
Diabetes Mellitus
in Primary Care
Grzegorz
Grzegorz
Margas
Margas

Joanna Nowak, 41 years old housewife has been
Joanna Nowak, 41 years old housewife has been
complaining from intensive thirst and polyuria for two
complaining from intensive thirst and polyuria for two
weeks. In this time she lost approx. 2 kg. Since her older
weeks. In this time she lost approx. 2 kg. Since her older
brother is diabetic, using his tests at home she detected
brother is diabetic, using his tests at home she detected
presence of sugar in the urine. She was healthy in the
presence of sugar in the urine. She was healthy in the
past. She had never complained from fever, dysuria,
past. She had never complained from fever, dysuria,
back pain, cough or headache. She had regular menses.
back pain, cough or headache. She had regular menses.
She gave birth three healthy children, every with birth
She gave birth three healthy children, every with birth
weight above 3,5 kg, but no above 4 kg. Her family
weight above 3,5 kg, but no above 4 kg. Her family
history is positive - brother is diabetic on oral glucose-
history is positive - brother is diabetic on oral glucose-
lowering drugs, mother has impaired glucose tolerance.
lowering drugs, mother has impaired glucose tolerance.
There are no other endocrine disturbances.
There are no other endocrine disturbances.
Mrs. Nowak weights 65 kg at height 155 cm. BP 130 / 85
Mrs. Nowak weights 65 kg at height 155 cm. BP 130 / 85
mmHg, HR 75/min - regular. Apart from slight
mmHg, HR 75/min - regular. Apart from slight
overweight physical examination did not reveal any
overweight physical examination did not reveal any
other pathology.
other pathology.

1 What is your diagnostic
1 What is your diagnostic
consideration?
consideration?
2 What additional examinations
2 What additional examinations
should be performed?
should be performed?
3 What is your treatment?
3 What is your treatment?

Additional
Additional
investigations ordered
investigations ordered
by you showed:
by you showed:
Glycaemia: 15, 6 mmol/l,
Glycaemia: 15, 6 mmol/l,
C
C
holesterol 250 mg / dl, TG 300
holesterol 250 mg / dl, TG 300
mg / dl
mg / dl
G
G
lucosuria (5 %), without acetone.
lucosuria (5 %), without acetone.

Diabetes Mellitus in
Diabetes Mellitus in
Primary Care
Primary Care
Detection
Detection
Treatment
Treatment

Definition
Definition
A disorder of carbohydrate
A disorder of carbohydrate
metabolism associated with
metabolism associated with
relative or absolute deficiency
relative or absolute deficiency
of insulin
of insulin

Diabetes mellitus type
Diabetes mellitus type
1
1
Insulin dependent diabetes mellitus, IDDM
Insulin dependent diabetes mellitus, IDDM
β
β
-cell destruction usually leading to absolute
-cell destruction usually leading to absolute
insulin deficiency
insulin deficiency
more prevalent in young persons
more prevalent in young persons
little or no endogenous secretion of insulin and
little or no endogenous secretion of insulin and
therefore requiring insulin replacement
therefore requiring insulin replacement
more severe
more severe

Etiology of diabetes
Etiology of diabetes
type 1
type 1
Genetic factors:
Genetic factors:
–
increased frequency of HLA DR3 and HLA DR4
increased frequency of HLA DR3 and HLA DR4
–
Increased frequency of diabetes in siblings
Increased frequency of diabetes in siblings
Immunological
Immunological
–
Islet cell antibodies present in the early stages of
Islet cell antibodies present in the early stages of
the disease
the disease
–
Immune-suppresion with cyclosporin A soon after
Immune-suppresion with cyclosporin A soon after
the onset of the diabetes can produce lasting
the onset of the diabetes can produce lasting
remission of IDDM
remission of IDDM
Environmental
Environmental
–
Viral infection (Coxsackie B and rubella) trigger in
Viral infection (Coxsackie B and rubella) trigger in
genetically-predisposed individuals
genetically-predisposed individuals
–
Breast-feeding can offer some protection against
Breast-feeding can offer some protection against
the development of diabetes
the development of diabetes

Diabetes mellitus type
Diabetes mellitus type
2
2
Non-insulin dependent diabetes mellitus,
Non-insulin dependent diabetes mellitus,
NIIDM)
NIIDM)
From predominantly insulin resistance with
From predominantly insulin resistance with
relative insulin deficiency to predominantly
relative insulin deficiency to predominantly
an insulin secretory defect with insulin
an insulin secretory defect with insulin
resistance
resistance
mature onset
mature onset
insulin still produced
insulin still produced
associated with obesity
associated with obesity

