest
among
children
and
adults.
JAMA
2006;295:50–7.
7.
Peberdy
MA,
Kaye
W,
Ornato
JP,
et
al.
Cardiopulmonary
resuscitation
of
adults
in
the
hospital:
a
report
of
14720
cardiac
arrests
from
the
National
Registry
of
Cardiopulmonary
Resuscitation.
Resuscitation
2003;58:297–308.
8.
Hunziker
S,
Johansson
AC,
Tschan
F,
et
al.
Teamwork
and
leadership
in
cardiopul-
monary
resuscitation.
J
Am
Coll
Cardiol
2011;57:2381–8.
9.
Schaefer
HG,
Helmreich
RL.
The
importance
of
human
factors
in
the
operating
room.
Anesthesiology
1994;80:479.
10.
Schaefer
HG,
Helmreich
RL,
Scheidegger
D.
Human
factors
and
safety
in
emer-
gency
medicine.
Resuscitation
1994;28:221–5.
11.
Schaefer
HG,
Helmreich
RL,
Scheidegger
D.
Safety
in
the
operating
theatre
–
part
1:
interpersonal
relationships
and
team
performance.
Curr
Anaesth
Crit
Care
1995;6:48–53.
12.
Siassakos
D,
Bristowe
K,
Draycott
TJ,
et
al.
Clinical
efficiency
in
a
simulated
emer-
gency
and
relationship
to
team
behaviours:
a
multisite
cross-sectional
study.
BJOG
2011;118:596–607.
13.
Siassakos
D,
Draycott
TJ,
Crofts
JF,
Hunt
LP,
Winter
C,
Fox
R.
More
to
teamwork
than
knowledge,
skill
and
attitude.
BJOG
2010;117:1262–9.
14.
Siassakos
D,
Fox
R,
Crofts
JF,
Hunt
LP,
Winter
C,
Draycott
TJ.
The
management
of
a
simulated
emergency:
better
teamwork,
better
performance.
Resuscitation
2011;82:203–6.
15.
Tourgeman-Bashkin
O,
Shinar
D,
Zmora
E.
Causes
of
near
misses
in
critical
care
of
neonates
and
children.
Acta
Paediatr
2008;97:299–303.
16.
Manser
T.
Teamwork
and
patient
safety
in
dynamic
domains
of
health-
care:
a
review
of
the
literature.
Acta
Anaesthesiol
Scand
2009;53:
143–51.
17.
Olasveengen
TM,
Sunde
K,
Brunborg
C,
Thowsen
J,
Steen
PA,
Wik
L.
Intravenous
drug
administration
during
out-of-hospital
cardiac
arrest:
a
randomized
trial.
JAMA
2009;302:2222–9.
18.
Brown
CG,
Martin
DR,
Pepe
PE,
et
al.
A
comparison
of
standard-dose
and
high-
dose
epinephrine
in
cardiac
arrest
outside
the
hospital.
The
Multicenter
High-
Dose
Epinephrine
Study
Group.
N
Engl
J
Med
1992;327:1051–5.
19. Abella
BS,
Alvarado
JP,
Myklebust
H,
et
al.
Quality
of
cardiopulmonary
resusci-
tation
during
in-hospital
cardiac
arrest.
JAMA
2005;293:305–10.
20. Abella
BS,
Sandbo
N,
Vassilatos
P,
et
al.
Chest
compression
rates
during
cardiopulmonary
resuscitation
are
suboptimal:
a
prospective
study
during
in-
hospital
cardiac
arrest.
Circulation
2005;111:428–34.
21.
Kramer-Johansen
J,
Myklebust
H,
Wik
L,
et
al.
Quality
of
out-of-hospital
car-
diopulmonary
resuscitation
with
real
time
automated
feedback:
a
prospective
interventional
study.
Resuscitation
2006;71:283–92.
22. Chan
PS,
Nichol
G,
Krumholz
HM,
Spertus
JA,
Nallamothu
BK.
