
Benign Thyroid
Benign Thyroid
Diseases
Diseases
University of Texas Medical Branch
Dept of Otolaryngology
Grand Rounds Presentation
Alan Cowan, MD
Shawn Newlands, MD, PhD
May 2006

History
History
Goiter
Goiter
–
Fist described in China in 2700 BC
Fist described in China in 2700 BC
Thyroid Function
Thyroid Function
–
Da Vinci – thyroid is designed to fill empty spaces in the
Da Vinci – thyroid is designed to fill empty spaces in the
neck
neck
–
Parry – thyroid works as a buffer to protect the brain from
Parry – thyroid works as a buffer to protect the brain from
surges in blood flow
surges in blood flow
–
Roman physicians – thyroid enlargement is a sign of
Roman physicians – thyroid enlargement is a sign of
puberty
puberty
Cures
Cures
–
“
“
application of toad’s blood to the neck”
application of toad’s blood to the neck”
–
“
“
stroking of the thyroid gland with a cadaverous hand”
stroking of the thyroid gland with a cadaverous hand”

Surgical advances
Surgical advances
500 AD
500 AD
–
Abdul Kasan Kelebis Abis performed the first goiter excision in
Abdul Kasan Kelebis Abis performed the first goiter excision in
Baghdad.
Baghdad.
–
Procedure: unknown
Procedure: unknown
1200’s AD
1200’s AD
–
Advancements in goiter procedures included applying hot irons
Advancements in goiter procedures included applying hot irons
through the skin and slowly withdrawing them at right angles.
through the skin and slowly withdrawing them at right angles.
The remaining mass or pedicled tissue was excised.
The remaining mass or pedicled tissue was excised.
–
Patients were tied to the table and held down to prevent
Patients were tied to the table and held down to prevent
unwanted movement.
unwanted movement.
–
Most died from hemorhage or sepsis
Most died from hemorhage or sepsis
.
.
1646 AD
1646 AD
–
Wilhelm Fabricus performed a thyroidectomy with standard
Wilhelm Fabricus performed a thyroidectomy with standard
surgical scalpels.
surgical scalpels.
–
The 10 y/o girl died, and he was imprisoned
The 10 y/o girl died, and he was imprisoned
1808 AD
1808 AD
–
Guillaume Dupuytren performed a total thyroidectomy.
Guillaume Dupuytren performed a total thyroidectomy.
–
The patient died postoperatively of “shock
The patient died postoperatively of “shock
”
”

Surgical advances
Surgical advances
1866
1866
–
“
“
If a surgeon should be so foolhardy as to
If a surgeon should be so foolhardy as to
undertake it [thyroidectomy] … every step of
undertake it [thyroidectomy] … every step of
the way will be environed with difficulty, every
the way will be environed with difficulty, every
stroke of his knife will be followed by a torrent
stroke of his knife will be followed by a torrent
of blood, and lucky will it be for him if his
of blood, and lucky will it be for him if his
victim lives long enough to enable him to finish
victim lives long enough to enable him to finish
his horrid butchery.”
his horrid butchery.”
–
–
Samuel David Gross
Samuel David Gross

Surgical advances
Surgical advances
1883
1883
Kocher’s performs a retrospective review
Kocher’s performs a retrospective review
5000 career thyroidectomies
5000 career thyroidectomies
Mortality rates decreased
Mortality rates decreased
–
40% in 1850 (pre-Kocher & Bilroth)
40% in 1850 (pre-Kocher & Bilroth)
–
12.6% in 1870’s (Kocher begins practice)
12.6% in 1870’s (Kocher begins practice)
–
0.2% in 1898 (end of Kocher’s career)
0.2% in 1898 (end of Kocher’s career)
Many patients developed cretinism or myxedema
Many patients developed cretinism or myxedema
His conclusions ….
His conclusions ….