Etiology of diabetes
Etiology of diabetes
type 2
type 2
Genetic factors: more important
Genetic factors: more important
than in IDDM
than in IDDM
Insulin resistance
Insulin resistance
Abnormal beta-cell function
Abnormal beta-cell function
Environmental factors:
Environmental factors:
–
Obesity
Obesity
–
Physical activity
Physical activity
–
Diet
Diet
Insulin
dependent
(type I)
10%
Non-insulin
dependent
(type II)
90%
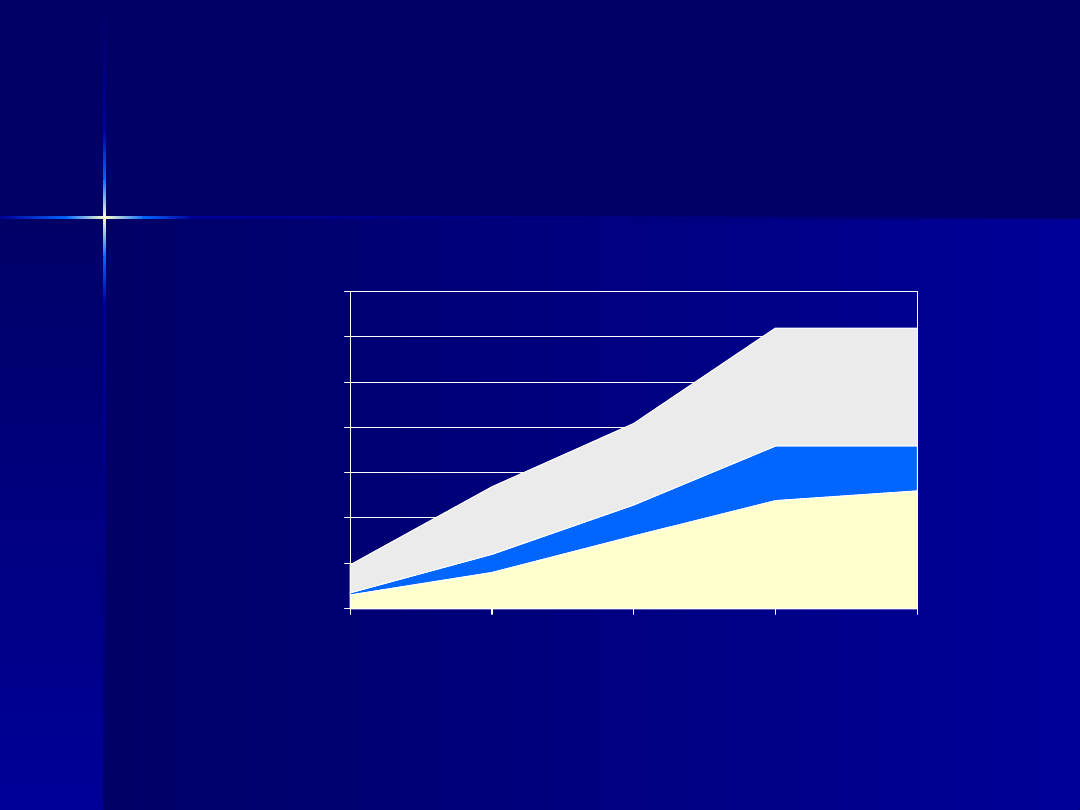
Prevalence
Prevalence
Diagnosed DM
Undiagnosed DM
IFG
0
5
10
15
20
25
30
35
20-39
40-49
50-59
60-74
>75
Age
% of population
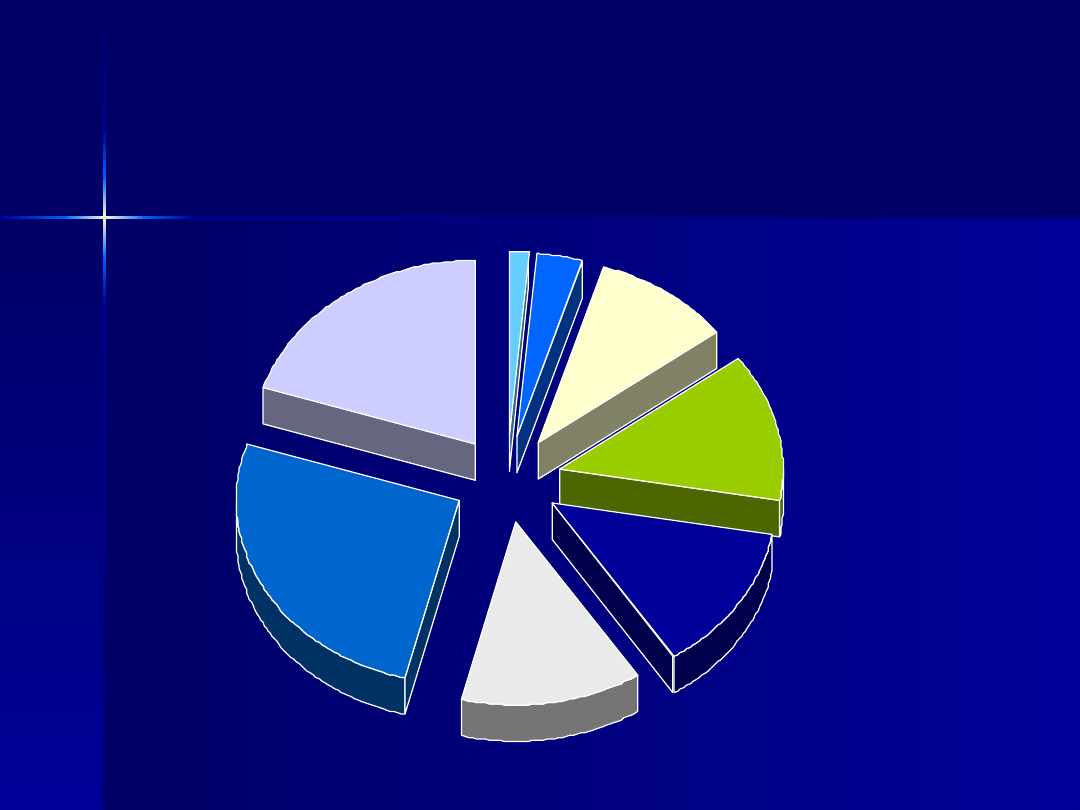
Age at first diagnosis
Age at first diagnosis
0-9
1%
10-19
3%
20-29
10%
30-39
13%
40-49
13%
50-59
13%
60-69
27%
>70
20%
Diabetics in practice of 2000
Diabetics in practice of 2000
patients
patients
120
120
60
60
Patients with DM
Patients with DM
Patients with undiagnosed
Patients with undiagnosed
DM
DM

