Contents
lists
available
at
Resuscitation
j o
u
r n
a l
h o m
e p a g e
:
w w w . e l s e v i e r . c o m / l o c a t e / r e s u s c i t a t i o n
Clinical
paper
Impacting
sudden
cardiac
arrest
in
the
home:
A
safety
and
effectiveness
study
of
privately-owned
AEDs
夽
Dawn
B.
Jorgenson
,
Tamara
B.
Yount
,
Roger
D.
White
,
P.Y.
Liu
,
Mickey
S.
Eisenberg
,
Lance
B.
Becker
a
Philips
Healthcare,
Bothell,
WA,
United
States
b
Mayo
Clinic,
Rochester,
MN,
United
States
c
Fred
Hutchinson
Cancer
Research
Center,
Seattle,
WA,
United
States
d
Department
of
Medicine,
University
of
Washington,
Seattle,
WA,
United
States
e
Center
for
Resuscitation
Science,
Department
of
Emergency
Medicine,
University
of
Pennsylvania,
Philadelphia,
PA,
United
States
a
r
t
i
c
l
e
i
n
f
o
Article
history:
Received
23
February
2012
Received
in
revised
form
11
September
2012
Accepted
19
September
2012
Keywords:
Automated
external
defibrillator
Cardiac
arrest
Resuscitation
Defibrillation
Emergency
medical
services
Safety
a
b
s
t
r
a
c
t
Background:
Sudden
cardiac
arrest
(SCA)
remains
a
major
public
health
problem.
The
majority
of
SCA
events
occur
in
the
home;
however,
scant
data
has
been
published
regarding
the
effectiveness
of
privately
owned
AEDs.
Methods:
The
study,
initiated
in
2002
under
prescription
labeling,
continued
with
over
the
counter
avail-
ability
in
2004
and
was
completed
in
2009.
Surveillance
methods
included
annual
surveys,
follow-up
phone
calls,
media
reports,
and
use
queries
upon
order
of
replacement
pads.
AED
owners
reporting
emergency
use
of
the
device
were
contacted
for
an
in-depth
interview,
and
the
ECG
and
event
data
in
the
device’s
internal
memory
were
evaluated.
Results:
25
cases
were
identified
in
which
an
AED
was
used
on
a
patient
in
SCA.
Two
uses
were
on
children.
The
SCA
was
witnessed
in
76%
(19/25)
of
the
cases.
In
56%
(14/25),
the
patient
presented
in
VF
and
at
least
one
shock
was
delivered.
All
14
patients
who
were
shocked
had
termination
of
VF;
6
(43%)
required
more
than
one
shock
due
to
refibrillation.
Shock
efficacy
was
100%
(25/25)
for
termination
of
VF
for
all
delivered
shocks.
Of
the
patients
with
a
witnessed
arrest
who
were
shocked,
67%
(8/12)
survived
to
hospital
discharge.
There
were
no
circumstances
of
unsafe
emergency
use
of
the
AED
or
harm
to
the
patient,
responder,
or
bystanders.
Conclusions:
People
who
purchase
an
AED
for
their
home,
even
without
previous
AED
experience,
are
able
to
use
the
device
successfully
in
both
adults
and
children.
The
high
survival
rate
observed
in
this
study
demonstrates
that
lay
responders
with
privately
owned
AEDs
can
successfully
and
safely
use
the
devices.
© 2012 Elsevier Ireland Ltd. All rights reserved.
1.
Introduction
Sudden
cardiac
arrest
(SCA)
is
a
leading
cause
of
death
and
a
major
public
health
problem
worldwide.
because
of
its
unpredictable
nature,
patients
cannot
be
identified
a
priori.
Prompt
defibrillation
for
those
patients
in
ventricular
fibril-
lation
(VF)
is
the
definitive
treatment.
Delayed
defibrillation
is
far
less
successful,
with
reduced
survival
for
every
passing
minute
from
the
moment
of
cardiac
arrest.
the
past
30
years,
automated
external
defibrillators
(AEDs)
have
been
broadly
夽 A
Spanish
translated
version
of
the
abstract
of
this
article
appears
as
Appendix
in
the
final
online
version
at
http://dx.doi.org/10.1016/j.resuscitation.2012.09.033
.
∗ Corresponding
author
at:
Philips
Healthcare,
22100
Bothell
Everett
Highway,
Bothell,
WA
98021,
United
States.
Tel.:
+1
425
908
2703;
fax:
+1
425
487
7478.
address:
(D.B.
Jorgenson).
disseminated
to
facilitate
more
timely
defibrillation
and
increase
survival.
AEDs
have
gone
from
exclusive
use
by
highly
trained
responders
(paramedics)
to
successful
use
by
lay
responders
in
airports
and
airplanes,
casinos,
and
other
public
places
where
sig-
nificant
numbers
of
people
gather.
