Prof Eugene Schif
Diagnosis and Management
of Hepatitis at the Frontline
Chronic Hepatitis B
Patient Evaluation
and Clinical
Management
Prof Eugene R. Schif, M.D.
University of Miami, Florida,
USA

•
Incubation period:
Average 60–90
days
Range 45–180
days
•
Clinical illness (jaundice):
<5 yrs, <10%
>5 yrs, 30%–50%
•
Acute case-fatality rate: 0.5%–1%
•
Chronic infection:
<5 yrs, 30%–90%
>5 yrs, 2%–10%
•
Premature mortality from
chronic liver disease:
15%–25%
Hepatitis B – Clinical Features
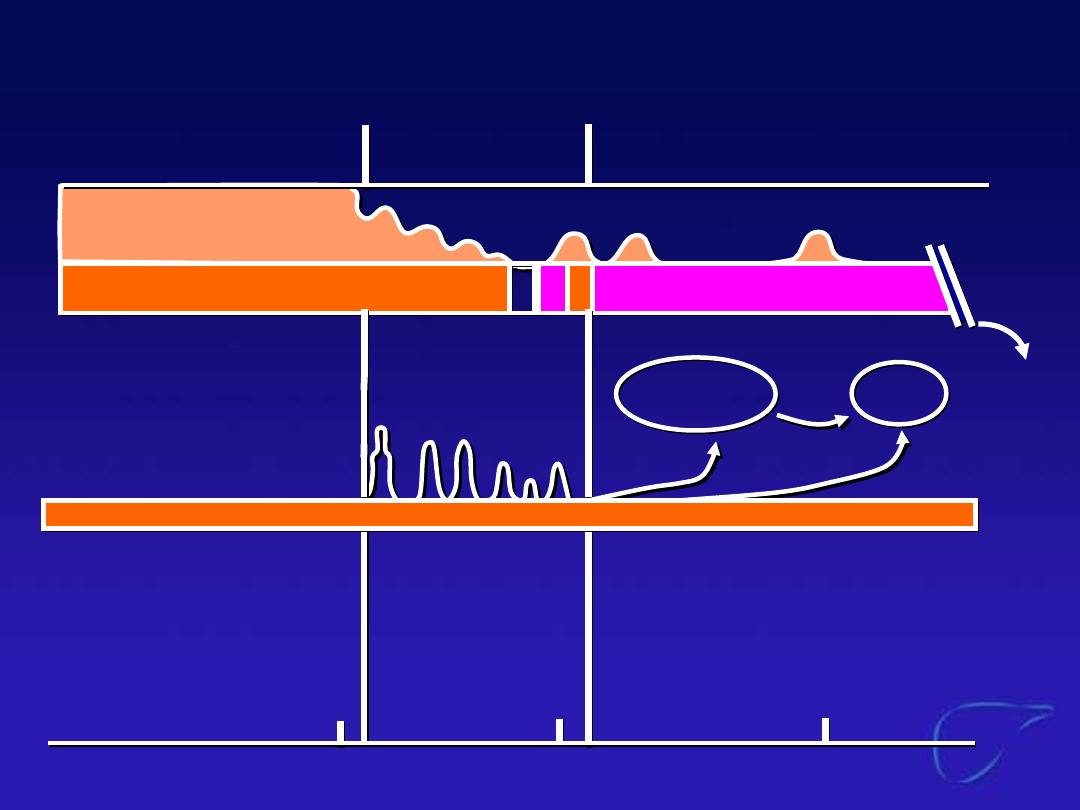
Natural Course of CHB
HBeAg
Nuclear
Cytoplasm (++ ~)
(-)
(+++)
Membrane (++ ~)
HBsAg/preS
Membrane Cytoplasm (++ ~)
Cytoplasm (+++)
(+++)
Membrane (++ ~)
HLA-1
(-)
(++)
(++)
HBeAg
Nuclear
Cytoplasm (++ ~)
(-)
(+++)
Membrane (++ ~)
HBsAg/preS
Membrane Cytoplasm (++ ~)
Cytoplasm (+++)
(+++)
Membrane (++ ~)
HLA-1
(-)
(++)
(++)
Phase
Phase
Immune
Tolerance
Immune
Tolerance
Immune
Clearance
Immune
Clearance
Late/Residual
Late/Residual
Reactivation
Reactivation
Pre-C mutant
Pre-C mutant
HBV-DNA
HBV-DNA
HBeAg(+)
HBeAg(+)
anti-HBe(+)
anti-HBe(+)
HBsAg
Clearance
HBsAg
Clearance
ALT/Grading
ALT/Grading
HCC
HCC
Cirrhosis
Cirrhosis
20
20
40
40
60
60
Age
Age