Diabetes type 1
Diabetes type 1
presentation
presentation
Severe acute
Severe acute
diabetes
diabetes
–
Dehydratation
Dehydratation
–
Nausea and
Nausea and
vomiting
vomiting
–
Abdominal pain
Abdominal pain
–
Circulatory
Circulatory
collapse
collapse
–
Stupor
Stupor
coma
coma
Subacute
diabetes:
– Polyuria and
polydypsia
– Loss of weight
– Fatigue and
weakness
– Pruritus
– Paraesthesiae
– Visual
disturbances

Diabetes type 2
Diabetes type 2
presentation
presentation
Many are asymptomatic
Many are asymptomatic
Symptoms are often mild and gradual-
Symptoms are often mild and gradual-
thirst, polyuria and loss of weight
thirst, polyuria and loss of weight
developing over several months
developing over several months
Other symptoms:
Other symptoms:
–
Susceptibility to staphylococcal skin infections
Susceptibility to staphylococcal skin infections
–
Candida vaginitis
Candida vaginitis
–
Balanitis
Balanitis
–
Increased mortality from atherosclerotic
Increased mortality from atherosclerotic
complications
complications

A seventy-one-year-old man was found to have
A seventy-one-year-old man was found to have
diabetes when he presented with thirst,
diabetes when he presented with thirst,
polyuria, and gangrene of the right big toe,
polyuria, and gangrene of the right big toe,
which required amputation of the leg. His
which required amputation of the leg. His
record showed that five years previously he
record showed that five years previously he
had been treated for balanitis. Three years
had been treated for balanitis. Three years
previously he had pain in both legs. X-ray
previously he had pain in both legs. X-ray
showed flattening of the lumbosacral disc. He
showed flattening of the lumbosacral disc. He
was treated with a plaster cast and was off
was treated with a plaster cast and was off
work four months. The orthopedic report stated
work four months. The orthopedic report stated
that his leg reflexes were absent and that there
that his leg reflexes were absent and that there
was sensory loss on the inner side of the left
was sensory loss on the inner side of the left
foot. Later in the same year he was treated for
foot. Later in the same year he was treated for
a purulent blister on the finger. There was no
a purulent blister on the finger. There was no
record of any urine tests.
record of any urine tests.