Increasing
public
awareness
of
SCA
and
defibrillation
has
helped
drive
the
placement
of
AEDs
still
further
to
locations
such
as
churches,
schools,
and
libraries.
However,
studies
have
shown
that
approximately
80%
of
SCAs
occur
in
the
home,
and
the
survival
rate
is
lower
in
the
home
than
in
public
places.
early
as
1984,
studies
were
conducted
with
AEDs
in
the
homes
of
SCA
survivors
to
see
if
family
members
could
be
adequately
trained
to
use
the
device
1989,
59
patients
at
high
risk
were
provided
an
AED;
there
were
10
arrests
over
a
57
month
period,
and
the
devices
were
used
in
6
events.
two
patients
were
in
VF,
one
died
at
the
scene
and
one
was
resuscitated
with
residual
neurologic
deficits.
0300-9572/$
–
see
front
matter ©
2012 Elsevier Ireland Ltd. All rights reserved.
150
D.B.
Jorgenson
et
al.
/
Resuscitation
84 (2013) 149–
153
Over
the
past
15
years,
AEDs
have
undergone
significant
human
factors
design
development,
such
as
incorporating
voice
prompts
to
guide
users.
User
testing
in
simulated
use
scenarios
has
demon-
strated
the
ability
of
minimally
trained
and
lay
responders
and
even
untrained
people
to
use
the
concerns
regarding
safety
issues
and
FDA
panel
supported
over-the-counter
(OTC)
sales
of
one
AED
model
in
2004.
study
was
initiated
to
capture
infrequent
home
AED
use
data.
2.
Methods
This
was
a
prospectively-designed
observational
post-market
study
voluntarily
initiated
by
the
manufacturer.
Information
was
collected
from
owners
of
the
HeartStart
Home
AED,
model
M5068A,
from
November
2002
to
December
2009.
This
is
a
semi-automatic
device
with
adhesive
pads
and
voice
prompts
to
guide
the
user.
At
study
initiation,
in
2002,
the
devices
were
sold
only
with
a
physician
prescription.
In
November
2004,
OTC
sales
were
allowed
and
the
FDA
mandated
a
surveillance
study.
For
pediatric
patients
(under
8
years
old
or
55
pounds)
a
special
pad
cartridge
inserted
into
the
device
reduces
the
delivered
energy;
this
pediatric
cartridge
remains
available
only
through
a
prescription.
The
study
was
approved
by
Western
Institutional
Review
Board,
and
a
Data
Safety
Monitoring
Committee
routinely
reviewed
data.
All
participation
was
voluntary,
and
persons
interviewed
provided
consent.
Multiple
methods
were
employed
to
identify
AED
uses:
• Product
labeling
and
the
manufacturer’s
website
encouraged
reporting
uses
to
the
manufacturer.
Incentivized
product
regis-
tration
cards,
shipped
with
each
AED,
offered
a
practice
kit
or
accessory
kit.
Owners
who
contacted
the
manufacturer
for
any
reason
were
added
to
the
registered
owners
database.
All
reg-
istered
owners
were
sent
a
yearly
survey
inquiring
if
the
AED
had
been
taken
to
the
scene
of
an
emergency,
even
if
pads
were
never
applied
to
a
patient.
If
a
survey
was
not
returned,
follow-up
telephone
calls
were
used.
• Media
reports
on
the
Internet
were
scanned
for
reported
uses.
• The
only
avenue
for
purchasing
home
replacement
pad
cartridges
was
directly
from
the
manufacturer;
all
who
called
for
replace-
ment
pads
were
queried
regarding
a
use.
Owners
who
indicated
they
had
taken
their
AED
to
the
scene
of
an
emergency
were
asked
to
volunteer
for
a
recorded
interview
con-
ducted
by
a
healthcare
professional.
The
interviewer
asked
specific
questions
on
safety
and
efficacy,
and
the
responder
described
the
use
in
his
or
her
own
words.
The
interview
was
designed
to
cap-
ture
any
difficulty
in
using
the
AED,
and
responder
information
(age,
gender,
training),
patient
information
(age,
gender,
previous
conditions),
and
resuscitation
factors
(location
of
arrest,
bystander
CPR,
shock
delivery,
patient
outcome).
If
an
AED
was
used
in
an
emergency,
a
replacement
device
was
sent
in
exchange
for
the
involved
AED
so
its
internal
memory
could
be
examined.
The
memory
includes
use
time,
number
of
shocks,
patient
impedance,
shock
analysis
decisions,
and
ECG.
