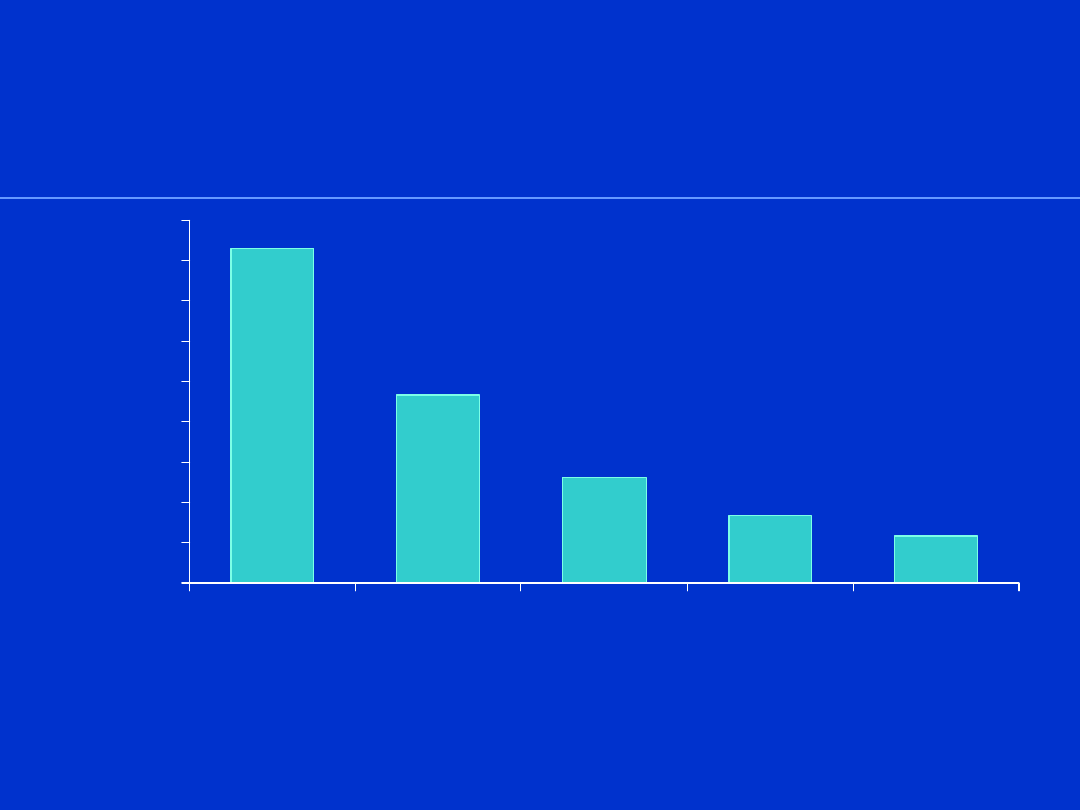
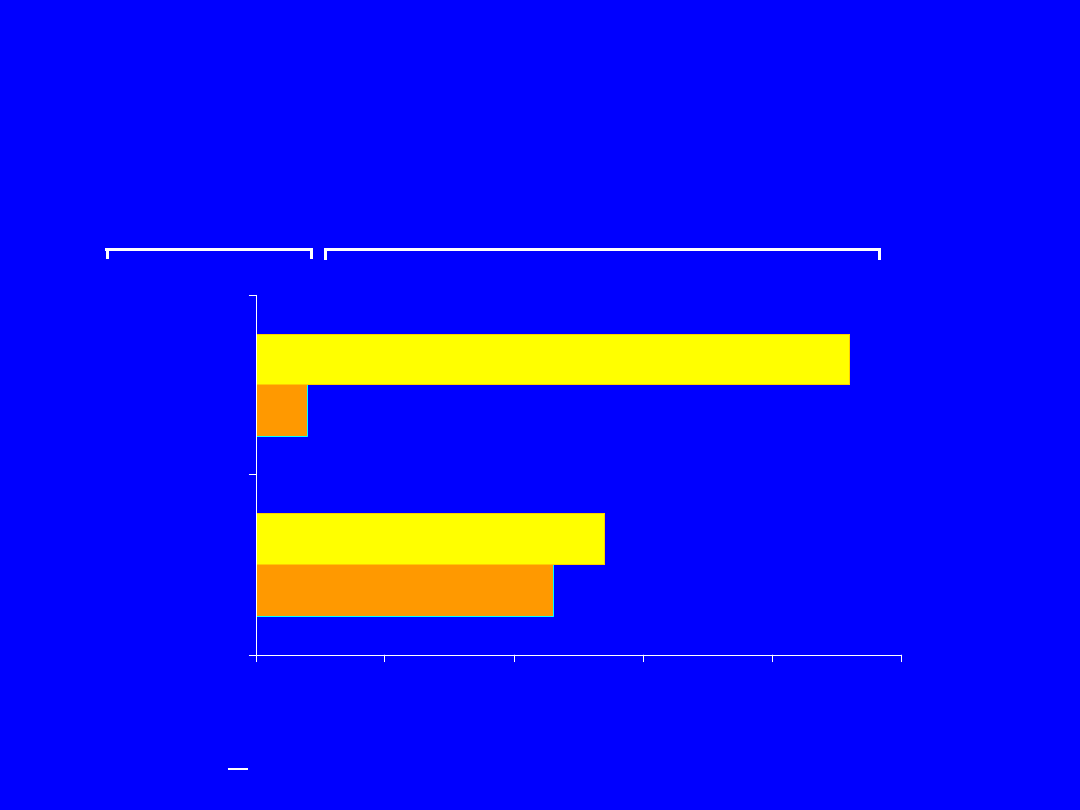
Kessler et al. Arch Gen Psychiatry. 1995;52:1048.
