Diaphragm
anatomy
hernias
treatment
Anatomy of the
diaphragm
A dome-shaped anatomical structure consisting
of a muscular and tendineous part
Diaphragmatic attachments:
posterior: the first, second and third lumbar
vertebra
anterior: the inferior part of the sternum
lateral: the costal arch
It separates abdominal and thoracic cavities
from each other
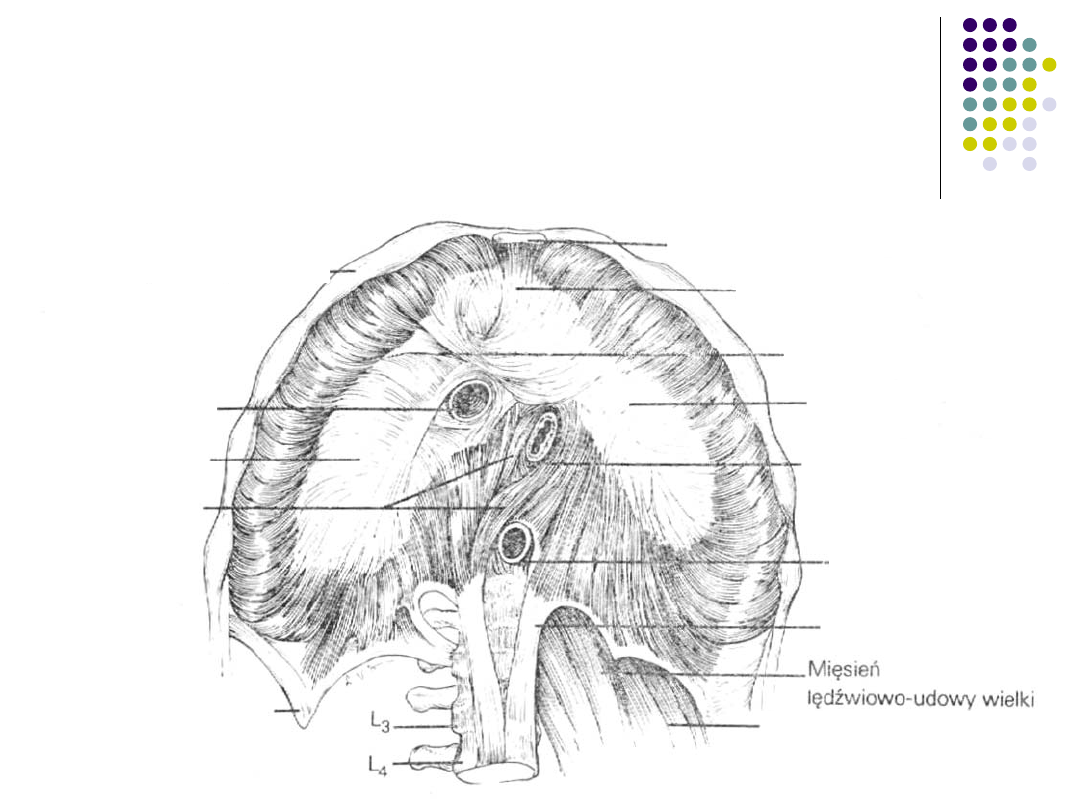
Anatomy of the
diaphragm
Cartilaginous part of a rib
Xyphoid process
Central lobe
Central tendon
Left lobe
Esophageal hiatus
Aortic hiatus
Left crus
Right lobe
Right crus
Foramen of the
caval vein
Lumbar quadrate
muscle
XII rib
Diaphragmatic hernias
Etiology
Numerous hiatuses and foramina in the diaphragm
Complex embryology
Difference of pressure over and beneath the diaphragm
Diaphragmatic hernias
Classification
General classification:
congenital
acquired
posttraumatic
Akerlund’s classification:
caused by congenital short esophagus
paraesophageal
sliding
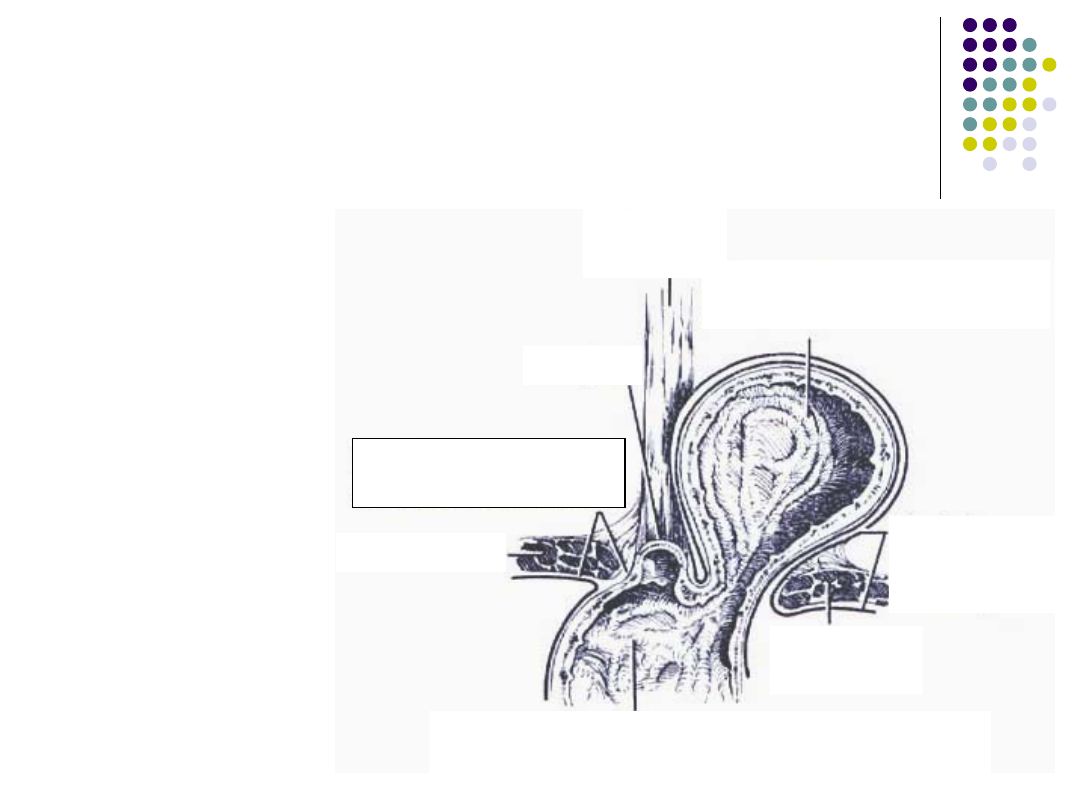
Paraesophageal hernia
Normal position
of
gastroesophage
al junction.
Protrusion of the
stomach
alongside the
esophagus.
Phrenoesophageal
membrane
Bending of
the parietal
peritoneum
Diaphragm
Diaphrag
m
Protrusion of the stomach
into a hernia sac
Part of the stomach localized within the
abdominal space
Esophagu
s
Cardia
Paraesophageal hernia
good function of the lower esophageal
