
ERC
ALS UNIVERSAL
TREATMENT ALGORITHM

ERC
Objectives
To understand:
• Treatment of patients in:
– ventricular fibrillation and
pulseless ventricular
tachycardia
– asystole or pulseless electrical
activity (non-VF/VT rhythms)
ERC
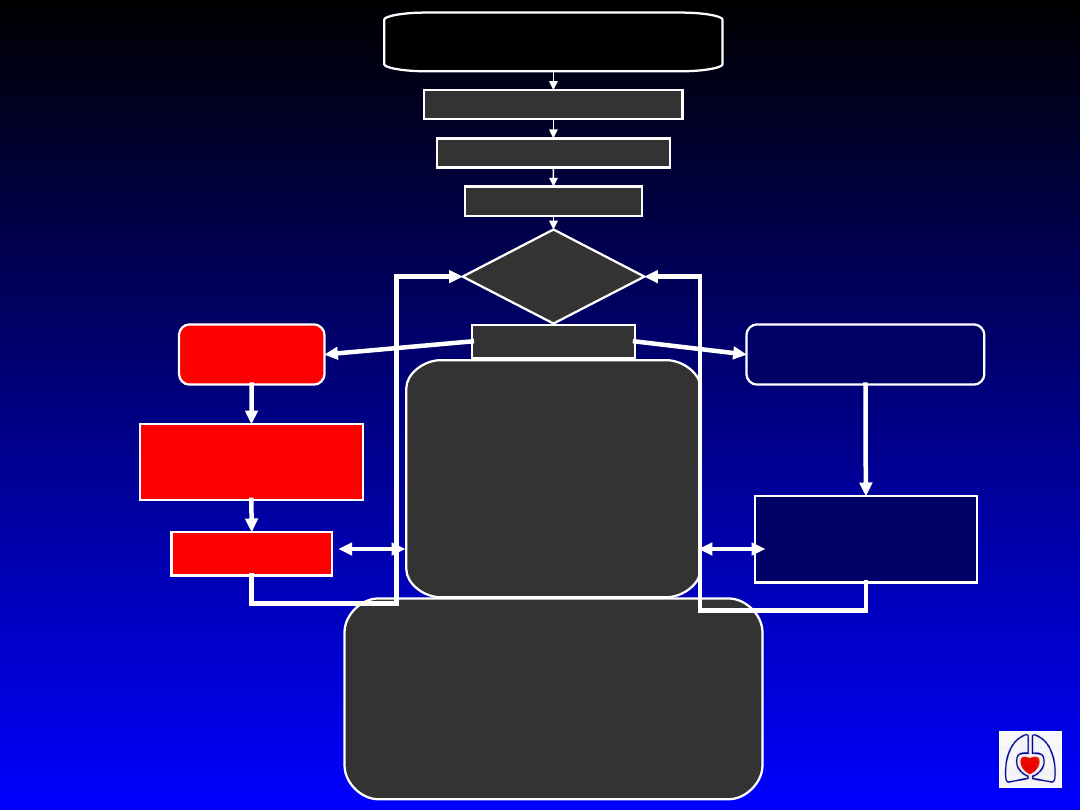
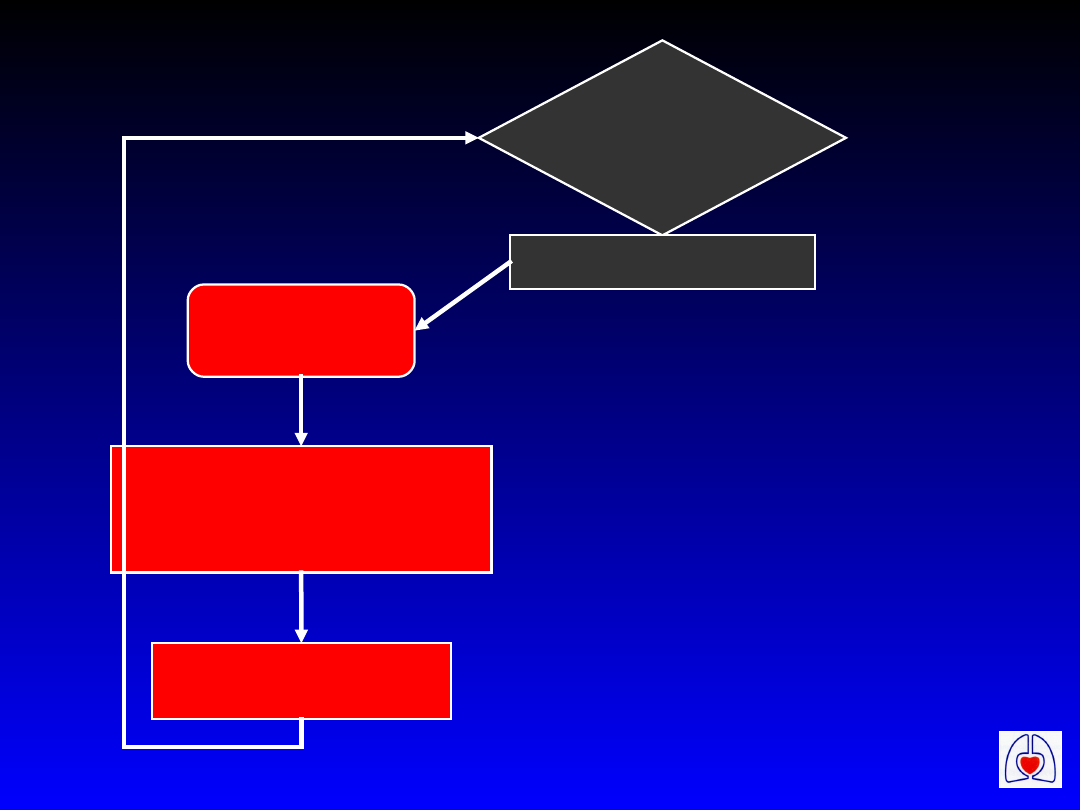
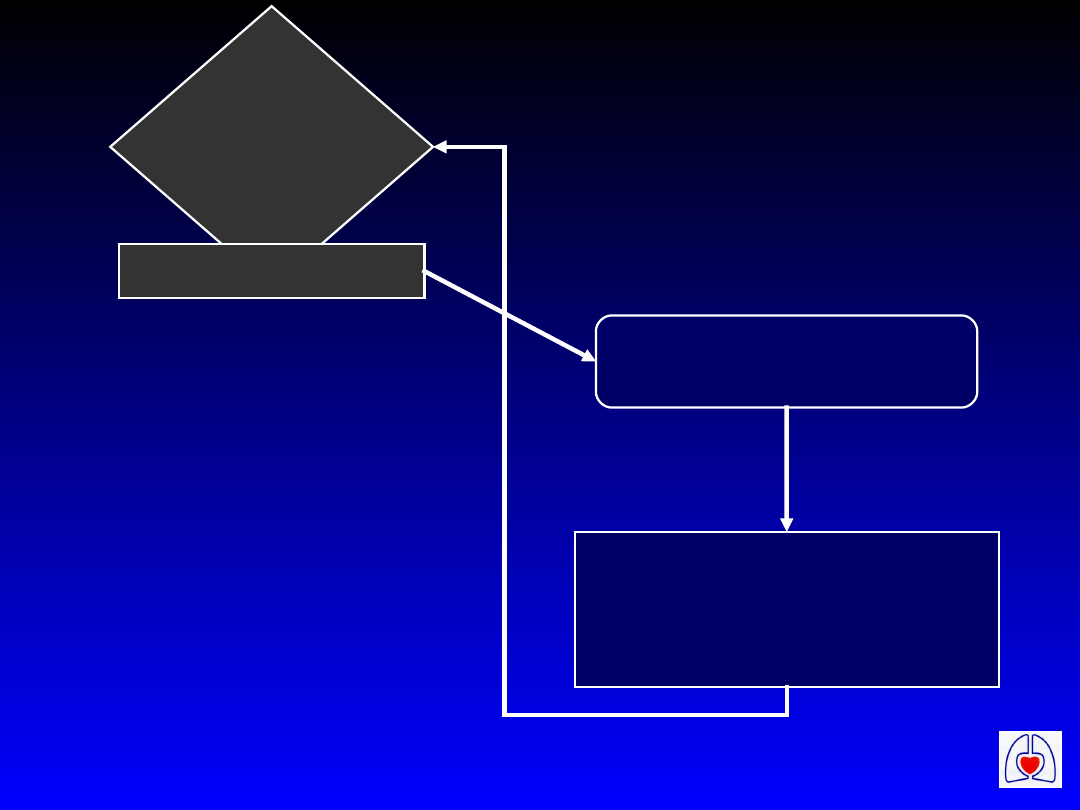
Cardiac Arrest
Precordial Thump if appropriate
BLS Algorithm if appropriate
Attach Defib-Monitor
Assess
Rhythm
+/- Check Pulse
VF/VT
Non-VF/VT
Defibrillate X 3