Kessler et al. Arch Gen Psychiatry. 1994;51:8.
0
3
6
9
12
15
18
21
24
27
Any Anxiety
Disorder
Social
Anxiety
Disorder
PTSD
Generalized
Anxiety
Disorder
Panic
Disorder
L
if
et
im
e
P
re
va
le
n
ce
(
%
)
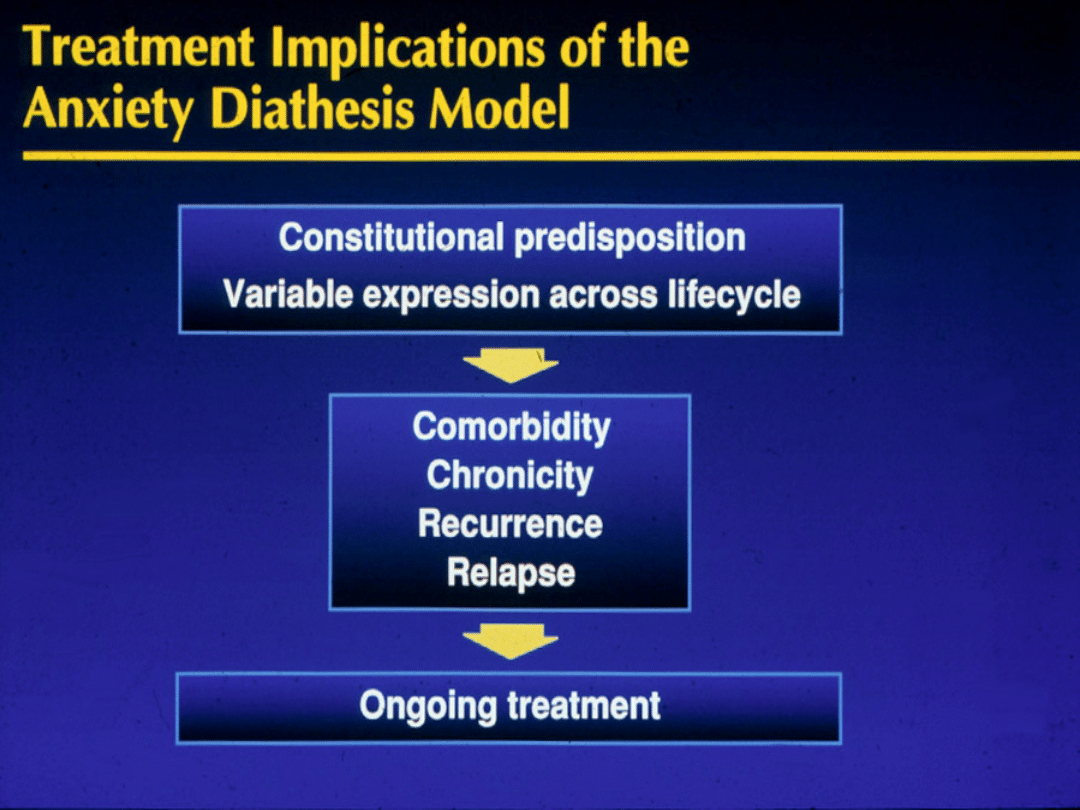
Prevalence of Anxiety
Disorders
Outcome of Panic
Disorder at Long-Term
Follow-up
Persistence of
Rate (%) Range (%)
Panic attacks
46
17-70
Phobic avoidance
69
36-82
Functional impairment
50
39-67
Roy-Byrne & Cowley, 1995
Pharmacopoeia for
Anxiety Disorders
Antidepressants
Serotonin Selective Reuptake Inhibitors (SSRIs)
Serotonin-Norepinephrine Reuptake Inhibitors (SNRIs)
Atypical Antidepressants
Tricyclic Antidepressants (TCAs)
Monoamine Oxidase Inhibitors (MAOIs)
Benzodiazepines
Other Agents
Azaspirones
Beta blockers
Anticonvulsants