Screening for diabetes mellitus
Screening for diabetes mellitus
patients with at least one of the following risk
patients with at least one of the following risk
factors:
factors:
Age > 45
Age > 45
obesity (BMI >27)
obesity (BMI >27)
diabetes mellitus in close family
diabetes mellitus in close family
diabetes mellitus during pregnancy or borning child > 4 kg
diabetes mellitus during pregnancy or borning child > 4 kg
Hypertension
Hypertension
HDL cholesterol < 0,9 mmol/l and/or triglycerides > 2,2
HDL cholesterol < 0,9 mmol/l and/or triglycerides > 2,2
mmol/l
mmol/l
IGT or IFG in recent test
IGT or IFG in recent test
cardiovascular event in the history
cardiovascular event in the history
symptoms of diabetes
symptoms of diabetes
If results are normal: repeat every three years
If results are normal: repeat every three years
Diagnostic criteria
Diagnostic criteria
Normal
IFG
IGT
Diabetes
mellitus
Random
< 5,5
mmol/l
11,1
mmol/l
Fasting
< 6,1
mmol/l
6,1 – 6,9
mmol/l
7,0
mmol/l
2 h after
intake 75
g glucose
< 7,8
mmol/l
< 7,8
mmol/l
7,8 – 11,0
mmol/l
11,1
mmol/l

Symptomatic
Symptomatic
or
or
glycosuria
glycosuria
or
or
incidental hyperglycaemia:
incidental hyperglycaemia:
Check
Check
random venous plasma glucose
random venous plasma glucose
–
If
If
≥11.1 mmol/l = "Diabetes"
≥11.1 mmol/l = "Diabetes"
–
If
If
>5.5 mmol/l
>5.5 mmol/l
then
then
proceed to next
proceed to next
step (and review cause of symptoms)
step (and review cause of symptoms)
Diagnosis of Diabetes Mellitus

Diagnosis of Diabetes Mellitus
Diagnosis of Diabetes Mellitus
Fasting glucose:
Fasting glucose:
normal
normal
< 6,1 mmol/l
< 6,1 mmol/l
IFG
IFG
6,1-6,9 mmol/l
6,1-6,9 mmol/l
diabetes
diabetes
≥
≥
7,0 mmol/l
7,0 mmol/l

Diagnosis of Diabetes Mellitus
Diagnosis of Diabetes Mellitus
OGTT (venous plasma glucose):
OGTT (venous plasma glucose):
If
If
2-h >11.0 mmol/l = "Diabetes"
2-h >11.0 mmol/l = "Diabetes"
If
If
2-h
2-h
11.0 mmol/l and
11.0 mmol/l and
7.8
7.8
mmol/l = "IGT"
mmol/l = "IGT"
If fasting >6.0 mmol/l and 2-h
If fasting >6.0 mmol/l and 2-h
<7.8 mmol/l = "IFG"
<7.8 mmol/l = "IFG"

1. Fasting glucose estimations requires
1. Fasting glucose estimations requires
no caloric intake for at least 8 hours
no caloric intake for at least 8 hours
–
diagnosis cannot be based on a single
diagnosis cannot be based on a single
abnormal glucose estimation in the
abnormal glucose estimation in the
absence of symptoms
absence of symptoms
2. Venous plasma glucose estimation is
2. Venous plasma glucose estimation is
preferred
preferred

HbA
HbA
1c
1c
(glycated haemoglobin) can
(glycated haemoglobin) can
be useful in clinical diagnosis and
be useful in clinical diagnosis and
follow-up
follow-up
–
HbA
HbA
1c
1c
>7.5 % = fasting plasma
>7.5 % = fasting plasma
glucose
glucose
7.0 mmol/l
7.0 mmol/l
–
HbA
HbA
1c
1c
>6.5 % = fasting plasma
>6.5 % = fasting plasma
glucose >6.0 mmol/l
glucose >6.0 mmol/l

Objectives of
Objectives of
treatment
treatment
To relieve symptoms
To relieve symptoms
To prevent or delay complications
To prevent or delay complications
To prolong life
To prolong life

