
Cardivascular problems in
the neonates
Iwona Maroszyńska
Polish Mother’s Health Centre

• Fetal circulation
• Congenital cardiac defect
– Critical heart malformation
• TGA
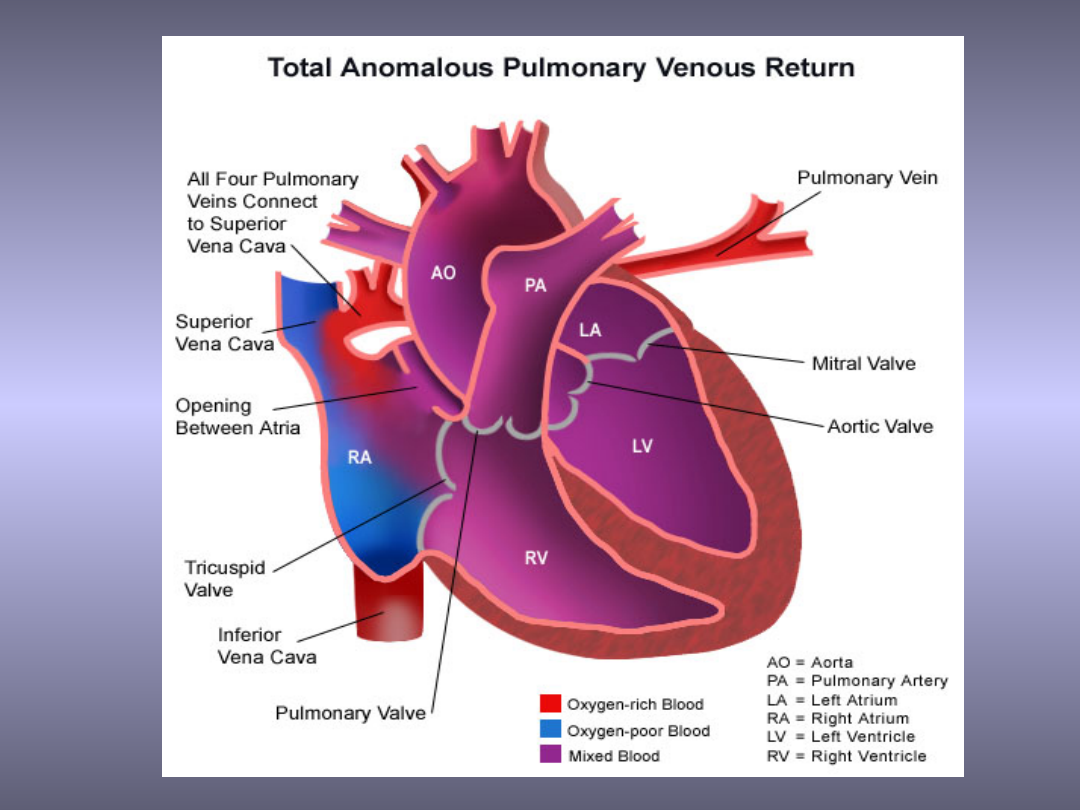
• TAPVR
• TA, PA, PS
• AS, CoA
– Treatment
• Prostaglandins
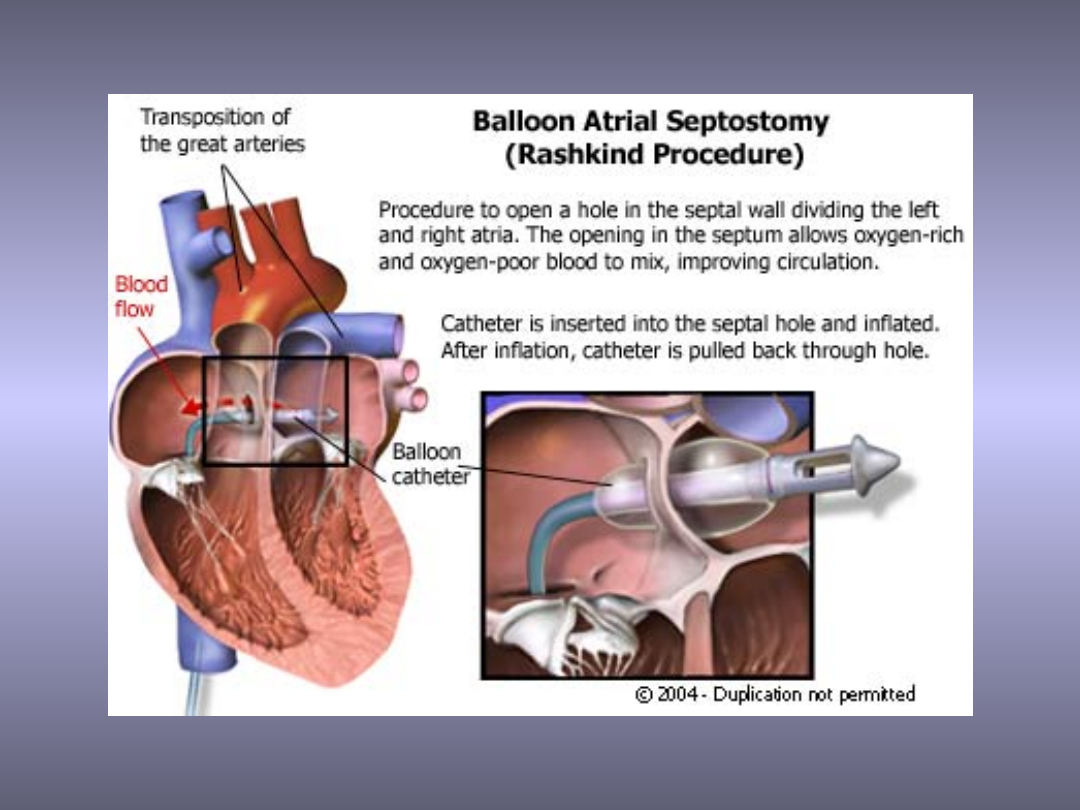
• Rashkind procedure
• Congestive heart failure

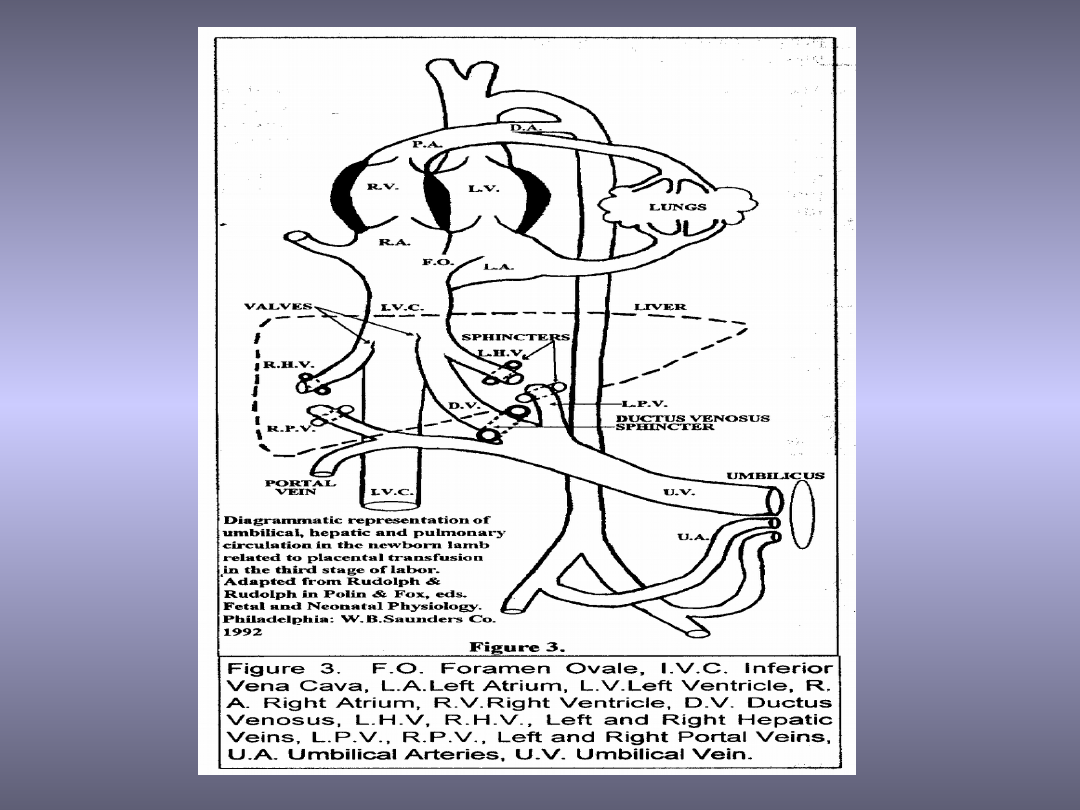
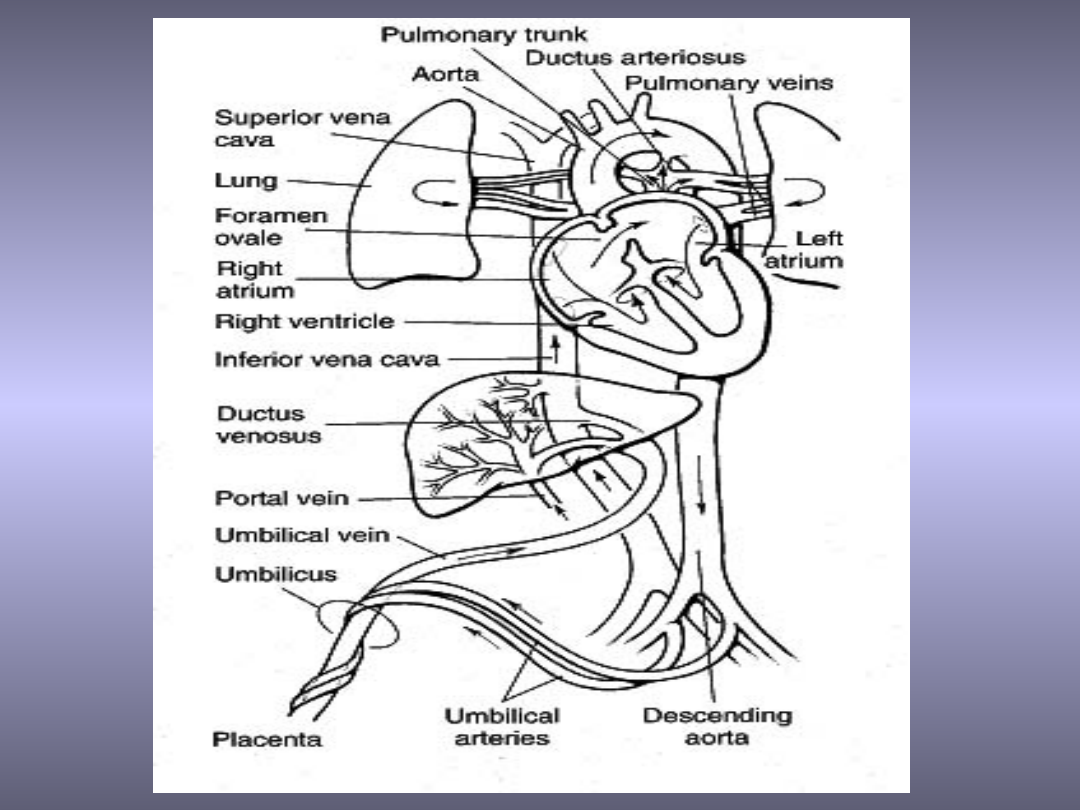
Fetal circulation
The fetus is connected by the umbilical cord to
the placenta, the organ that develops and
implants in the mother's uterus during pregnancy
Through the blood vessels in the umbilical cord,
the fetus receives all the necessary nutrition,
oxygen, and life support from the mother
Waste products and carbon dioxide from the fetus
are sent back through the umbilical cord and
placenta to the mother's circulation to be
eliminated
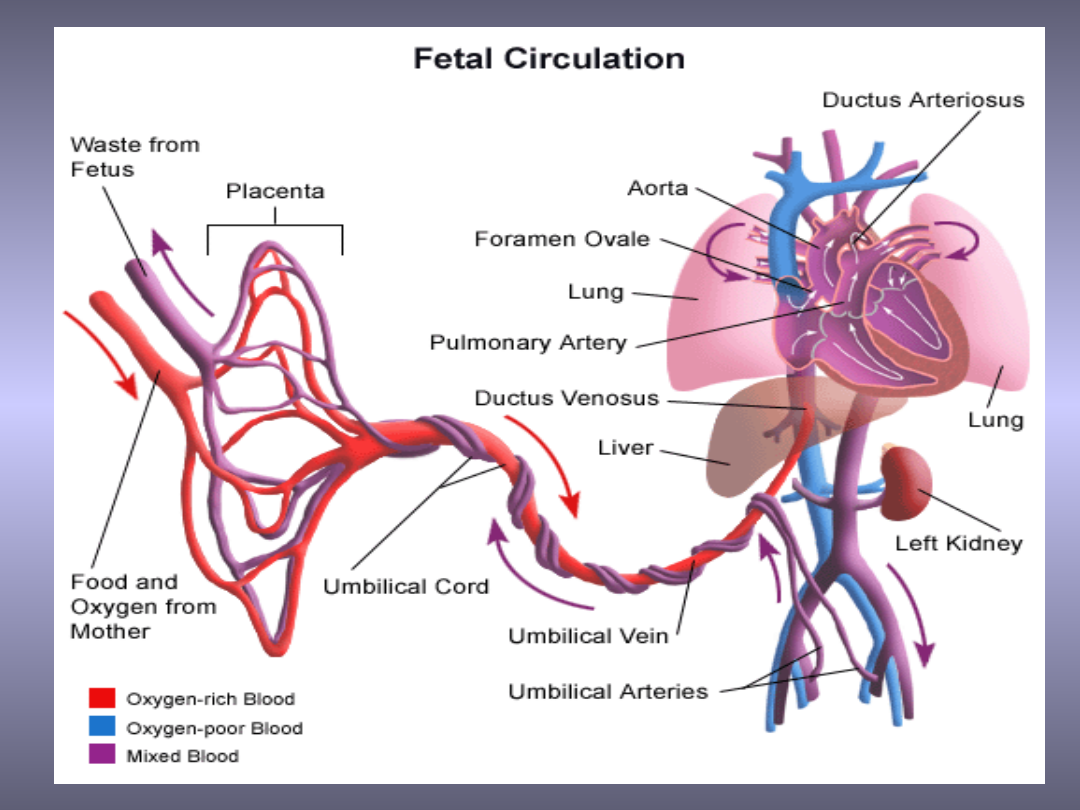

