
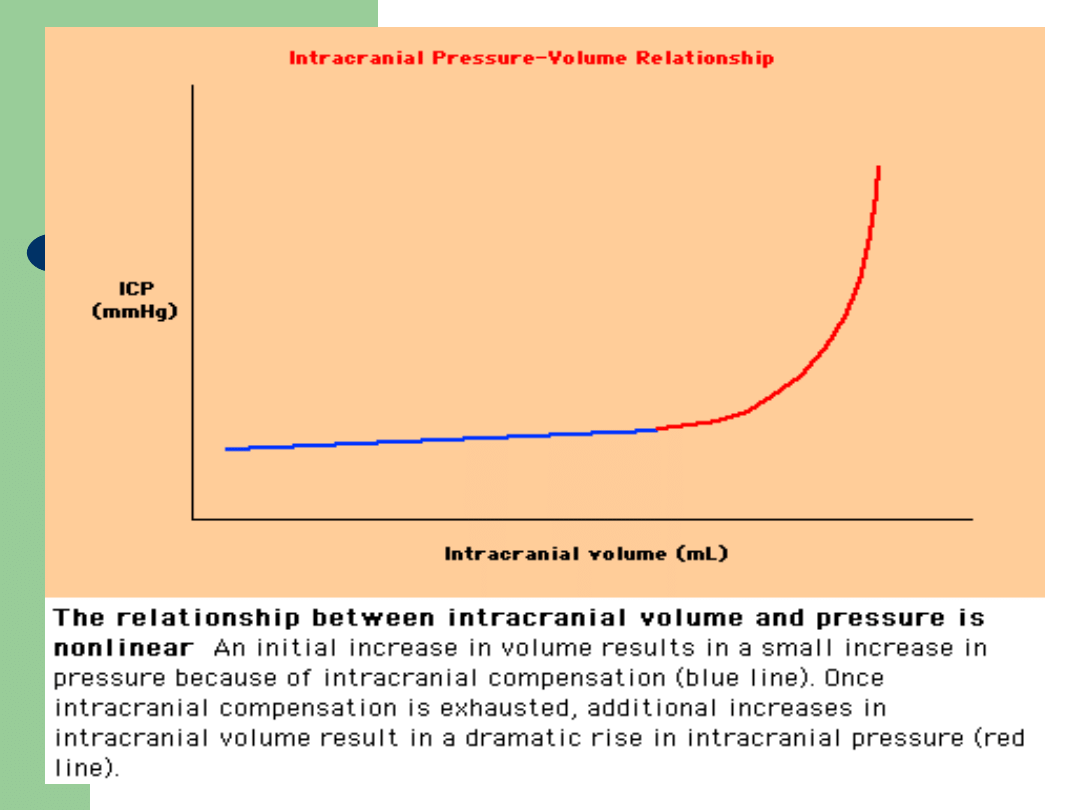
Monro-Kellie Doctrine
Cranial cavity is a rigid sphere
Filled to capacity with non compressible
contents
Increase in the volume of one of the
constituents will lead to a rise in
pressure