Surgical advances
Surgical advances
In presentation to the German Surgical
In presentation to the German Surgical
Congress …
Congress …
“ …
“ …
the thyroid gland in fact had a
the thyroid gland in fact had a
function….”
function….”
- Theodor Kocher, 1883
- Theodor Kocher, 1883

Medical Advances
Medical Advances
1820 AD
1820 AD
–
Johann Straub and Francois Coindet found that
Johann Straub and Francois Coindet found that
use of seaweed (iodine) reduced goiter size
use of seaweed (iodine) reduced goiter size
and vascularity
and vascularity
1830 AD
1830 AD
–
Graves and von Basedow describe a toxic
Graves and von Basedow describe a toxic
goiter condition they referred to as “Merseburg
goiter condition they referred to as “Merseburg
Triad” – goiter, exopthalmos, palpitations.
Triad” – goiter, exopthalmos, palpitations.

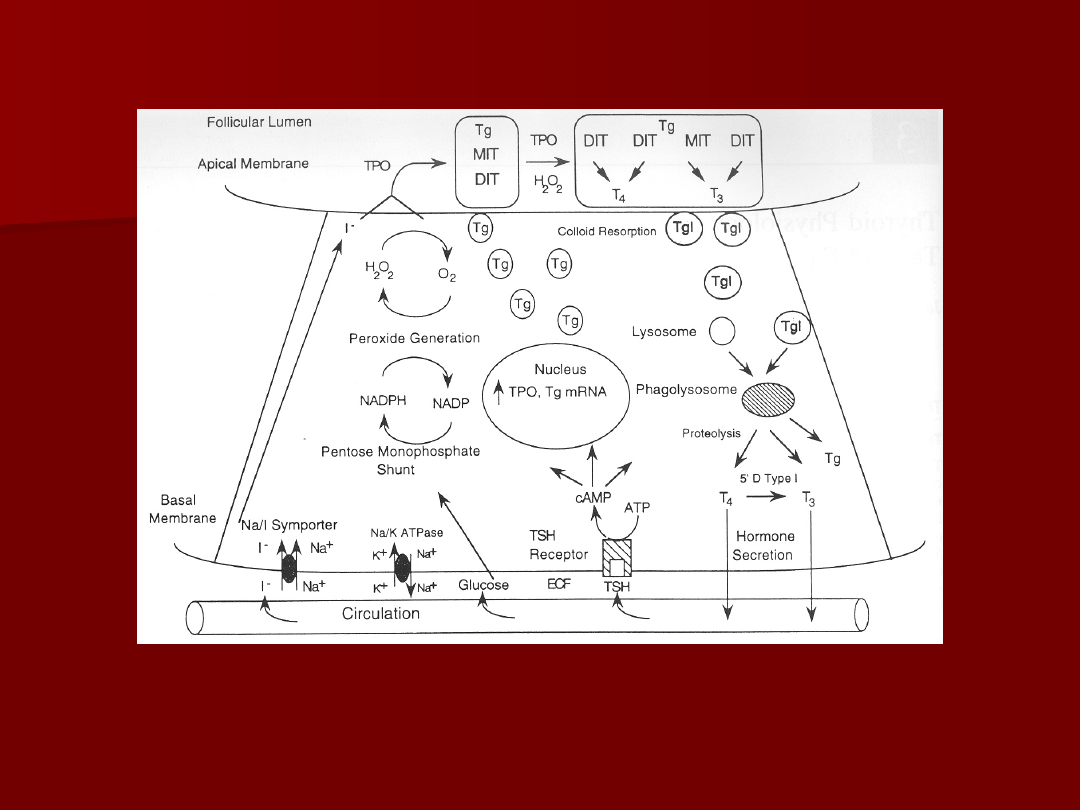
Thyroid Physiology
Thyroid Physiology
Iodine transport
Iodine transport
Na
Na
+
+
/I
/I
-
-
symport
symport
protein controls
protein controls
serum I
serum I
-
-
uptake
uptake
Based on Na
Based on Na
+
+
/K
/K
+
+
antiport potential
antiport potential
Stimulated by TSH
Stimulated by TSH
Inhibited by
Inhibited by
Perchlorate
Perchlorate

