
Treatment with
blood products
Mirosław Franków
Department of Hematology
Pomeranian Medical
University
BLOOD
COMPONEN
TS
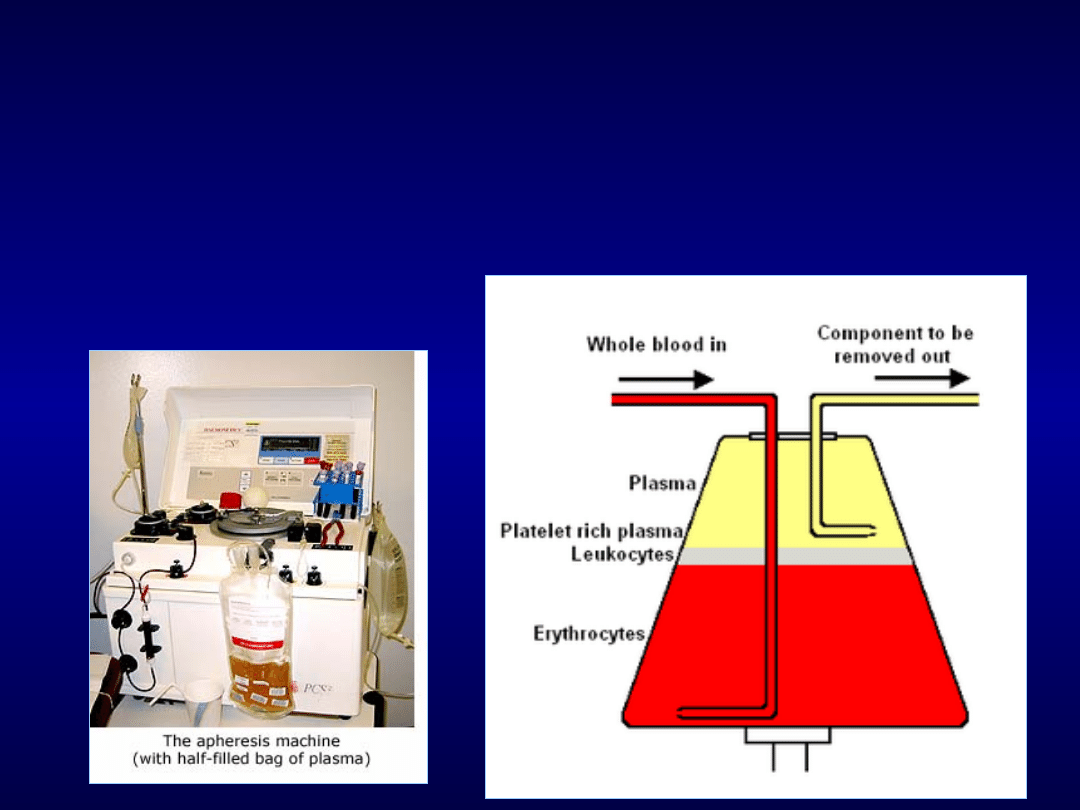
Apheresis
Whole blood enters the centrifuge on
the left and separates into layers so that
selected components can be drawn off
on the right.

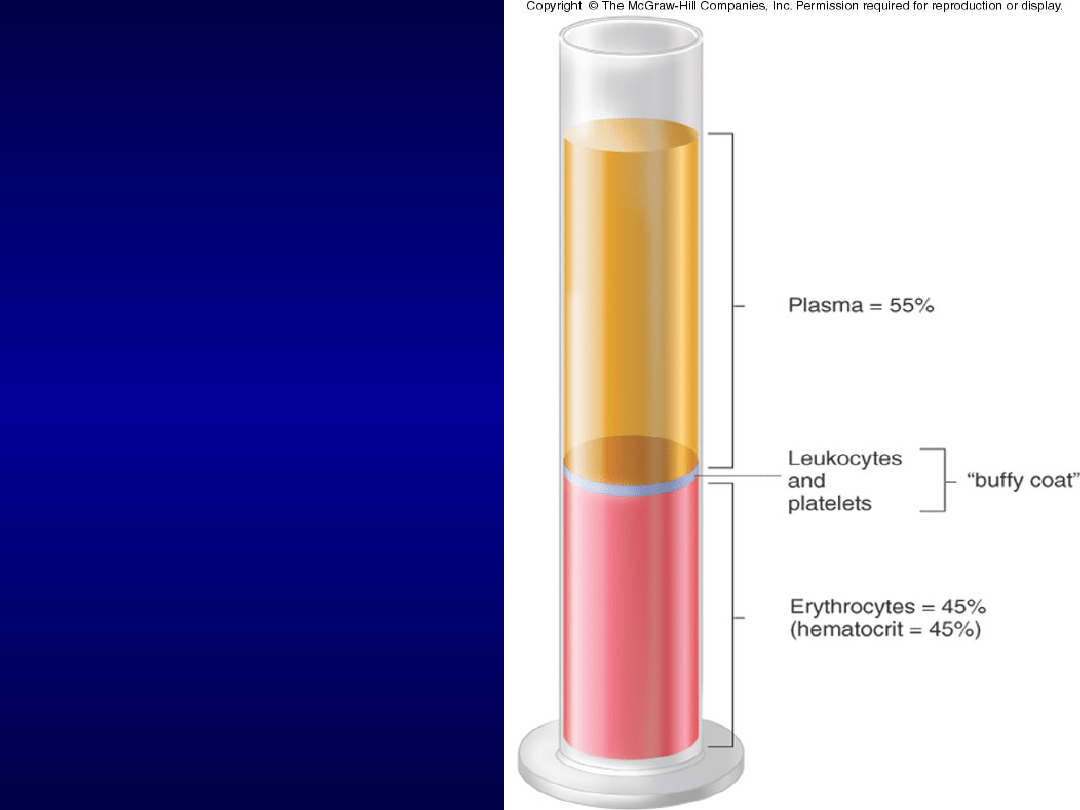
BLOOD COMPONENTS
Blood separated into
different parts:
Packed red cells
Packed red cells
Platelets
Platelets
Fresh frozen plasma
Fresh frozen plasma
Cryoprecipitate
Cryoprecipitate
Granulocytes
Granulocytes
Factor IX conc.
Factor IX conc.
Factor VIII conc
Factor VIII conc
.
.