Management
Management
Survival in diabetes depends
Survival in diabetes depends
primarily on the presence or
primarily on the presence or
absence of vascular complications
absence of vascular complications

Treatment
Treatment
Education
Education
Diet
Diet
Drugs
Drugs
–
Biguanides
Biguanides
–
Sulphonylureas
Sulphonylureas
–
Acarbose
Acarbose
Insulin
Insulin

Diabetics are managed
Diabetics are managed
by:
by:
Diet alone
Diet alone
30%
30%
Diet and drugs
Diet and drugs
40%
40%
Insulin
Insulin
30%
30%

Diet
Diet
Non-insulin dependent type II diabetes
Non-insulin dependent type II diabetes
is highly correlated with obesity
is highly correlated with obesity
There is popular misconception that
There is popular misconception that
eating too much sugar causes diabetes
eating too much sugar causes diabetes
Excessive energy intake, usually from
Excessive energy intake, usually from
a high fat consumption, which
a high fat consumption, which
contributes to obesity and may in turn
contributes to obesity and may in turn
cause diabetes
cause diabetes

Diet in DM
Diet in DM
Moderate caloric restriction
Moderate caloric restriction
Reduction of total fat (especially
Reduction of total fat (especially
saturated)
saturated)
Limiting the total carbohydrate
Limiting the total carbohydrate
intake (not only simple sugars,
intake (not only simple sugars,
but also bread, rice, potatoes etc.)
but also bread, rice, potatoes etc.)
Meals should be spaced throughot
Meals should be spaced throughot
the day
the day

PHYSICAL EXERCISE
PHYSICAL EXERCISE
Can benefit insulin sensitivity, blood
Can benefit insulin sensitivity, blood
pressure, and blood lipid control
pressure, and blood lipid control
Should be taken at least every 2-3
Should be taken at least every 2-3
days for optimum effect
days for optimum effect
May increase the risk of acute and
May increase the risk of acute and
delayed hypoglycaemia
delayed hypoglycaemia
Examples :
Examples :
–
brisk walking, swimming, jogging
brisk walking, swimming, jogging

Oral glucose-lowering
Oral glucose-lowering
drugs
drugs
Begin
Begin
oral agent therapy when :
oral agent therapy when :
an adequate trial of life-style
an adequate trial of life-style
intervention / education has been given
intervention / education has been given
either
either
(usually): HbA
(usually): HbA
1c
1c
>6.5 %, fasting
>6.5 %, fasting
venous plasma glucose >6.0 mmol/l
venous plasma glucose >6.0 mmol/l
or
or
(occasionally) if thin and no other
(occasionally) if thin and no other
arterial risk factor: HbA
arterial risk factor: HbA
1c
1c
>7.5 %, fasting
>7.5 %, fasting
venous plasma glucose
venous plasma glucose
7.0 mmol/l
7.0 mmol/l