Other strategies
Serotonin Selective Reuptake
Inhibitors
• Fluoxetine (Prozac), 20-80 mg/d
– Initiate with 5-10 mg/d
• Sertraline (Zoloft), 50-200 mg/d
– Initiate with 25-50 mg/d
• Paroxetine (Paxil), 20-50 mg/d
– Initiate with 10mg/d
• Fluvoxamine (Luvox), 50-300 mg/d
– Initiate with 25 mg/d
• Citalopram (Celexa)
-
Initiate with 10-20 mg/d
• Start low to minimize anxiety
Adjunctive BZD, beta blocker
Serotonin Selective
Reuptake Inhibitors (cont)
• Typical SSRI side effects:
– GI distress, jitteriness, headaches,
sleep disturbance, sexual disturbance
• Clomipramine (Anafranil), 25-250
mg/d
– Initiate with 25 mg/d
• Efficacy: PDAG, PTSD, SP, OCD,
GAD
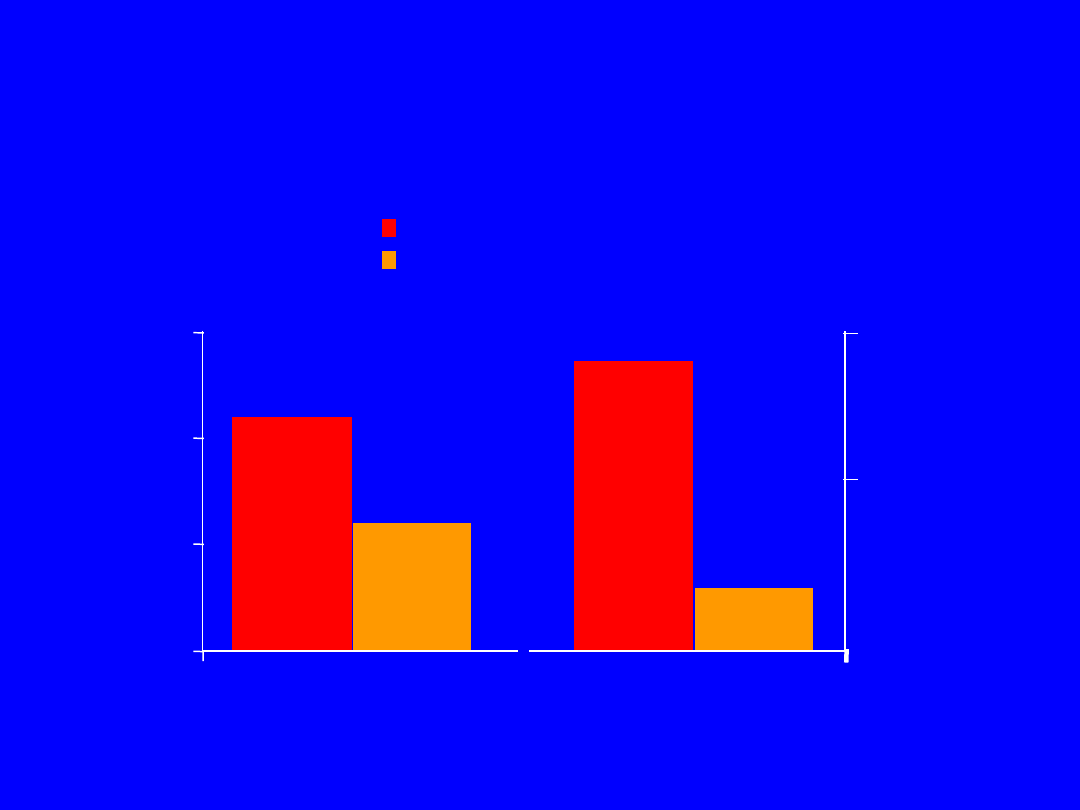
Post-treatment
Post-treatment
Brady et al. J Clin Psychiatry. 1995;56:502.