Blood
Blood
component
component
Contents
Contents
Volume
Volume
Shelf life
Shelf life
Whole blood
Whole blood
Hct.35%,RBCs,
Hct.35%,RBCs,
WBCs.450ml
WBCs.450ml
blood,63ml
blood,63ml
CPDA1
CPDA1
520ml
520ml
35 days at
35 days at
4deg.C.
4deg.C.
Red cells
Red cells
Hct.60%,RBCs,25mlpla
Hct.60%,RBCs,25mlpla
sma,
sma,
100 ml Adsol.
100 ml Adsol.
340ml
340ml
42 days at
42 days at
4deg.C
4deg.C
Platelets
Platelets
Platelets,
Platelets,
few
few
WBCs,
WBCs,
RBCs,
RBCs,
50ml plasma
50ml plasma
50ml
50ml
5 days at
5 days at
22deg.C
22deg.C
FFP
FFP
Cryoppt.
Cryoppt.
Pl.
Pl.
proteins,
proteins,
clot.
clot.
Factors
Factors
Fibrinogen,factor
Fibrinogen,factor
VIII,IX.
VIII,IX.
225ml
225ml
15ml
15ml
1year at
1year at
-18deg.C
-18deg.C

Obtaining the Blood or
Component
•
Hospital employee obtaining blood/component
Hospital employee obtaining blood/component
from Transfusion Medicine must state the
from Transfusion Medicine must state the
patient’s name and hospital (unique) number.
patient’s name and hospital (unique) number.
•
An ‘issue report’ will be given to them along
An ‘issue report’ will be given to them along
with the blood/component.
with the blood/component.
•
Blood and components are to be infused
Blood and components are to be infused
immediately when received on the ward.
immediately when received on the ward.
•
If unable to do so, the product must be
If unable to do so, the product must be
returned to Transfusion Medicine.
returned to Transfusion Medicine.
•
Blood that is out of approved storage for
Blood that is out of approved storage for
longer than 30 minutes
longer than 30 minutes
MUST NOT
MUST NOT
be
be
transfused.
transfused.

Blood Component
Verification
P
P
hysician
hysician
must verify the blood component
must verify the blood component
with
with
issue report:
issue report:
•
The blood component
The blood component
•
The blood component unit number
The blood component unit number
•
Group and Rh of the blood
Group and Rh of the blood
component
component
A visual assessment of the blood unit should
A visual assessment of the blood unit should
be performed.
be performed.
Visual Assessment of
Blood
Is the seal secure and leak free?
Is there
hemolysis?
Is the
plasma
pink?
Are the red
cells red or are
they purple or
black?
Are there any
large clots
visible?
There should be no leakage, visible clots or hemolysis.
Red cells should be a normal color. If any abnormality
is noted, this should be reported to Transfusion
Medicine.

Patient Verification
Compare the patient’s name and
Compare the patient’s name and
hospital unique number on their ID
hospital unique number on their ID
armband with the blood/component
armband with the blood/component
label and the issue report.
label and the issue report.
The
The
P
P
hysician must sign the issue
hysician must sign the issue
report.
report.
In case of any discrepancy:
In case of any discrepancy:
blood/component must NOT be transfused
blood/component must NOT be transfused

Frequency of Transfusion
Adverse Events
Transfusion Associated Circulatory Overload
Transfusion Associated Circulatory Overload
1:200
1:200
TRALI
TRALI
1:5000
1:5000
ABO incompatible transfusion
ABO incompatible transfusion
1
1
:
:
30000-
30000-
60000
60000
Severe anaphylactoid reaction
Severe anaphylactoid reaction
1:20000
1:20000
GVHD/Post Transfusion Purpura
GVHD/Post Transfusion Purpura
1:750000 to
1:750000 to
1:1million
1:1million
Frequency of Transfusion
Adverse Events
Virus
Virus
Risk per Unit
Risk per Unit
Transfusion
Transfusion
Transmission
Transmission
Rate
Rate
Window
Window
Period
Period
HIV 1&2
HIV 1&2
1:2,135,000
1:2,135,000
90%
90%
11 days
11 days
HCV
HCV
1:1,935,000
1:1,935,000
90%
90%
10 days
10 days
HBV
HBV
1:205,000
1:205,000
70%
70%
59 days
59 days
HTLV
HTLV
1:3,000,000
1:3,000,000
30%
30%
51 days
51 days
WNV
WNV
1:10,000 to
1:10,000 to
1,000
1,000
(prior to NAT)
(prior to NAT)
Unknown
Unknown
-
-
Parvo B19
Parvo B19
1:40,000 to
1:40,000 to
3,000
3,000
Low
Low
-
-
Hepatitis
Hepatitis
A/E
A/E
1:1,000,000
1:1,000,000
Low
Low
-
-