Oral glucose-lowering
Oral glucose-lowering
drugs
drugs
First-generation agents
First-generation agents
–
Tolbutamide, Chlopropamide
Tolbutamide, Chlopropamide
Second-generation sulfonylureas
Second-generation sulfonylureas
–
Glipizide, Glibenclamide, Gliclazide
Glipizide, Glibenclamide, Gliclazide
Third generation sulfonylureas
Third generation sulfonylureas
–
Glimepiride, Repaglinide
Glimepiride, Repaglinide
Inhibitor of hepatic gluconeogenesis
Inhibitor of hepatic gluconeogenesis
–
Metformin
Metformin
Inhibitors of rapid glucose absorption
Inhibitors of rapid glucose absorption
–
Glycosidase inhibitors e.g. Acarbose
Glycosidase inhibitors e.g. Acarbose
Insulin sensitisers
Insulin sensitisers
–
Troglitazone
Troglitazone
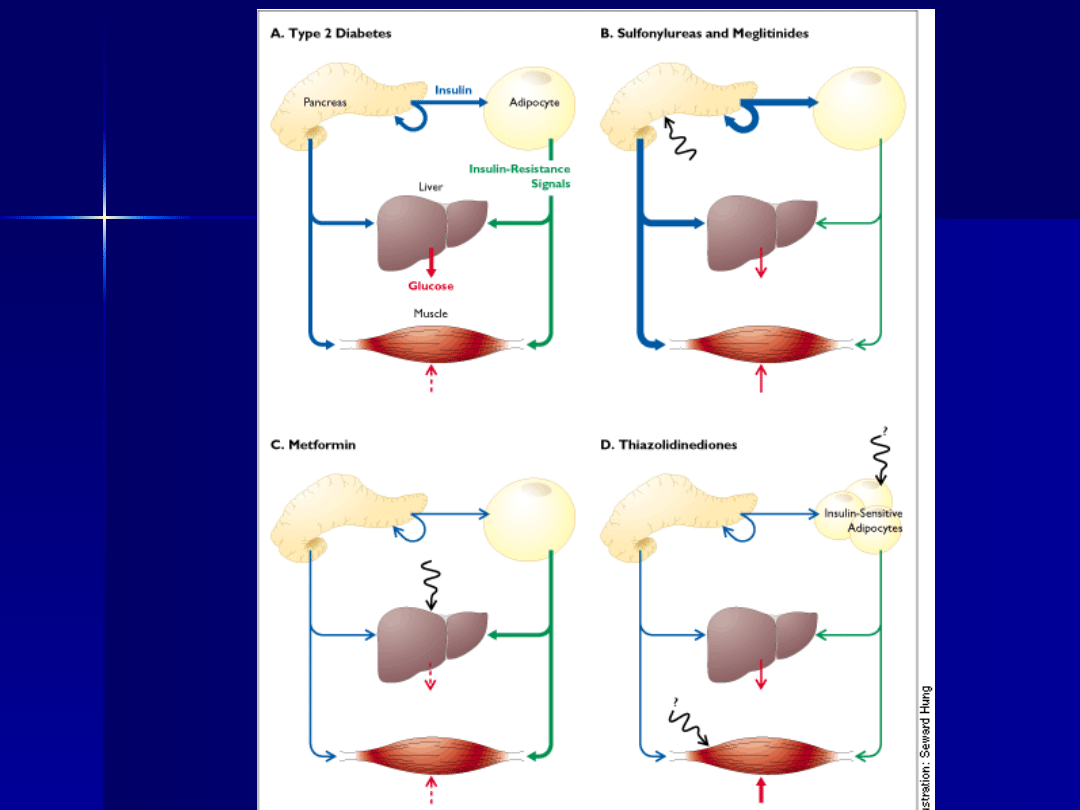

Metformin
Metformin
Acts by decreasing hepatic
Acts by decreasing hepatic
gluconeogenesis and increases tissue
gluconeogenesis and increases tissue
sensitivity to insulin
sensitivity to insulin
Strong evidence base in the
Strong evidence base in the
overweight: patients tend to lose
overweight: patients tend to lose
weight
weight
Hypoglycaemia is very rare
Hypoglycaemia is very rare

Sulphonylureas
Sulphonylureas
Act by increasing insuline secretion
Act by increasing insuline secretion
Good evidence base, provided patient
Good evidence base, provided patient
has useful islet
has useful islet
β
β
-cell function
-cell function
May increase patient’s weight
May increase patient’s weight
First-line treatment in non-obese patients
First-line treatment in non-obese patients
who are poorly controlled by diet and
who are poorly controlled by diet and
exercise
exercise
May lead to hypoglycaemia 4 or more
May lead to hypoglycaemia 4 or more
hours after food, especially in elderly
hours after food, especially in elderly
patients
patients

Repaglinide
Repaglinide
first beta-cell mediated prandial glucose regulator
first beta-cell mediated prandial glucose regulator
allows for the rapid release of insulin from pancreatic
allows for the rapid release of insulin from pancreatic
beta-cells followed by a rapid lowering of blood glucose
beta-cells followed by a rapid lowering of blood glucose
(fast in-fast out)
(fast in-fast out)
stimulates insulin secretion from pancreatic beta
stimulates insulin secretion from pancreatic beta
cells
cells
closes ATP-sensitive potassium channels on the
closes ATP-sensitive potassium channels on the
beta cells membrane
beta cells membrane
binds to a distinct binding site from sulphonylurea
binds to a distinct binding site from sulphonylurea
compounds
compounds
In contrast to sulphonylureas, REPAGLINIDE
In contrast to sulphonylureas, REPAGLINIDE
preserves insulin biosynthesis in the pancreatic
preserves insulin biosynthesis in the pancreatic
islet cells
islet cells

Alpha-glucosidase
Alpha-glucosidase
inhibitors
inhibitors
(acarbose)
(acarbose)
Effective control of post-prandial
Effective control of post-prandial
hyperglycaemia,
hyperglycaemia,
Poorly tolerated by many patients
Poorly tolerated by many patients