Pre-treatment
Pre-treatment
Standard
Standard
drinks/week
drinks/week
140
140
IES
IES
Alcohol use
Alcohol use
0
0
70
70
0
20
40
60
IES
IES
score
score
Sertraline In Comorbid
PTSD
And Alcoholism

Discontinuation of
Treatment for Anxiety
Disorders
• Withdrawal/rebound more common with Bzd
than other anxiolytic treatment
• Relapse: a significant problem across
treatments. Many patients require
maintenance therapy
• Bzd abuse is rare in non-predisposed
individuals
• Clinical decision: balance comfort/compliance/
comorbidity during maintenance treatment
with discontinuation-associated difficulties
Strategies for Anxiolytic
Discontinuation
• Slow taper
• Switch to longer-acting agent for
taper
• Cognitive-Behavioral therapy
• Adjunctive
– Antidepressant
– Anticonvulsant
– ?clonidine, ?beta blockers, ? buspirone
Serotonin-Norepinephrine
Reuptake Inhibitor
• Venlafaxine-XR (Effexor-XR) 75-300
mg/d
– Initiate with 37.5 mg/d
• Indicated for GAD; effective for panic
disorder, social phobia, PTSD, OCD
• Typical side effects
– GI distress, jitteriness, headaches,
sexual disturbance

Atypical
Antidepressants
• Nefazadone (300-500 mg/d)
– 5-HT reuptake inhibitor
– 5-HT2 antagonist
– Initiate with 50 mg bid
• Mirtazapine
– Limited experience to date in anxiety
disorders
Atypical Antidepressants
(cont.)
• Bupropion
– Based on limited data, considered less
effective for panic and other anxiety disorders,
but reports suggestive of efficacy for
• panic disorder
• social anxiety disorder
• PTSD
• Trazodone
– Based on limited data, considered less
effective for panic and other anxiety disorders
Tricyclic Antidepressants
• Imipramine (Tofranil)
• Nortriptyline (Pamelor)
• Desipramine (Norpramin)
• Amitriptyline (Elavil)
• Doxepin (Sinequan)
• Effective in anxiety with or without comorbid depression
• Recommended dosage 2.25 mg/kg/d Imipramine or its
equivalent for panic
• Initial anxiety worsening (Initiate with “test” dose, e.g. 10
mg/d IMI)
Tricyclic Antidepressants
(cont)
• Typical TCA side effects
– anticholinergic effects (dry mouth, blurred vision,
constipation)
– orthostatic hypotension
– cardiac conduction disturbance
– weight gain
– sexual dysfunction
• Lethal in overdose
• Weight gain and sedation often become increasingly
problematic over time
• Efficacy: PDAG, GAD, PTSD

Monoamine Oxidase
Inhibitors
• Phenelzine (Nardil) 45-90 mg/d
• Tranylcypromine (Parnate) 30-60 mg/d
• Isocarboxacid (Marplan) 10-30 mg/d
• Initial worsening of anxiety is unusual
• Side effects: light-headedness, neurological
symptoms, weight gain, sexual dysfunction, edema
• Dietary restrictions/Hypertensive crisis; “cheese
reaction”
• Risk of lethal overdose and toxicity
• Generally reserved for refractory cases
• Efficacy: PDAG, SP, OCD, PTSD
Benzodiazepines
• Potency was considered critical
determinant of anti-panic efficacy
– Alprazolam (Xanax)
– Clonazepam (Klonopin)
– +/- Lorazepam (Ativan)
• But comparable doses of diazepam as
effective as alprazolam
• All benzodiazepines effective for
generalized anxiety
Potential Benefits of
Benzodiazepine Therapy
• Effective
• Short latency of therapeutic onset
• Well tolerated
• Rapid dose adjustment feasible
• Can be used “prn” for situational
anxiety
Potential Drawbacks of
Benzodiazepine Therapy
• Initial sedation
• Discontinuation difficulties
• Potential for abuse in substance
abusers
• Not effective for comorbid
depression
Alprazolam
•Effective as AD in panic
•Advantages: rapid onset of effect, lacks typical AD
side effects
•Disadvantages: short duration of effect (i.e.,
multiple dosing, interdose rebound),
discontinuation syndromes, early relapse, abuse
potential, disinhibition
•Dosing: anticipate initial sedation (tachyphylaxis
usually develops).