Natural History of Chronic
Hepatitis B
•
Ranges from mild infection
(asymptomatic) to more severe chronic
liver disease
•
Fibrosis and subsequent cirrhosis
•
Liver failure
•
Hepatocellular carcinoma
•
Mortality
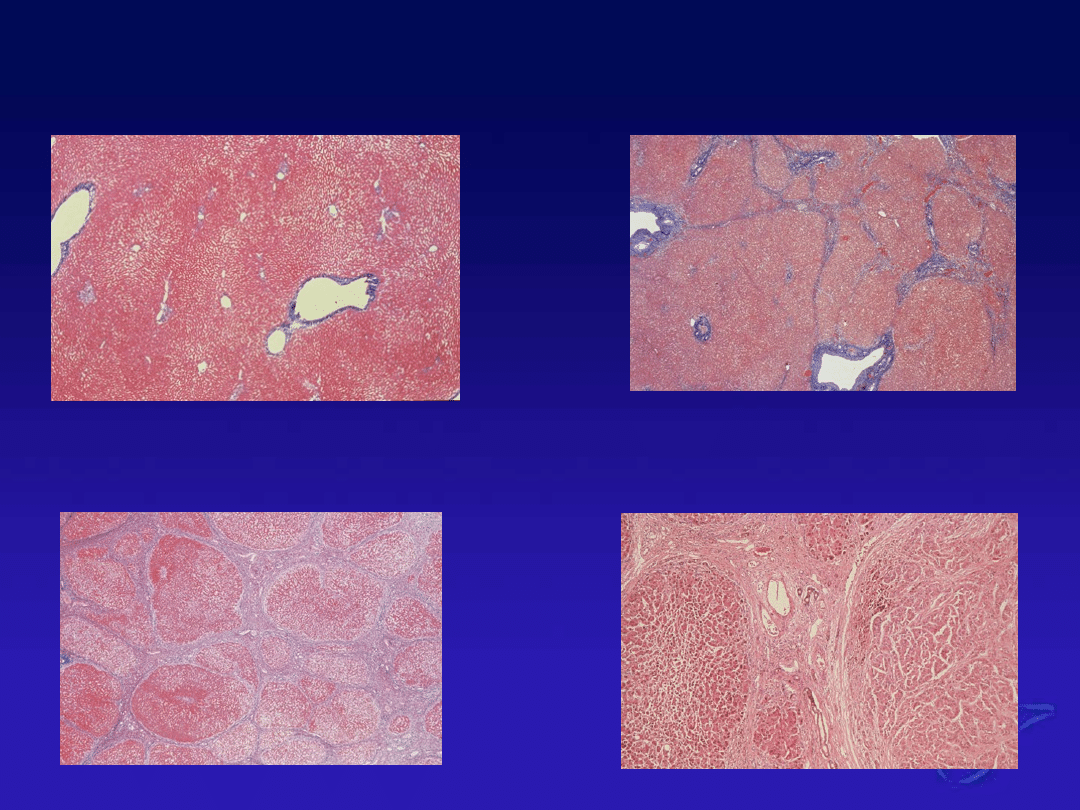
Healthy Liver
Liver Fibrosis
Cirrhosis
Liver Cancer
Natural History of Chronic HBV
Infection
Acute
Infection
Chronic
Chronic
Carrier
Carrier
Resolution
Resolution
30–50 Years
Chronic
Hepatitis
Stabilisatio
Stabilisatio
n
n
Progression
Progression
Cirrhosis
Compensated
Compensated
Cirrhosis
Cirrhosis
Liver
Cancer
Deat
h
Adapted from Feitelson, Lab Invest 1994
Decompensated
Decompensated
Cirrhosis
Cirrhosis
(Death)
(Death)

