
HYPERTENSION
IN CHILDREN AND
ADOLESCENTS

• Hypertension is defined as average SBP
and/or diastolic BP (DBP)
that is 95th
percentile for gender, age, and height
on 3 occasions.
• Prehypertension in children is defined
as average SBP or DBP
levels that are >
90th percentile but <95th percentile.
DEFINITION OF
HYPERTENSION

DEFINITION OF
HYPERTENSION
• As
with adults, adolescents with BP levels
120/80 mm Hg should
be considered
prehypertensive.
• A patient with BP levels >95th
percentile
in
a physician's
office or clinic, who is
normotensive
outside a clinical setting,
has "white-coat hypertension."
Ambulatory
BP monitoring (ABPM)
is
usually required to make this diagnosis.

MEASUREMENT OF BP IN
CHILDREN
• Children >3 years old who are seen in a
medical setting should
have their BP
measured.
• The preferred method of BP
measurement
is auscultation.
• Correct measurement requires a cuff
that
is appropriate to the
size of the
child's upper arm.

Conditions Under Which Children
<3 Years Old Should Have BP
Measured
• History of prematurity, very low birth
weight, or other neonatal complication
requiring intensive care
• Congenital heart disease (repaired or
nonrepaired)
• Recurrent urinary tract infections,
hematuria, or proteinuria
• Known renal disease or urologic
malformations
• Family history of congenital renal disease

• Solid-organ transplant
• Malignancy or bone marrow transplant
• Treatment with drugs known to raise BP
• Other systemic illnesses associated
with hypertension (neurofibromatosis,
tuberous sclerosis, etc)
• Evidence of elevated intracranial
pressure
Conditions Under Which
Children <3 Years Old Should
Have BP Measured

Signs and symptoms of
hypertension
• Headache
• Nose bleeding
• Polyuria/oliguria
• Blurred vision
• Seizures
• Stroke
• Heart failure
• Coma
Most of the patients are asymptomatic, which
emphasizes the importance of frequent BP
measuring

• the BP in children should
be measured with
a standard clinical sphygmomanometer,
using
a stethoscope placed over the
brachial artery pulse, proximal
and medial
to the cubital fossa, and below the bottom
edge of
the cuff
• the child should have avoided stimulant
drugs or foods, have been sitting quietly
for 5 minutes, and
seated with his or her
back supported, feet on the floor and
right
arm supported, cubital fossa at heart level.
BP measurement
BP measurement

• Correct measurement of BP in children
requires use of a cuff
that is appropriate
to the size of the child's upper right arm.
• The equipment necessary to measure BP
in children, ages 3 through
adolescence,
includes child cuffs of different sizes and
must
also include a standard adult cuff, a
large adult cuff, and
a thigh cuff.
• The latter 2 cuffs may be needed for use
in adolescents.
BP measurement

BP measurement

• SBP is determined by the onset of the
"tapping" Korotkoff sounds (K1).
• Population data in children and risk-
associated epidemiologic data in adults
have established the fifth Korotkoff
sound (K5), or the disappearance of
Korotkoff sounds, as the definition of
DBP.
BP measurement
• The standard device for BP
measurements has been the mercury
manometer.
• Because of its environmental toxicity,
mercury
has been increasingly removed
from health care settings. Aneroid
manometers are quite accurate when
calibrated on a semiannual
basis and
are recommended when mercury-
column devices cannot
be obtained.
BP measurement

• ABPM refers to a procedure in which a
portable BP device, worn
by the patient,
records BP over a specified period,
usually
24 hours. ABPM is very useful in
the evaluation of hypertension
in
children.
ABPM

• By frequent measurement and
recording
of BP, ABPM enables
computation of the mean BP during the
day,
night, and over 24 h as well as
various measures to determine
the
degree to which BP exceeds the upper
limit of normal over
a given time period,
ie, the BP load.
ABPM

• ABPM is especially helpful
in the
evaluation of white-coat hypertension as
well as the
risk for hypertensive organ
injury, apparent drug resistance,
and
hypotensive symptoms with
antihypertensive drugs.
• ABPM is
also useful for evaluating
patients for whom more information
on
BP patterns is needed, such as those
with episodic hypertension,
chronic
kidney disease, diabetes, and autonomic
dysfunction.
ABPM

