P5140018
Functional Correction
Tendon Correction Application Technigue
Use of tendon correction technique applied to create increased stimuli over the area of a tendon results in increased stimulation to the mechanoreceptors.
The proper application of the tendon correction techniąue will have an increased tension moderate to severe (50-75% of available tension) over the lengthof the tendon. Priortothe tendon and following the tendon the tape tension should be appropriate for an Origin to Insertion or Insertion to Origin application.

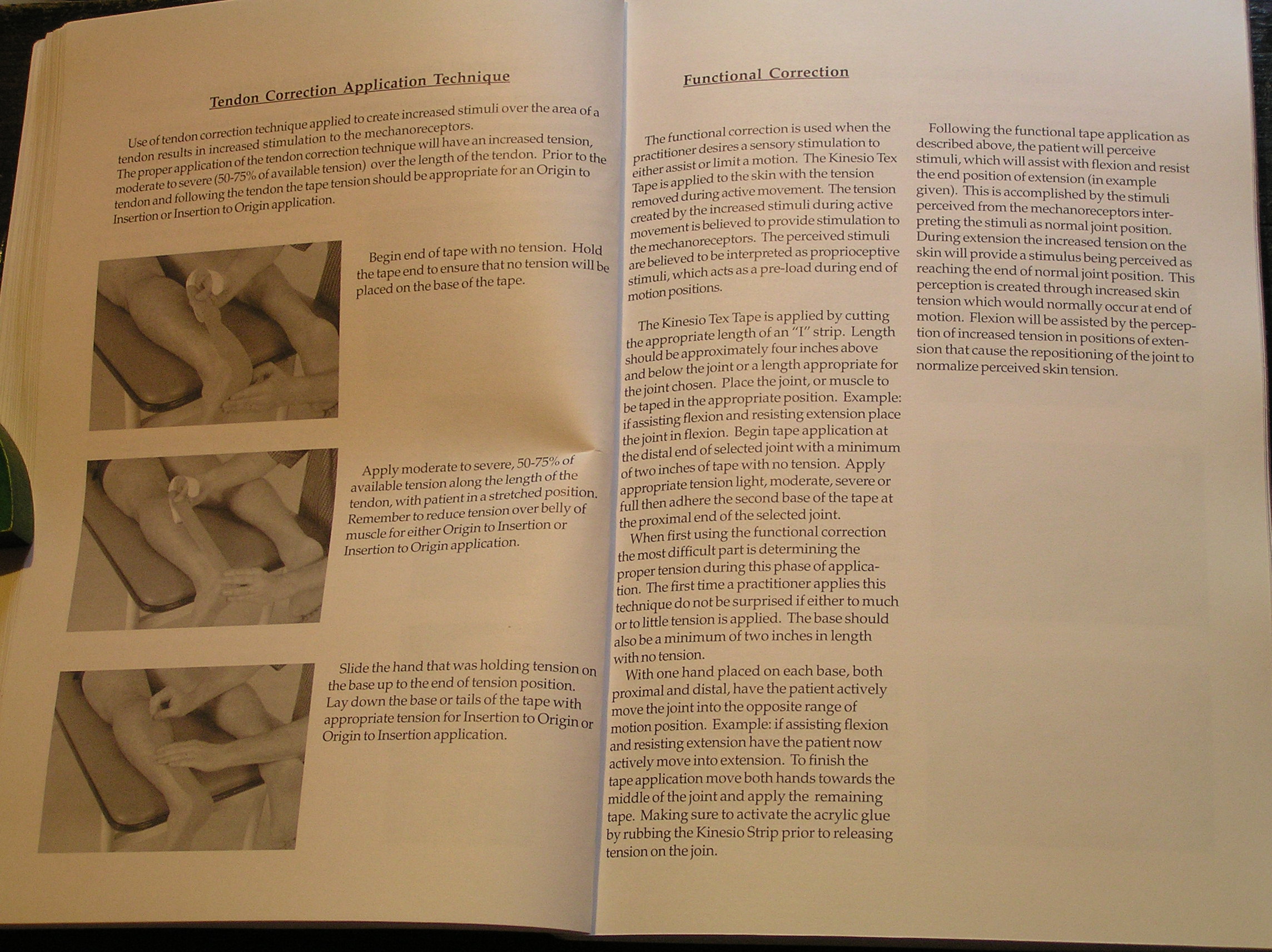
Begin end of tape with no tension. Hołd the tape end to ensure that no tension will be placed onthebaseof the tape.