Chronic Hepatitis B: Definition
•
HBsAg+ for >6 months
•
Variable clinical course
•
Morbidity and mortality from chronic
necroinflammatory disease in liver
•
Disease progression is associated with
persistently high HBV replication

Predictors of Progression in
Chronic Hepatitis B
•
Bridging necrosis on liver biopsy
•
Persistence of HBeAg
•
Persistence of HBV DNA and elevated ALT
after HBeAg seroconversion (pre-core
mutation with HBeAg-negative CHB)

Predictors of Improved
Outcome in Chronic HBV
•
Loss of HBeAg
•
Associated with decreased viral replication
•
Improved survival
•
Persistently positive HBV DNA predicts pre-
core mutation and persistent chronic
hepatitis
•
Normalisation of ALT predicts better survival
•
Shorter duration of disease (age) predicts
survival
•
Extent of histologically-assessed liver damage
is also a predictor of survival

•
Mild
Raised ALT and/or AST only
•
More severe
Raised ALT/AST and raised
bilirubin
•
Severe, impending liver failure
Reduced albumin
Prolonged prothrombin time
Assessing Severity of Liver
Disease in Hepatitis B

Management of Chronic
Hepatitis B
•
Suppression of viral replication
•
Improvement in hepatic
necroinflammatory
disease
•
Reduction in long-term sequelae of
HBV-associated liver disease (cirrhosis,
hepatocellular carcinoma)
Goals of patient management
Antibodies to the
virus
•
Anti-HBc
•
Anti-HBe
•
Anti-HBs
Severity of liver
damage
•
Bilirubin
•
Albumin
•
Prothrombin time
Markers of the virus
•
HBV DNA
•
HBeAg
•
HBsAg
Markers of liver damage
•
ALT
•
AST
•
Bilirubin
Hepatitis B – Diagnostic
Tools
Never Been Exposed to Hepatitis
B
No viral markers
•
HBsAg
-
•
HBeAg
-
•
HBV DNA -
No immune
response to the
virus
•
Anti-HBc -
•
Anti-HBs -
•
Anti-HBe -
Sensitivity of HBV DNA Assays
Test
Method
Range of quantification
Dot blot
Rapid test
Abbott
Liquid hybridisation
Digene
RNA-DNA hybrid
Chiron
Branched DNA
Amplicor
Quantitative PCR
Monitor
10
6
10
5
10
3
10
2
10
4