Troglitazone
Troglitazone
Lowers blood glucose by improving target cell
Lowers blood glucose by improving target cell
response to insulin.
response to insulin.
Mechanism of action dependent on the
Mechanism of action dependent on the
presence of insulin.
presence of insulin.
Troglitazone decreases hepatic glucose
Troglitazone decreases hepatic glucose
output and increases insulindependent
output and increases insulindependent
glucose disposal in skeletal muscle.
glucose disposal in skeletal muscle.
Its mechanism of action is thought to involve
Its mechanism of action is thought to involve
binding to nuclear receptors (PPAR) that
binding to nuclear receptors (PPAR) that
regulate the transcription of a number of
regulate the transcription of a number of
insulin responsive genes critical for the
insulin responsive genes critical for the
control of glucose and lipid metabolism.
control of glucose and lipid metabolism.

Insulin therapy in NIDDM
Insulin therapy in NIDDM
Many of the patients have raised
Many of the patients have raised
insulin levels in their blood, giving
insulin levels in their blood, giving
more insulin may enhance the
more insulin may enhance the
development of atherosclerosis
development of atherosclerosis

Mortality
Mortality
Diabetics have excess mortality
Diabetics have excess mortality
rates –
rates –
3-fold compared with
3-fold compared with
non-diabetics. Those on insulin
non-diabetics. Those on insulin
have 5-fold excess
have 5-fold excess
Causes of death in diabetics:
Causes of death in diabetics:
–
Ischaemic heart disease
Ischaemic heart disease
–
Renal failure
Renal failure
–
Infections
Infections

Follow-up in patients with
Follow-up in patients with
diabetes
diabetes
Routine follow-up every 3-4 months
Routine follow-up every 3-4 months
Weight and blood pressure
Weight and blood pressure
Blood sugar control
Blood sugar control
Urine examination for ketones and
Urine examination for ketones and
albumin (including microalbuminuria)
albumin (including microalbuminuria)
Symptoms and signs of any
Symptoms and signs of any
complications especially vascular
complications especially vascular
disease
disease

Annual Review
Annual Review
Symptoms:
Symptoms:
–
ischaemic heart
ischaemic heart
disease,
disease,
–
peripheral vascular
peripheral vascular
disease,
disease,
–
neuropathy,
neuropathy,
–
erectile dysfunction
erectile dysfunction
Feet:
Feet:
–
footwear,
footwear,
–
deformity / joint
deformity / joint
rigidity,
rigidity,
–
poor skin condition,
poor skin condition,
–
ischaemia,
ischaemia,
–
ulceration,
ulceration,
–
absent pulses,
absent pulses,
–
sensory impairment
sensory impairment
Annual Review
Annual Review
Annual Review
Eyes:
Eyes:
–
visual acuity
visual acuity
–
retinal review
retinal review
Kidney damage:
Kidney damage:
–
albumin excretion
albumin excretion
–
serum creatinine
serum creatinine

Annual Review
Annual Review
•
Arterial risk:
•
blood glucose,
•
blood pressure,
•
blood lipids,
•
smoking
•
Attendance: podiatry / ophthalmology
/ other

Morbidity
Morbidity
Complications of the diabetes are
Complications of the diabetes are
related to
related to
Degree of control
Degree of control
Duration of disorder
Duration of disorder
Type of diabetes
Type of diabetes
Age of diabetic
Age of diabetic
Document Outline
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Slide 45
- Slide 46
- Slide 47
Wyszukiwarka
Podobne podstrony:
Cukrzyca bydła (diabetes mellitus bovis)
AN Increased Osteoprotegerin Serum Release Characterizes The Early Onset of Diabetes Mellitus and Ma
LECZENIE STANÓW NAGLĄCYCH W DIABETOLOGII WYNIKAJĄCYCH Z NIEDOBORU INSULINY
ref 2004 04 26 object pascal
antropomotoryka 26 2004 id 6611 Nieznany (2)
2004 07 Szkoła konstruktorów klasa II
brzuch i miednica 2003 2004 23 01
2004 06 21
dz u 2004 202 2072
Mathematics HL May 2004 TZ1 P1
Deklaracja zgodno¶ci CE 07 03 2004
biuletyn 9 2004
Prawo telekomunikacyjne 2004
więcej podobnych podstron