Each
case
was
categorized
in
terms
of
a
patient
in
SCA
or
a
patient
who
was
recognized
as
not
being
in
SCA
or
was
determined
later
not
to
have
been
in
SCA
(e.g.,
shortness
of
breath
or
loss
of
consciousness).
The
inclusion
criteria
required
that
the
AED
be
owned
by
an
indi-
vidual
and
intended
for
the
“home.”
If
the
owner
brought
the
AED
along
when
leaving
home
(e.g.,
in
their
car),
that
use
was
included
wherever
it
occurred.
Those
who
declined
to
participate
or
could
not
be
contacted
were
excluded.
Uses
with
insufficient
information,
no
interview,
and
no
exchanged
AED
(for
memory
examination)
where
the
report
could
not
be
verified
were
excluded.
Two
reported
Table
1
Patient
and
responder
demographics.
Adult
patients,
n
=
23
Pediatric
patients,
n
=
2
Responders,
n
=
24
(1
unknown)
Age
Median:
68
years,
range:
26–90
years
4.5
months,
5
years
Median:
63
years,
range:
33–82
years
Gender
20
male,
3
female
1
male,
1
female
14
male,
10
female
Table
2
Location
of
arrest
and
responder’s
relationship
to
patient.
Location
n
Home
18
Family
business
2
Exercise
facility
2
Street/parking
lot
1
Church
1
Club
1
Relationship
n
None
5
Wife
5
Neighbor
4
Husband
2
Daughter
2
Friend
2
Father
2
Mother
1
Son-in-law
1
Brother-in-law
1
uses
were
excluded
from
analysis.
In
one
case,
an
AED
owner
who
had
a
child
at
high
risk
for
SCA
routinely
kept
a
pediatric
car-
tridge
installed
in
the
device.
This
owner
witnessed
an
arrest
at
a
parking
lot
where
an
adult
had
been
involved
in
a
bicycle/auto
accident
with
resulting
severe
blunt
trauma.
She
retrieved
the
AED
from
her
car
but
was
unable
to
remove
the
pediatric
cartridge
to
insert
an
adult
cartridge.
One
50
J
pediatric
energy
shock
was
deliv-
ered;
defibrillation
was
unsuccessful.
In
addition,
reports
of
AED
use
on
family
dogs
were
excluded;
in
these
cases
the
resuscitation
attempts
failed.
3.
Results
There
were
25
cases
where
the
device
was
used
on
a
patient
in
SCA.
These
uses
were
identified
through
direct
calls
to
the
manu-
facturer
(13),
owner
surveys
(10),
and
Internet
reporting
(2).
OTC
purchasers
accounted
for
18
uses
and
prescription-device
pur-
chasers
accounted
for
7
uses,
including
2
pediatric
patients.
In
addition,
there
were
10
uses
where
the
AED
was
placed
on
patients
not
in
cardiac
arrest;
one
of
these
was
a
pediatric
patient.
3.1.
Uses
on
patients
in
SCA
Patient
and
responder
demographics
are
provided
in
The
majority
of
AED
uses,
18
(72%),
occurred
in
the
home
(
with
a
responder
who
was
a
family
member,
14
(56%).
Most
respon-
ders,
17
(68%),
had
no
formal
medical
training;
the
remainder
were
physician/dentist
(3),
registered
nurse
(2),
military
caregivers
(2),
and
CPR/AED
instructor
(1).
the
responders’
level
of
CPR
and
AED
exposure
prior
to
use;
the
most
common,
18
(72%),
involved
watching
the
CD
that
is
shipped
with
the
AED.
Two
respon-
ders
reported
no
formal
AED
training;
one
knew
the
patient
had
an
AED
and
retrieved
it,
and
the
other
had
seen
an
AED
demonstrated
on
television
and
remembered
that
it
was
supposed
to
be
easy
to
use.
Both
patients
treated
by
these
two
responders
survived
and
later
received
an
ICD
implant.
D.B.
Jorgenson
et
al.
/
Resuscitation
84 (2013) 149–
153
151
Table
3
Level
of
CPR
&
AED
exposure
(multiple
answers
permitted).
CPR
and
AED
exposure
n
Watched
product
training
video
18
Read
product
materials
8
Current
CPR
(
≤5
years
ago)
9
CPR
5
and
≤
10
years
ago
3
CPR
10
and
≤
20
years
ago
1
CPR
20
and
≤
30
years
ago
6
CPR
30
years
ago
1
Practiced
use
2
Watched
TV
demonstration
show
2
Watched
demonstration
by
AED
distributor
1
First
aid
class
(year
unknown)
1
a
Some
responders
specified
that
their
CPR
class
did
not
cover
AED
training,
par-
ticularly
those
who
took
the
class
a
long
time
ago.
Table
4
Resuscitation
characteristics.