•Range: 2-10 mg/d (4-6 mg/d usual) (QID dosing)
Clonazepam
• Labeled as anticonvulsant
• As effective as alprazolam for panic; issue of potency
for anti-panic efficacy
• Advantages: Pharmacokinetic: longer duration of
effect results in less frequent dosing, interdose
symptoms, early relapse, or acute withdrawal
symptoms. Slower onset of effect diminishes abuse
potential
• Disadvantages: Depression not more frequent than
with other Bzd”s; disinhibition, headaches
• Dosing: anticipate initial sedation (initiate at 0.25-0.5
mg qhs)
• Range: 1-5 mg/d (BID dosing)
Combining
Antidepressants
with Benzodiazepines
• Provides rapid anxiolysis during
antidepressant lag
• Decreases early anxiety associated
with initiation of antidepressant
• Treats residual anxiety wtih
antidepressant treatment
• Prevents and treats depression on
benzodiazepines
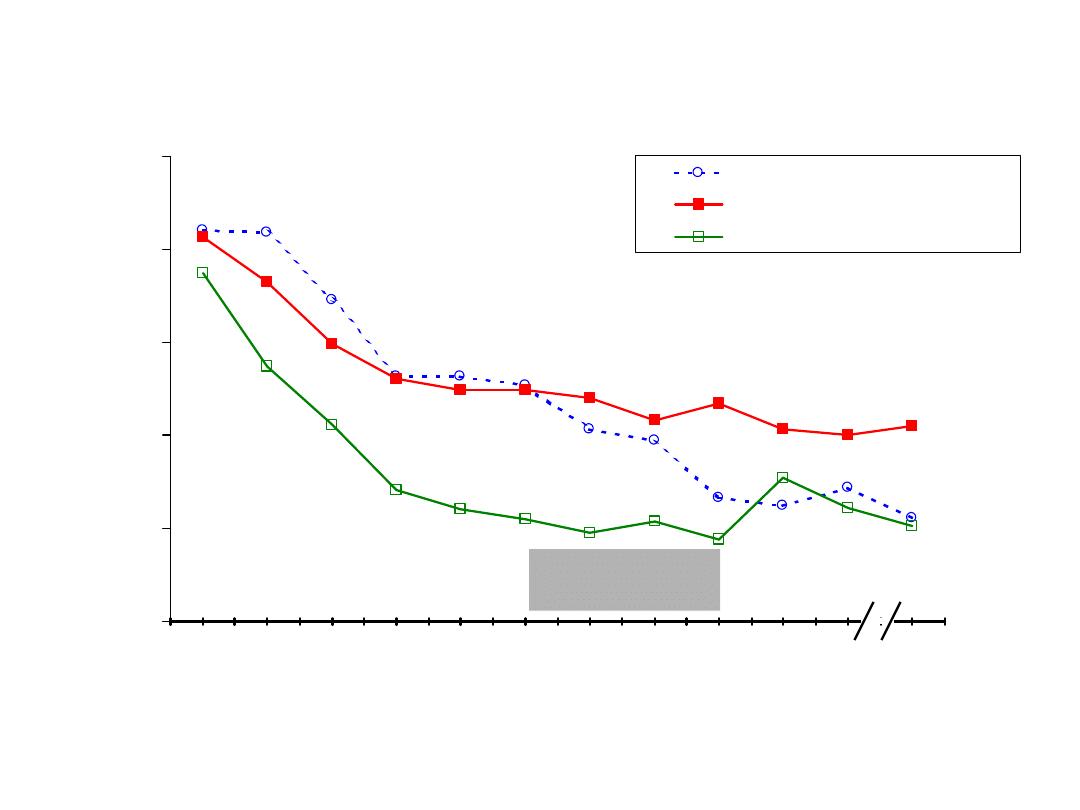
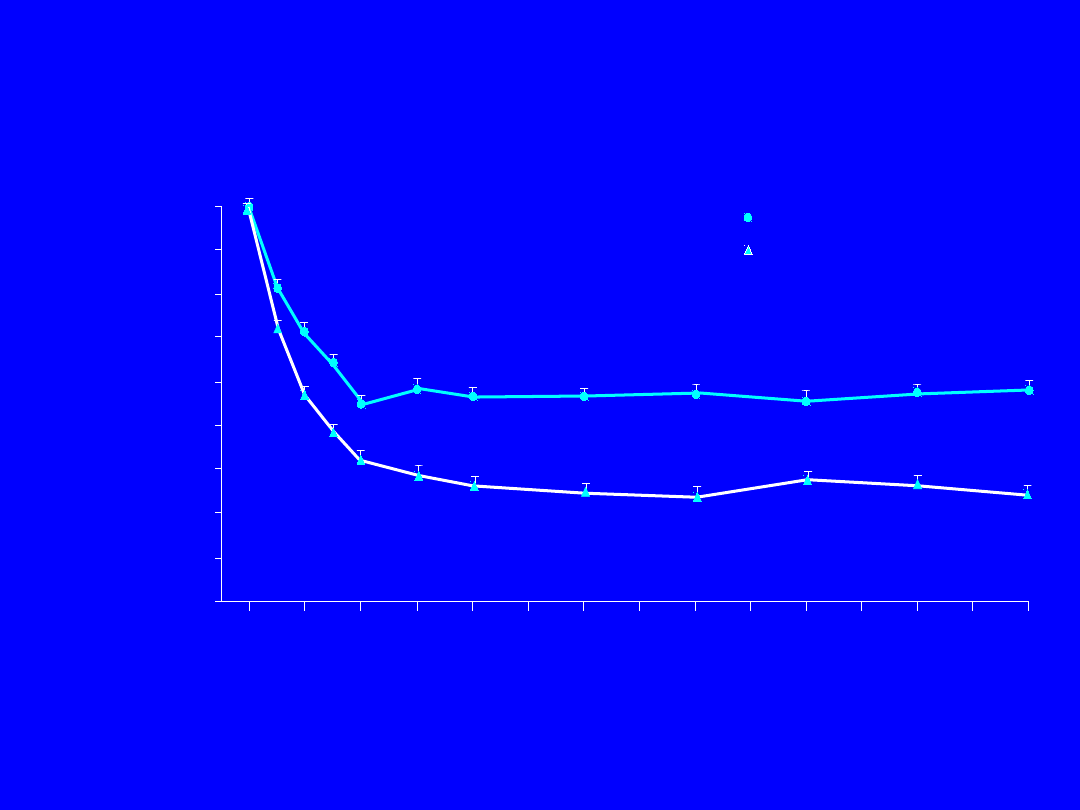
End-Point (LVCF) Analysis of Panic Disorder Severity
Scale Scores for Each Group
0
0.5
1
1.5
2
2.5
Week
00
Week
01
Week
02
Week
03
Week
04
Week
05
Week
06
Week
07
Week
08
Week
09
Week
10
Week
12
A
ve
ra
ge
P
D
SS
s
co
re
s
Paroxetine + Placebo
Paroxetine + Clonazepam
Paroxetine + Clonazepame w/taper
†
*
*
*
*
* Together the Clonazepam groups differ from the Placebo group at p< .05
† Clonazepam groups differ from each other at p<.05
Clonazepam
Taper Phase
Pollack, et al 2001

Buspirone
• Non-benzodiazepine anxiolytic
• Non-sedating, muscle relaxant,
anticonvulsant
• Effects on serotonin and dopamine receptors
• Indicated for GAD; weak antidepressant
effects