as necessary
CPR 1 min
CPR 3 min*
* 1 min if immediately
after defibrillation
During CPR
Correct reversible causes
If not already:
•check electrodes, paddle
position and contact
•attempt / verify airway & O
2
i.v. access
•give epinephrine every 3 min
Consider:
amiodarone, atropine / pacing
buffers
Potential reversible causes:
•Hypoxia
•Hypovolaemia
•Hypo/hyperkalaemia & metabolic disorders
•Hypothermia
•Tension pneumothorax
•Tamponade
•Toxic/therapeutic disorders
•Thrombo-embolic & mechanical obstruction
Universal ALS
Algorithm
ERC
ERC
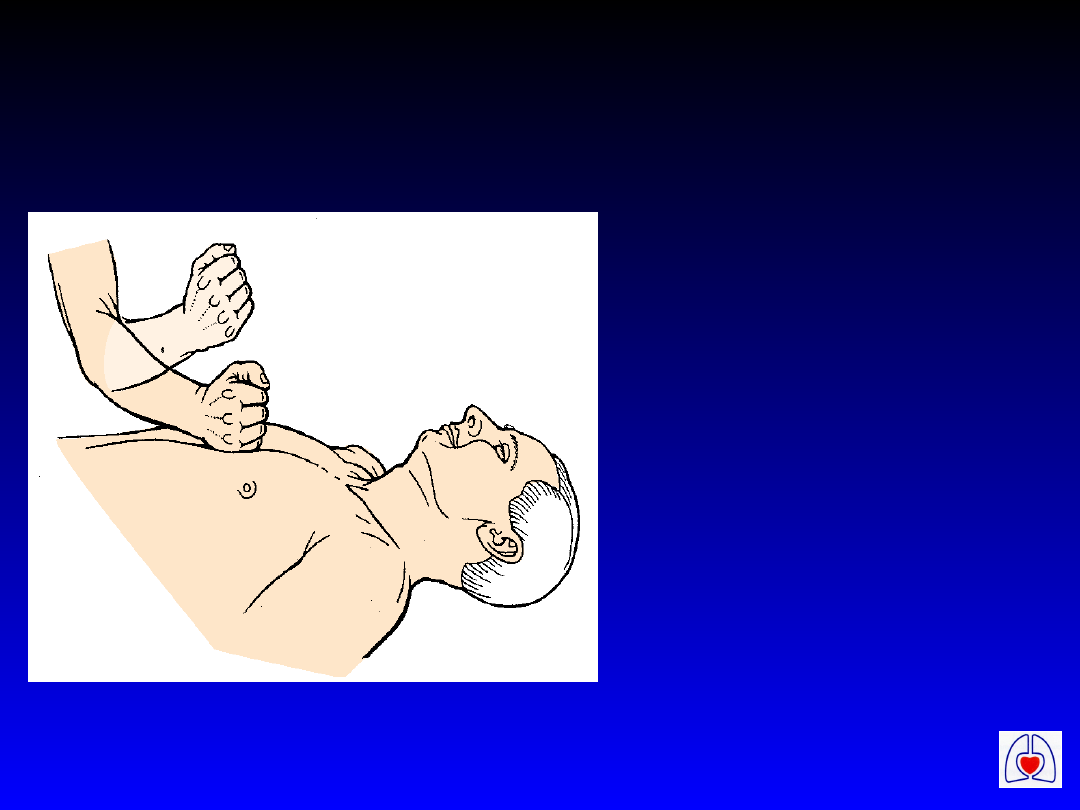
Precordial thump
• Indication:
– witnessed
or
monitored
cardiac
arrest
ERC
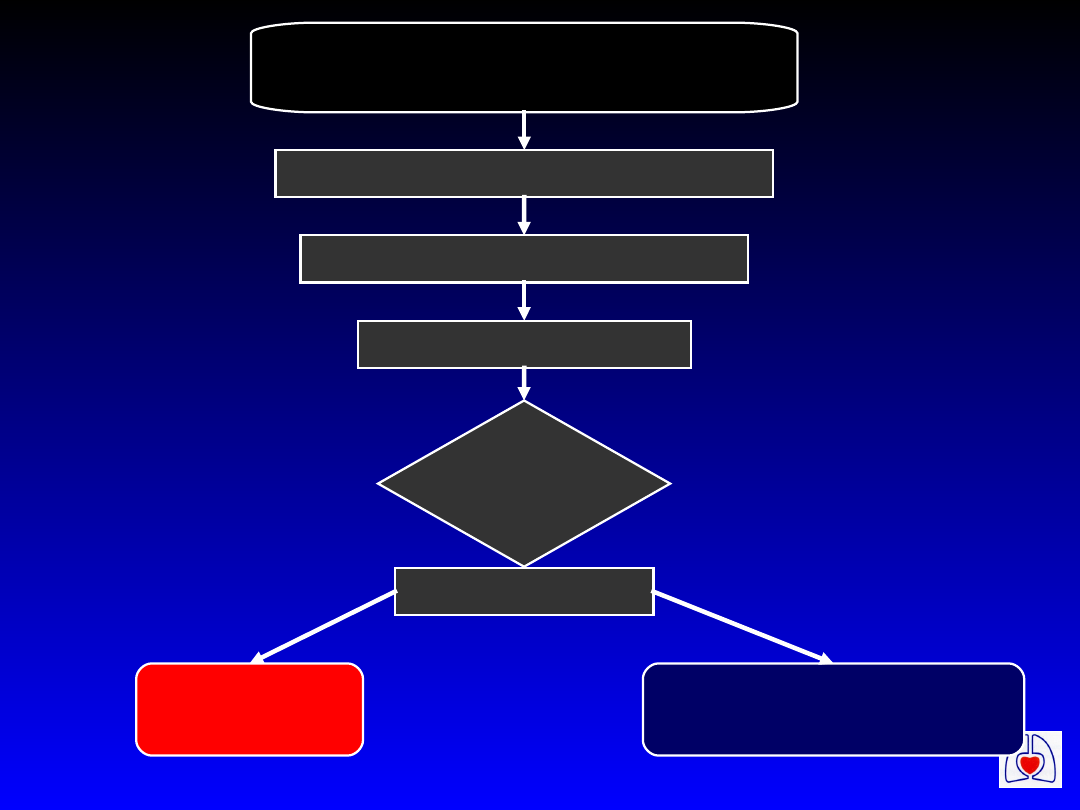
Cardiac Arrest
Precordial Thump if appropriate
BLS Algorithm if appropriate
Attach Defib-Monitor
Assess
Rhythm
+/- Check Pulse
VF/VT
Non-VF/VT
ERC
Assess
Rhythm
+/- Check Pulse
VF/VT
Defibrillate X 3
as necessary
CPR 1 min
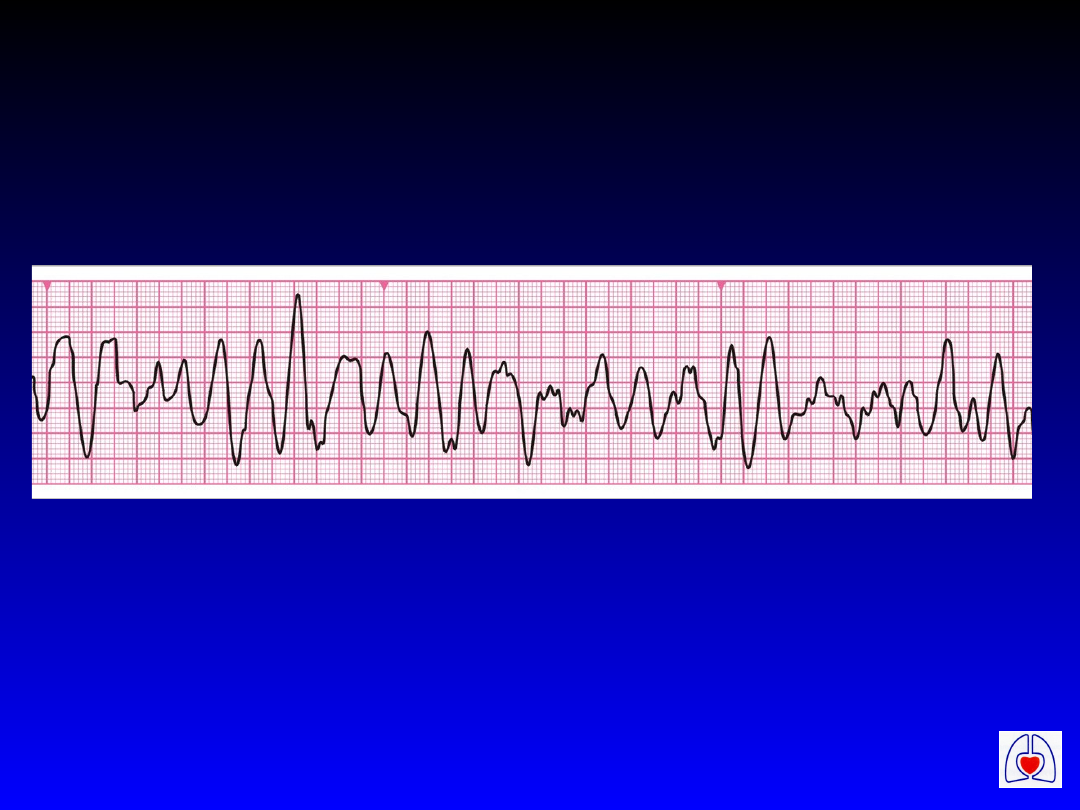
Ventricular Fibrillation/
Pulseless Ventricular
Tachycardia
ERC