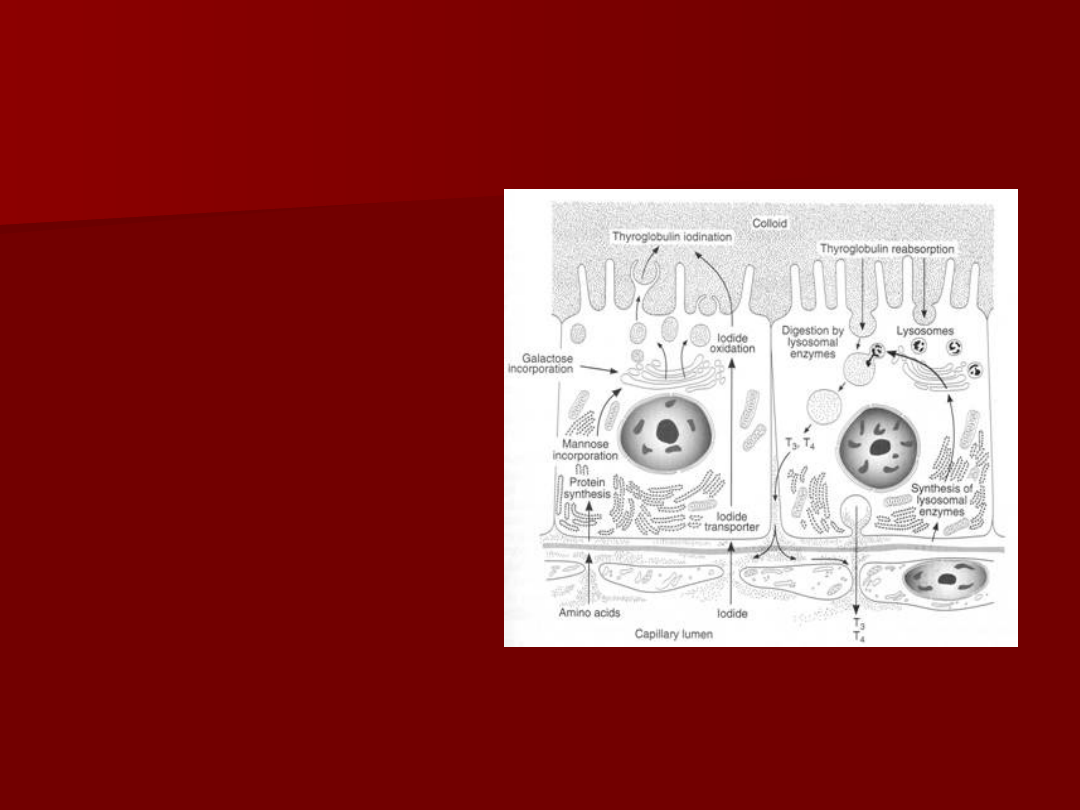
Thyroid hormone formation
Thyroid hormone formation
Thyroid Peroxidase (TPO)
Thyroid Peroxidase (TPO)
–
Apical membrane protein
Apical membrane protein
–
Catalyzes Iodine organification to tyrosine
Catalyzes Iodine organification to tyrosine
residues of thyroglobulin
residues of thyroglobulin
–
Antagonized by methimazole, PTU
Antagonized by methimazole, PTU
Iodine coupled to Thyroglobulin
Iodine coupled to Thyroglobulin
–
Monoiodotyrosine (Tg + one I
Monoiodotyrosine (Tg + one I
-
-
)
)
–
Diiodotyrosine (Tg + two I
Diiodotyrosine (Tg + two I
-
-
)
)
Pre-hormones secreted into follicular space
Pre-hormones secreted into follicular space
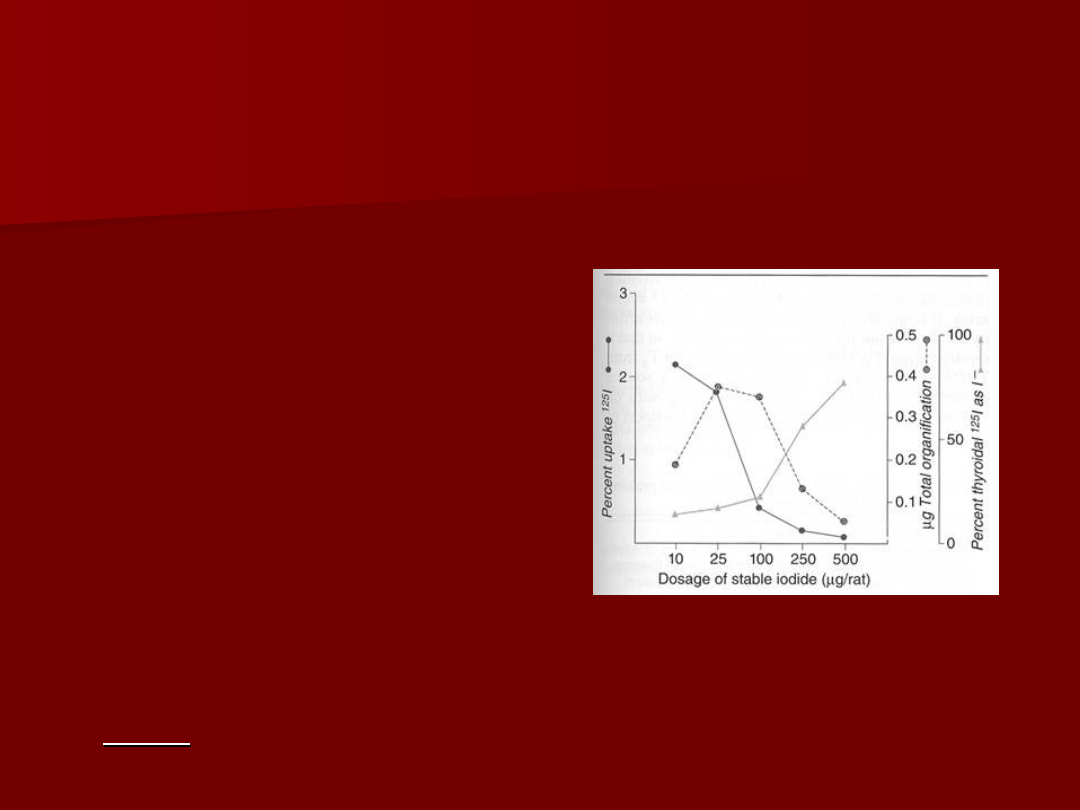
Wolff-Chaikoff Effect
Wolff-Chaikoff Effect
Increasing doses of I
Increasing doses of I
-
-
increase hormone
increase hormone
synthesis initially
synthesis initially
Higher doses cause
Higher doses cause
cessation of hormone
cessation of hormone
formation.
formation.
This effect is countered by
This effect is countered by
the Iodide leak from
the Iodide leak from