sphincter
asymptomatic clinical course- frequently
air eructation
postprandial fulness
Complications:
bleeding
incarceration
acute dysphagia
strangulation
Treatment - surgical management
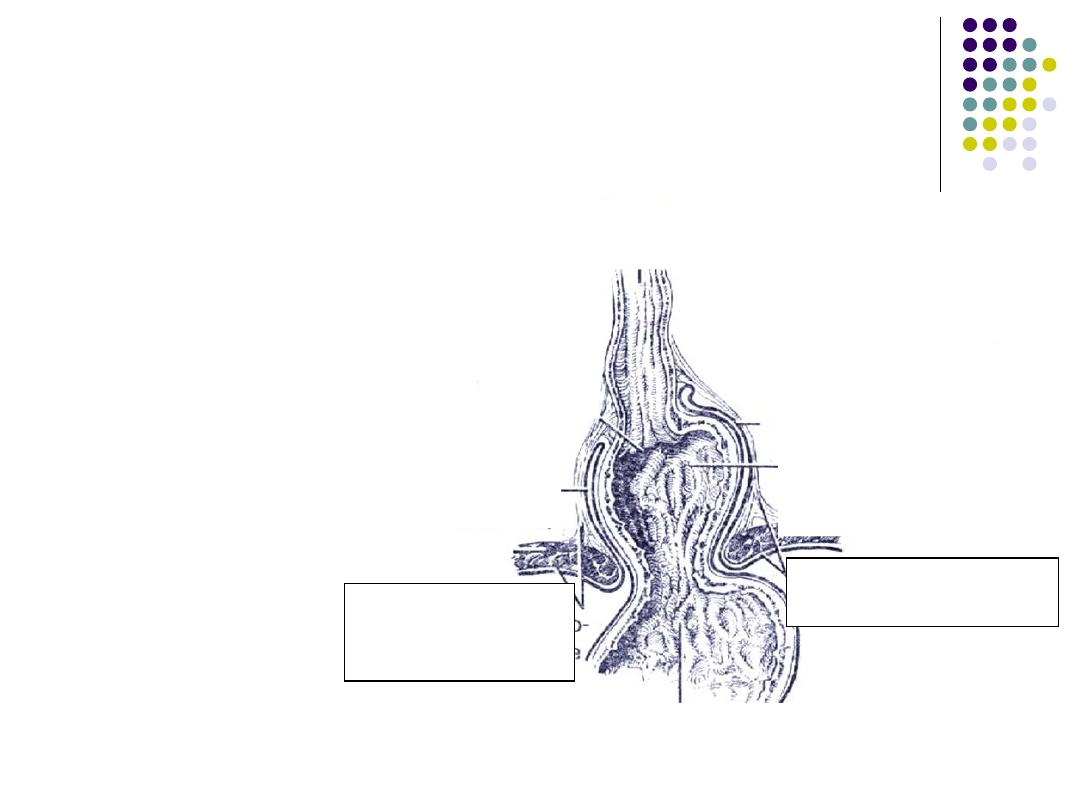
Sliding hernia
Most common.
Gastroesophageal
junction above the
diapragm.
Esophagu
s
Protrusion of the
stomach into a hernia
sac
Phrenoesophageal
membrane
Cardia
Diaphragm
Bending of
the parietal
peritoneum
Part of the stomach localized within the
abdominal space
Phrenoesophage
al membrane
Bending of
the parietal
peritoneum
Diaphragm
Sliding hernia
dysfunction of the lower esophageal
sphincter
heartburn frequently made worse when a
patient lies down
typical picture on x-ray examination
decreased resting pressure of the lower
esophageal sphincter
Complications
esophagitis
esophageal strictures
Sliding hernia
Treatment
1.
Medical treatment
2.
Surgical
Abdominal approach
Chest approach
Aims of surgical management:
Reduction of hernia
Closure of a hernial ring
Reconstruction of the Hiss’s angle
Congenital hernias
Morgagni’s and Bochdalek’s
hernia
frequently asymptomatic
diagnosed accidentally
paroxysmal or constant epigastric pain
respiratory and circulatory disturbances
ileus
Treatment- surgical management.

Congenital hernias
Morgagni’s and Bochdalek’s
hernia
Parasternal diaphragmatic hernia (Morgagni)