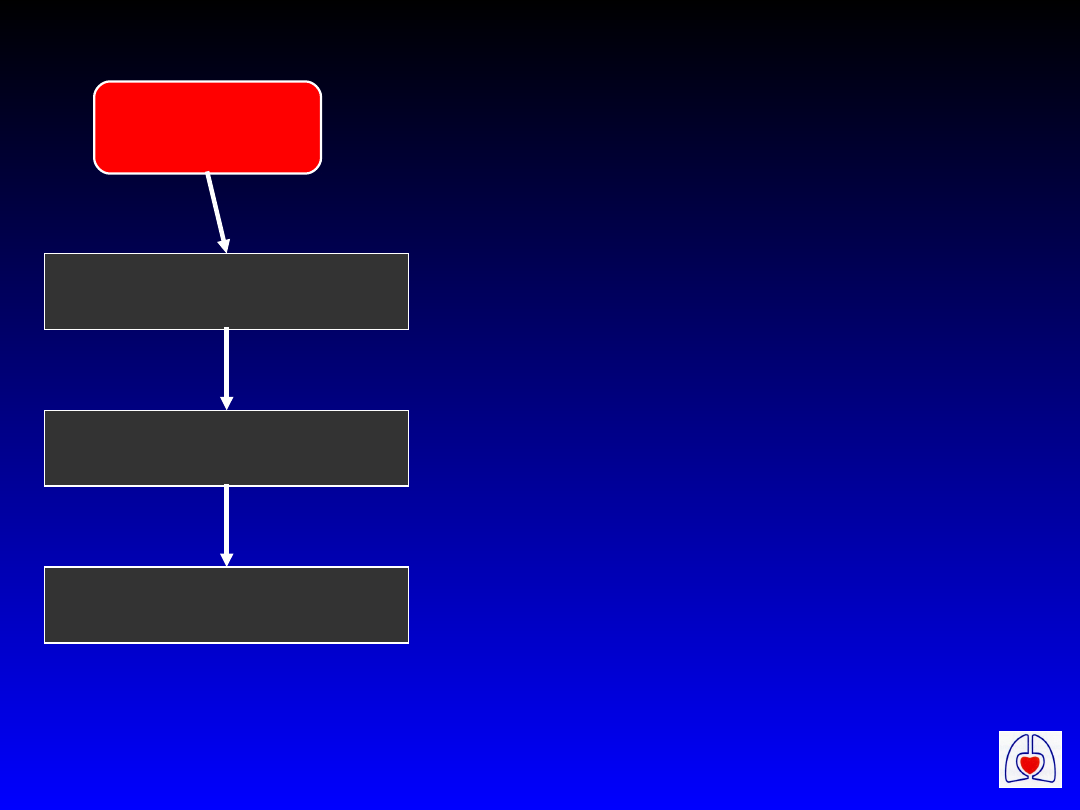
VF/VT
Shock 200 J*
Shock 200 J*
Shock 360 J*
*or biphasic equivalent
• Deliver 3 shocks, if
required, in < 1 minute
• Do not interrupt shock
sequence for BLS
• After shock/s, palpate
carotid pulse only if
waveform compatible
with a cardiac output
ERC
During CPR
Correct reversible causes
If not already:
• check electrodes, paddle position and
contact
• attempt / verify: airway & O
2
i.v. access
• give epinephrine every 3 min
Consider:
amiodarone, atropine / pacing, buffers