Fetal circulation
• Blood from the mother enters the
fetus through the vein in the
umbilical cord. It goes to the liver
and splits into three branches. The
blood then reaches the inferior
vena cava

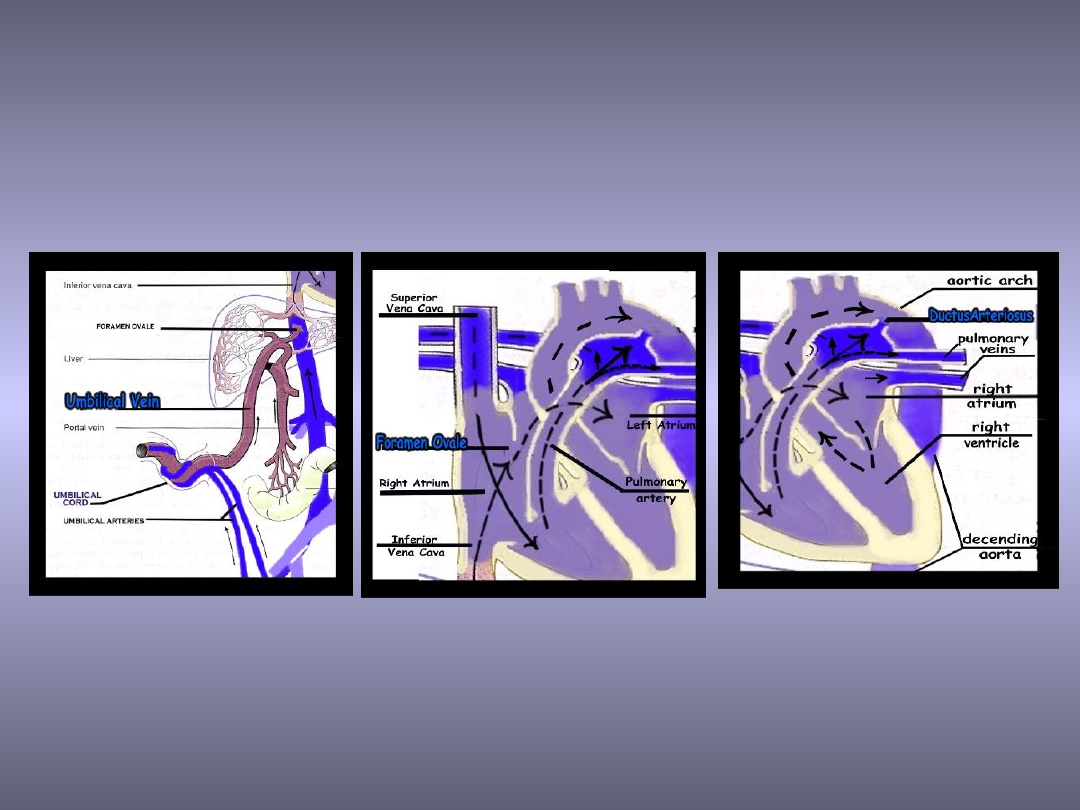
Inside the fetal heart:
Blood enters the right atrium. Most of the blood
flows to the left side through a special fetal opening
between the left and right atria - foramen ovale
Blood then passes into the left ventricle and then to
the aorta
From the aorta, blood is sent to the head and upper
extremities
After circulating there, the blood returns to the right
atrium of the heart through the superior vena cava
About one-third of the blood entering the right
atrium does not flow through the foramen ovale,
but, instead, stays in the right side of the heart,
eventually flowing into the pulmonary artery

Fetal circulation
• Because the placenta does the work of
exchanging oxygen (O2) and carbon dioxide
(CO2) through the mother's circulation, the
fetal lungs are not used for breathing. Instead
of blood flowing to the lungs to pick up oxygen
and then flowing to the rest of the body, the
fetal circulation shunts (bypasses) most of the
blood away from the lungs through a
connecting blood vessel called the ductus
arteriosus

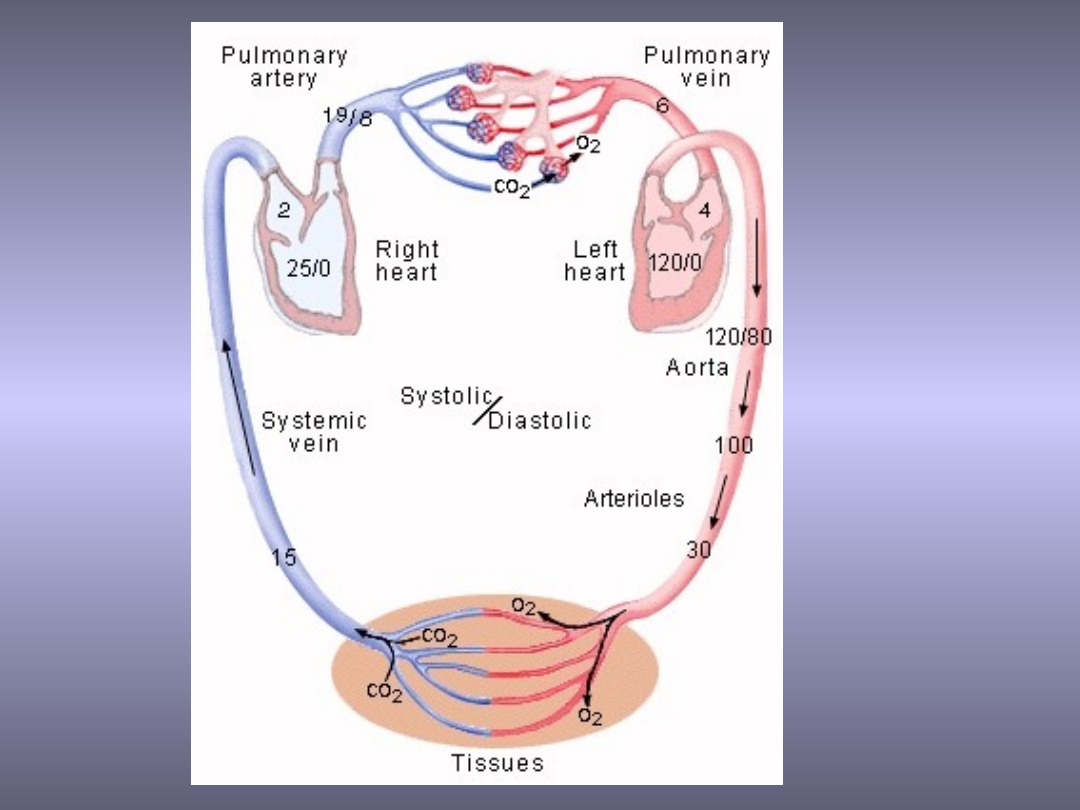
Fetal circulation
• Dependent on the mother’s circulation
• Gas exchange take place in the placenta
• Blood oxygenation
– Umbilical vein > Vena cava superior > Left
atrium > Left ventricle > Ascendens aorta (PaO2
20-22 mmHg, SaO2-90-95%) > Descendens
aorta (PaO2 16-18mmHg, SaO2-75-80%)
• Lung - extraction of the oxygen from the blood,
fluid production