• Conducting ABPM requires specific
equipment and trained staff.
• Therefore, ABPM in children and
adolescents should be used by
experts
in the field of pediatric hypertension
who are experienced
in its use and
interpretation.
ABPM

• BP standards based on gender, age,
and height provide a precise
classification of BP according to body
size.
• The revised BP
tables now include the
50th, 90th, 95th, and
99th percentiles
(with standard deviations) by gender,
age,
and height.
BP TABLES

1. Use the standard height charts to determine
the height percentile.
2. Measure and record the child's SBP and DBP.
3. Use the correct gender table for SBP and DBP.
4. Find the child's age on the left side of the
table. Follow the age row horizontally across
the table to the intersection of the line for the
height percentile (vertical column).
5. There, find the 50th, 90th, 95th, and 99th
percentiles for SBP in the left columns and for
DBP in the right columns.
Using the BP Tables

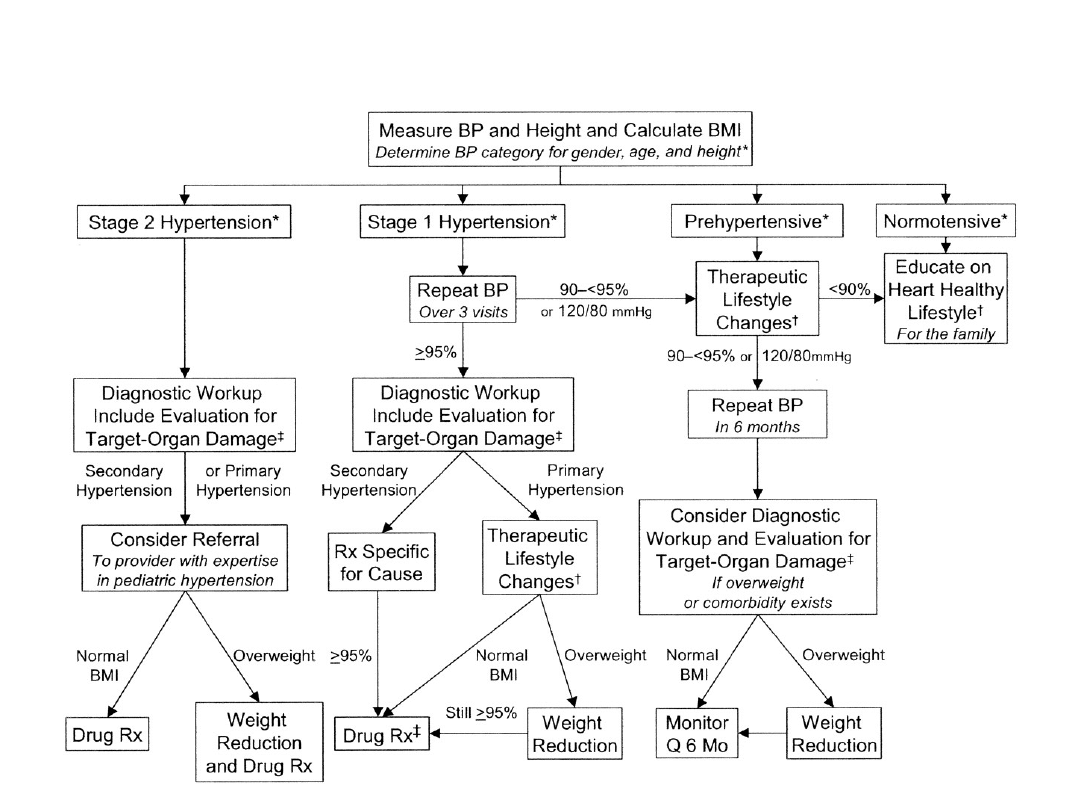
• BP <90th percentile is normal.
• BP between the
90th and 95th percentile
is prehypertension.
In adolescents,
BP >
120/80 mm Hg is prehypertension, even if
this figure is <90th
percentile.
• BP >95th percentile may be hypertension.
• If the BP is >90th percentile, the BP
should be repeated twice at the same
office visit, and an average SBP and DBP
should be used.
Using the BP Tables