Slide the hand that was holding tension on the base up to the end of tension position. Lay down the base or tails of the tape with appropriate tension for Insertion to Origin or Origin to Insertion application.
8

Apply moderate to severe, 50-75% of available tension along the length of the • tendon, with patient in a stretched posihon. Remember to reduce tension over belly of muscle foreither Origin to Insertion or Insertion to Origin application.
The functional correction is used when the practidoner desires a sensory stimulation to eitherassistorlimitamotion. TheKinesioTex Tape is applied to the skin with the tension removed during active movement. The tension created by the increased stimuli during active movement is believed to provide stimulation to the mechanoreceptors. The perceived stimuli are believed to be interpreted as proprioceptive stimuli, which acts as a pre-load during end of motionpositions.
The Kinesio Tex Tape is applied by cutting the appropriate length of an "I" strip. Length should be approximately four inches above and below the joint or a length appropriate for the joint chosen. Place the joint, or muscle to be tapedin the appropriate position. Example: if assisting flexion and resisting extension place the joint in flexion. Begin tape application at the distal end of selected joint with a minimum of two inches of tape with no tension. Apply appropriate tension light, moderate, severe or fuli then adhere the second base of the tape at the proximal end of the selected joint.
When first using the functional correction the most difficult part is determining the proper tension during this phase of application. The first time a practitioner applies this techniąue do not be surprised if either to much or to little tension is applied. The base should also be a minimum of two inches in length with no tension.
With one hand placed on each base, both proximal and distal, have the patient actively move the joint into the opposite rangę of motion position. Example: if assisting flexion and resisting extension have the patient now activelymoveintoextension. Tofinishthe tape application move both hands towards the middle of the joint and apply the remaining tape. Making surę to activate the acrylic glue by rubbing the Kinesio Strip prior to releasing tension on the join.
Following the functional tape application as described above, the patient will perceive stimuli, which will assist with flexion and resist the end position of extension (in example given). This isaccomplished by the stimuli perceived from the mechanoreceptors inter-preting the stimuli as normal joint position. During extension the increased tension on the skin will provide a stimulus being percei ved as reaching the end of normal joint position. This perception is created through increased skin tension which would normally occur at end of motion. FlexionwiU be assisted by the perception of increased tension in positions of exten-sion that cause the repositioning of the joint to normalize perceived skin tension.
Wyszukiwarka
Podobne podstrony:
P5140019 Functional Correction Application Technigno Use of functional correction techniąue to assis
P5140015 The space correction is applied to create more space directly above an area of pain, i
lnnovative use of information from CRM systems to create strategie actions of companies on the marke
lnnovative use of Information from CRM systems to create strategie actions of companies on the marke
lnnovative use of Information from CRM systems to create strategie actions ofcompanies on the market
lnnovative use of Information from CRM systems to create strategie actions ofcompanies on the market
25 lnnovative use of Information from CRM systems to create strategie actions ofcompanies on the
Factsheet: Belgium - FlandersCurrent use of EPCs and potential links to iBRoad The Belgian Region of
- 3 - Another feature of th© "Austrian way" was th© use of incomes policy in order to prev
P5140006 Table of Contents Introduction Corrective Application Techniques Mechanical Correction
P5140007 INTRODUCTFON The Corrective Application Techniques are a continuation in the development of
P5140012 Mechanical Correction Application Technigues Application of Y Technigue Application of Y Te
P5140014 Fascła Correction Application Techniąue Useof faseta correction technigue to reposition fas
więcej podobnych podstron