Posterolateral diaphragmatic hernia (Bochdalek)
Posttraumatic
diaphragmatic hernia
Traumatic rupture of the diaphragm may
result from penetrating or blunt traumas
Diaphragmatic rupture occurs usually
within the central tendon more
frequently on its left side
Viscera can immediately translocate into
the pleural space through the
diaphragmatic rupture or their
displacement may be gradual and it can
last months or even years.
Posttraumatic
diaphragmatic hernia
Clinical presentation of the hernia
depends on the part and amount of
viscera that displaced into the pleural
space.
We can observe:
bleeding
ileus
Circulatory and respiratory failure
Posttraumatic
diaphragmatic hernia
Surgical approach through the
abdominal
cavity
is advocated if:
recent trauma
injuries of viscera are suspected or diagnosed.
Surgical approach through the
chest
is
advocated if diagnosis is substantially
delayed and intra-abdominal injuries are
excluded.
Document Outline
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
Wyszukiwarka
Podobne podstrony:
Posterior Diaphragm KT method
16 Electrostatic actuators with P silicon diaphragms
Posterior Diaphragm tapeSP
Anterior Diaphragm KT method
Anterior Diaphragm tapeSP
Posterior Diaphragm KT method
16 Electrostatic actuators with P silicon diaphragms
BJCCFSB2006 143 V3i Earpiece distortion in a call Diaphragm not Adhered Fir
więcej podobnych podstron