Blood Testing
Syphilis
Syphilis
HIV 1
HIV 1
HIV 2
HIV 2
Human T-lymphotrophic virus 1 (HTLV-1)
Human T-lymphotrophic virus 1 (HTLV-1)
Hepatitis B surface antigen (HbsAg)
Hepatitis B surface antigen (HbsAg)
Hepatitis C virus (HCV)
Hepatitis C virus (HCV)
Alanine aminotrans
Alanine aminotrans
fer
fer
ase (ALT)
ase (ALT)
Hepatitis B core antibody (HbcAB)
Hepatitis B core antibody (HbcAB)
Surrogate marker for HIV infection
Surrogate marker for HIV infection
Surrogate marker for non-A, non-B hepatitis
Surrogate marker for non-A, non-B hepatitis
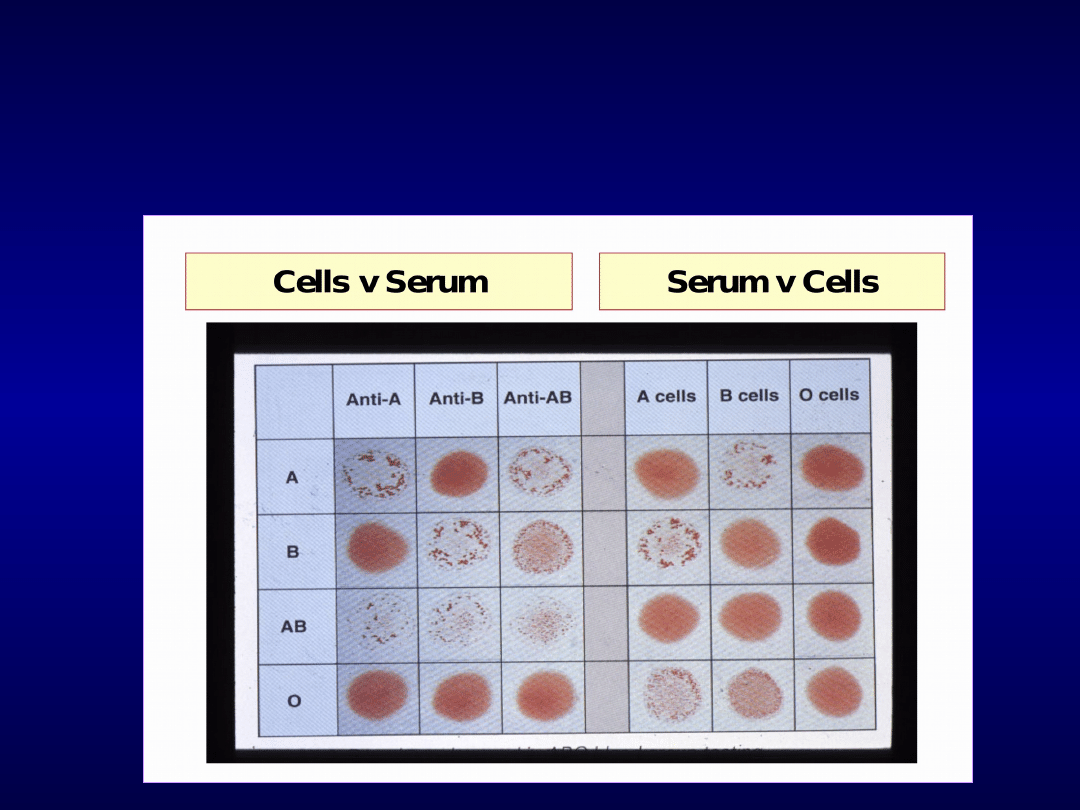
Cross-match – red cell
compatibility testing
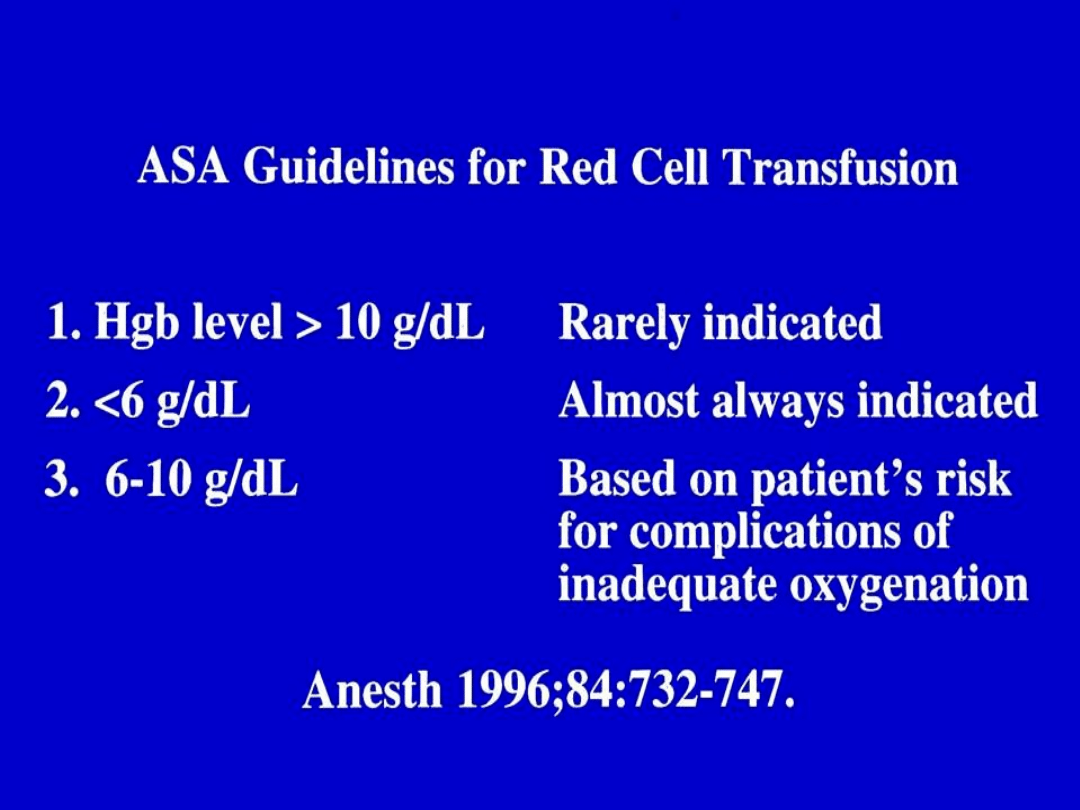
Red Cell Products
Indication: Restore oxygen carrying capacity in
Indication: Restore oxygen carrying capacity in
symptomatic anemia
symptomatic anemia
Packed Red Blood Cells
Packed Red Blood Cells
Volume: 350 ml (250 ml CPDA units)
Volume: 350 ml (250 ml CPDA units)
Hct: 50 – 60% (70 – 80% CPDA units)
Hct: 50 – 60% (70 – 80% CPDA units)
Whole Blood
Whole Blood
Also replaces volume loss
Also replaces volume loss
Volume: 500 ml
Volume: 500 ml
Dose: 1 unit should raise the Hgb 1g/dl
Dose: 1 unit should raise the Hgb 1g/dl
(Hct 2-3%)
(Hct 2-3%)
Shelf-life: 35 – 42 days
Shelf-life: 35 – 42 days