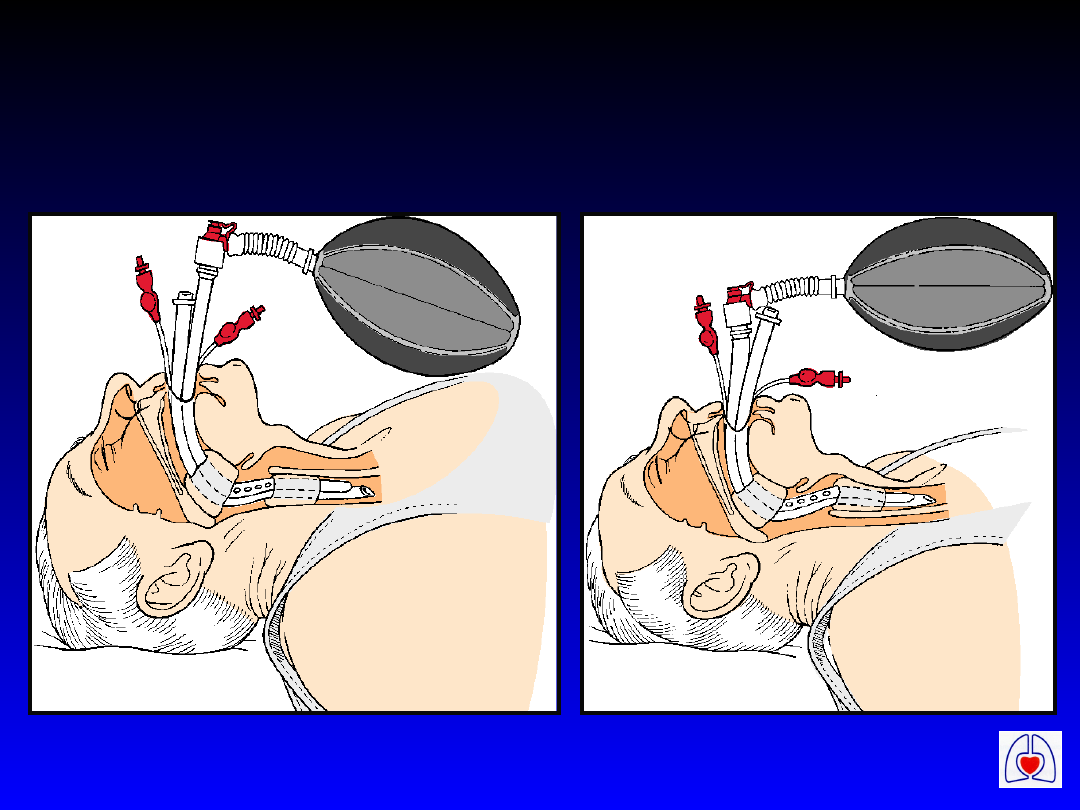
ERC
Chest compressions,
airway and ventilation
• Secure airway:
– tracheal tube
– LMA
– Combitube
• Once airway secured, do not
interrupt chest compressions for
ventilation
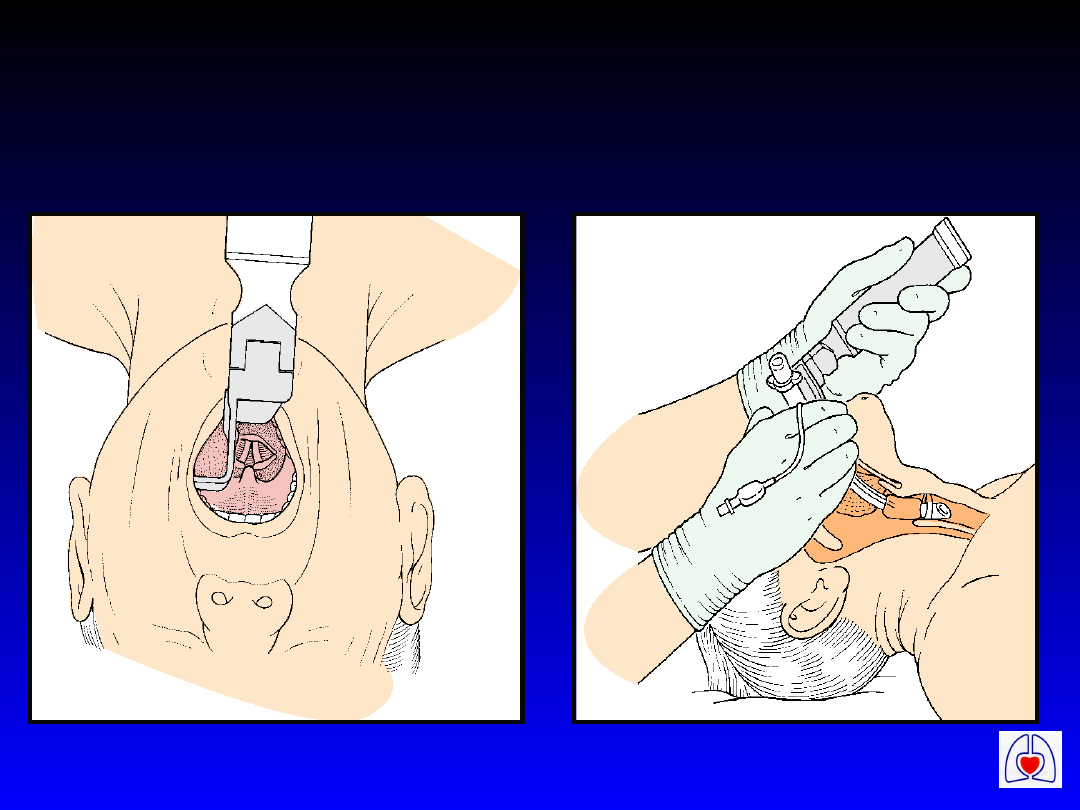
ERC
Insertion of tracheal
tube
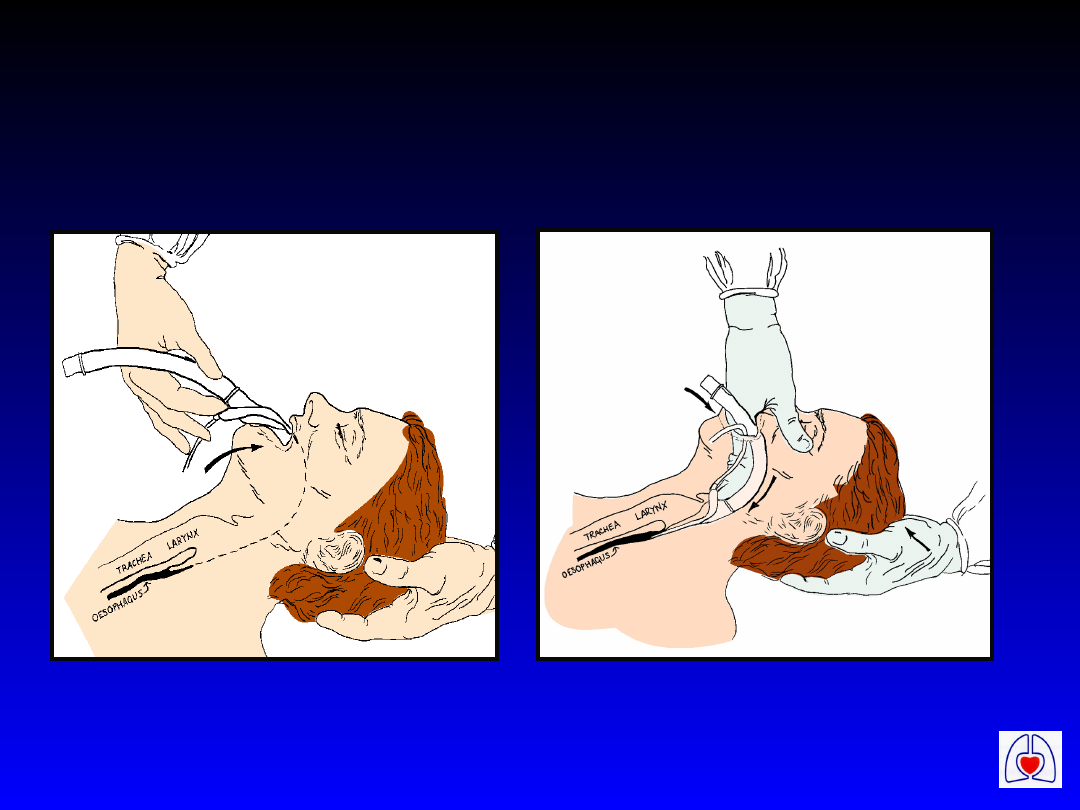
ERC
LMA Insertion
ERC
Ventilation with the
Combitube