• If the BP is >95th percentile, BP
should be staged. If stage 1 (95th
percentile to the 99th percentile plus 5
mm Hg), BP measurements should be
repeated on 2 more occasions. If
hypertension is confirmed, clinical
evaluation should proceed.
Using the BP Tables

• If BP is stage 2 (>99th percentile plus
5 mm Hg), prompt referral should be
made for evaluation and therapy. If
the patient is symptomatic, immediate
referral and treatment are indicated.
Those patients with a compelling
indication would be treated as the
next higher category of hypertension.
Using the BP Tables
Copyright ©2004 American Academy of
Pediatrics
National High Blood Pressure Education Program
Working Group on High Blood Pressure in Children and
Adolescents, Pediatrics 2004,11,4:555-576

• RENAL
• ENDOCRINE
• VASCULAR
• NEUROLOGIC
• MEDICATIONS
• TRAUMA
• MISCELLANEOUS
CAUSES OF ACUTE AND CHRONIC
HYPERTENSION IN THE PEDIATRIC
POPULATION

RENAL CASES
ACUTE
• Acute poststreptococcal
glomerulonephrosis
• Hemolytic uremic
syndrome
• Acute nephritis, any case
• Acute renal failure, any
case
• Renal or urinary tract
surgery
CHRONIC
• Chronic renal insufficiency
or failure, any case
• Chronic glomerulopathies
• Obstructive uropathy
• Polycytic kidney disease
• Reflux nephropathy
• Postrenal transplantation
• Wilms tumor
VASCULAR CASES
ACUTE
• Renal artery thrombosis
CHRONIC
• Renal artery stenosis
• Coarctation of the aorta
• Systemic vasculisitis
• William syndrome
• Renal artery embolism
• Neurofibromatosis

MEDICATION CASES
ACUTE
• Steroids
• Oral contraceptives
• Amphetamines/cocaine
• Rebound of
discontinuation of
antihypertensives
• Beta-adrenergic
agonists/theophylline
• Cafffeine/nicotine
CHRONIC
• Steroids
• Erythropoetin
• Cyclosporine/tacrolimus
• Oral contraceptives

NEUROLOGIC CASES
ACUTE
• Autonomic dysfunction
(Guillan-Barre)
• Anxiety/pain
• Seizures
• Encephalitis
• Subdural hemorrhage
CHRONIC
• Increased
intracranial pressure
• Poliomyelitis
• Neurofibromatosis
• Quadriplegia

MISCELLANEOUS CASES
ACUTE
• Volume overload
• Hypercalcemia
CHRONIC
• Essential hypertension
• Obesity
• Bronchopulmonary
dysplasia
• pregnancy

TRAUMA
CASES
ACUTE
• Burns
• Traction (especially
femoral)
• Perirenal hematoma
• Increased intracranial
pressure
• Spinal cord injury
CHRONIC
• Pheochromocytoma
• Cushing syndrome
• Congenital adrenal
hyperplasia
• Hypo/hyperthyroidism
• Neuroblastoma
• Hyperparathyroidism
• Primary
hyperaldosteronism
• Genetic hypertensive
endocrinopathies
• Diabetic nephropathy
ENDOCRINE
CASES

• Primary hypertension is identifiable in
children and adolescents.
• Both hypertension and
prehypertension have become a
significant
health issue in the young
because of the strong association
of
high BP with overweight and the
marked increase in the prevalence
of
overweight children.
PRIMARY HYPERTENSION

• Primary hypertension
in childhood is
usually characterized by mild or stage
1 hypertension
and is often associated
with a positive family history of
hypertension
or cardiovascular disease
(CVD).
PRIMARY HYPERTENSION
• The evaluation of hypertensive
children
should include assessment
for
additional risk factors (low plasma
high-density lipoprotein cholesterol,
elevated plasma
triglyceride, and
abnormal glucose tolerance).
• Because
of an association of sleep
apnea with overweight and
high BP,
a
sleep history should be obtained.
PRIMARY HYPERTENSION

• Secondary hypertension is more
common in children than in adults.
• Because overweight is strongly linked
to hypertension, BMI
should
be
calculated as part of the physical
examination.
EVALUATION FOR SECONDARY
HYPERTENSION