Red Cell Products
Irradiated
Irradiated
(
( irradiation inactivates donor
lymphocytes, reduce risk for GVHD)
Washed
Washed
(
(Removes plasma proteins; Risk of
allergic reactions may be reduced)
Leukocytes Reduced
Leukocytes Reduced
(
(Risk of febrile
reactions, HLA alloimmunization, and
CMV infection reduced)
MODIFIED PRODUCTS
MODIFIED PRODUCTS

Rapid development of
anemia needing
transfusion
Massive hemorrhage
Massive hemorrhage
hemolytic/aplastic crises
hemolytic/aplastic crises
Autoimmune haemolysis - often
Autoimmune haemolysis - often
elderly but even young patients may
elderly but even young patients may
require transfusion in this setting
require transfusion in this setting
Delayed haemolytic transfusion
Delayed haemolytic transfusion
-SHOT -Delays in providing blood
-SHOT -Delays in providing blood
cause of death
cause of death
not
not
hemolysis
hemolysis

Iron overload and
chelation
Can occur in any patient requiring
Can occur in any patient requiring
chronic transfusion therapy or in
chronic transfusion therapy or in
hemochromatosis.
hemochromatosis.
Liver biopsy is the most accurate
Liver biopsy is the most accurate
test though MRI is being
test though MRI is being
investigated.
investigated.
Ferritin is a good starting test.
Ferritin is a good starting test.
Chelator, deferoxamine
Chelator, deferoxamine
Platelet Products
Indications:
Indications:
Correct bleeding due to thrombocytopenia or
Correct bleeding due to thrombocytopenia or
platelet dysfunction
platelet dysfunction
Prevent bleeding in critical thrombocytopenia
Prevent bleeding in critical thrombocytopenia
Platelet Concentrates (PCs)
Platelet Concentrates (PCs)
Volume:
Volume:
1 unit =
1 unit =
50 ml (majority is plasma)
50 ml (majority is plasma)
Dose: Approximately 1 unit/10kg (Adults, pool of
Dose: Approximately 1 unit/10kg (Adults, pool of
six units)
six units)
Shelf-life:
Shelf-life:
5 days (7 days with additional testing)
5 days (7 days with additional testing)
4 hrs if pooled
4 hrs if pooled
PLATELET PRODUCTS
Contain platelets,
Contain platelets,
plasma, and WBC from
plasma, and WBC from
4-8 donors
4-8 donors
Pooled
Pooled
Platelets
Platelets
Pooled
Pooled
Platelets
Platelets
Contain platelets,
Contain platelets,
plasma, and WBC from
plasma, and WBC from
one donor
one donor
Apheresis
Apheresis
Platelets
Platelets
Apheresis
Apheresis
Platelets
Platelets