Fetal circulation
• Low systemic vascular resistance because
of the placenta (low perfusion pressure,
high flow)
• High pulmonary vascular resistance
• Intracardiac and extracardiac bypass
system
• Tissue perfusion is determined by the local
vascular resistance
• Preload: RV > LV
• Afterload: RV > LV
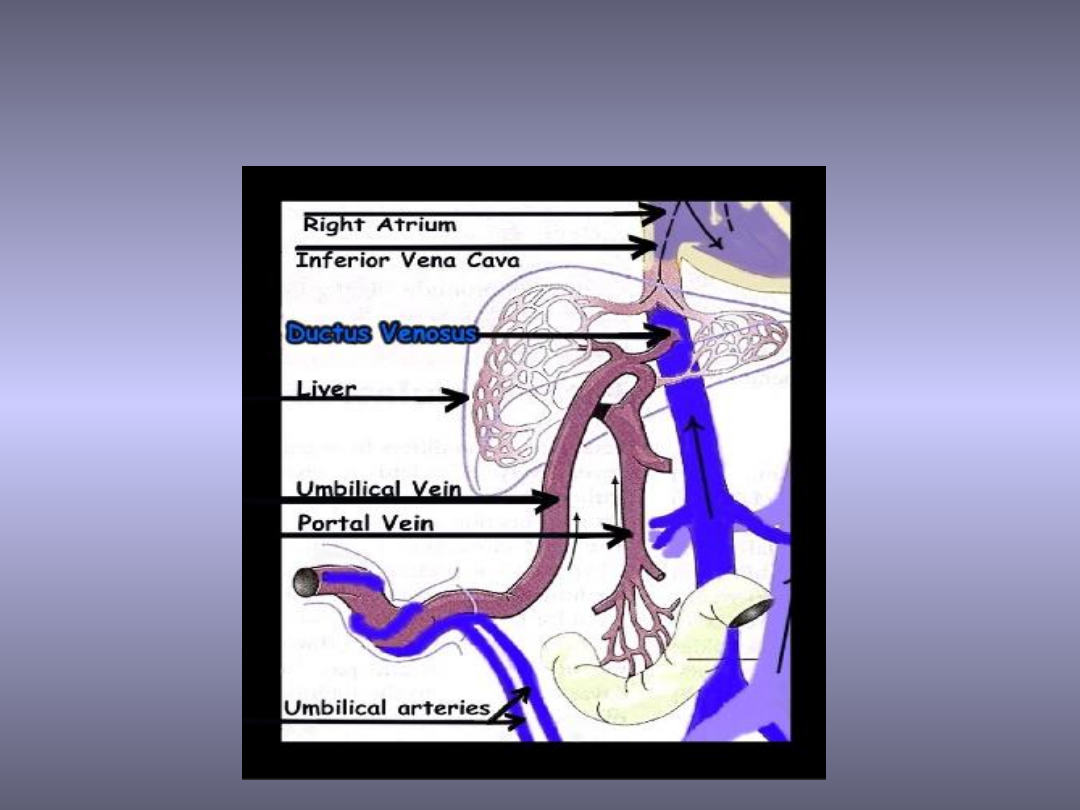
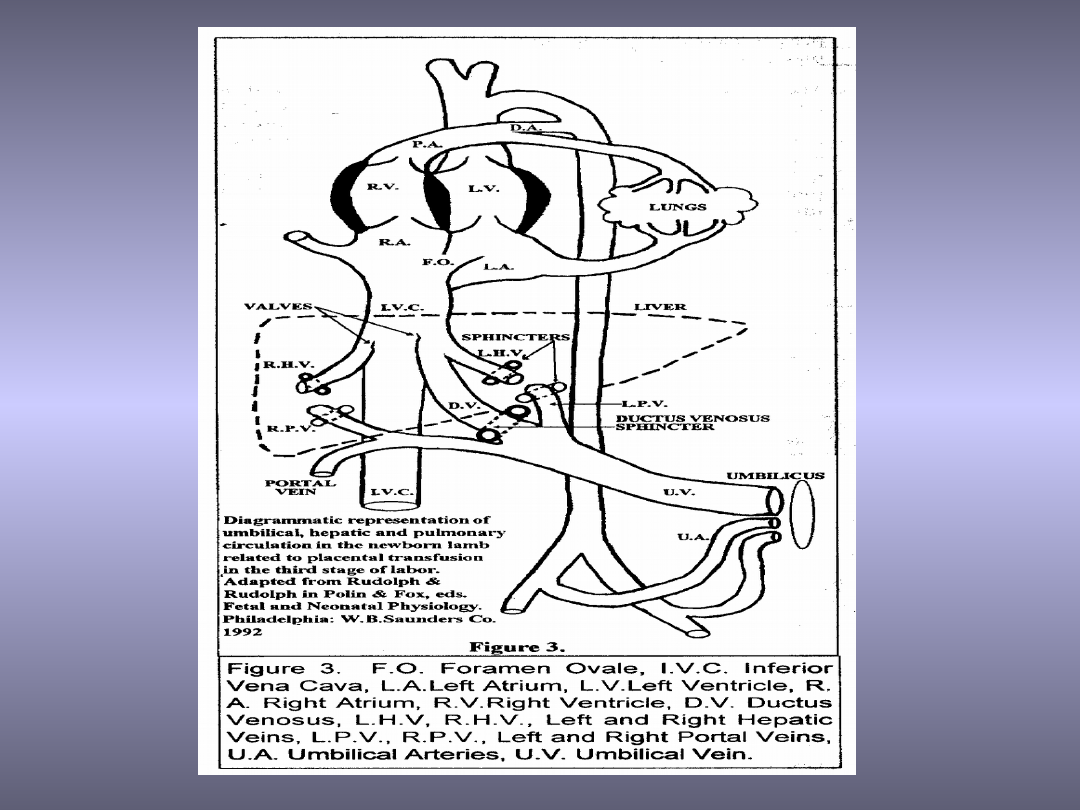
Liver – the first organ that receives
oxygenated blood
The mixing of the oxygenated i
deoxygenated blood

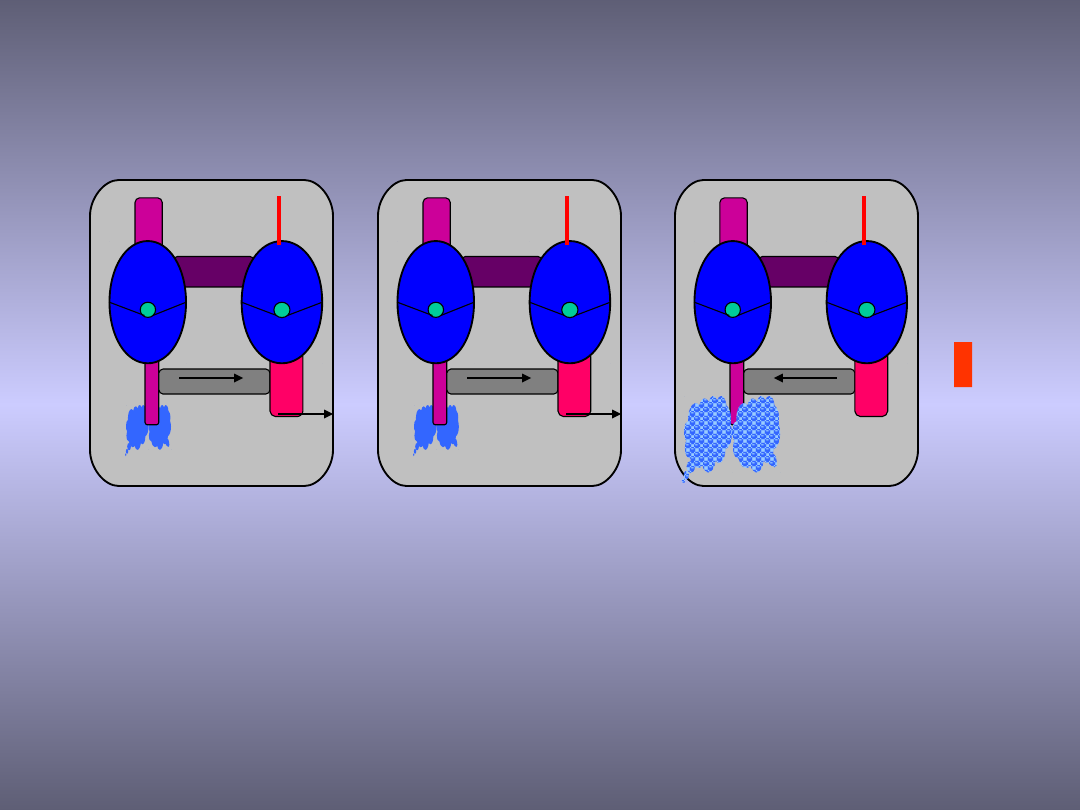
Blood circulation after
birth:
• With the first breaths of air the baby takes at
birth, the fetal circulation changes. A larger
amount of blood is sent to the lungs to pick up
oxygen
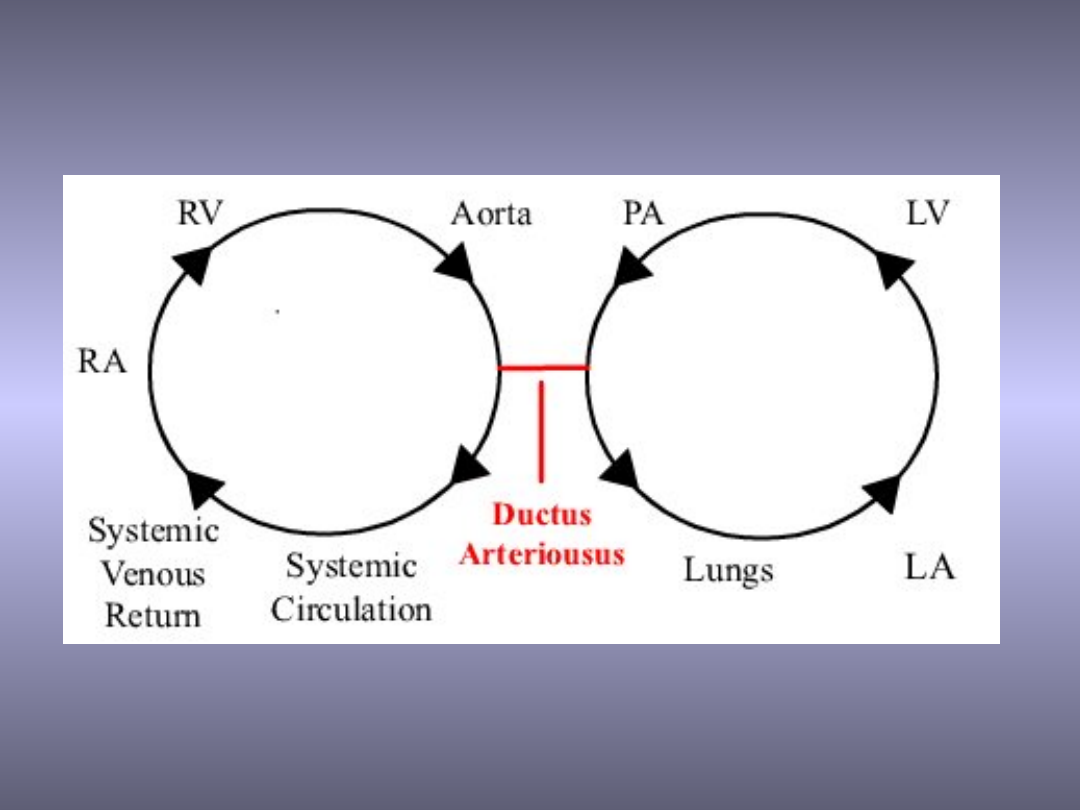
Because the ductus arteriosus (the normal
connection between the aorta and the
pulmonary arteria) is no longer needed, it
begins to wither and close of
The circulation in the lungs increases and more
blood flows into the left atrium of the heart.
This increased pressure causes the foramen
ovale to close and blood circulates normally
PDA
40%
50%
40%
90%
10%
FO
10%
90%
50%
PDA
40%
40%
20%
80%
20%
FO
20%
80%
60%
PDA
120%
0%
100%
120%
FO
100%
100%
20%
120%
20 t.c.
38 t.c.
Postnat.

Catecholamines
• Contraction of the uterus
– Hypoxia
– Increased cardiac output
• Stimulation of the new-born baby
• Increase of the systemic vascular
resistance
• Preparing the lungs to the breathing

Newborn’s circulation
• Afterload of the left ventricle
50%
• Afterload of the right ventricle
Replacement of placenta by the lungs
Katecholamines
Decreased pulmonary vascular
resistance
Newborn’s circulation
• Preload of the left ventricle
• Preload of the right ventricle
75%
Increased venous return
Constans
Parturition
• Right ventricle
• Left ventricle

Newborn’s circulation
• CO double than that of the adult as
measured against unit of body weight
– Elevation of stroke volume
– Higher heart rate
• Fetal myocardium works at near peak
capacity (catecholamines realising)
– Maintaining of a greater passive tension
– Developing of a smaller active tension