• Once
hypertension is confirmed, BP should
be measured in both
arms
and a leg.
• Very young children, children with stage 2
hypertension,
and
children or adolescents
with clinical signs that suggest
systemic
conditions associated with hypertension
should be evaluated
more completely than
in those with stage 1 hypertension.
EVALUATION FOR SECONDARY
HYPERTENSION
Physical Examination Findings
Suggestive of Definable
Hypertension
Finding
Possible Etiology
Vital signs
Tachycardia
Decreased lower
extremity pulses;
drop in BP from
upper to lower
extremities
Hyperthyroidism,
pheochromocytoma,
neuroblastoma, primary
hypertension
Coarctation of the aorta
Eyes
Retinal changes
Severe hypertension, more
likely to be associated with
secondary hypertension

Finding
Possible Etiology
Ear, nose,
and throat
Adenotonsillar
hypertrophy
Suggests association with
sleep-disordered breathing
(sleep apnea), snoring
Height/weigh
t
Growth
retardation
Obesity (high
BMI)
Truncal obesity
Chronic renal failure
Primary hypertension
Cushing syndrome, insulin
resistance syndrome
Head and
neck
Moon faces
Elfin faces
Webbed neck
Thyromegaly
Cushing syndrome
William syndrome
Turner syndrome
Hyperthyroidism
Skin
Pallor, flushing,
diaphoresis
Acne, hirsutism,
striae
Pheochromocytoma
Cushing syndrome, anabolic
steroid abuse
Skin
Café-au-lait spots
Adenoma
sebaceum
Malar rash
Acanthrosis
nigricans
Neurofibromatosis
Tuberous sclerosis
Systemic lupus erythematosus
Type 2 diabetes
Chest
Widely spaced
nipples
Heart murmur
Friction rub
Apical heave
Turner syndrome
Coarctation of the aorta
Systemic lupus erythematosus
(pericarditis), collagen-
vascular disease, end stage
renal disease with uremia
LVH/chronic hypertension
Finding
Possible Etiology
Abdomen
Mass
Epigastric/flank
bruit
Palpable kidneys
Wilms tumor, neuroblastoma,
pheochromocytoma
Renal artery stenosis
Polycystic kidney disease,
hydronephrosis, multicystic-
dysplastic kidney, mass (see
above)
Genitalia
Ambiguous/virilizati
on
Adrenal hyperplasia
Extremitie
s
Joint swelling
Muscle weakness
Systemic lupus erythematosus,
collagen vascular disease
Hyperaldosteronism, Liddle
syndrome
Clinical Evaluation of Confirmed
Hypertension
Study or Procedure
Purpose
Target Population
Evaluation for identifiable
causes
History, including sleep
history, family history, risk
factors, diet, and habits such
as smoking and drinking
alcohol; physical
examination
History and physical
examination help focus
subsequent evaluation
All children with
persistent BP
95th percentile
BUN, creatinine, electrolytes,
urinalysis, and urine culture
RBC
Renal ultrasound
renal disease and
chronic pyelonephritis
anemia, consistent with
chronic renal disease
renal scar, congenital
anomaly, or disparate
renal size
All children with
persistent BP
95th percentile
Study or Procedure
Purpose
Target Population
Evaluation for
comorbilidity
Fasting lipid panel, fasting
glucose
Identify
hyperlipidemia,
identify metabolic
abnormalities
Overweight patients
with BP at 90th–94th
percentile; all patients
with BP 95th
percentile; family
history of
hypertension or CVD;
child with chronic
renal disease
Drug screen
Polysomnography
Identify substances
that might cause
hypertension
Identify sleep
disorder in
association with
hypertension
History suggestive of
possible contribution
by substances or
drugs.
History of loud,
frequent snoring
Study or Procedure
Purpose
Target Population
Evaluation for target-
organ damage
Echocardiogram
Identify LVH and
other indications of
cardiac
involvement
Patients with
comorbid risk factors
*
and BP 90th–94th
percentile; all patients
with BP 95th
percentile
Retinal exam
Identify retinal
vascular changes
Patients with
comorbid risk factors
*
and BP 90th–94th
percentile; all patients
with BP 95th
percentile
Study or Procedure
Purpose
Target Population
Additional evaluation as
indicated
ABPM
Identify white-coat
hypertension,
abnormal diurnal
BP pattern, BP load
Patients in whom
white-coat
hypertension is
suspected, and when
other information on
BP pattern is needed
Plasma renin determination
Identify low renin,
suggesting
mineralocorticoid-
related disease
Young children with
stage 1 hypertension
and any child or
adolescent with stage
2 hypertension
Study or Procedure
Purpose
Target Population
Renovascular imaging
Isotopic scintigraphy (renal
scan)
Duplex Doppler flow studies
3-Dimensional CT
Arteriography: DSA or classic
Identify
renovascular
disease
Young children with
stage 1 hypertension
and any child or
adolescent with stage
2 hypertension
Plasma and urine steroid
levels
Plasma and urine
catecholamines
Identify steroid-
mediated
hypertension
Identify
catecholamine-
mediated
hypertension
Young children with
stage 1 hypertension
and any child or
adolescent with stage
2 hypertension
Young children with
stage 1 hypertension
and any child or
adolescent with stage
2 hypertension
Study or Procedure
Purpose
Target Population
Additional evaluation as
indicated
Thyroid hormones:FT3, FT4,
TSH
Thyroid USG
Identify
hyperthyroidism or
hypothyroidism
Young children with
stage 1 hypertension
and any child or
adolescent with stage
2 hypertension with
symptoms of thyroid
disease
MIBG
Identify
pheochromocytom
a