• Useful as SSRI augmentation for panic, social
phobia, depression, sexual dysfunction
• Dosing: 30-60 mg/d
Beta Blockers
• Decrease autonomic arousal
• May be useful as adjunct for somatic
symptoms of panic and GAD but not
as primary treatment
• Useful for non-generalized social
phobia, performance anxiety subtype
• Propranolol 10-60 mg/d; Atenolol 50-
150 mg/d

Anticonvulsants
• Valproate and gabapentin effective
for non-ictal panic
• Gabapentin effective for social phobia
• Gabapentin (600-5400 mg/d) used as
alternative to benzodiazepine
• Valproate, Carbamazepine,
Gabapentin, Topiramate and
Lamotrigine for PTSD

Strategies for Refractory
Anxiety Disorder
• Maximize dose
• Combine antidepressant and
benzodiazepine
• Administer cognitive-behavioral
therapy
• Attend to psychosocial issues
.

Strategies for Refractory
Anxiety Disorders
• Augmentation
– Anticonvulsants
• Gabapentin
• Valproate
• Topiramate
– Beta blocker
– Buspirone
– Clonidine/Guanfacin
e
– Pindolol
– D
opaminergic agonists
(e.g., Ropinirole) for
social phobia
– Cyproheptadine
• Combined
SSRI/TCA
• Alternative
antidepressant
– Clomipramine
– MAOI
• Other
– Inositol
– Kava-kava
– Atypical
neuroleptics
Cognitive-Behavioral
Therapy for Anxiety
Disorders
• CBT useful alone or in combination with
medication for
– Refractory symptoms
– Persistent cognitive factors, behavioral patterns and
anxiety sensitivity
– Comorbid conditions
– Early intervention for PTSD prophylaxis
• CBT may be provided by therapist or self-
administered
(
TherapyWorks manuals 800-228-
0752///http://www.psychcorp.com)
• CBT may facilitate medication discontinuation
.