ERC
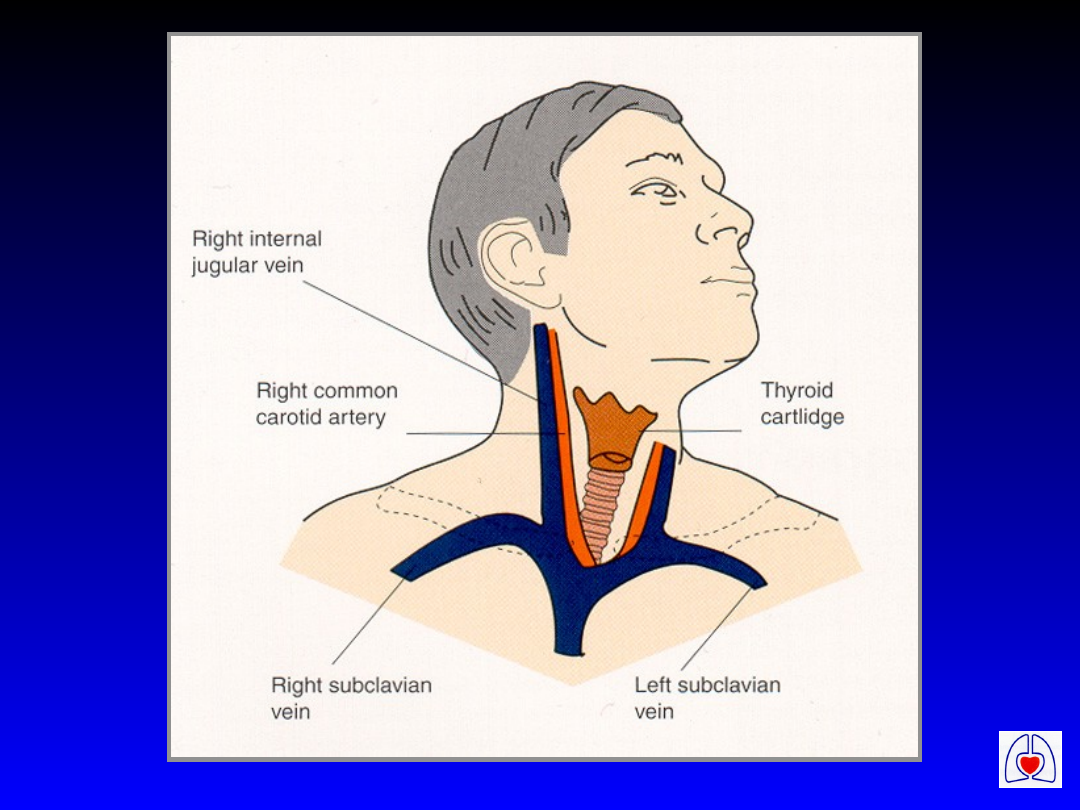
Intravenous access and drugs
VF/VT
• Central veins versus peripheral
• Epinephrine 1 mg i.v. or 2-3 mg
tracheal tube
• Consider amiodarone 300 mg if
VF/VT persists after 3rd shock
• Alternatively - lidocaine 100 mg
• Consider magnesium 8 mmol
ERC