• Target-organ abnormalities are
commonly associated with
hypertension
in children and
adolescents.
• Left ventricular hypertrophy
(LVH)
is the most prominent evidence
of target-organ damage.
TARGET-ORGAN ABNORMALITIES
IN CHILDHOOD HYPERTENSION

• Pediatric patients with established
hypertension should have
echocardiographic assessment of
left ventricular mass at diagnosis
and periodically thereafter.
• The presence of LVH is an
indication
to initiate or intensify
antihypertensive therapy.
TARGET-ORGAN ABNORMALITIES
IN CHILDHOOD HYPERTENSION

• Weight reduction is the primary therapy
for obesity-related
hypertension.
Prevention of excess or abnormal weight
gain will
limit future increases in BP.
• Regular physical activity and
restriction
of sedentary activity
will improve efforts
at weight
management and may prevent
an
excess increase in BP over time.
THERAPEUTIC LIFESTYLE
CHANGES

• Dietary modification should be
strongly encouraged in children
and
adolescents who have BP levels in
the prehypertensive range
as well as
those with hypertension.
• Family-based intervention
improves
success.
THERAPEUTIC LIFESTYLE
CHANGES

• Symptomatic hypertension
• Secondary hypertension
• Hypertensive target-organ damage
• Diabetes (types 1 and 2)
• Persistent hypertension despite
nonpharmacologic measures
Indications for Antihypertensive
Drug Therapy in Children

• Indications for antihypertensive drug
therapy in children include
secondary
hypertension and insufficient
response to lifestyle
modifications.
• Recent clinical trials have expanded
the number
of drugs that
have
pediatric dosing information. Dosing
recommendations
for
many of the
newer drugs are provided.
PHARMACOLOGIC THERAPY OF
CHILDHOOD HYPERTENSION

• Pharmacologic therapy,
when
indicated, should be initiated with
a
single drug. Acceptable
drug classes
for use in children include
ACE
inhibitors, angiotensin-receptor
blockers, ß-blockers,
calcium channel
blockers, and
diuretics.
PHARMACOLOGIC THERAPY OF
CHILDHOOD HYPERTENSION
• The goal for antihypertensive
treatment in children
should be
reduction of BP to <95th percentile
unless concurrent
conditions
are
present, in which case BP should be
lowered to
<90th
percentile.
• Severe, symptomatic hypertension
should
be treated with intravenous
antihypertensive drugs.
PHARMACOLOGIC THERAPY OF
CHILDHOOD HYPERTENSION