Newborn’s circulation
• Reduced shortening velocity
– Larger ratio of non-contractile to contractile
components in the fetal myocardium
– Lower content of intercellular calcium
• Incomplete sympathetic innervation
– The reduced number of sympathetic nerves
fibres compares with normal numbers of
receptors
– Supersensitivity to catecholamines
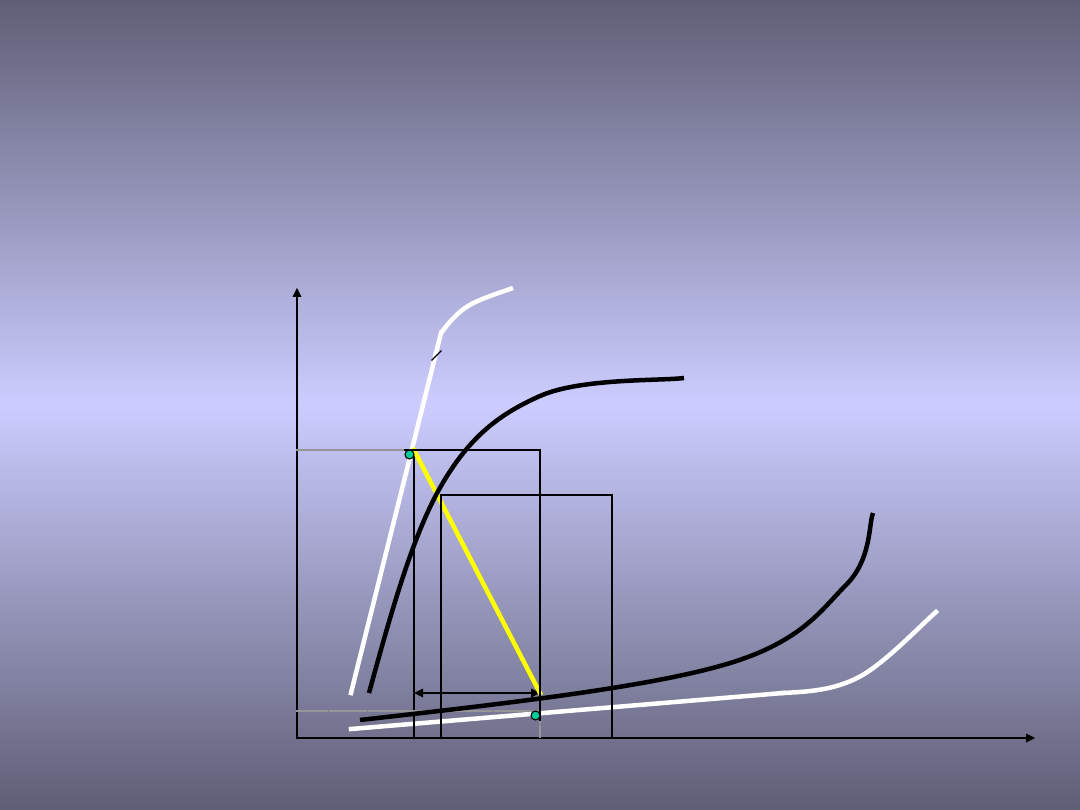
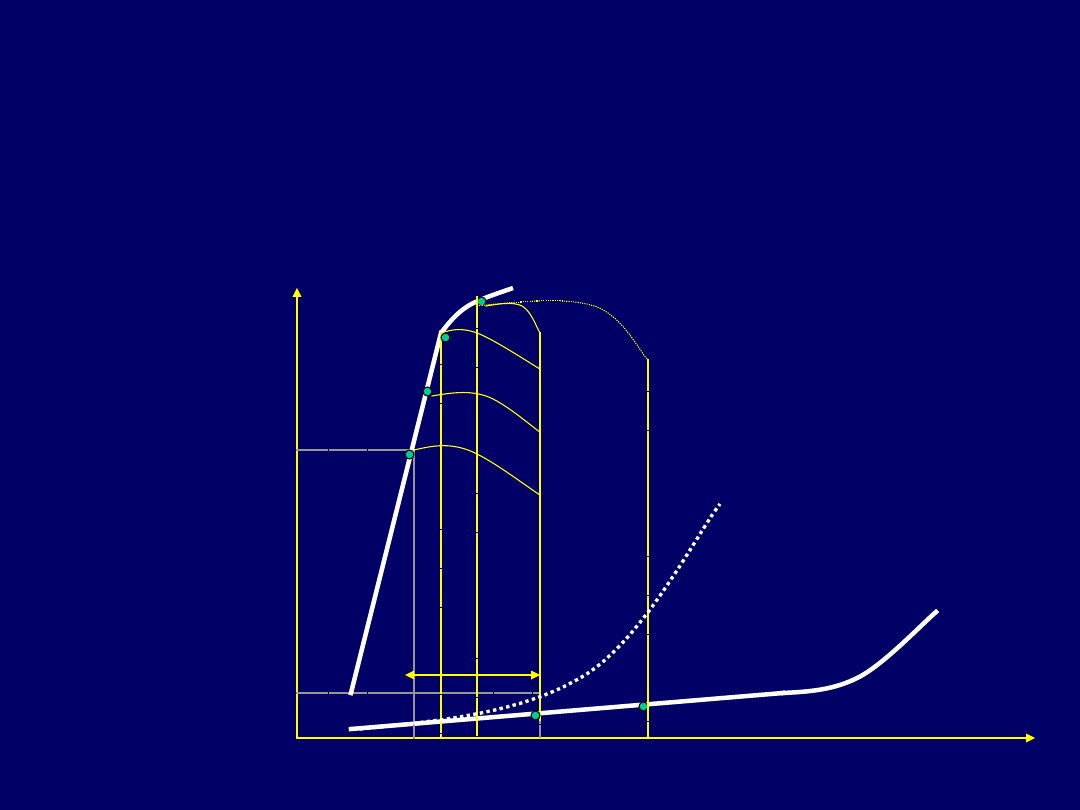
SV
TSV
TDV
TSP
TDP
Pressure
Volume
Systole
Diastole
A
B
CO = F x SV
SV = TDV - TSV
TDV = SV + TSV
TSP = SBP
TSP/TSV
Newborn’s circulation

• At birth the lungs can inflate and perform
their true function meaning that the fetal
bypass systems are no longer required
Umbilical vein - Constricts to form the
ligamentum teres, which extends from
the umbilicus to the liver. The
mesentery that surrounded the
umbilical vein becomes the falciform
ligament
Ductus venosus - A sphincter in the
ductus venosus constricts so that all
blood entering the liver passes through
the hepatic sinusoids

• Foramen ovale - Due to aeration of
the lungs, pulmonary resistance
decreases and pulmonary blood flow
increases. The increase in
pulmonary blood flow causes the
pressure in the left atrium to raise
above that of the right which results
in the valve of the foramen ovale
being pushed against the septum
secundum. This closes the foramen
ovale and its vestige is known as the
fossa ovale

• Ductus arteriosus - The change
in the partial pressure of oxygen in
the blood once the lungs become
functional controls the constriction
of the ductus arteriosus. Closure of
the duct is usually complete soon
after birth and its remnant is known
as the ligamentum arteriosus

Umbilical arteries - The intra-
abdominal portions of the umbilical
arteries constrict. Some parts remain
patent supplying the urinary bladder
and these are contained within the
lateral vesicle ligaments which are
vestiges of the mesentery
surrounding the umbilical arteries

Congenital cardiac defect
• The word congenital means 'inborn or
existing at birth.' The phrases congenital
heart defect and congenital heart disease
are often used to mean the same thing,
but the word defect is more accurate. It
means an abnormality, not a disease. The
defect was caused by the incorrect
development of the heart, or blood
vessels near the heart, before birth

Congenital cardiac defect
• Frequency - eight of every 1,000 infants
born alive. That is almost one percent of
live-born infants.
• Surgery helps many children whose
lives are endangered, or who are
severely afected by their heart
abnormality

What cause the congenital heart
defect?
• About ten percent of heart defects are
caused by specific genetic abnormalities
• These may result from:
– abnormal chromosomes, as in Down's
syndrome
– abnormal gene that is passed down
from one generation to the next, as in
Marfan syndrome

What cause the congenital heart
defect?
• For the remaining 90 percent, a poorly understood
combination of genetic predisposition and
environmental factors is thought to be responsible
• Some congenital heart defects result from
abnormalities in the mother's health during
pregnancy (diabetes or systemic lupus
erythematosus)
• Certain infections in the expectant mother may
also cause abnormalities. For example, rubella is a
significant risk of developing a heart defect
(approximately 35 percent)

What cause the congenital heart
defect?
• Certain drugs are felt to cause
developmental heart abnormalities. This
includes the mother's use of alcohol,
drugs, and seizure medications

What cause the congenital heart
defect?
• Parents with congenital heart defects are
more likely to have afected children than
are parents with normal hearts
(approximately ten percent versus one
percent)
• If one child in the family has a congenital
heart defect, the chance of having other
children with a heart defect is slightly
increased (four percent versus one percent)
10
90
60
40
60
40
0%
20%
40%
60%
80%
100%
First exam.
Symptoms (+)
Not
diagnosed
Symptoms (-)
Symptoms (+)
Not dignosed
Diagnosed
Died, symtoms<6week
• The time of greatest hazard to the
infant with congenital heart defect
• The time before admission to the
specialist centre
• Framework for the future
• Efficient stabilisation of the sick
child in the local hospital while
awaiting transfer

• 25% - not diagnosed before birth
• Mortality after switch operation -
1%
• Mortality before surgery - 4%

• A full sequential diagnosis is rarely
available during the initial phase of
the resuscitation
• Decision has to be based on
clinical findings