PLATELET PRODUCTS
MODIFIED PRODUCTS
MODIFIED PRODUCTS
•
Irradiated
Irradiated
•
Washed
Washed
•
Leukocytes Reduced
Leukocytes Reduced
Platelet Therapy
Count
Count
Risk of Major
Risk of Major
Bleed
Bleed
>10,000/ul
>10,000/ul
Low
Low
5-10,000/ul
5-10,000/ul
Moderate
Moderate
<5,000/ul
<5,000/ul
High
High
One unit of PC can elevate the platelet count
One unit of PC can elevate the platelet count
by 5-10,000/ul in a stable, non-alloimmunized
by 5-10,000/ul in a stable, non-alloimmunized
70kg recipient
70kg recipient
A pre-operative platelet count of >50,000/ul
A pre-operative platelet count of >50,000/ul
is generally adequate for surgery
is generally adequate for surgery
Fresh Frozen Plasma
Indications: Correction of clotting factor deficiencies
Indications: Correction of clotting factor deficiencies
where clotting factor concentrates are not available or
where clotting factor concentrates are not available or
when multiple clotting deficiencies are present (e.g. liver
when multiple clotting deficiencies are present (e.g. liver
disease, Coumadin reversal, DIC)
disease, Coumadin reversal, DIC)
; u
; u
sed in TTP in
sed in TTP in
conjunction with
conjunction with
p
p
lasma
lasma
e
e
xchange
xchange
Volume: 200- 250 ml
Volume: 200- 250 ml
Dose: Approximately 10-15 ml/kg body weight
Dose: Approximately 10-15 ml/kg body weight
(Therapy is guided by coagulation studies (PT, aPTT)
(Therapy is guided by coagulation studies (PT, aPTT)
Storage: < -18C (requires thawing prior to
Storage: < -18C (requires thawing prior to
issuing –
issuing –
approx. 30 minutes to thaw)
approx. 30 minutes to thaw)
Shelf-life: 1 year; 24 hours if thawed
Shelf-life: 1 year; 24 hours if thawed
Contraindications
Contraindications
Available specific therapy: FVIII, FIX, Vit K
Available specific therapy: FVIII, FIX, Vit K
Volume expansion
Volume expansion
Patients with IgA antibodies or selective IgA
Patients with IgA antibodies or selective IgA
Deficiency
Deficiency

Cryoprecipitate
Preparation: Precipitates from FFP thawed
Preparation: Precipitates from FFP thawed
at 4C are refrozen
at 4C are refrozen
Contents:
Contents:
>80 IU Factor VIII
>80 IU Factor VIII
150 – 250 mg Fibrinogen
150 – 250 mg Fibrinogen
30 – 50 mg Fibronectin
30 – 50 mg Fibronectin
40 – 70% WB vWF
40 – 70% WB vWF
30% of WB Factor XIII
30% of WB Factor XIII
Volume: 5 – 15 ml
Volume: 5 – 15 ml
Storage: <-18C, must be thawed
Storage: <-18C, must be thawed

Cryoprecipitate
Indications:
Indications:
Correct bleeding due to fibrinogen, vWF, FVIII or
Correct bleeding due to fibrinogen, vWF, FVIII or
FXIII deficiency or dysfunction
FXIII deficiency or dysfunction
Bleeding due to uremia
Bleeding due to uremia
Dose:
Dose:
Depends on number of units of factor or
Depends on number of units of factor or
fibrinogen needed
fibrinogen needed
Usual adult dose (70 kg) = pool of 10 units (~ 2
Usual adult dose (70 kg) = pool of 10 units (~ 2
grams fibrinogen)
grams fibrinogen)
NOT concentrated plasma and should not be used
NOT concentrated plasma and should not be used
as a substitute for plasma
as a substitute for plasma

Factor VIII Concentrate
Intravenous infusion
Intravenous infusion
IV push
IV push
Continuous infusion
Continuous infusion
Dose varies depending on type of bleeding
Dose varies depending on type of bleeding
Ranges from 20-50+ units/kg. body
Ranges from 20-50+ units/kg. body
weight
weight
Half-life 8-12 hours
Half-life 8-12 hours
Each unit infused raises serum factor VIII
Each unit infused raises serum factor VIII
level by 2 %
level by 2 %

Factor IX Concentrate
Intravenous infusion
Intravenous infusion
IV push
IV push
Continuous infusion
Continuous infusion
Dose varies depending on type of bleeding
Dose varies depending on type of bleeding
Ranges from 20-100+ units/kg. body
Ranges from 20-100+ units/kg. body
weight
weight
Half-life 12-24 hours
Half-life 12-24 hours
Each unit infused raises serum factor IX
Each unit infused raises serum factor IX
level by 1%
level by 1%

Factor VII a
in the treatment of patients with
coagulation factor VIII or IX inhibitors or
in close collaboration with a physician
specialised in treatment of haemophilia
FVIIa is injected, which is the active form
FVIIa is injected, which is the active form
of Factor VII
of Factor VII
This probably associates with tissue factor
This probably associates with tissue factor
at the site of injury and activates IX and X
at the site of injury and activates IX and X
Inject 90 ug/kg and achieve 3 to 20 nM
Inject 90 ug/kg and achieve 3 to 20 nM
FVIIa; half life 2.7 hours
FVIIa; half life 2.7 hours

FEIBA
Factor Eight Inhibitor bypassing agent
Factor Eight Inhibitor bypassing agent
Purify the vitamin K dependent factors
Purify the vitamin K dependent factors
that undergo contact activation at some
that undergo contact activation at some
point
point
Contains FVIIa and Xa in addition to
Contains FVIIa and Xa in addition to
non-activated factors (amounts unclear)
non-activated factors (amounts unclear)
1 unit shortens the aPTT of an inhibitor
1 unit shortens the aPTT of an inhibitor
plasma by 50%
plasma by 50%
Give 50 to 100 U/kg up to twice a day
Give 50 to 100 U/kg up to twice a day

What is a transfusion
reaction?
Any untoward event that occurs as a result
Any untoward event that occurs as a result
of infusion of a blood component
of infusion of a blood component
(immediate or delayed)
(immediate or delayed)
When any unexpected or untoward sign or
When any unexpected or untoward sign or
symptom occurs during or shortly after the
symptom occurs during or shortly after the
transfusion of a blood component, a
transfusion of a blood component, a
transfusion reaction must be considered as
transfusion reaction must be considered as
the precipitating event until proven
the precipitating event until proven
otherwise
otherwise
Only a high index of suspicion will allow a
Only a high index of suspicion will allow a
transfusion reaction to be diagnosed
transfusion reaction to be diagnosed