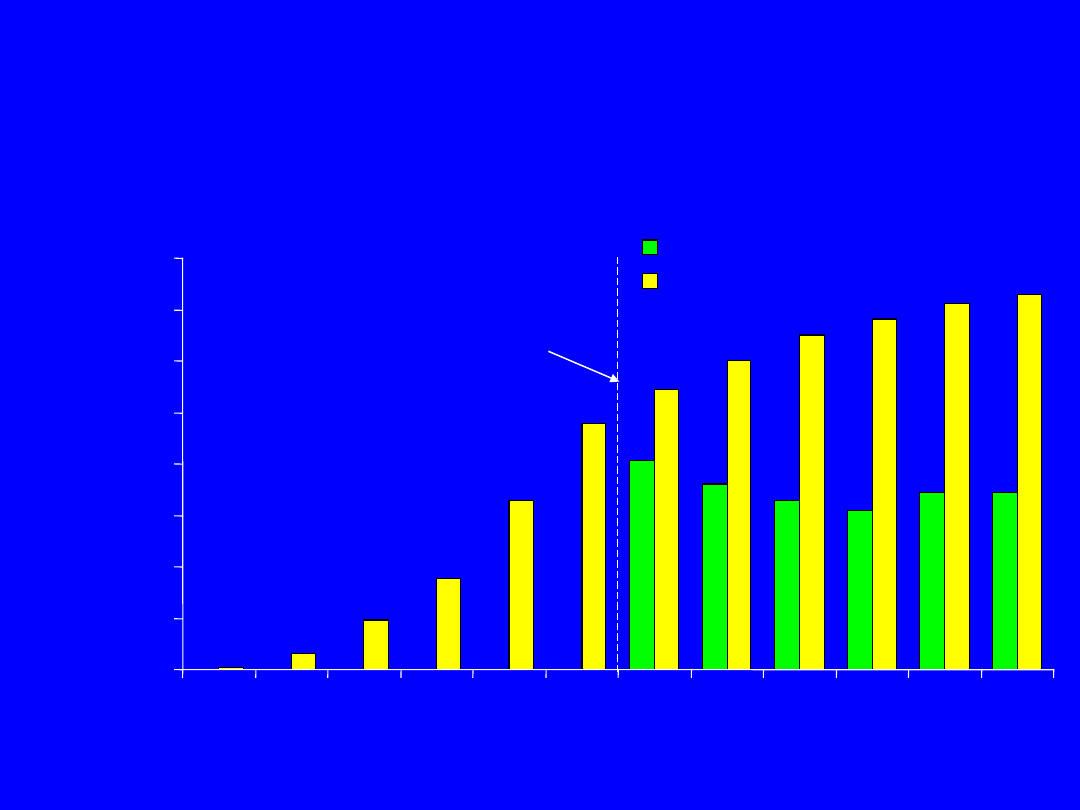
Responder = > 30% decrease CAPS and CGI-S = 1 or 2
Londborg et al. J Clin Psychiatry, in press.
46%
8%
54%
92%
0%
20%
40%
60%
80%
100%
Acute Phase
Responders
Sustained
Response
Converted to responder
Acute Phase
Responder Status
Continued
Continued
non-response
non-response
Lost response
Continuation Phase
Responder Status
Continuation Phase Outcome with
Sertraline Treatment of PTSD Based
on
Acute Phase Response Category
Acute Phase
Non-responders
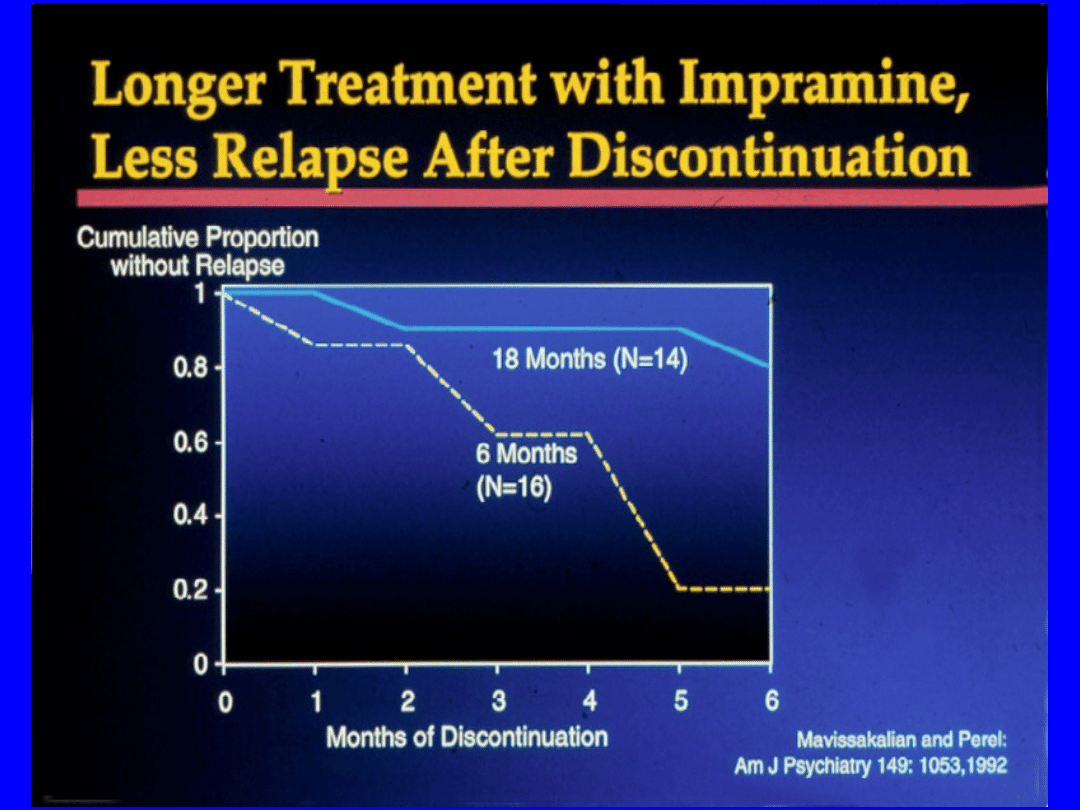
Long-Term Treatment
Of GAD
• Need to treat long-term
• Full relapse in approximately 25% of
patients 1 month after stopping treatment
• 60%-80% relapse within 1st year after
stopping treatment
Hales et al. J Clin Psychiatry. 1997;58(suppl 3):76.