Hospital
varia-
tion
in
time
to
defibrillation
after
in-hospital
cardiac
arrest.
Arch
Intern
Med
2009;169:1265–73.
23. Hunziker
S,
Tschan
F,
Semmer
NK,
Howell
MD,
Marsch
S.
Human
factors
in
resuscitation:
lessons
learned
from
simulator
studies.
J
Emerg
Trauma
Shock
2010;3:389–94.
24.
Hunziker
S,
Tschan
F,
Semmer
NK,
et
al.
Hands-on
time
during
cardiopulmonary
resuscitation
is
affected
by
the
process
of
teambuilding:
a
prospective
ran-
domised
simulator-based
trial.
BMC
Emerg
Med
2009;9:3.
25.
Thomas
EJ,
Taggart
B,
Crandell
S,
et
al.
Teaching
teamwork
during
the
Neonatal
Resuscitation
Program:
a
randomized
trial.
J
Perinatol
2007;27:
409–14.
26.
Thomas
EJ,
Williams
AL,
Reichman
EF,
Lasky
RE,
Crandell
S,
Taggart
WR.
Team
training
in
the
neonatal
resuscitation
program
for
interns:
teamwork
and
quality
of
resuscitations.
Pediatrics
2010;125:539–46.
27.
Cooper
S.
Developing
leaders
for
advanced
life
support:
evaluation
of
a
training
programme.
Resuscitation
2001;49:33–8.
28.
Hunziker
S,
Buhlmann
C,
Tschan
F,
et
al.
Brief
leadership
instructions
improve
cardiopulmonary
resuscitation
in
a
high-fidelity
simulation:
a
randomized
con-
trolled
trial.
Crit
Care
Med
2010;38:1086–91.
29.
Bhanji
F,
Mancini
ME,
Sinz
E,
et
al.
Part
16:
education,
implementation,
and
teams:
2010
American
Heart
Association
Guidelines
for
Cardiopul-
monary
Resuscitation
and
Emergency
Cardiovascular
Care.
Circulation
2010;122:S920–33.
30.
Mancini
ME,
Soar
J,
Bhanji
F,
et
al.
Part
12:
education,
implementation,
and
teams:
2010
International
Consensus
on
Cardiopulmonary
Resuscitation
and
Emergency
Cardiovascular
Care
Science
with
Treatment
Recommendations.
Cir-
culation
2010;122:S539–81.
31.
Eisenberg
MS,
Mengert
TJ.
Cardiac
resuscitation.
N
Engl
J
Med
2001;344:1304–13.
Document Outline
- Impact of resuscitation system errors on survival from in-hospital cardiac arrest
Wyszukiwarka
Podobne podstrony:
Impact of resuscitation system errors on survival from in-hospital cardiac arrest, MEDYCYNA, RATOWNI
In hospital cardiac arrest Is it time for an in hospital chain of prevention
Impact of Artificial Gummy Fingers on Fingerprint Systems
Does the number of rescuers affect the survival rate from out-of-hospital cardiac arrests, MEDYCYNA,
THE IMPACT OF SOCIAL NETWORK SITES ON INTERCULTURAL COMMUNICATION
Hospital care after resuscitation from out of hospital cardiac arrest The emperor's new clothes
Does the number of rescuers affect the survival rate from out-of-hospital cardiac arrests, MEDYCYNA,
Marina Post The impact of Jose Ortega y Gassets on European integration
The Impact of Mary Stewart s Execution on Anglo Scottish Relations
Impact of Chronic Lead Exposure on Selected Biological Markers
social networks and planned organizational change the impact of strong network ties on effective cha
Detection and Function of Opioid Receptors on Cells from the Immune System
Impact of opiate addiction on n Nieznany
Effect of?renaline on survival in out of hospital?rdiac arrest
effect of AVR on survival
więcej podobnych podstron