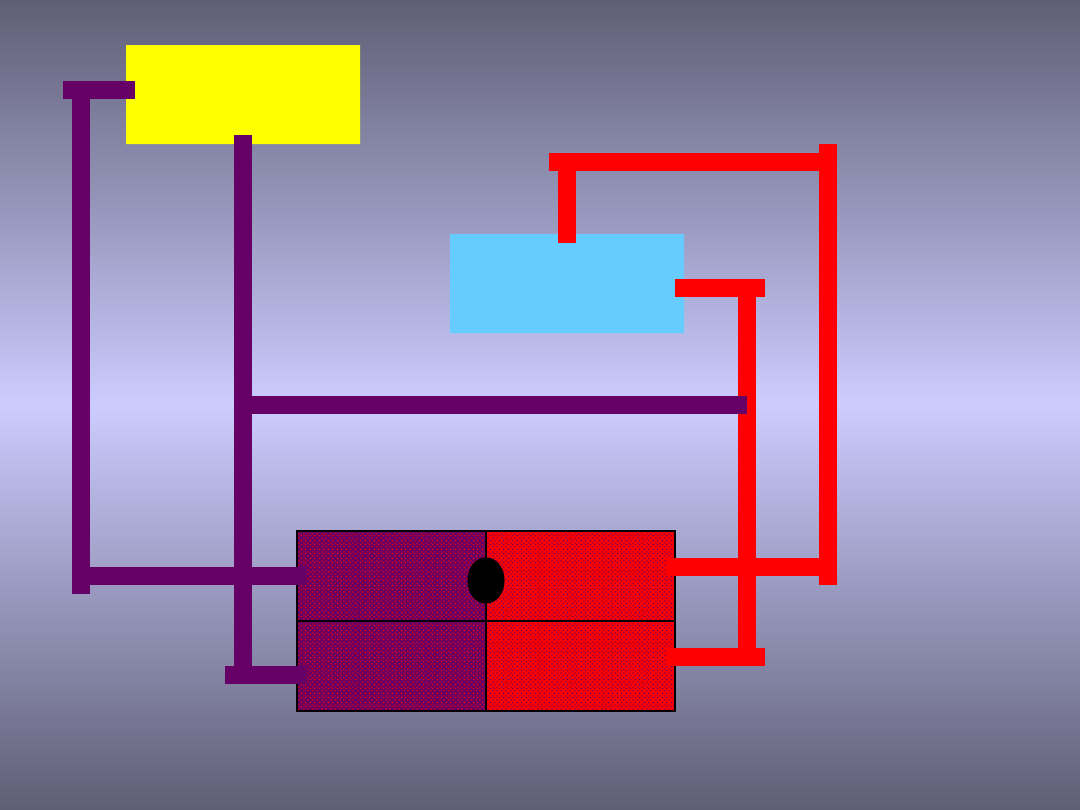
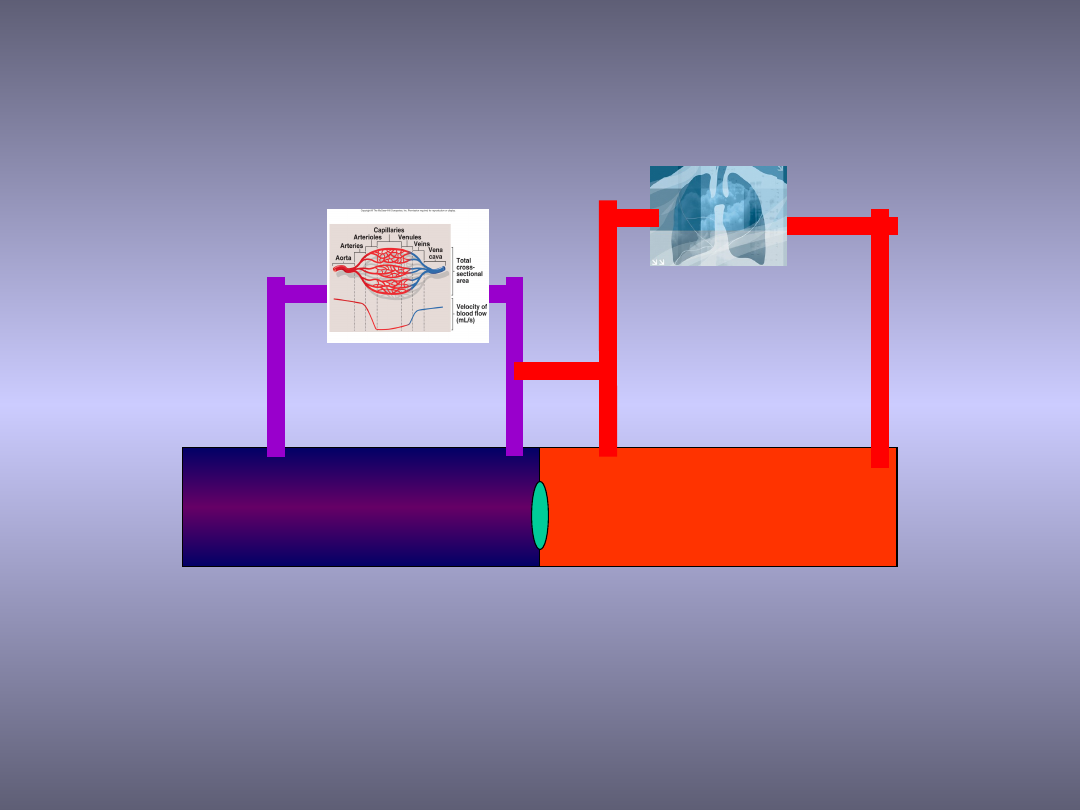
Critical heart diseases
• Cyanotic
– Pulmonary flow dependent on PDA
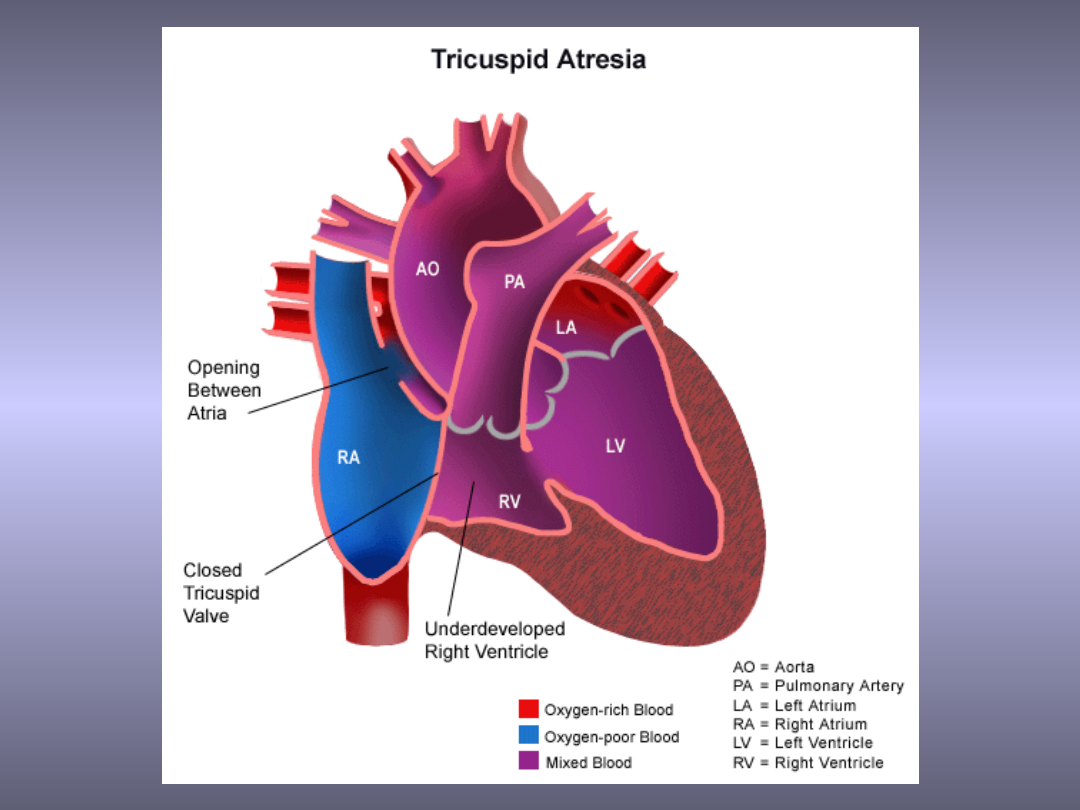
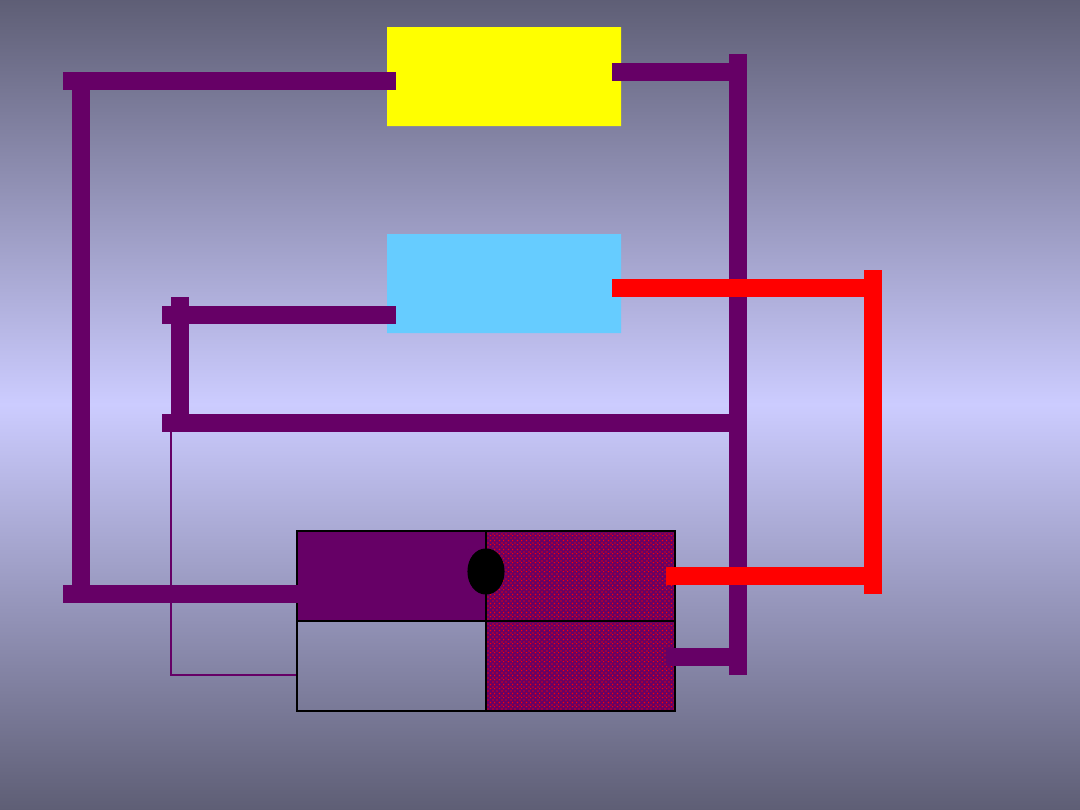
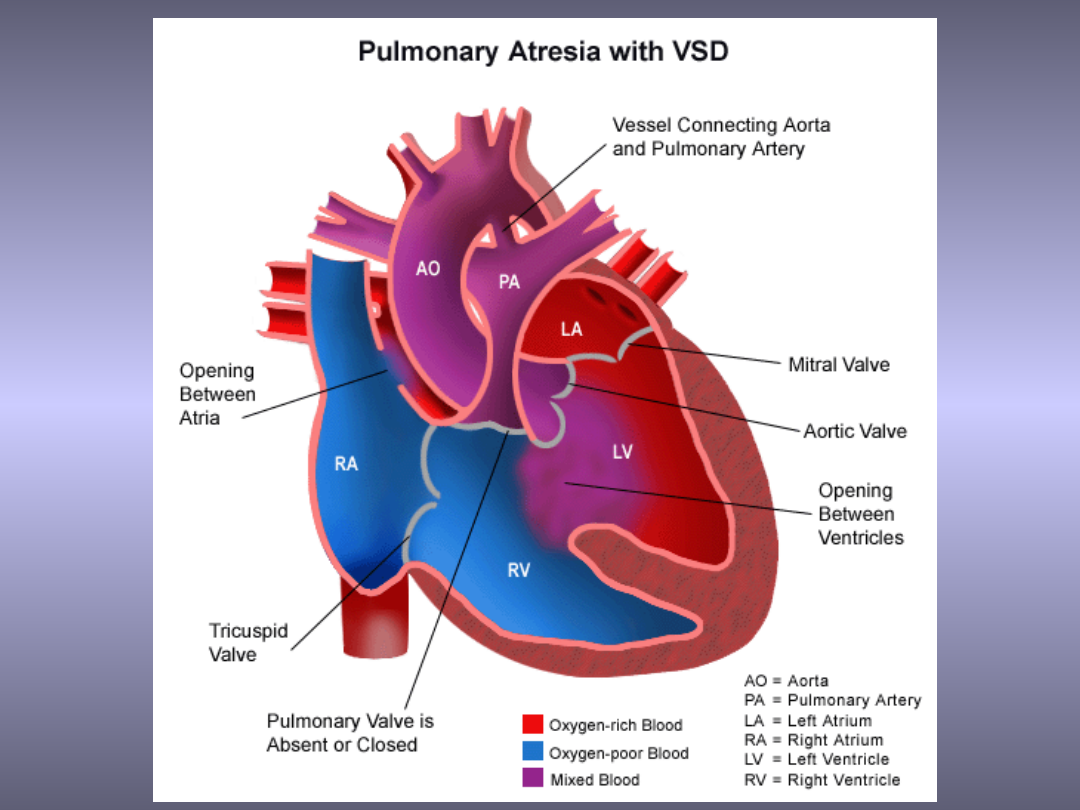
• Tricuspid atresia
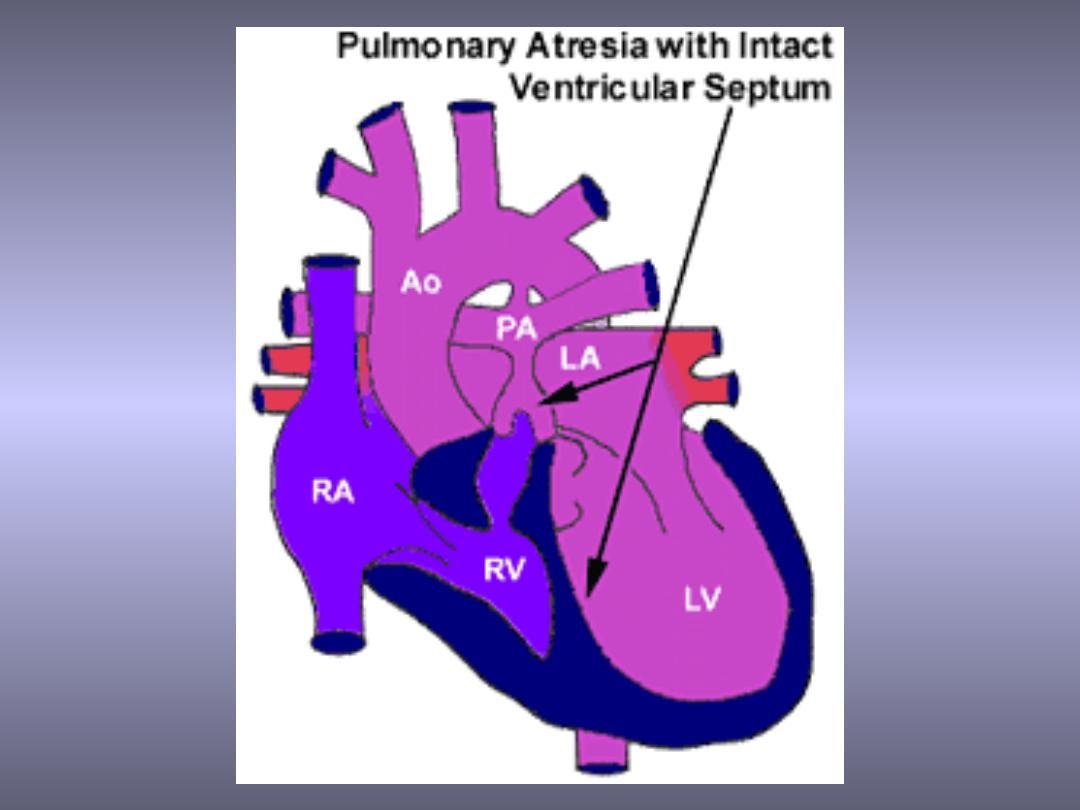
• Pulmonary artesia
– TGA
– TAPVR