Contents
Brain – 80%
Blood – 10%
CSF – 10%
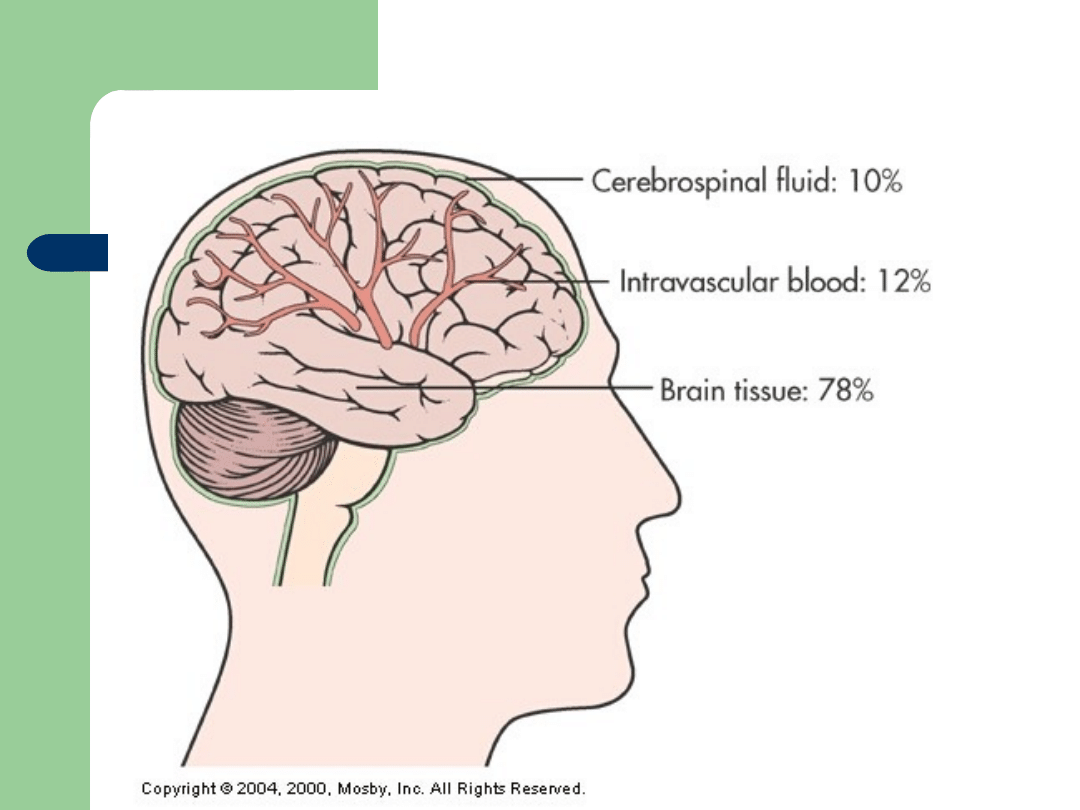
Components of the Brain
Components of the Brain
Fig. 55-
1

Intracranial Pressure
•
Normal ICP = 4 -15 mmHg
•
Factors that influence ICP
–
Arterial pressure
–
Venous pressure
–
Intraabdominal and intrathoracic pressure
–
Posture
–
Temperature
–
Blood gases (CO
2
levels)
Intracranial Pressure
Importance of ICP to BP and CPP
–
Brain needs constant supply O2 and Glucose
–
BP: heart delivers blood to brain at an average
BP of 120/80 (Mean BP = 100); this mean
arterial pressure (MAP) must be higher than
ICP
–
CPP (Cerebral Perfusion Pressure): is the
pressure needed to overcome ICP in order to
deliver O2 & nutrients

Intracranial Pressure
Importance of ICP to BP and CPP
–
MAP is the DRIVING FORCE
–
ICP is the RESISTENCE
–
CPP = MAP – ICP
= 100 mmHg – 15 mmHg
= 85 mmHg (Normal)
CPP < 50 mmHg→ cerebral ischemia
CPP < 30 mmHg → brain death

Intracranial Pressure:
Regulatory Mechanisms of
Cerebral Blood Flow
•
Autoregulation of cerebral blood
flow
•
Metabolic Regulation of cerebral
blood flow
Intracranial Pressure:
Regulatory Mechanisms of
Cerebral Blood Flow
•
Autoregulation
–
The automatic alteration in the
diameter of the cerebral blood
vessels to maintain a constant
blood flow to the brain
–
Maintains CPP regardless of
changes in BP

Intracranial Pressure:
Regulatory Mechanisms of
Cerebral Blood Flow
•
Problem: Autoregulation is limited
•
If BP and/or ICP rises:
Autoregulation fails
•
When autoregulation fails, blood
flow to brain increases or deceases
→ poor perfusion and cellular
ischemia or death
Intracranial Pressure:
Regulatory
Mechanisms
of
Cerebral Blood
Flow
•
Metabolic Regulation of
cerebral blood flow
Factors affecting cerebral blood
flow
–
PCO
2
–
PO
2
–
Acidosis

Cerebral Blood Flow
Cerebral Blood Flow
Blood supply matches metabolic
needs
Regulated:
- Mechanically – metabolic by-products
which alter blood vessel caliber
- By sensitivity to CO2 and O2
- By adenosine and oxygenases
- Perfusion pressure