normal thyroid tissue.
normal thyroid tissue.
Patients with autoimmune
Patients with autoimmune
thyroiditis may fail to
thyroiditis may fail to
adapt and become
adapt and become
hypo
hypo
thyroid.
thyroid.
Jod-Basedow Effect
Jod-Basedow Effect
Opposite of the Wolff-Chaikoff effect
Opposite of the Wolff-Chaikoff effect
Excessive iodine loads induce
Excessive iodine loads induce
hyper
hyper
thyroidism
thyroidism
Observed in hyperthyroid disease processes
Observed in hyperthyroid disease processes
–
Graves’ disease
Graves’ disease
–
Toxic multinodular goiter
Toxic multinodular goiter
–
Toxic adenoma
Toxic adenoma
This effect may lead to symptomatic
This effect may lead to symptomatic
thyrotoxicosis in patients who receive large
thyrotoxicosis in patients who receive large
iodine doses from
iodine doses from
–
Dietary changes
Dietary changes
–
Contrast administration
Contrast administration
–
Iodine containing medication (Amiodarone)
Iodine containing medication (Amiodarone)
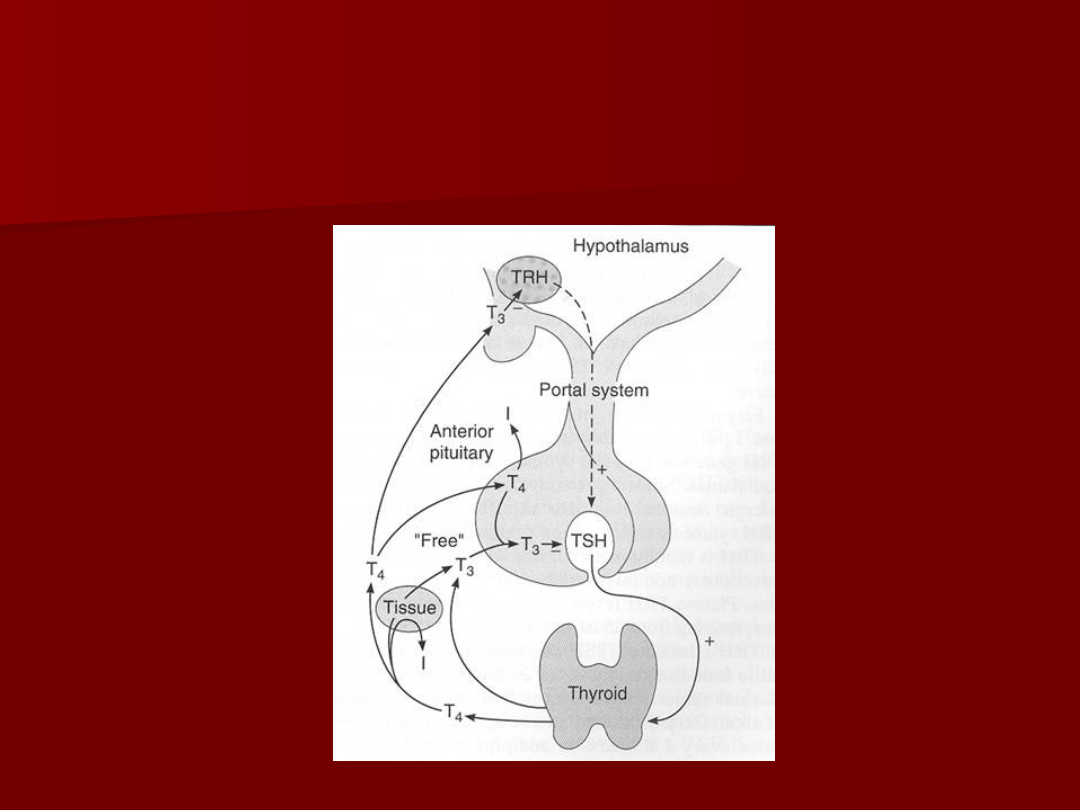
Thyroid Hormone Control
Thyroid Hormone Control