• Non-cyanotic
– Systemic flow dependent on PDA
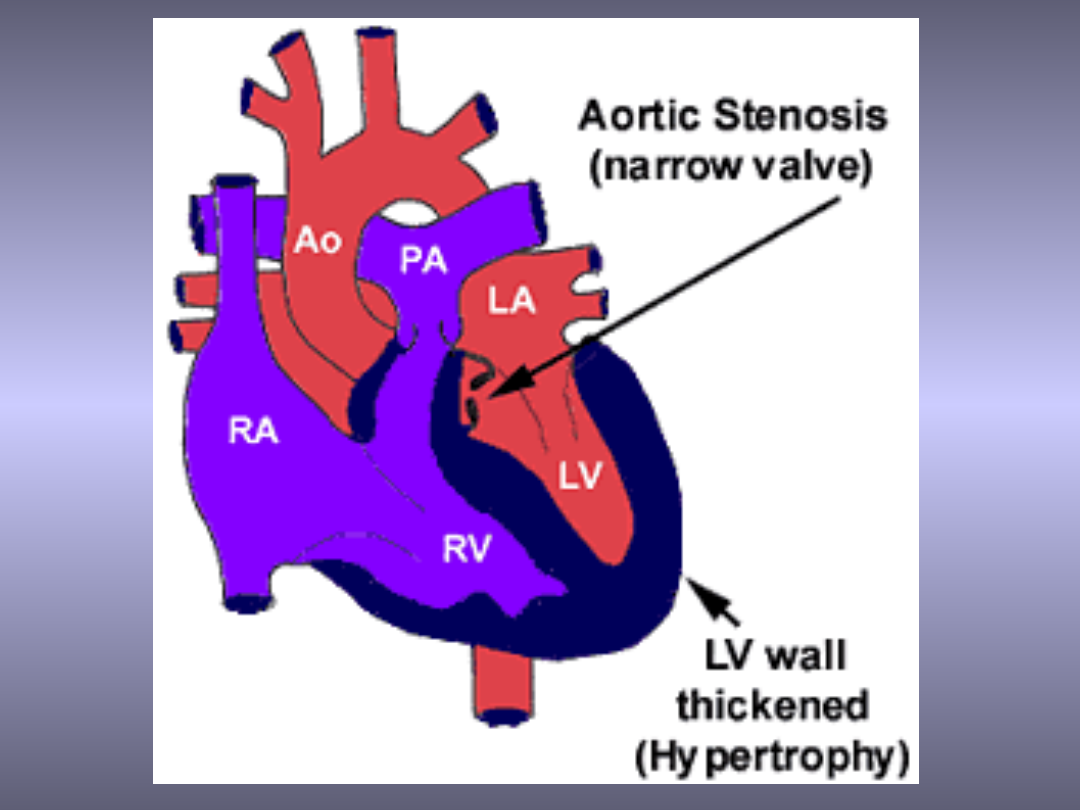
• Aortic stenosis
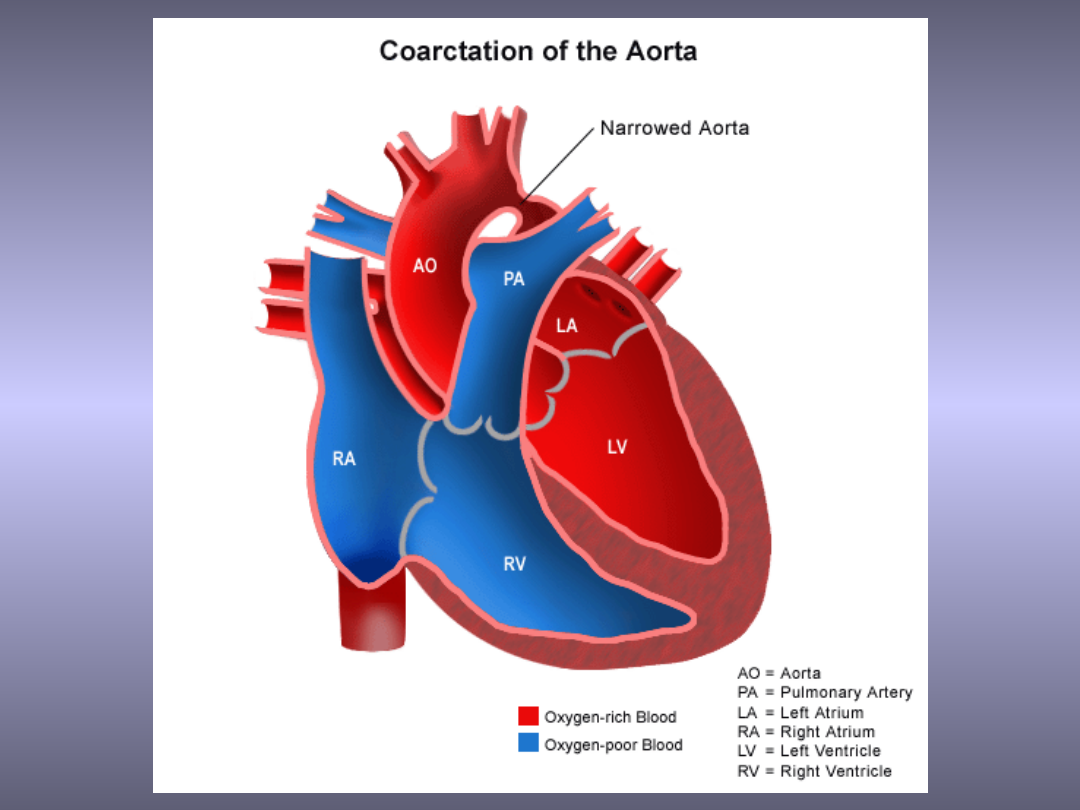
• Coarctation of the aorta
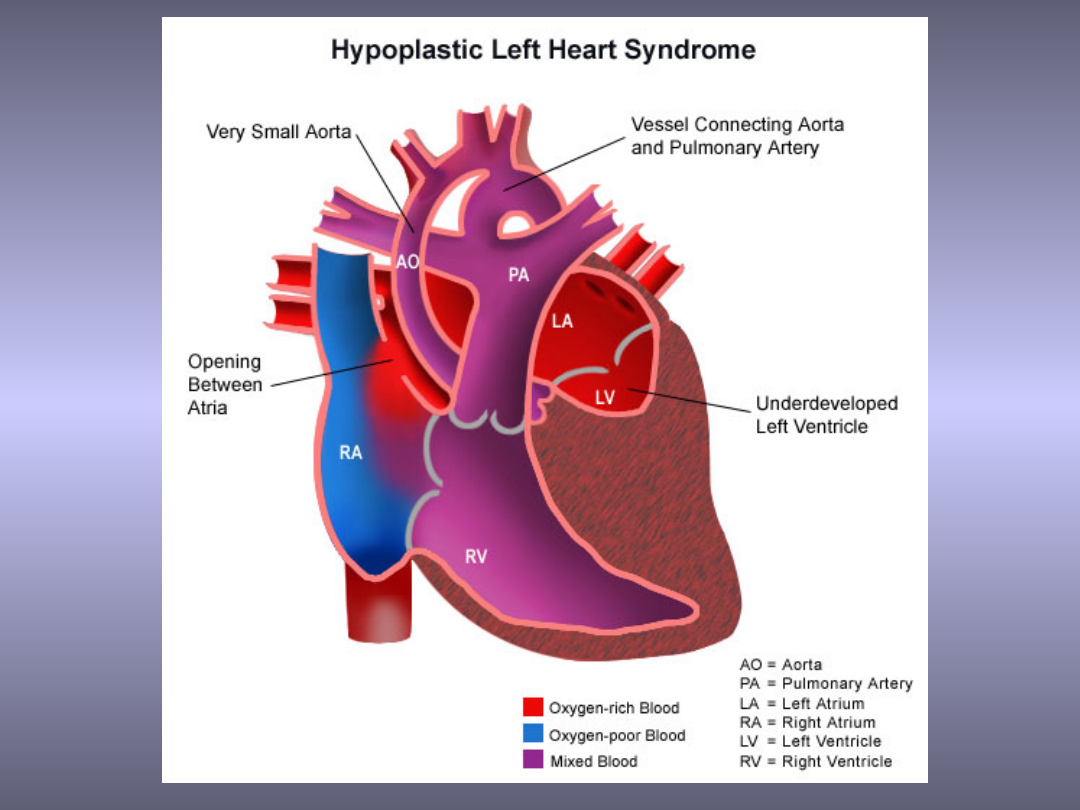
• Congestive heart failure dur4ing fetal
live
– HLHS
– PS and AS (congestive heart failure)
RV
LV
RA
LA
Body
Lungs
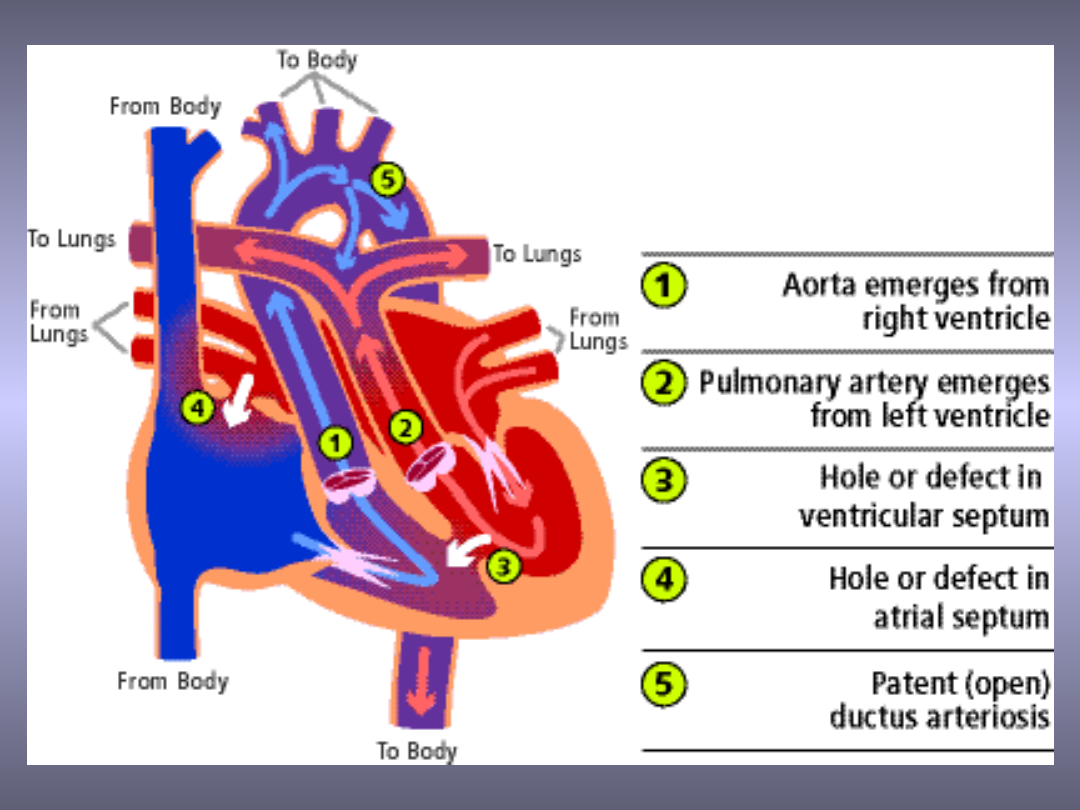