ERC
Epinephrine
Dose:
• 1 mg intravenous 10 ml 1:10,000 (1 ml
1:1,000) every 2-3 mins during
resuscitation
• 2-3 mg via tracheal tube
• 2–10 mcg min
-1
for atropine resistant
bradycardia
• 0.5ml 1:1,000 i.m., 3-5 ml 1:10,000 i.v.
in anaphylaxis, depending on severity

ERC
Atropine
Dose:
• Asystole / PEA (rate < 60 beats min
-1
)
– 3 mg i.v., once only
– 6 mg via tracheal tube
• Bradycardia
– 0.5 mg i.v., repeated as necessary,
maximum 3 mg

ERC
Amiodarone
Indications:
• Refractory VF / Pulseless VT
• Haemodynamically stable VT
• Other resistant tachyarrhythmias

ERC
Amiodarone
Dose:
• Refractory VF / Pulseless VT
– 300 mg in 20 ml 5% dextrose, bolus i.v.
• Stable tachyarrhythmias
– 150 mg in 20 ml 5% dextrose over 10 mins
– Repeat 150 mg if necessary
– 300 mg in 100 ml 5% dextrose over 1 hour

ERC
Amiodarone
Actions:
• Lengthens duration of action
potential
• Prolongs Q-T interval
• Mild negative inotrope - may cause
hypotension

ERC
Magnesium
Indications:
• Shock refractory VF
(with possible hypomagnesaemia)
• Ventricular tachyarrhythmias
(with possible hypomagnesaemia)
• Torsades de pointes

ERC
Magnesium
Dose:
Shock Refractory VF
• 2–4 ml 50% (4–8 mmol) i.v. over 1-2 mins
• Can be repeated after 10-15 minutes
Other circumstances
• 5 ml of 50% (10 mmol) i.v. over 30 mins

ERC
Magnesium
Actions:
• Depresses neurological and
myocardial function
• Acts as a physiological calcium
blocker

ERC
Lidocaine
Dose:
• Refractory VF / Pulseless VT
– 100 mg i.v.
– further boluses of 50 mg, max 200 mg
• Haemodynamically stable VT
– 50 mg i.v.
– further boluses of 50 mg, max 200 mg
• Reduce dose in elderly or hepatic failure

ERC
Sodium Bicarbonate
Dose:
• 50 mmol (50 ml of 8.4% solution)
i.v.