TRH
TRH
Produced by Hypothalamus
Produced by Hypothalamus
Release is pulsatile, circadian
Release is pulsatile, circadian
Downregulated by T
Downregulated by T
3
3
Travels through portal venous
Travels through portal venous
system to adenohypophysis
system to adenohypophysis
Stimulates TSH formation
Stimulates TSH formation

TSH
TSH
Produced by Adenohypophysis Thyrotrophs
Produced by Adenohypophysis Thyrotrophs
Upregulated by TRH
Upregulated by TRH
Downregulated by T
Downregulated by T
4
4
, T
, T
3
3
Travels through portal venous system to
Travels through portal venous system to
cavernous sinus, body.
cavernous sinus, body.
Stimulates several processes
Stimulates several processes
–
Iodine uptake
Iodine uptake
–
Colloid endocytosis
Colloid endocytosis
–
Growth of thyroid gland
Growth of thyroid gland
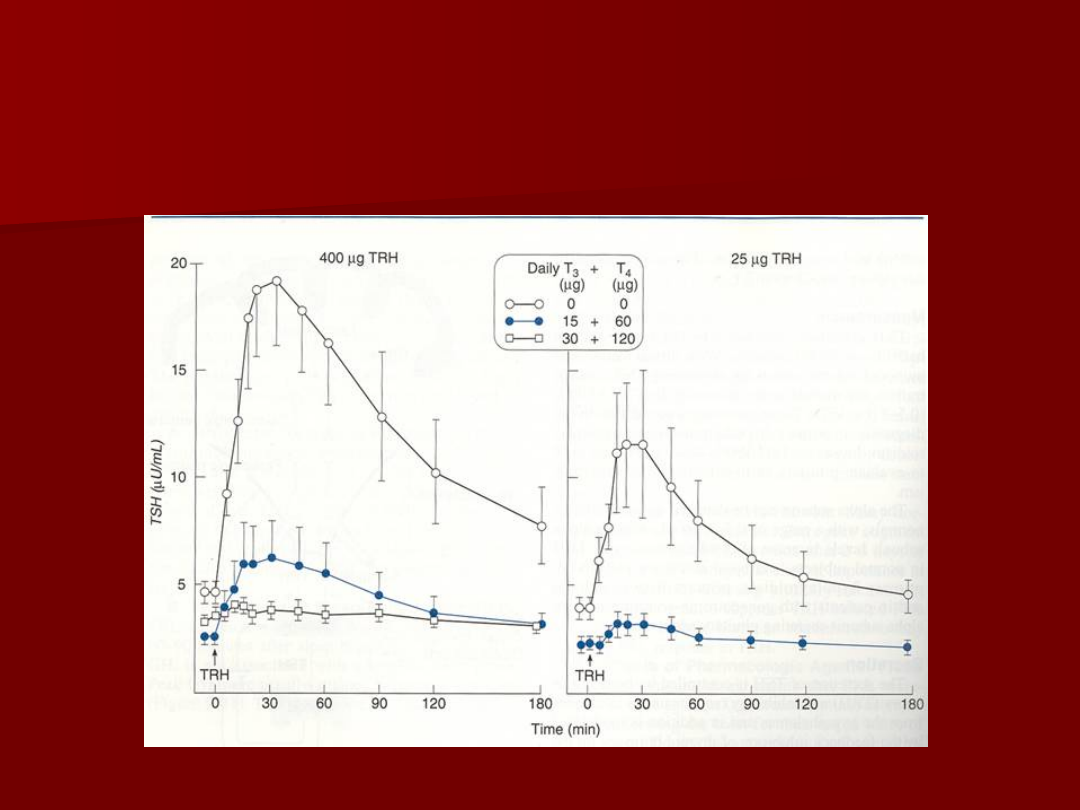
TSH Response
TSH Response

