P5140036
ą^iraHon oLKines^ V ,, .
of mtemal rotattoS1
by ^oftbe Kinesio Y strip on thc post^C1
^rofhumerus. ł\
. « »Ke patient supine wilh their should*,. •
Plt^bduction and extema\ rotadon as pa^* %^ortallows. Providmg support to lirnl, p^
pain-
. 10-20% of available tensionto^ s^pply otuy g tails. The superior taił s\^ he Kinesio d.aviele and endouthester*,
sUg^tlybeio
•phe inferior taił should foUow ^ ■ yicular )oinJ H peCtoralis major to the costoęfcJ
yerfibersofthep
fSi . ■!____
Bicipital Tenosynovitis
Bidpital tenosynovitis is an inflammation between the long head of the biceps tendon and the sheath which surrounds it. The inflammation most commonly occurs where the biceps tendon crosses under the transverse humerał ligament as it passes through the bicipital groove of the humerus. This condition is most commonly seen in overhead motion activities: tennis, baseball/ volleyball, and javelin.
The Kinesio taping method will assist in reducing inflammation and pain. Bicipital tensosynovitis is generally also associated with rotator cuff impingement or tendonitis.

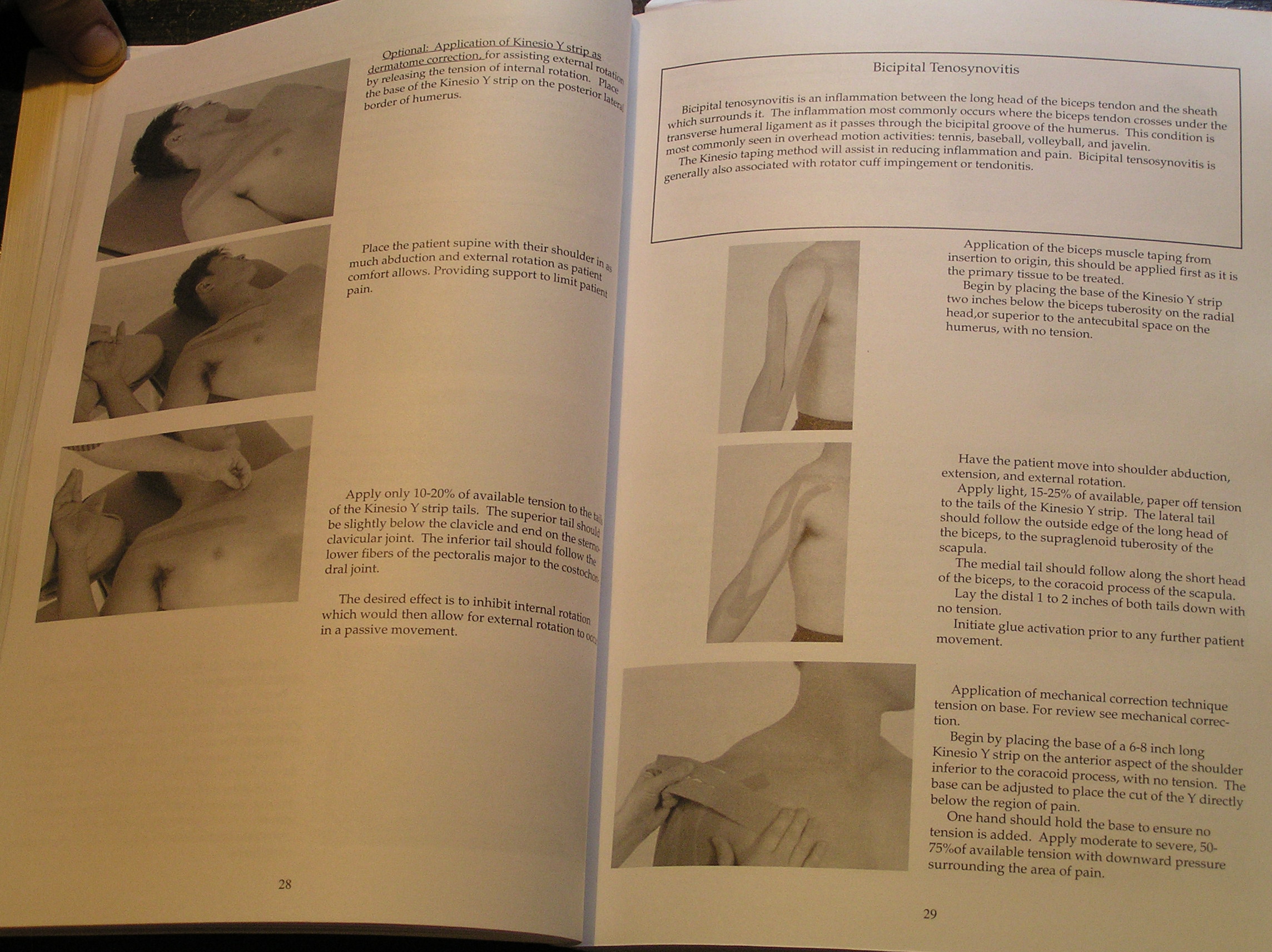
Application of the biceps musde taping from insertion to origin, this should be applied first as it is the primary tissue to be treated.
Bogiń by placing the base of the Kinesio Y strip two inches below the biceps tuberosity on the radial head/Or superior to the antecubital space on the humeruS/ with no tension.
Ha ve the patient move into shoulder abduction, extension, and extemal rotation.
Apply light, 15-25% of available/ paper off tension to the tails of the Kinesio Y strip. The iateral taił should follow the outside edge of the long head of the biceps, to the supraglenoid tuberosity of the scapula.
The medial taił should follow along the short head of the biceps, to the coracoid process of the scapula.
Lay the distal 1 to 2 inches of both tails down with no tension.
Initiate glue activation prior to any further patient movement.
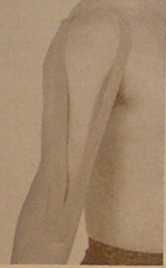
Application of mechanical correction technique tension on base. For review see mechanical correction.
Begin by placing the base of a 6-8 inch long Kinesio Y strip on the anterior aspect of the shoulder inferior to the coracoid process, with no tension. The base can be adjusted to place the cut of the Y directly below the region of pain.
One hand should hołd the base to ensure no tension is added. Apply moderate to severe, 50-75%of available tension with downward pressure surrounding the area of pain.
29
Wyszukiwarka
Podobne podstrony:
Research Papers 1 Characteńzation of PF ńngs by the finite topology on duals of R
3 6 Yeronica Franco FIGURĘ 4 A portrait of Yeronica Franco by Jacopo Tintoretto. Gil on canvas, sixt
image001 (From The Geography of Calamity: Geopolitics of Humań Dieback, by J. Holdren) Attributable
image001 RAIDERS of theSOLAR FRONTIER By A. BERTRAM CHANDLER Orły one QfOup of delendoit itood botwo
image002 A Novel of the Futurę by
kolibry w malwach (2) Next, add the details as descnbed, using the number of strands indicated by th
JPRS-UMS-92-003 16 March 1992ANALYSIS, TESTING 15 of sequential loading, the amount of damage incurr
17. Ferma duo to deposltlon of minerał salta by he&ted underground water 1. Co
więcej podobnych podstron