Autoregulation
Autoregulation
CBF is regulated over a wide range of MAP
Range of 60-150 mmHg
Regulated by the tone of small arteries
and arterioles and by Blood Brain Barrier
(BBB)

Causes of raised ICP
Increased volume of normal contents
–
Brain: oedema, benign intracranial HTN
–
CSF: hydrocephalus
–
Blood: vasodilatation, venous thrombosis
Space occupying lesions
–
Tumour
–
Abscess
–
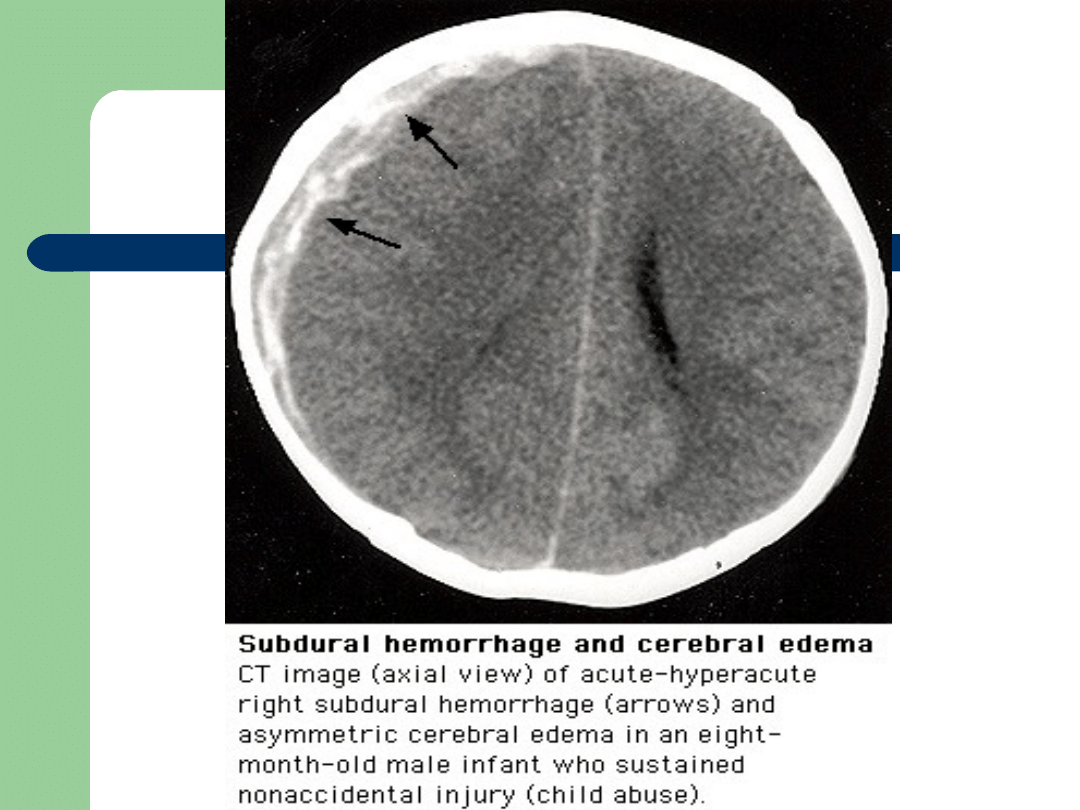
Intracranial heamorrhage

PATHOPHYSIOLOGY
PATHOPHYSIOLOGY
Primary injury
- parenchymal injury
Secondary injury
-
reaction of neural tissue to primary injury
edema
cell death

Pathophysiology
Pathophysiology
Cerebral Edema
increase in brain volume
increase in Na+ and H
2
O

Classification of
Classification of
Cerebral Edema
Cerebral Edema
Interstitial
Vasogenic
Cytotoxic

Interstitial Edema
Interstitial Edema
Increased CSF hydrostatic pressures
Altered absorption of CSF
Increased edema of periventricular white
matter due to CSF movement across
ventricles.
Prototype
- obstructive hydrocephalus