TGA
• Complete transposition of the great arteries
(TOGA)
– The great arteries are reversed from their normal
connections
– The aorta, which normally comes of the left ventricle
and pumps red blood to the body, arises from the right
ventricle and pumps blue blood returning from the
body back to the body bypassing the lungs completely
– The pulmonary artery, which normally arises from the
right ventricle and pumps blue blood to the lungs,
arises from the left ventricle and sends red blood
returning from the lungs right back to the lungs

TGA
• The most common cyanotic
congenital heart disease (accounts
for 5 to 7% of all congenital heart
defects)
• It is more common in males
• Babies are usually normal birth
weight and size

TGA
• There are several other heart abnormalities
that may occur along with TGA
–
The most common associated problems are:
• ventricular septal defectt it can cause left ventricular
outflow tract obstruction
• coronary Artery Anomalies
• single ventricular morphology
• cardiac malposition

TGA
• For survival an atrial septal defect
and a patent ducts arteriosus is
necessary
RV
LV
RA
LA
Body
Lungs
RV RA
LA LV
LV
RA
LA
Body
Lungs
RV
LV
RA
LA
Body
Lungs
RV
LA
LV
RA

Obstructed systemic flow
• Diagnosis
– Systemic hypoperfusion
– Acidosis
– Hypotension
– Organ impairment
– CoA - femoral pulses weaker than the right
brachial pulse
• Treatment
– Optimise systemic oxygen delivery
– Prevent metabolic acidosis
RA
LA
Body
Lungs
RV
LV
RV
RA
LA LV
FiO
2
↑
MAP↓
Katecholamin
y
FiO2↓
MAP↑
Milrinon

Treatment of critical heart
diseases
• Prostaglandins
– Duct dependent
• Pulmonary flow (PA, TA)
• Systemic flow (CoA, AS, HLHS)
– Mixing of the blood (TAPVR, TGA)
• Rshkind procedure
– Restrictive FoA

Use of prostaglandins
• The risk of withholding
prostaglandins infusion depends on
the patient’s clinical condition
Cyanosed neonate
Noncyanosed neonate
Murmur
Abnormal puls
Prostaglandin infusion
Infant in extremis
Infant in good condition
+
+

Use of prostaglandins
• Ductal patency is vital for the survival
• Apnea secondary to prostaglandin
infusion - indication for intubation not to
reduce the dose and never to stop the
infusion
• Balance between the systemic and
pulmonary blood flow

Systemic, myocardial,
pulmonary circulation are in
parallel and constant
dynamic competition with
one another

Recommendations
• Prostaglandin infusion must be started at
a rate sufficient to maintain ductal
patency
• Ventilatory parameters should be
adjusted to manipulate the pulmonary
vascular resistance to avoid pulmonary
overcirculation, so as to maintain a
pulmonary to systemic blood flow ratio
about 1:1
Hypoxia
PEEP
Mean airway perssure
Pulmonary vasular resistance
Systemic saturation 75-85%
Hyperoxia
Respiratory alkalosis
Systemic vasular resistance
Systemic saturation 75-85%
PEEP
Mean airway perssure
Nitroprusside
Katecholamine

Recommendation
• Apply a modest PEEP - 4-6 cmH
2
O
• Ventilation with room air in the first
instance
• Adjusting inspiratory pressures, rate, tidal
volume to achieve an arterial CO
2
tension
50-60mmHg, systemic saturation 75-85%
• Avoiding respiratory alkalosis

Low cardiac output
• Reassess the baby to ensure that the
prostaglandin infusion is adequate and
intravascular volume is satisfactory
• Aneamia should be corrected
• Nitroprusside infusion- if the systemic
pressure is normal
• Low dose inotrope infusion may be benefit
in arresting the vicious cycle of metabolic
acidosis and worsening ventricular function

• High dose of katechlamine should
be avoided because they may
increase systemic vascular
resistance, forcing more blood into
lungs and worsening the
pulmonary to systemic blood flow
distribution
Lack of response to prostaglandin infusion
Obstructed total anomalous pulmonary venous return
Reduced pulmonary vascular resistance
Increased pulmonary flow
Congestive heart failure
Lack of response to prostaglandin infusion
Transposition of great arteries
with
Intact intraventricular septum
Restrictive atrial septum
Atrial septostomy

Diferential diagnosis
• Obstructed systemic circulation and sepsis
– Incidence of the two is about the same
– 22-47% of neonates with HLHS have non
cardiac murmur
– Neonate with severe sepsis may have
reduced peripheral pulses secondary to
low cardiac output

Persistence Pulmonary Hypertension
(PPH or PFC) and duct dependent
pulmonary flow
• 9% patients treated with ECMO have CHD
• RTG-oligaemic lungs
• NO test
– Improvement in CHD because of decreased
pulmonary vascular resistance
– Negative in PFC because of intracardiac right
to left shunt
• Prostaglandins
– Decreases pulmonary vascular resistance

• Indications for early ECMO
– Cyanosis
– CO
2
clearance is relatively easy to achieve
– Radiologically normal (or oligaemic) lungs

CHD and parenchymal lung
disease
• Obstructed TAPVR
• Unremarkable clinical cardiovascular
examination
• Clinically and radiologically
indistinguishable from diseases of lung
parenchyma (pneumonia, meconium
aspiration, early emphysema)

In utero diagnosis
• HLHS - mortality is similar after in-utero
and ex-utero diagnosis
• TGA - mortality after in-utero diagnosis
is lower than after ex-utero diagnosis
• Transfer in-utero and delivery in the
tertiary care centre

Transport
• The timing of transfer is determined by the
diagnosis and clinical condition of the
newborn
–
Stabilisation before transfer
–
Vascular access
–
Prostaglandin infusion
• The infant with the duct dependent lesion will
improve greatly once ductal patency has
been achieved with prostaglandin infusion

Transport
• Despite of prostaglandin infusion clinical
improvement and stability are not achieved
• Asses the infusion of prostaglandin and
venous access
• TGA with restrictive atrial septum and
TAPVR - stabilisation may not be possible
(prompt transfer to a cardiac centre)

Transport
• Indications for intubation
– Respiratory distress
– Sever metabolic acidosis
– Apnoea caused by prostaglandin infusion
• Mechanical ventilation should optimise
systemic myocardial and pulmonary
blood flow
SV
TSV
TDV
TSP
TDP
Pressure
Volume
Systole
Diastole
A
B
CO = F x SV
SV = TDV - TSV
TDV = SV + TSV
TSP = SBP
TSP/TSV
Newborn’s circulation