Characteristic
Percentage
(n)
Witnessed
76%
(19/25)
CPR
performed
88%
(22/25)
CPR
before
AED
applied
to
patient
52%
(11/21,
1
unknown)
AED
CPR
instruction
set
utilized
55%
(12/22)
Patients
presenting
in
VF
56%
(14/25)
Patients
with
refibrillation
43%
(6/14)
Shock
efficacy
100%
(25/25)
a
summary
of
event
characteristics.
SCA
was
witnessed
in
19
(76%)
of
the
25
cases.
In
22
(88%)
cases,
CPR
was
performed
and
in
12
(55%)
cases
the
user
initiated
the
AED’s
CPR
instruction
set
and
audio
metronome
for
compression
timing.
In
14
(56%)
cases,
the
patient
presented
in
VF
and
at
least
one
shock
was
delivered;
the
median
shock
number
was
1
(range
1–5).
The
median
(range)
time
from
pads
placed
on
the
patient
to
the
first
shock
was
21
(15–53)
s.
All
14
patients
who
were
shocked
had
ter-
mination
of
VF;
6
of
the
14
(43%)
required
more
than
one
shock
due
to
refibrillation.
Shock
efficacy
was
100%
(25/25)
for
termina-
tion
of
VF
for
all
delivered
shocks.
Of
the
14
shocked,
12
(86%)
had
a
witnessed
arrest
and
2
(14%)
had
an
unwitnessed
arrest.
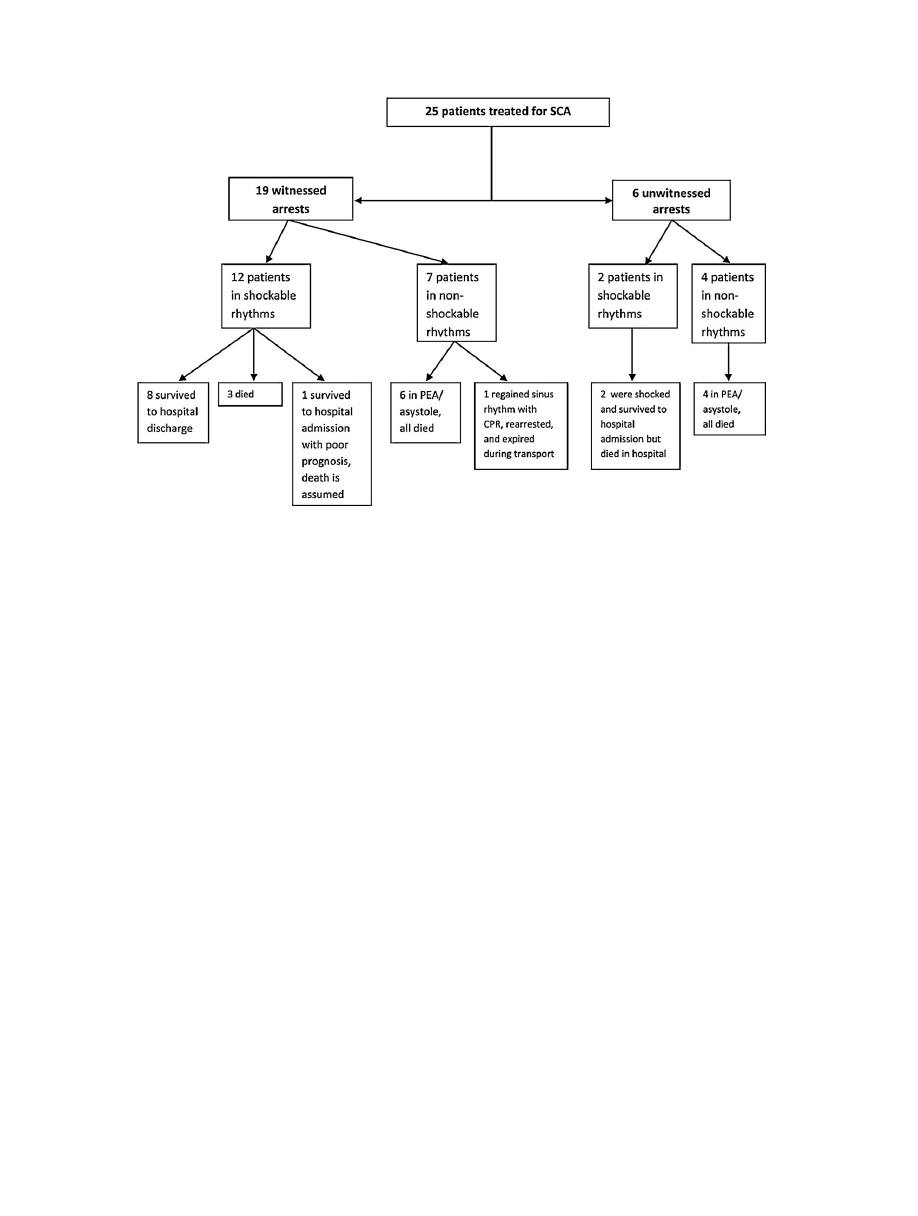
A
summary
flowchart
is
shown
in
patients
with
an
unwitnessed
arrest
who
were
shocked
survived
to
hospital
admis-
sion
but
later
died
in
hospital.