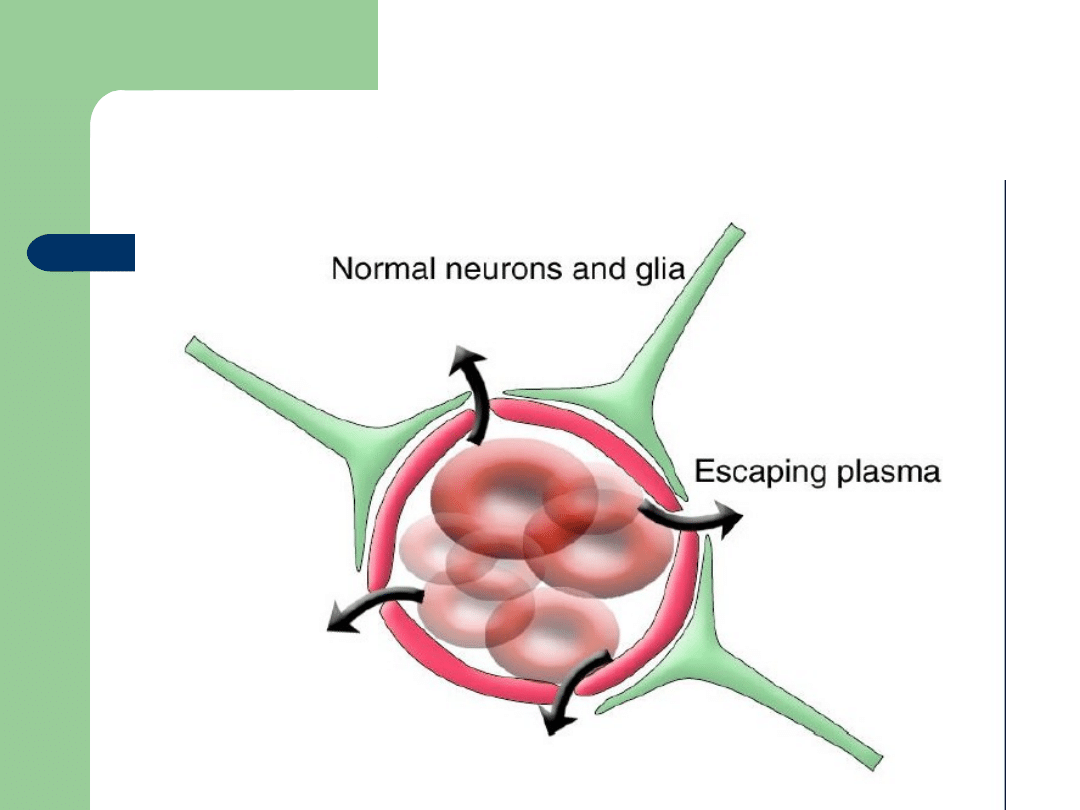
Vasogenic Edema
Vasogenic Edema
Increased permeability of brain capillary
endothelial cells to macromolecules.
Neurons are not primarily injured
Vasogenic
Edema

Vasogenic Edema
Vasogenic Edema
Tumor
Abscess
Hemorrhage
Contusion
Infarction
Meningitis
Lead encephalopathy