Value of Serum HBV DNA
Assessment
•
Prognosis
•
Identification of viraemia irrespective of
HBeAg status
•
Therapy selection
•
Monitoring
–
Virological response to therapy
–
Disease progression
–
HBV replication after liver
transplantation
Acute Hepatitis
B
Full complement of
viral markers, all
present for
< 6 months
•
HBsAg
+
•
HBeAg
+
•
HBV DNA +
Some immune
response to the virus
•
Anti-HBc +
•
Anti-HBs -
•
Anti-HBe -
Evidence of acute
infection
•
Anti-HBc IgM
+
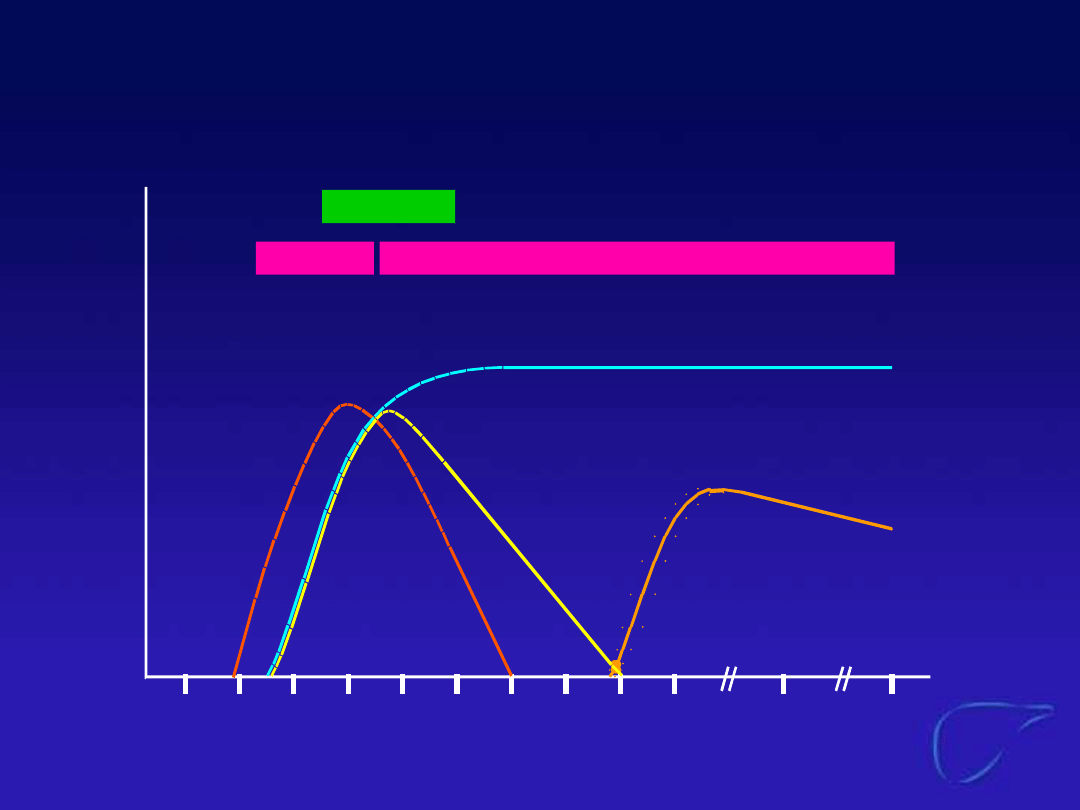
Acute Hepatitis B Virus Infection
with Recovery Typical Serologic
Course
Weeks after
exposure
Titer
Symptom
s
HBeAg
anti-HBe
Total anti-HBc
IgM anti-HBc
anti-HBs
HBsAg
0
4