Immediate Adverse Effects
Associated with Transfusion
Acute Hemolytic
Acute Hemolytic
Transfusion Reaction
Transfusion Reaction
Febrile Non-Hemolytic
Febrile Non-Hemolytic
Transfusion Reaction
Transfusion Reaction
Allergic Reactions
Allergic Reactions
Urticarial
Urticarial
Anaphylactic
Anaphylactic
Hypervolemia
Hypervolemia
Non-immune Red Cell
Non-immune Red Cell
Hemolysis
Hemolysis
Transfusion-Related
Transfusion-Related
Acute Lung Injury
Acute Lung Injury
(TRALI)
(TRALI)
Septic Transfusion
Septic Transfusion
Reaction (Bacterial
Reaction (Bacterial
Contamination)
Contamination)
Hypotensive Reactions
Hypotensive Reactions
ACE Inhibitors
ACE Inhibitors
Metabolic Disturbances
Metabolic Disturbances
Hypothermia
Hypothermia
Hyperkalemia
Hyperkalemia
Acidosis
Acidosis

Delayed Adverse Effects
Associated with Transfusion
Delayed Hemolytic Transfusion Reaction
Delayed Hemolytic Transfusion Reaction
Alloimmunization
Alloimmunization
Red Cell Antigens
Red Cell Antigens
HLA
HLA
Leukocytes
Leukocytes
Platelets
Platelets
Graft versus Host Disease (TA-GVHD)
Graft versus Host Disease (TA-GVHD)
Post-transfusion Purpura
Post-transfusion Purpura
Hemosiderosis
Hemosiderosis
Viral and Parasitic Infections
Viral and Parasitic Infections
Transfusion Related Immunomodulation
Transfusion Related Immunomodulation
(TRIM)
(TRIM)
Estimates of Non-Infectious Risks of
Transfusion
Type
Type
Incidence
Incidence
Type
Type
Incidence
Incidence
Acute
Acute
Hemolytic
Hemolytic
1:38,000 to
1:38,000 to
1:70,000
1:70,000
Delayed
Delayed
Hemolytic
Hemolytic
1:5000 to
1:5000 to
1:11,000
1:11,000
Anaphylactic
Anaphylactic
1:20,000 to
1:20,000 to
1:50,000
1:50,000
HLA
HLA
Alloimmunization
Alloimmunization
10 – 20%
10 – 20%
TRALI
TRALI
1:5,000
1:5,000
Red Cell
Red Cell
Alloimmunization
Alloimmunization
1 – 2%
1 – 2%
Circulatory
Circulatory
Overload
Overload
1:10,000
1:10,000
TA-GVHD
TA-GVHD
Rare
Rare
Febrile Non-
Febrile Non-
Hemolytic
Hemolytic
1:200 – 1:17
1:200 – 1:17
(RBC)
(RBC)
1:100 – 1:3
1:100 – 1:3
(Plts)
(Plts)
Post-Transfusion
Post-Transfusion
Purpura
Purpura
Rare
Rare
Urticaria
Urticaria
1:100 to 1:33
1:100 to 1:33
Hemosiderosis
Hemosiderosis
Dependent
Dependent
on # units
on # units
transfused
transfused

Acute Hemolytic
Transfusion Reaction
Etiology: Red cell incompatibility
Etiology: Red cell incompatibility
Most severe reactions are seen following ABO
Most severe reactions are seen following ABO
incompatible transfusions
incompatible transfusions
As little as 5 – 20 ml of red cells can precipitate
As little as 5 – 20 ml of red cells can precipitate
severe reactions
severe reactions
Occur within minutes to hours after transfusion
Occur within minutes to hours after transfusion
Signs & Symptoms
Signs & Symptoms
Chills
Chills
Fever
Fever
Hemoglobinuria
Hemoglobinuria
Hypotension
Hypotension
Renal failure with oliguria
Renal failure with oliguria
DIC (oozing from IV sites)
DIC (oozing from IV sites)
Back Pain
Back Pain
Pain at infusion site
Pain at infusion site
Anxiety
Anxiety

Clinical Approach/Assessment
Clinical Approach/Assessment
Stop transfusion
Stop transfusion
Initiate a transfusion reaction work-up
Initiate a transfusion reaction work-up
Notify the blood bank
Notify the blood bank
Return remaining product or empty bag and all attached tubing and
Return remaining product or empty bag and all attached tubing and
IV fluid bags to the blood bank
IV fluid bags to the blood bank
Send new patient sample to blood bank and send urine sample
Send new patient sample to blood bank and send urine sample
Management
Management
Maintain urine output at appropriate level with fluids and diuretics
Maintain urine output at appropriate level with fluids and diuretics
Analgesics
Analgesics
Pressors for hypotension (low dose Dopamine)
Pressors for hypotension (low dose Dopamine)
Hemostatic components (FFP, cryo, platelets) for bleeding/coagulopathy
Hemostatic components (FFP, cryo, platelets) for bleeding/coagulopathy
Follow-up labs (total/indirect bilirubin, creatinine, LDH, haptoglobin,
Follow-up labs (total/indirect bilirubin, creatinine, LDH, haptoglobin,
CBC, PT/PTT)
CBC, PT/PTT)
Prevention
Prevention
Adequate training
Adequate training
Follow specified procedures and policies
Follow specified procedures and policies
Reliable patient and sample identification
Reliable patient and sample identification
Acute Hemolytic
Transfusion Reaction