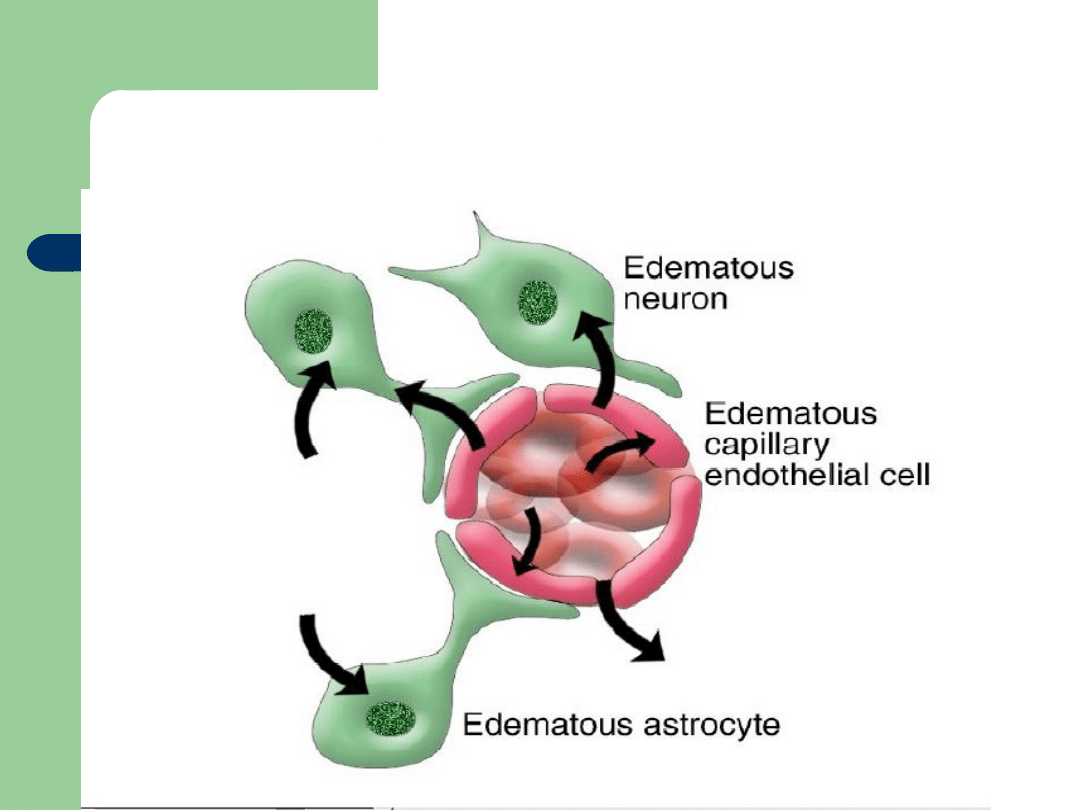
Cytotoxic Edema
Cytotoxic Edema
Cellular swelling due to cell injury
- neuronal, glial, and endothelial
Failure of ATPase dependant Na
exchange
Edema is a reflection of cell death rather
than a contributing factor
Cytotoxic Edema

Symptoms/signs
DROWSINESS
Headache
Nausea/vomiting
Papilloedema
Cushing’s triad
Altered mental status
Altered mental status
Cushing
Cushing
Reflex
Reflex
Bradycardia
Hypertension
Altered respiratory status
OFTEN A VERY LATE CLINICAL
FINDING!

Symptoms of
Symptoms of
Increased ICP
Increased ICP
Altered mental status
Neurological deficit
- common is 3rd or 6-th nerve palsy
- dilated pupil(s)
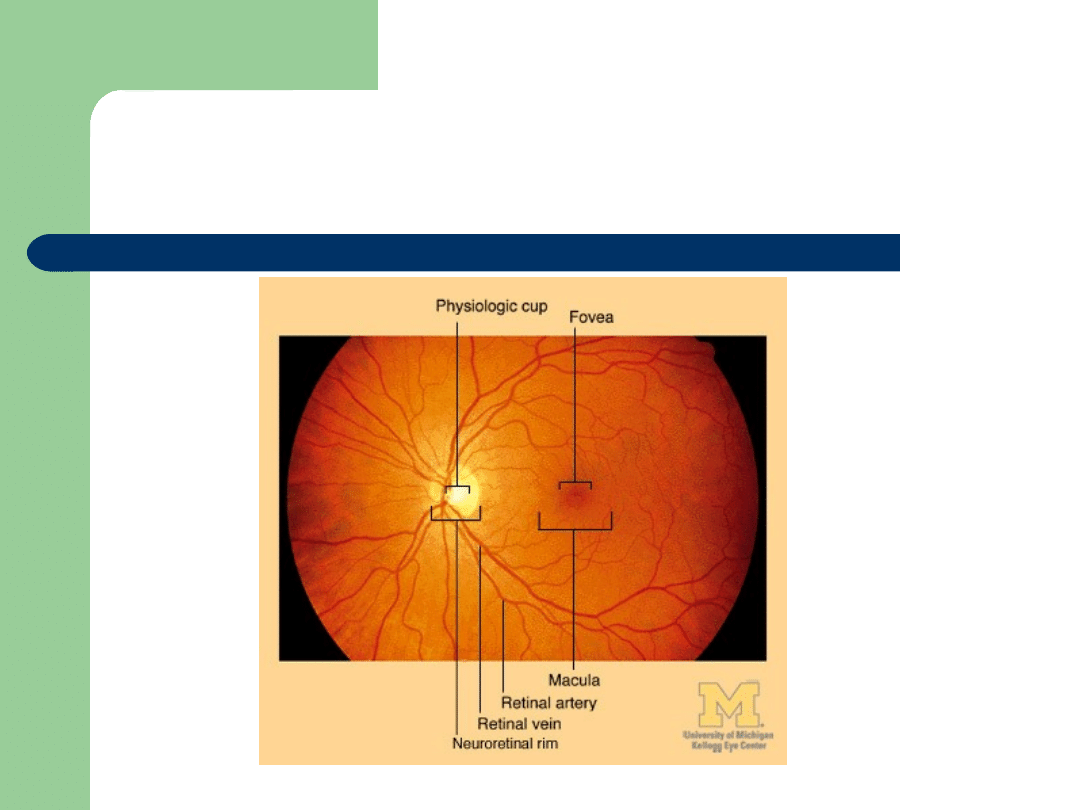
Normal fundus