Of
the
12
patients
with
a
witnessed
arrest
who
were
shocked,
8
(67%)
survived
to
hospital
discharge.
Of
the
remaining
4
patients,
3
were
known
to
have
died
(one
had
a
pulse
during
transport
but
the
resuscitation
was
stopped
due
to
a
DNR
order)
and
1
survived
to
hospital
admission
but
had
a
poor
prognosis;
death
is
assumed.
There
were
7
patients
with
a
witnessed
arrest
who
presented
with
a
non-shockable
rhythm.
All
of
these
patients
died;
6
were
in
asystole/PEA
and
1
reportedly
regained
sinus
rhythm
with
CPR
but
rearrested
and
expired
during
transport.
3.2.
Pediatric
SCA
Due
to
the
scarcity
of
pediatric
SCA
events,
a
brief
qualitative
summary
of
two
uses
is
presented.
A
4.5-month-old
baby
girl,
who
had
survived
a
previous
SCA,
was
defibrillated
by
her
parents.
The
patient’s
physician
had
recommended
an
AED
to
the
family.
The
father
reported
the
infant
had
been
awakened
to
have
propra-
nolol
administered;
she
began
crying,
became
limp
and
apneic
and
then
lost
consciousness.
The
father
began
CPR,
called
EMS,
placed
the
AED
with
pediatric
pads
in
an
anterior/posterior
position,
and
delivered
one
shock.
The
infant
was
awake
and
crying
when
EMS
arrived.
The
infant
had
an
ICD
implanted
and
survived
to
hospital
discharge.
In
the
second
pediatric
case,
the
mother
of
a
five-year-old
boy
with
congenital
atrioventricular
canal
defect
and
pulmonary
steno-
sis
had
an
AED
because
their
doctor
ordered
it
after
the
insertion
of
an
artificial
heart
valve.
After
waking
the
child
for
the
first
day
of
kindergarten,
she
saw
him
fall
and
not
get
up.
She
applied
the
AED
and
delivered
one
shock
then
began
CPR
using
the
AED
CPR
instruction
set.
He
refibrillated
and
the
AED
advised
a
second
shock,
which
she
delivered.
He
survived
this
episode
and
received
an
ICD
implant.
3.3.
Uses
of
the
AED
on
patients
not
in
SCA
There
were
9
instances
of
AED
use
on
adults
and
1
use
on
a
child
not
in
arrest.
In
all
cases,
the
AED
did
not
advise
a
shock.
In
each
case
concern
for
the
patient
resulted
in
caregivers’
applying
the
AED
even
though
in
several
instances
the
patient
was
conscious
and/or
breathing
(allowed
under
AED
instructions).
In
all
but
two
cases,
EMS
was
called
and
assumed
care.
Brief
summaries
of
these
cases
are
given
as
follows:
• A
responsive
man
who
had
had
a
previous
myocardial
infarction
was
having
severe
chest
pain,
shortness
of
breath,
and
sweating.
The
patient
felt
better
within
minutes
after
the
AED
was
applied;
EMS
was
not
called.
• A
woman
who
had
previously
had
a
stroke
became
unresponsive.
The
AED
was
applied
but
no
CPR
was
performed.
The
responder
reported
breathing
and
faint
pulses
at
the
neck
and
wrist.
The
patient
reportedly
had
another
stroke.
• A
physician
self-applied
pads
when
he
was
in
atrial
fibrillation
to
see
“what
the
AED
would
do”
and
reported
he
“knew
it
would
not
shock.”
• A
patient
with
an
extensive
cardiac
history
reported
she
was
not
feeling
well
and
was
light-headed.
She
checked
her
pulse
and
self-applied
oxygen
and
the
AED.
She
reported
relief
and
did
not
call
EMS.
• A
responder
applied
his
AED
to
a
man
who
was
conscious
and
sweating.
He
thought
the
man
was
having
a
myocardial
infarction
and
wanted
to
be
ready.
• A
responder
was
called
to
a
neighbor’s
home
because
someone
had
collapsed.
The
responder
applied
the
AED
as
he
was
not
sure
if
the
patient
was
breathing
and
thought
there
was
a
slight
pulse.