8 12 16 20 24 28 32 36
52
100
Chronic Hepatitis B with
Evidence
of Viral Replication
Full complement of
viral markers, all
present for
>6 months
•
HBsAg
+
•
HBeAg
+
•
HBV DNA +
Some immune
response to the
virus
•
Anti-HBc +
•
Anti-HBs -
•
Anti-HBe -
No evidence of acute
infection
•
Anti-HBc IgM
-
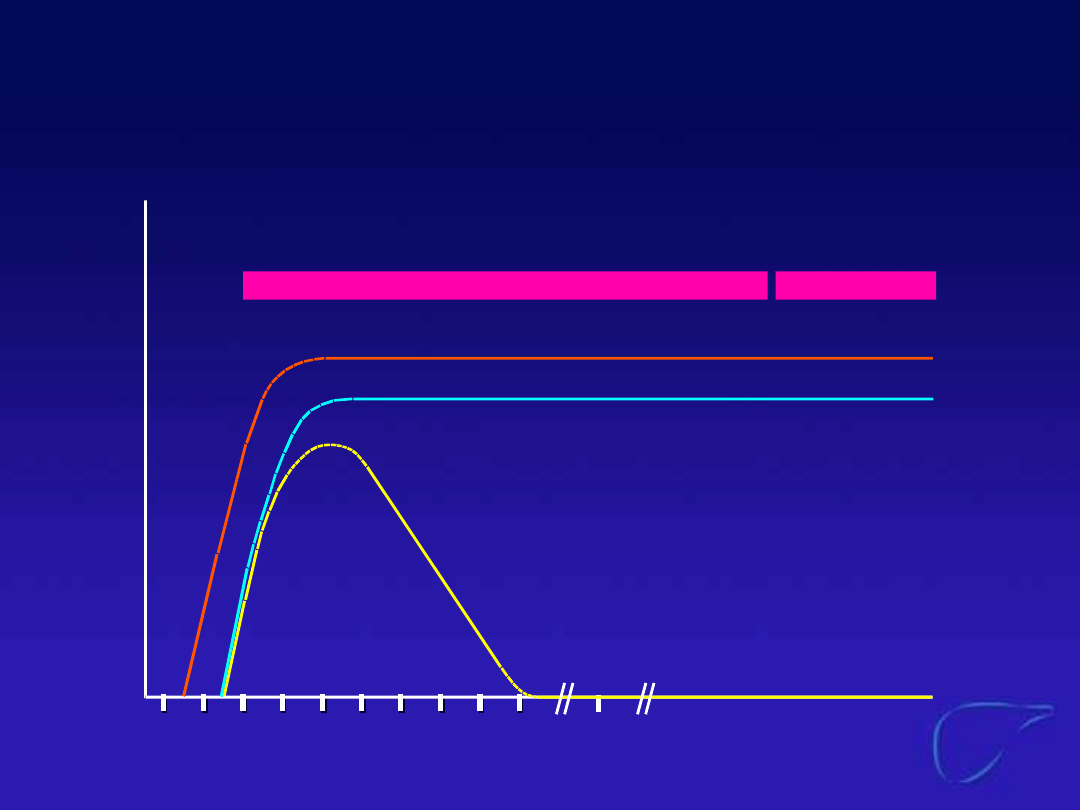
Weeks after exposure
Titer
IgM anti-
HBc
Total anti-
HBc
HBsAg
Acute
(6
months)
HBeAg
Chronic
(years)
anti-HBe
0 4 8 12 16 20 24 28 32 36
52
Years
Progression to Chronic Hepatitis
B Virus Infection Typical
Serologic Course
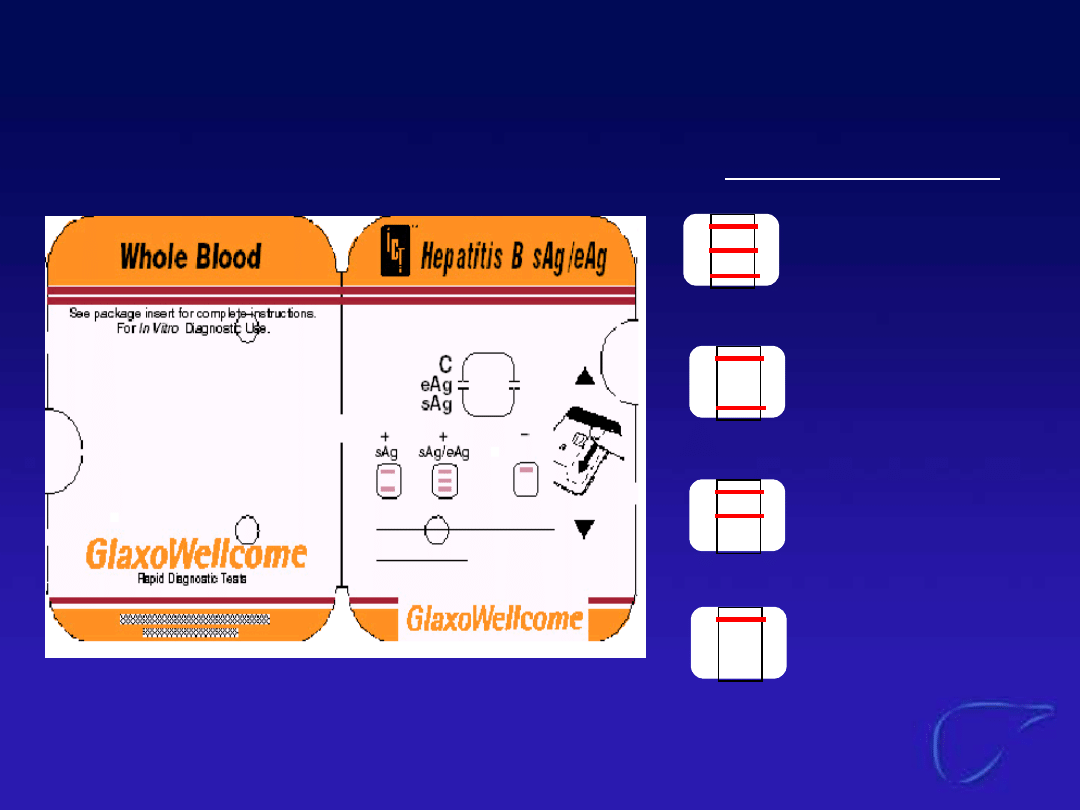
Amrad Rapid Test
sAg/eAg positive
sAg positive
eAg positive
-ve
Test results