Papilloedema

Factors That Worsen
Factors That Worsen
Secondary Injury
Secondary Injury
↓ BP
↓ PaO2
↑ PaCO2

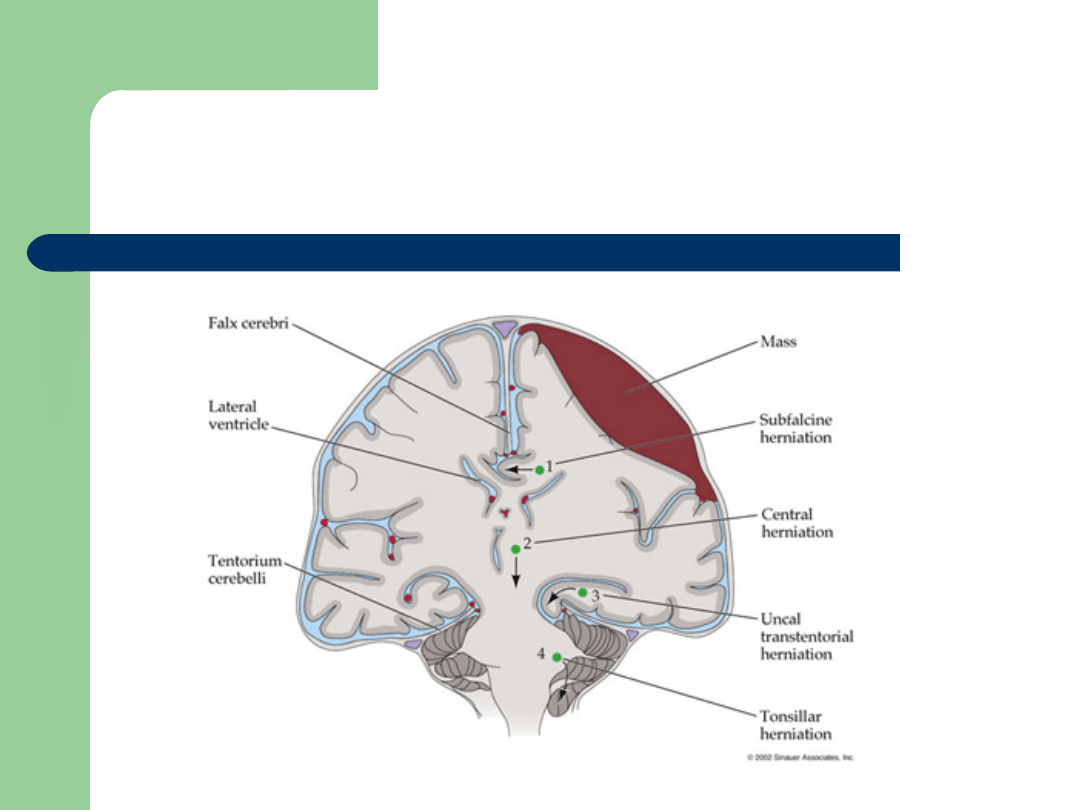
Cerebral herniation
Can occur depending on cause of raised
ICP
3 major types:
–
Transtentotial
–
Foramen magnum
–
subfalcine