ERC
Calcium
Indications:
• Pulseless electrical activity caused by:
– severe hyperkalaemia
– severe hypocalcaemia
– overdose of calcium channel blocking drugs
Dose
• 10 ml 10% calcium chloride (6.8 mmol)
Do not give immediately before or after
sodium bicarbonate
ERC
Shock 360 J*
Shock 360 J*
Shock 360 J*
*or biphasic equivalent
VF/VT (continued)
• Epinephrine every 3
minutes
• Consider
bicarbonate 50
mmol if pH < 7.1
• Consider paddle
positions
ERC
Non-VF/VT
CPR 3 min*
* 1 min if immediately
after defibrillation
Assess
Rhyth
m
+/- Check Pulse
Asystole
Pulseless Electrical
Activity

ERC
Non-VF/VT immediately
after defibrillation
• Withhold epinephrine/atropine - check
rhythm and pulse after 1 minute of CPR
– Delay in recovery of monitor display
– Electrical stunning - few seconds of
true asystole after defibrillation
– Myocardial stunning - temporarily
impaired contractility
ERC
Potential reversible causes:
•Hypoxia
•Hypovolaemia
•Hypo/hyperkalaemia & metabolic disorders
•Hypothermia
•Tension pneumothorax
•Tamponade
•Toxic/therapeutic disorders
•Thrombo-embolic & mechanical
obstruction

ERC
Asystole
• Confirm:
– check leads - view via leads I and II
– check gain
• Epinephrine 1 mg every 3 minutes
• Atropine 3 mg i.v. or 6 mg via
tracheal tube

ERC
Spurious asystole
• When monitoring with paddle-gel
pads
• More likely with increasing number
of shocks and high chest impedance
• Displays apparent “asystole”
• Confirm rhythm with monitoring
leads

ERC
Pulseless electrical
activity
• Exclude/treat reversible causes
• Epinephrine 1 mg every 3 minutes
• Atropine 3 mg if PEA with rate < 60
min
-1

ERC
Summary
• In patients in VF/pulseless VT
attempt defibrillation without
delay
• In patients in refractory VF or
with a non-VF/VT rhythm
identify and treat any
reversible cause
Document Outline
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
Wyszukiwarka
Podobne podstrony:
ALS algorytmy , dokumenty pisma
5 Algorytm zaawansowanych zabiegów resuscytacyjnych ALS
ALGORYTM ALS, Ratownictwo Medyczne, Materiały ze studiów, Medycyna Ratunkowa
ALS - 001-000 - Zadania - ZAJECIA, Informatyka - uczelnia, WWSI i WAT, wwsi, SEM II, Algorytmy i Str
ALS - 009-005 - Program Sortowanie INSERTION SORT, Informatyka - uczelnia, WWSI i WAT, wwsi, SEM II,
ALS - 002-001, Informatyka - uczelnia, WWSI i WAT, wwsi, SEM II, Algorytmy i Struktury Danych
ALS - 004-000b - Zajęcia - STOS - LIFO - Ćwiczenie ONP, Informatyka - uczelnia, WWSI i WAT, wwsi, SE
algorytmy lista dwukierunkowa, WAT, SEMESTR II, ALS
ALS - 007-005a - Program drzewa BST, Informatyka - uczelnia, WWSI i WAT, wwsi, SEM II, Algorytmy i S
04 Algorytm ALS 28Jan06
ALS - 009-000 - Zajęcia - Sortowanie bąbelkowe, Informatyka - uczelnia, WWSI i WAT, wwsi, SEM II, Al
algorytmy kolejka, WAT, SEMESTR II, ALS
ALS - 005-001 - Program Stos ONP-RPN, Informatyka - uczelnia, WWSI i WAT, wwsi, SEM II, Algorytmy i
ALS - 004-000 - Zajęcia - Listy - teoria, Informatyka - uczelnia, WWSI i WAT, wwsi, SEM II, Algorytm
ALS - 007-002 - Program drzewa BST - AVL, Informatyka - uczelnia, WWSI i WAT, wwsi, SEM II, Algorytm
ALS - 004-002 - Program - Lista - Sito Eratostenesa, Informatyka - uczelnia, WWSI i WAT, wwsi, SEM I
algorytm ALS, ratownicto 2012 2013, ratownictwo medyczne, ALS
5 Algorytm zaawansowanych zabiegów resuscytacyjnych ALS
5 Algorytm zaawansowanych zabiegów resuscytacyjnych ALS
więcej podobnych podstron