• These drugs are most efficacious in the
settings of renin-mediated hypertension,
such as reflux nephropathy, chronic
glomerulonephritis, and renovascular
disease.
• They have additional renal protective
effects in states of prevalent
glomerulosclerosis (especially diabetic
nephropathy) and may slow the
progression of renal insufficiency from a
number of acquired and inherited renal
diseases.
ACEls

• Adverse effects of ACEls are generally
few, but include impairment of renal
functional when the glomerular filtration
rate (GFR) is less than 30 mL/min, in the
presence of bilateral renal artery
disease or renal artery disease in a
single kidney, or following kidney
transplantation.
• Other
adverse
effects
include
hyperkalemia, neutropenia, anemia, dry
cough (1% to 5%), and angioedema.
ACEls

• Inhibit calcium movement into vascular
smooth muscle, thereby inhibiting
vasoconstriction.
• The
dihydropyridines
(nifedipine,
nicardipine, amlodipine, isradipine) are
most selective for arteriolar smooth
muscle, they are used most commonly
to treat hypertension.
CALCIUM CHANNEL BLOCKERS

• The most extensively used beta blocker
in pediatric experience is the prototype,
propranolol.
• However, its adverse effect profile is
substantial, and its lack of selectivity for
cardio- vascular receptors results in
problems with insulin resistance, and
altered lipid profiles.
BETA-ADRENERGIC
ANTAGONISTS

• Many pediatricians now use labetalol,
which also has significant alpha-
adrenergic blockade properties and,
therefore,
significant
synergistic
vasodilation.
• Adverse effects of all drugs in this class
include bradycardia, syncope, central
nervous system depression, and rarely,
hematologic problems.
BETA-ADRENERGIC
ANTAGONISTS

• Diuretics exert their antihypertensive
effects by promoting salt and water
excretion.
• They frequently are used as second- or
third-line medications and are especially
helpful in states characterized by fluid
retention.
• Diuretics should be considered the first
line of treatment for hypertension due to
acute
poststreptococcal
glomerulonephritis
.
DIURETICS

• These agents are extremely helpful
when rapid diuresis is necessary, and
they are effective in patients who have
renal insufficiency.
• Adverse effects include hypokalemic
alkalosis,
hypercalciuria
and
nephrocalcinosis,
and
ototoxicity,
especially when used concomitantly
with other ototoxic drugs.
DIURETICS
• The appropriate duration of treatment for a
child or adolescent is unknown. Some patients
require
lifelong
therapy;
others
may
experience improvement or even resolution of
their hypertension.
• For these reasons, if blood pressure is under
excellent control and no organ system damage
is present, medications can be tapered and
discontinued under careful observation.
• When patients have been weaned from
medication, they still should have their blood
pressure monitored routinely.
LENGTH OF THERAPY
Document Outline
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Slide 45
- Slide 46
- Slide 47
- Slide 48
- Slide 49
- Slide 50
- Slide 51
- Slide 52
- Slide 53
- Slide 54
- Slide 55
- Slide 56
- Slide 57
- Slide 58
- Slide 59
- Slide 60
- Slide 61
Wyszukiwarka
Podobne podstrony:
Alpay Self Concept and Self Esteem in Children and Adolescents
Immobilization and hypercalciuria in children
Variations in Risk and Treatment Factors Among Adolescents Engaging in Different Types of Deliberate
Stability and Change in Temperament During Adolescence
Immune function biomarkers in children exposed to lead and organochlorine compounds a cross sectiona
(Parenting) Anger and Aggression in Children Teaching Self Control
Ileal lymphoid nodular hyperplasia, non specific colitis, and pervasive developmental disorder in ch
Estimation of Dietary Pb and Cd Intake from Pb and Cd in blood and urine
automating with step 7 in lad and fbd simatic (1)
Key Concepts in Language and Linguistics
Guide to the properties and uses of detergents in biology and biochemistry
2008 4 JUL Emerging and Reemerging Viruses in Dogs and Cats
2002 3 MAY Lasers in Medicine and Surgery
In vivo MR spectroscopy in diagnosis and research of
Numerical methods in sci and eng
conceptual storage in bilinguals and its?fects on creativi
20090602 01 ANSF, Coalition Forces further disable IED?lls in Khowst and Zabul
więcej podobnych podstron