• A
wife
noticed
that
her
husband,
who
had
an
extensive
cardiac
history,
could
not
speak.
She
checked
for
signs
of
stroke
and
applied
the
AED,
wanting
to
be
prepared.
• A
woman
reported
that
her
husband
was
unresponsive
on
two
separate
occasions;
each
time,
she
applied
the
AED.
• An
AED
was
placed
on
a
two-year-old
child,
with
a
history
of
long
QT
syndrome,
after
a
four-year-old
sibling
(also
diagnosed
with
long
QT
syndrome)
alerted
their
mother.
The
AED
was
applied
after
a
seizure
started
because
the
mother
“knew
it
would
not
hurt
her.”
CPR
was
started.
EMS
arrived,
and
the
child
recovered.
3.4.
Safety
and
post-use
assessment
The
post-use
interview
included
questions
about
both
patients
and
rescuers,
including
specific
inquiries
regarding
shock
safety
and
inappropriate
shocks.
There
were
no
reported
instances
of
unsafe
emergency
use
of
the
AED
or
harm
during
use
to
the
patient,
responder,
or
bystanders.
Responders
who
treated
patients
in
SCA
reported
they
felt
adequately
trained
in
24
(96%)
of
the
cases;
one
felt
she
should
have
rehearsed
more
in
order
to
be
faster.
Twenty-
four
of
25
(96%)
reported
they
would
use
the
AED
again
if
needed,
while
one
rescuer
was
uncertain.
152
D.B.
Jorgenson
et
al.
/
Resuscitation
84 (2013) 149–
153
Fig.
1.
Event
summary
flowchart.
4.
Discussion
Efforts
to
disseminate
AEDs
to
public
areas
were
initiated
in
1993,
yet
the
overall
survival
rate
for
SCA
in
the
U.S.
remains
at
approximately
2000,
Valenzuela
studied
AED
use
in
casinos
by
security
officers.
of
the
105
patients
(53%)
survived
to
hospital
discharge.
In
2002,
Caffrey
demonstrated
the
successful
use
of
AEDs
at
three
Chicago
airports.
that
study,
18
patients
presented
in
VF
and
11
(61%)
were
resuscitated,
a
survival
rate
for
witnessed
VF/VT
quite
similar
to
that
in
this
report.
The
Public
Access
Defibrillation
Trial
in
2004
studied
randomized
AED
placement
in
community
units
such
as
shopping
malls,
recreation
centers
and
hotels.
were
30
survivors
out
of
128
arrests
(23%)
in
the
AED
arm.
In
another
study
of
public
access
defibrilla-
tion,
an
AED
was
applied
in
4.4%
of
VF
arrests,
with
spontaneous
pulses
present
in
84%
by
the
end
of
EMS
care,
resulting
in
a
52.5%
survival
2008,
the
Home
Automated
External
Defibrilla-
tor
Trial
(HAT)
enrolled
7001
patients
at
increased
risk
for
sudden
cardiac
arrest.
They
compared
survival
with
an
AED
in
the
home
to
a
control
group
without
AEDs
who
were
instructed
to
call
EMS
and
perform
CPR.
the
two-year
enrollment
period
and
two-
year
follow-up
period,
AEDs
were
used
on
32
patients,
14
received
an
appropriate
shock,
and
4
survived
to
discharge.
Mortality
did
not
differ
significantly
between
the
groups.
It
is
noteworthy
that
for
the
HAT
study,
AEDs
were
provided
to
specific
high-risk
indi-
viduals
with
training
and
follow-up
whereas
this
study
followed
people
who
purchased
an
AED
due
to
personal
choice.
While
80%
of
SCAs
occur
in
the
home,
on
private
AED
use
is
limited.
In
this
study
there
were
very
few
uses
reported
from
owners
who
purchased
their
AEDs
with
a
prescription,
and
we
found
no
obvious
differences
in
these
uses
or
training
versus
those
who
purchased
OTC.
Many
owners
could
not
recall
the
condition
under
which
they
purchased
their
AED.
In
this
study,
the
ability
of
home
users,
some
with
no
training
or
experience,
to
use
an
AED
has
been
demonstrated.
We
have
reported
that,
of
home
AEDs
uses,
8
of
12
(67%)
patients
with
witnessed
VF
arrest
and
subsequent
shock
survived
to
hospital
discharge.
In
one
use
a
responder
(a
prescription
purchaser)
was
unable
to
remove
a
pediatric
cartridge,
resulting
in
the
delivery
of
a
pediatric
energy
dose
to
an
adult.
Of
note,
this
same
owner
responded
to
another
adult
SCA
about
one
year
later
with
a
success-
ful
outcome.
In
all
other
uses
the
responders
were
able
to
use
the
AEDs
as
intended,
and
there
were
no
safety
issues
or
harm
reported
to
bystanders
or
responders
or
effectiveness
issues.