Herniation
Herniation
Syndromes
Syndromes
Critically important herniation
Critically important herniation
syndromes:
syndromes:
Uncal Herniation
Uncal Herniation
:
:
-
-
occurs when a lateral expanding mass
occurs when a lateral expanding mass
lesions pushes the uncus and hippocampal
lesions pushes the uncus and hippocampal
gyrus over the lateral edge of the tentorium
gyrus over the lateral edge of the tentorium
- Unilateral dilated pupil
- Unilateral dilated pupil
progresses to
progresses to
brain stem dysfunction
brain stem dysfunction

Transtentorial
Displacement of brain and herniation of
uncus of temporal lobe through the
tentorial hiatus
Causes compression of:
–
midbrain : contralateral hemiparesis
(usually), Cushing response, , respiratory
failure (cheyne-stokes)
–
CN III: dilatation of ipsilateral pupil initially
–
Posterior cerebral artery: hemianopia

Foramen magnum (coning)
Progressively increasing ICP causes further
downward herniation of the cerebellar tonsils
into foramen magnum or coning.
With progressive herniation pupils change
from dilated and fixed to midsize and
unreactive.
Signifying irreversible events leading to
brainstem death.

Subfalcine
Cingulate gyrus herniates under falx.
Usually asymptomatic unless ACA kinks
and occludes causing bifrontal
infarction.

ICP monitoring
Indications:
–
Head injury
–
Following major intracranial surgery
–
Assessment of benign intracranial HTN
Normal ICP: 10-15mmHg
Can be recorded from ventricle, brain
substance, subdural or extradural space
Risks: CNS infection and intracranial
haemorrhage

INCREASED ICP
INCREASED ICP
General Care
General Care
HOB elevated 30°
↑
venous drainage
Head midline
↑
venous drainage
No jugular catheters
prevent venous obstruction
Normothermia
avoid
↑
metabolism
↓ Pleural pressures (zero peep)
↑
venous
drainage

Management
Definitive treatment: treat underlying patholgy
To control raised ICP:
1.
Head elevation
2.
Controlled ventilation: maintain PaCO2 at 30-35 mmHg.
Reduction of CO2 will reduce cerebral vasodilatation
3.
Sedation/paralysis: decrease metabolic demand
4.
If ventricular catheter in situ, drain CSF
5.
Diuretic therapy: mannitol – osmotic diuretic, increases
serum osm and draws water out of the brain. Usual dose:
0.5-1.0g/kg. monitor serum osm
6.
Hypertonic saline
7.
Barbiturate therapy: thiopentone when given as a bolus
dose can be helpful in temporarily reducing ICP.

Manipulation of
Manipulation of
ICP
ICP
Brain
Brain
Mannitol
- dehydrates the brain, not the
patient
- monitor osmolality
Hypertonic saline

Manipulation of ICP
Manipulation of ICP
Blood
Blood
Decrease cerebral metabolic demands
- sedation, analgesia, barbiturates
- avoid hyperthermia
- avoid seizures
Hyperventilation
-
decreases blood flow to the brain
- only acutely for impending Herniation.
Mannitol
Document Outline
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
Wyszukiwarka
Podobne podstrony:
Prolonged intracranial pressure (ICP) monitoring
Prolonged intracranial pressure (ICP) monitoring
Blood Pressure in Intracerebral Hemorrhage
Pressure%20Cem[1]
2 7T Pressure Tester
How to build a Raised Formal Pool
68 979 990 Increasing of Lifetime of Aluminium and Magnesium Pressure Die Casting Moulds by Arc Ion
Atmospheric pressure
Pressure Points Chest
Pressure Points Legs
Finished drawing for air reservoir,pressure tank,calorifer
Capability of high pressure cooling in the turning of surface hardened piston rods
AllRoadFAQ com Audi C5 2 7T PressureLeakTesting
manometry Pressure id 764199 Nieznany
Pressure Points Head
13 161 172 Investigation of Soldiering Reaction in Magnesium High Pressure Die Casting Dies
flow and pressure
24 Intractable Pain
więcej podobnych podstron