How to Monitor?
•
During therapy: ALT, HBeAg and or HBV-
DNA every 3 months
•
After therapy: ALT, HBeAg and or HBV-
DNA every 6 months

Possible Causes of ALT Rises
During Lamivudine Therapy
Hepatitis related
•
HBeAg seroconversion
•
Fluctuations in disease activity
Treatment related
•
Non compliance with medication
•
Emergence of YMDD variant HBV
Concomitant disease
•
Alcoholism
•
HAV, HCV infection
•
NASH

Does Emergence of YMDD
Variants Lead to Serum ALT
Elevations?
•
Reappearance of HBV (wild-type or
YMDD variant) may lead to a rise in
serum ALT which is usually
temporary and asymptomatic
•
Serum ALT rises accompanied by
evidence of hepatic decompensation
are rare
Serum ALT Elevations During
Treatment for 3 Years
Definition
LAM 100 mg (n=58)
n
%
2 x baseline ALT
22*
38
3 x baseline ALT
14
24
2 x baseline ALT & >500 ALT (U/L)
6
10
2 x baseline ALT & >2 x ULN Bil &
2 x baseline Bil
2
3
Leung et al., 1999
* 4 patients HBeAg-ve, HBeAb+ve and DNA-ve
6 patients HBeAg-ve, HBeAb+ve and DNA+ve
Management Options for Patients
with YMDD Variant and
Loss of Clinical Efficacy
0
10
20
30
40
50
60
70
80
Continue
Stop
Add
%
Survey of 110 European doctors, Vienna, March 2001
•
Continue lamivudine treatment
•
Stop lamivudine treatment
•
Additional antiviral agent - adefovir,
IFN

•
HBeAg seroconversion can still occur
•
Suppression of the wild-type virus is
maintained
•
Improvements in serum ALT and HBV DNA
are maintained in most patients
•
Histological improvement can be obtained
•
No significant increase in adverse events
Benefits of Continued Lamivudine
Therapy in Patients with
YMDD Variant CHB

Conclusions
•
In endemic areas, it is particularly important
for physicians to screen for HBV infection so
that treatment can be initiated before
advanced disease develops
•
An understanding of the serological
parameters of HBV and ALT elevations is
important in the management of
hepatitis B patients
•
Eradication of hepatitis B will come with
universal vaccination
Document Outline
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
Wyszukiwarka
Podobne podstrony:
Diagnosis and Management of Hemochromatosis
Diagnosis and Management of the Painful Shoulder Part 1 Clinical Anatomy and Pathomechanics
Epidemiology and Prevention of Viral Hepatitis A to E
Introduction Blocking stock in warehouse management and the management of ATP
PSYCHIC METHODS OF DIAGNOSIS AND TREATMENT IN ACUPUNCTURE …
Can we accelerate the improvement of energy efficiency in aircraft systems 2010 Energy Conversion an
An Assessment of the Efficacy and Safety of CROSS Technique with 100% TCA in the Management of Ice P
Osteoporosis ľ diagnosis and treatment
05 DFC 4 1 Sequence and Interation of Key QMS Processes Rev 3 1 03
więcej podobnych podstron