Rickels et al. J Clin Psychopharmacol. 1990;10(3 suppl):101S.
Effect Of Venlafaxine On
Total
HAM-A Scores
0
-2
-4
-6
-8
-10
-12
-14
-16
-18
0
2
4
6
8
10 12 14 16 18 20 22 24 26 28
Week Of Treatment
Change In
Mean HAM-
A Total
Score
Placebo (N=123)
Venlafaxine XR (N=115)
P<.001 for venlafaxine XR vs placebo for all study weeks except week 1 (.003), week 4 (.002), and
week 20 (.007)
Venlafaxine XR doses: 75 to 225 mg/d.
Gelenberg et al. JAMA. 2000;283:3082.
Placebo (N=274)
Paroxetine (N=285)
*
*
*
*
*
*
Paroxetine 20-50 mg
(N=599 responders)
0
10
20
30
40
50
60
70
80
Patients
(%)
Paroxetine Long-Term GAD
Treatment
% Remission
*P<.01 vs placebo.
Remission = HAM-A 7; LOCF dataset.
GlaxoSmithKline data on file, 2001.
Randomization
Week
Phase I: Single-Blind
Phase II: Double-Blind
1
2
3
4
6
8
12
16
20
24
28
32

Discontinuation of
Treatment for Anxiety
Disorders
• Withdrawal/rebound more common with Bzd
than other anxiolytic treatment
• Relapse: a significant problem across
treatments. Many patients require
maintenance therapy
• Bzd abuse is rare in non-predisposed
individuals
• Clinical decision: balance comfort/compliance/
comorbidity during maintenance treatment
with discontinuation-associated difficulties
Strategies for Anxiolytic
Discontinuation
• Slow taper
• Switch to longer-acting agent for
taper
• Cognitive-Behavioral therapy
• Adjunctive
– Antidepressant
– Anticonvulsant
– ?clonidine, ?beta blockers, ? buspirone
Document Outline
- Prevalence of Anxiety Disorders
- Outcome of Panic Disorder at Long-Term Follow-up
- Slide 3
- Slide 4
- Slide 5
- Pharmacopoeia for Anxiety Disorders
- Serotonin Selective Reuptake Inhibitors
- Serotonin Selective Reuptake Inhibitors (cont)
- Sertraline In Comorbid PTSD And Alcoholism
- Discontinuation of Treatment for Anxiety Disorders
- Strategies for Anxiolytic Discontinuation
- Serotonin-Norepinephrine Reuptake Inhibitor
- Atypical Antidepressants
- Atypical Antidepressants (cont.)
- Tricyclic Antidepressants
- Tricyclic Antidepressants (cont)
- Monoamine Oxidase Inhibitors
- Benzodiazepines
- Potential Benefits of Benzodiazepine Therapy
- Potential Drawbacks of Benzodiazepine Therapy
- Alprazolam
- Clonazepam
- Combining Antidepressants with Benzodiazepines
- Slide 24
- Buspirone
- Beta Blockers
- Anticonvulsants
- Strategies for Refractory Anxiety Disorder
- Strategies for Refractory Anxiety Disorders
- Cognitive-Behavioral Therapy for Anxiety Disorders
- Slide 31
- Continuation Phase Outcome with Sertraline Treatment of PTSD Based on Acute Phase Response Category
- Long-Term Treatment Of GAD
- Effect Of Venlafaxine On Total HAM-A Scores
- Paroxetine Long-Term GAD Treatment % Remission
- Slide 36
- Slide 37
Wyszukiwarka
Podobne podstrony:
Pollack [Po Galicji (o Chasydach, HUCUŁACH, POLAKACH I RUSINACH)
Rachel Pollack Unquenchable Fire
Rachel Pollack Unquenchable Fire
Pollack, Freda Humor, learning, and socialization in middle level classrooms
Connectionism Past, Present, and Future [jnl article] J Pollack WW
Rachel Pollack Immortal Snake
The Fool the Stick and the Pr Rachel Pollack
Frank Lillie Pollack Finis
Pollack Religiousness inside and outside the Church
Temporary Agency Rachel Pollack
więcej podobnych podstron