There
are
several
limitations
to
this
study
of
privately
owned
AEDs.
The
number
of
patients
with
SCA
treated
with
AEDs
was
small.
Although
we
queried
owners,
it
is
likely
there
were
uses
not
reported
to
us
thus
the
ability
to
discover
complications
or
adverse
events
from
AED
use
was
limited.
Efforts
were
made
to
encourage
owners
to
register
their
devices;
however,
the
portable
nature
of
the
AEDs
along
with
the
inherent
difficulties
of
following
owners
(who
marry,
change
names,
die,
give
away
their
AEDs,
etc.)
and
the
reluctance
of
private
AED
owners
to
participate
in
this
type
of
sur-
vey
made
this
process
difficult.
It
may
be
that
responders
were
more
likely
to
report
a
use
or
be
interviewed
if
the
use
was
successful.
Although
we
interviewed
responders
and
reviewed
the
electron-
ically
recorded
memory
of
the
AEDs,
we
did
not
have
access
to
medical
records
for
verification.
5.
Conclusions
Although
the
number
of
uses
was
small,
this
study
demonstrates
the
safety
and
effectiveness
of
home
AEDs
used
by
lay
persons
with
no
or
minimal
training.
Both
adult
and
pediatric
patients
were
defibrillated
and
survived.
There
were
no
reports
of
injury
to
responders,
bystanders,
or
patients.
In
many
cases
CPR
was
per-
formed
with
the
guidance
of
the
AED’s
CPR
instruction
set.
In
this
study,
the
survival
rate
in
patients
with
witnessed
arrest
and
a
shockable
rhythm
treated
with
home
AEDs
was
similar
to
rates
reported
for
airports
and
casinos.
The
data
suggests
AED
technol-
ogy
designed
for
home
use
appears
to
be
safe
and
effective,
and
may
be
an
important
additional
strategy
for
treatment
of
SCA.

D.B.
Jorgenson
et
al.
/
Resuscitation
84 (2013) 149–
153
153
Conflict
of
interest
statement
Dawn
Jorgenson
and
Tamara
Yount
are
employees
of
Philips
Healthcare
which
manufacturers
the
AED
used
in
this
study.
The
other
authors
have
no
conflict
to
declare.
Acknowledgements
We
thank
the
AED
owners
and
responders
who
shared
their
personal
stories
with
us.
We
would
also
like
to
thank
Michael
Sayre
for
his
work
on
the
Data
Safety
and
Monitoring
Board
and
Robin
Havrda,
Karen
Uhrbrock,
Richard
O’Hara,
Garth
Bammer,
Francesca
Infantine
and
Emily
Mydynski
for
their
invaluable
assistance
with
this
study.
This
work
was
supported
by
Philips
Healthcare,
Bothell,
WA.
References
1.
Zheng
ZJ,
Croft
JB,
Giles
WH,
Mensah
GA.
Sudden
cardiac
death
in
the
United
States,
1989
to
1998.
Circulation
2001;104:2158–63.
2.
Goldberger
JJ,
Cain
ME,
Hohnloser
SH,
et
al.
American
Heart
Associ-
ation/American
College
of
Cardiology
Foundation/Heart
Rhythm
Society
scientific
statement
on
noninvasive
risk
stratification
techniques
for
identify-
ing
patients
at
risk
for
sudden
cardiac
death:
a
scientific
statement
from
the
American
Heart
Association
Council
on
Clinical
Cardiology
Committee
on
Elec-
trocardiography
and
Arrhythmias
and
Council
on
Epidemiology
and
Prevention.
Circulation
2008;118:1497–518.
3.
Larsen
MP,
Eisenberg
MS,
Cummins
RO,
Hallstrom
AP.
Predicting
survival
from
out-of-hospital
cardiac
arrest:
a
graphic
model.
Ann
Emerg
Med
1993;22:1652–8.
4.
Marenco
JP,
Wang
PJ,
Link
MS,
Homoud
MK,
Estes
3rd
NA.
Improving
survival
from
sudden
cardiac
arrest:
the
role
of
the
automated
external
defibrillator.
JAMA
2001;285:1193–200.
5. Swor
RA,
Jackson
RE,
Compton
S,
et
al.
Cardiac
arrest
in
private
locations:
differ-
ent
strategies
are
needed
to
improve
outcome.
Resuscitation
2003;58:171–6.
6.
Weisfeldt
ML,
Everson-Stewart
S,
Sitlani
C,
et
al.
Ventricular
tachyarrhythmias
after
cardiac
arrest
in
public
versus
at
home.
N
Engl
J
Med
2011;364:313–21.
7.