Congestive heart failure
• Failure to adequately perfuse the
capillary beds of various organs
• The loos of the possibility of
oxygenation transport to the organs
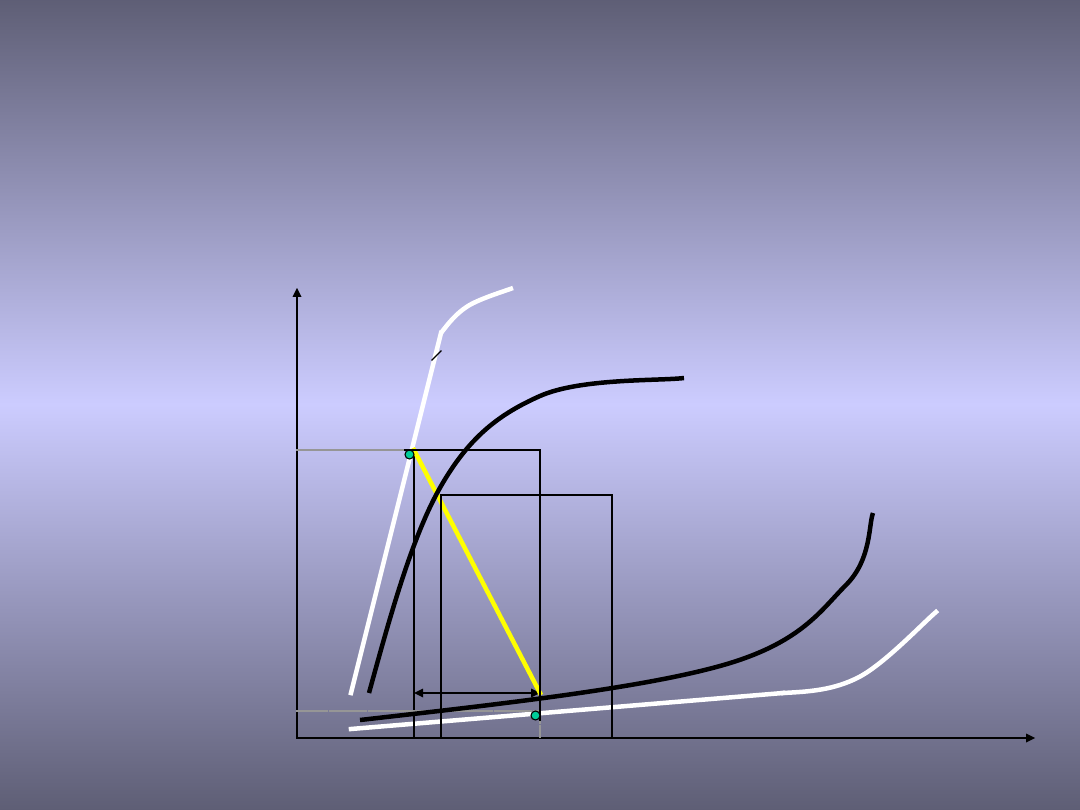
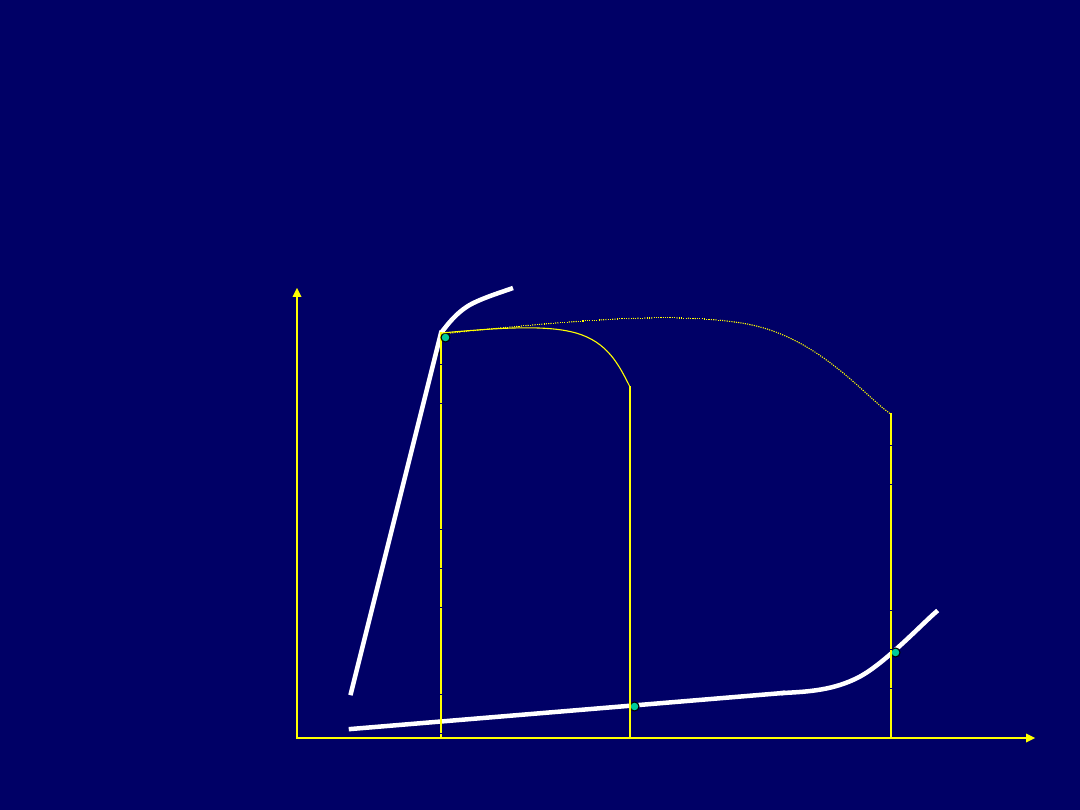
SV
TSV
TDV
TSP
TDP
Pressure
Volume
Contractility
Compliance
A
B
CO = F x SV
SV = TDV - TSV
TDV = SV + TSV
TSP = SBP
TSP/TSV
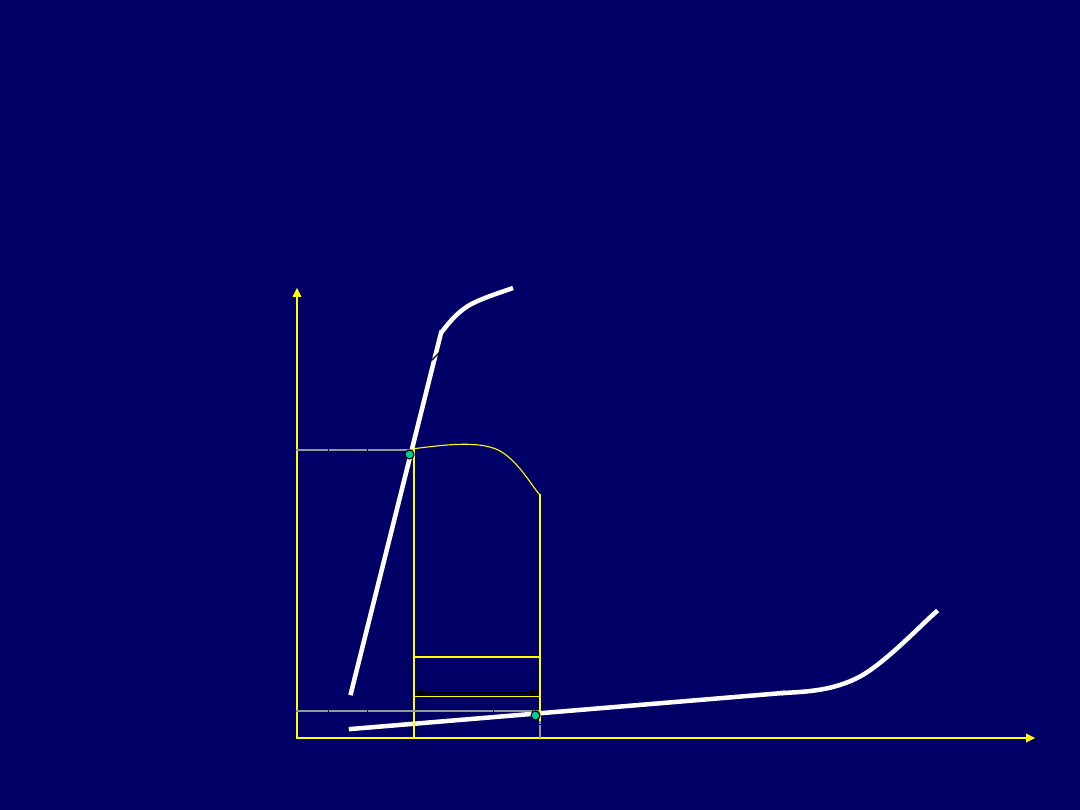
Isovolumetric
contraction
Ejection
filling
Isovolumetric
diastole
Relationship of pressure and volume
during contraction and diastole
SV
Pressure
Volume
Contraction
Diastole
A
B
A-1
B-1
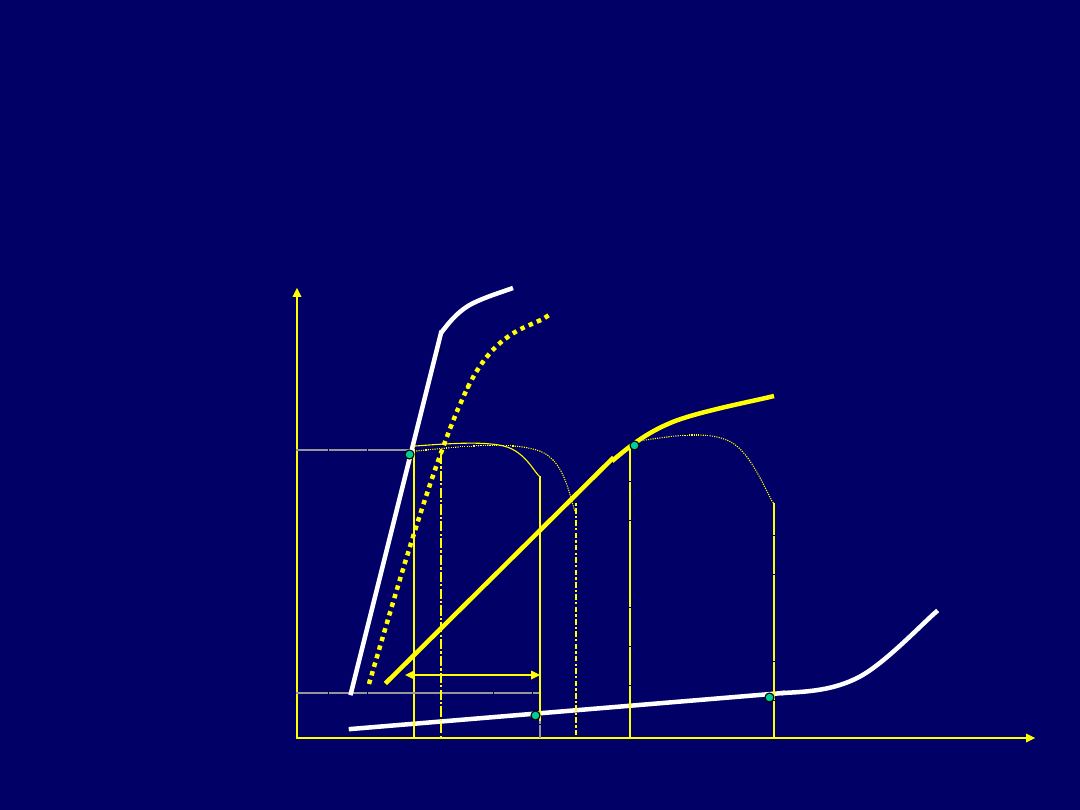
Decreased contraction
Pressure
Volume
B
A
B-1
Decreased compliance
SV
Pressure
Volume
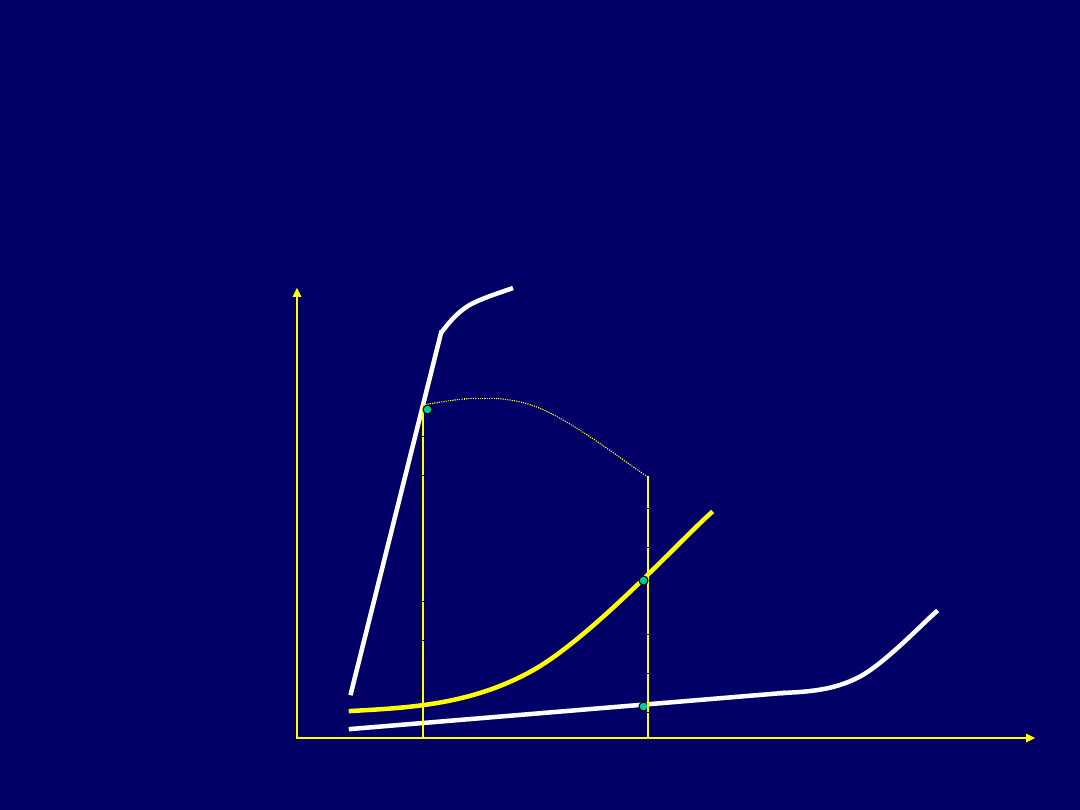
A
B
A-1
B-1
Change of the afterload
Pressure
Volume
B
A
B-1
Change the preload
Document Outline
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Slide 45
- Slide 46
- Slide 47
- Slide 48
- Slide 49
- Slide 50
- Slide 51
- Slide 52
- Slide 53
- Slide 54
- Slide 55
- Slide 56
- Slide 57
- Slide 58
- Slide 59
- Slide 60
- Slide 61
- Slide 62
- Slide 63
- Slide 64
- Slide 65
- Slide 66
- Slide 67
- Slide 68
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
Wyszukiwarka
Podobne podstrony:
If money were not a problem in the future I would like to live in a two
The problems in the?scription and classification of vovels
Infection in the neonatal period
Gambling in the United States A Quick Look at the Problem
Taylor & Francis The Problems of the Poor in Tudor and Early Stuart England (1983)
RÜDIGER SCHMITT The Problem of Magic and Monotheism in The Book of Leviticus
Diacu F Relative equilibria in the 3 dimensional curved n body problem (MEMO1071, AMS, 2014)(ISBN 97
The Problem of Unity in the Polish Lithuanian State 1963 [Oswald P Backus III]
The Immigration Problem in America and its Solvency doc
Haranas The Classical Problem of a Body Falling in a Tube Through the Center of the Earth in the Dy
Problems for the exam in the History of English
Griffiths, Turnbullb And White Re Examining The Small Cap Myth Problems In Portfolio Formation And L
Thomas C Holt The Problem of Race in the Twenty first Century (2001)
Dyson, Rebecca M i inni Interactions of the Gasotransmitters Contribute to Microvascular Tone (Dys)
Mettern S P Rome and the Enemy Imperial Strategy in the Principate
Early Variscan magmatism in the Western Carpathians
Applications and opportunities for ultrasound assisted extraction in the food industry — A review
In the end!
Cell surface in the interaction Nieznany
więcej podobnych podstron