Delayed Hemolytic
Transfusion Reaction
Etiology: Anamnestic immune response to RBC antigens
Etiology: Anamnestic immune response to RBC antigens
Signs & Symptoms
Signs & Symptoms
Fever
Fever
Decreasing hemoglobin
Decreasing hemoglobin
New positive antibody screening test
New positive antibody screening test
Mild jaundice
Mild jaundice
Laboratory testing
Laboratory testing
Antibody screen + DAT
Antibody screen + DAT
Visual inspection (plasma-free Hb or methemalbumin)
Visual inspection (plasma-free Hb or methemalbumin)
Hemolysis labs: LDH, bili, urine hemosiderin,
Hemolysis labs: LDH, bili, urine hemosiderin,
haptoglobin, H/H
haptoglobin, H/H
Therapeutic/Prophylactic Approach
Therapeutic/Prophylactic Approach
Identify antibody & transfuse compatible blood as needed
Identify antibody & transfuse compatible blood as needed

Febrile Non-hemolytic
Transfusion Reaction
Etiology
Etiology
Antibody to donor WBCs
Antibody to donor WBCs
Accumulated cytokines in bag
Accumulated cytokines in bag
Signs & Symptoms
Signs & Symptoms
Chills/rigors
Chills/rigors
Fever (generally defined as a 1C (2F) increase)
Fever (generally defined as a 1C (2F) increase)
Headache
Headache
May be accompanied by changes in BP and HR,
May be accompanied by changes in BP and HR,
dyspnea, nausea or vomiting
dyspnea, nausea or vomiting
Laboratory testing
Laboratory testing
Rule out hemolysis
Rule out hemolysis
Therapeutic/Prophylactic Approach
Therapeutic/Prophylactic Approach
Antipyretic premedication
Antipyretic premedication
Leukocyte-reduced blood products
Leukocyte-reduced blood products

Allergic (Urticarial)
Transfusion Reactions
Etiology: Antibody (IgE) to donor plasma
Etiology: Antibody (IgE) to donor plasma
proteins (found in platelets, FFP, Cryo,
proteins (found in platelets, FFP, Cryo,
RBCs)
RBCs)
Signs & Symptoms
Signs & Symptoms
Urticaria
Urticaria
Pruritis
Pruritis
Flushing
Flushing
Therapeutic/Prophylactic Approach
Therapeutic/Prophylactic Approach
Antihistamine, treatment or
Antihistamine, treatment or
premedication
premedication
May restart unit slowly after
May restart unit slowly after
antihistamine if symptoms resolve
antihistamine if symptoms resolve

Anaphylactic
Transfusion Reaction
Etiology: Ab to donor plasma proteins (IgE, IgA, C4)
Etiology: Ab to donor plasma proteins (IgE, IgA, C4)
Pathophysiology: Immediate generalized reaction caused by release of
Pathophysiology: Immediate generalized reaction caused by release of
histamine and other mediators
histamine and other mediators
Signs & Symptoms
Signs & Symptoms
Hypotension
Hypotension
Urticaria
Urticaria
Bronchospasm (respiratory distress, wheezing)
Bronchospasm (respiratory distress, wheezing)
Local edema
Local edema
Anxiety
Anxiety
Laboratory testing
Laboratory testing
Rule out hemolysis (DAT, inspect for Hb)
Rule out hemolysis (DAT, inspect for Hb)
Anti-IgA
Anti-IgA
IgA quantitative
IgA quantitative
Therapeutic/Prophylactic Approach
Therapeutic/Prophylactic Approach
Trendelenberg position
Trendelenberg position
Fluids
Fluids
Epinephrine, antihistamine, corticosteroids,
Epinephrine, antihistamine, corticosteroids,
ß
ß
2 agonists
2 agonists
IgA-deficient blood components
IgA-deficient blood components

Transfusion-Related Acute
Lung Injury (TRALI)
Mechanism:
Mechanism:
Anti-WBC (neutrophil, HLA) antibodies in donor which bind to
Anti-WBC (neutrophil, HLA) antibodies in donor which bind to
granulocytes or monocytes leading to complement activation and
granulocytes or monocytes leading to complement activation and
neutrophil aggregation in the pulmonary vasculature
neutrophil aggregation in the pulmonary vasculature
Activated neutrophils release inflammatory enzymes and biologic
Activated neutrophils release inflammatory enzymes and biologic
response mediators that result in endothelial injury and leakage
response mediators that result in endothelial injury and leakage
of protein-rich fluid into the lungs
of protein-rich fluid into the lungs
Rarely due to patient antibodies
Rarely due to patient antibodies
Signs & Symptoms
Signs & Symptoms
Acute respiratory distress
Acute respiratory distress
Severe bilateral pulmonary edema
Severe bilateral pulmonary edema
Severe hypoxia
Severe hypoxia
Tachycardia
Tachycardia
Fever
Fever
Hypotension
Hypotension
Cyanosis
Cyanosis
Usually arises within 1-6 hours of transfusion of plasma-
Usually arises within 1-6 hours of transfusion of plasma-
containing blood component
containing blood component
s
s