Cummins
RO,
Eisenberg
MS,
Bergner
L,
Hallstrom
A,
Hearne
T,
Murray
JA.
Automatic
external
defibrillation:
evaluations
of
its
role
in
the
home
and
in
emergency
medical
services.
Ann
Emerg
Med
1984;13:798–801.
8.
Eisenberg
MS,
Moore
J,
Cummins
RO,
et
al.
Use
of
the
automatic
external
defi-
brillator
in
homes
of
survivors
of
out-of-hospital
ventricular
fibrillation.
Am
J
Cardiol
1989;63:443–6.
9.
Callejas
S,
Barry
A,
Demertsidis
E,
Jorgenson
D,
Becker
LB.
Human
factors
impact
successful
lay
person
automated
external
defibrillator
use
during
simulated
cardiac
arrests.
Crit
Care
Med
2004;32:S406–13.
10. Mosesso
VN,
Shapiro
AH,
Stein
K,
Burkett
K,
Wang
H.
Effects
of
AED
device
fea-
tures
on
performance
by
untrained
lay
persons.
Resuscitation
2009;80:1285–9.
11. Brown
J,
Kellermann
AL.
The
shocking
truth
about
automated
external
defibril-
lators.
JAMA
2000;284:1438–41.
12. Eisenberg
M.
On
approving
the
over-the-counter
sale
of
automated
external
defibrillators.
Ann
Emerg
Med
2005;45:25–6.
13. Bar-Cohen
Y,
Walsh
EP,
Love
BA,
Cecchin
F.
First
appropriate
use
of
automated
external
defibrillator
in
an
infant.
Resuscitation
2005;67:135–7.
14. Kerber
RE,
Becker
LB,
Bourland
JD,
et
al.
Automatic
external
defibrillators
for
public
access
defibrillation:
recommendations
for
specifying
and
reporting
arrhythmia
analysis
algorithm
performance,
incorporating
new
waveforms,
and
enhancing
safety.
A
statement
for
health
professionals
from
the
American
Heart
Association
Task
Force
on
Automatic
External
Defibrillation,
Subcommittee
on
AED
Safety
and
Efficacy.
Circulation
1997;95:1677–82.
15.
Sasson
C,
Rogers
MAM,
Dahl
J,
Kellermann
AL.
Predictors
of
survival
from
out-of-
hospital
cardiac
arrest
a
systematic
review
and
meta-analysis.
Circ:
Cardiovasc
Qual
Outcomes
2010;3:63–81.
16.
Valenzuela
TD,
Roe
DJ,
Nichol
G,
Clark
LL,
Spaite
DW,
Hardman
RG.
Outcomes
of
rapid
defibrillation
by
security
officers
after
cardiac
arrest
in
casinos.
N
Engl
J
Med
2000;343:1206–9.
17. Caffrey
SL,
Willoughby
PJ,
Pepe
PE,
Becker
LB.
Public
use
of
automated
external
defibrillators.
N
Engl
J
Med
2002;347:1242–7.
18.
Hallstrom
AP,
Ornato
JP,
Weisfeldt
M,
et
al.
Public-access
defibrillation
survival
after
out-of-hospital
cardiac
arrest.
N
Engl
J
Med
2004;351:637–46.
19. Rea
TD,
Olsufka
M,
Bemis
B,
et
al.
A
population-based
investigation
of
pub-
lic
access
defibrillation:
role
of
emergency
medical
services
care.
Resuscitation
2010;81:163–7.
20.
Bardy
GH,
Lee
KL,
Mark
DB,
et
al.
Home
use
of
automated
external
defibrillators
for
sudden
cardiac
arrest.
N
Engl
J
Med
2008;358:1793–804.
Document Outline
Wyszukiwarka
Podobne podstrony:
(Gardening) Beneficial Insects In The Home Garden
In the Home Bathroom2
Dangers in the Home
Occult Experiments in the Home Personal Explorations of Magick and the Paranormal by Duncan Barford
57 Pattern Relationships in the Home
[Psilocybin]Experiment in the Home Cultivation of Psychedelic Mushrooms A journal of a growing proj
In The Home Living Room
Spanish Influence in the New World and the Institutions it I
93 Team Attacking in the Attacking 1 3 – Crossing and Finis
The main press station is installed in the start shaft and?justed as to direction
The Mammoth in the Myths, Ethnography, and Archeology of Northern Eurasia
Far Infrared Energy Distributions of Active Galaxies in the Local Universe and Beyond From ISO to H
At Work & In The Office Jobs and Occupations
Tourism Human resource development, employment and globalization in the hotel, catering and tourism
Test English tenses in the reported speech and passive voice
Edgar Allan Poe The Murders In the Rue Morgue and Other Stories
więcej podobnych podstron