Transfusion-Related Acute
Lung Injury (TRALI)
Laboratory testing
Laboratory testing
WBC antibody (HLA, granulocyte) screen in
WBC antibody (HLA, granulocyte) screen in
donor and recipient
donor and recipient
Consequences
Consequences
Mild to moderate cases
Mild to moderate cases
Lung injury and prolonged ventilator time
Lung injury and prolonged ventilator time
Predispose patient to pulmonary infection
Predispose patient to pulmonary infection
Severe cases
Severe cases
Fatal outcomes (3
Fatal outcomes (3
rd
rd
most common cause of
most common cause of
transfusion-related death)
transfusion-related death)
Therapeutic/Prophylactic Approach
Therapeutic/Prophylactic Approach
Supportive care until recovery
Supportive care until recovery
Defer implicated donors
Defer implicated donors

Transfusion-Associated
Graft versus Host Disease
Incidence: Rare
Incidence: Rare
Mechanism:
Mechanism:
Viable donor T-lymphocytes engraft in recipient
Viable donor T-lymphocytes engraft in recipient
and mount an immune response against recipient
and mount an immune response against recipient
tissues
tissues
Signs & Symptoms
Signs & Symptoms
Erythroderma
Erythroderma
Maculopapular rash
Maculopapular rash
Anorexia
Anorexia
Nausea & vomiting
Nausea & vomiting
Diarrhea
Diarrhea
Hepatitis
Hepatitis
Pancytopenia
Pancytopenia
Fever
Fever

Transfusion-Associated
Graft versus Host Disease
Laboratory testing
Laboratory testing
HLA typing
HLA typing
Skin biopsy
Skin biopsy
Treatment
Treatment
Approximately 90% of cases are fatal
Approximately 90% of cases are fatal
(complications of bone marrow failure)
(complications of bone marrow failure)
Irradiation of blood components for patients at risk
Irradiation of blood components for patients at risk
(including DDs and HLA-selected components)
(including DDs and HLA-selected components)
Dosage: 25 rad
Dosage: 25 rad
Detrimental effects on RBCs (K+ leakage)
Detrimental effects on RBCs (K+ leakage)
Shortened shelf-life: 28 days from time of
Shortened shelf-life: 28 days from time of
irradiation
irradiation

Who is at risk for TA-GVHD
and needs irradiated blood
products?
Significantly increased risk
Significantly increased risk
Congenital
Congenital
immunodeficiency
immunodeficiency
syndromes
syndromes
Bone marrow
Bone marrow
transplantation (allo & auto)
transplantation (allo & auto)
Transfusions from blood
Transfusions from blood
relatives
relatives
Intrauterine Transfusions
Intrauterine Transfusions
HLA-matched platelet
HLA-matched platelet
transfusions/blood
transfusions/blood
components
components
Hodgkin’s disease
Hodgkin’s disease
Patients treated with purine
Patients treated with purine
analogues
analogues
Minimally increased risk
Minimally increased risk
Acute leukemia
Acute leukemia
Non-Hodgkin’s lymphoma
Non-Hodgkin’s lymphoma
Solid tumors treated with
Solid tumors treated with
intensive
intensive
chemotherapy/radiation
chemotherapy/radiation
Exchange transfusion
Exchange transfusion
Premature neonates
Premature neonates
Neonates on ECMO
Neonates on ECMO
Solid organ transplant
Solid organ transplant
recipient
recipient
Perceived, but no reported risk
Perceived, but no reported risk
Healthy newborns
Healthy newborns
Patients with AIDS
Patients with AIDS

Post-Transfusion Purpura
Posttransfusion purpura (PTP) is
Posttransfusion purpura (PTP) is
characterized by severe
characterized by severe
thrombocytopenia following
thrombocytopenia following
blood transfusion (
blood transfusion (
5-12 days
5-12 days
)
)
that results from
that results from
alloimmunization to platelet-
alloimmunization to platelet-
specific alloantigens.
specific alloantigens.

Conclusion
Risks of transfusion are associated
Risks of transfusion are associated
with blood product safety and
with blood product safety and
administration
administration
Dramatic reduction of transfusion-
Dramatic reduction of transfusion-
transmitted infectious risk
transmitted infectious risk
Continued improvement needed to
Continued improvement needed to
reduce the non-infectious risks of
reduce the non-infectious risks of
transfusion
transfusion
Document Outline
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Slide 45
- Slide 46
Wyszukiwarka
Podobne podstrony:
Duration of wrinkle correction following repeat treatment with Juvéderm hyaluronic acid fillers
#0952 Dealing With Rising Production Costs
Mechanical evaluation of the resistance and elastance of post burn scars after topical treatment wit
Amon Amarth The Last With Pagan Blood
APA practice guideline for the treatment of patients with Borderline Personality Disorder
Periacetabular osteotomy for the treatment of dysplastic hip with Perthes like deformities
Breast and other cancers in 1445 blood relatives of 75 Nordic patients with ataxia telangiectasia
Differential Treatment Response for Eating Disordered Patients With and Without a Comorbid BPD Di
Makówka, Agnieszka i inni Treatment of chronic hemodialysis patients with low dose fenofibrate effe
A Proton MRSI Study of Brain N Acetylaspartate Level After 12 Weeks of Citalopram Treatment in Drug
The Effects of Probiotic Supplementation on Markers of Blood Lipids, and Blood Pressure in Patients
(IV)The effect of McKenzie therapy as compared with that of intensive strengthening training for the
Positive Options for Living with Lupus Self Help and Treatment (Positive Options for Health)
7 BEAUTY PRODUCTS TO REPLACE WITH TEA(1)
The treatment of behavioral sequelae of autism with dextromethorphan A case report
Product presentation XC100FC
~$Production Of Speech Part 2
Image Processing with Matlab 33
więcej podobnych podstron