Thyroid Hormone
Thyroid Hormone
Majority of circulating hormone is T
Majority of circulating hormone is T
4
4
–
98.5% T
98.5% T
4
4
–
1.5% T
1.5% T
3
3
Total Hormone load is influenced by serum
Total Hormone load is influenced by serum
binding proteins
binding proteins
–
Albumin 15%
Albumin 15%
–
Thyroid Binding Globulin 70%
Thyroid Binding Globulin 70%
–
Transthyretin 10%
Transthyretin 10%
Regulation is based on the free component of
Regulation is based on the free component of
thyroid hormone
thyroid hormone

Hormone Binding Factors
Hormone Binding Factors
Increased TBG
Increased TBG
–
High estrogen states (pregnancy, OCP, HRT,
High estrogen states (pregnancy, OCP, HRT,
Tamoxifen)
Tamoxifen)
–
Liver disease (early)
Liver disease (early)
Decreased TBG
Decreased TBG
–
Androgens or anabolic steroids
Androgens or anabolic steroids
–
Liver disease (late)
Liver disease (late)
Binding Site Competition
Binding Site Competition
–
NSAID’s
NSAID’s
–
Furosemide IV
Furosemide IV
–
Anticonvulsants (Phenytoin, Carbamazepine)
Anticonvulsants (Phenytoin, Carbamazepine)

Thyroid Evaluation
Thyroid Evaluation
TRH
TRH
TSH
TSH
Total T
Total T
3
3
, T
, T
4
4
Free T
Free T
3
3
, T
, T
4
4
RAIU
RAIU
Thyroglobulin
Thyroglobulin
Antibodies: Anti-TPO, Anti-TSHr
Antibodies: Anti-TPO, Anti-TSHr
Thyroid Evaluation
Thyroid Evaluation

RAIU
RAIU
Scintillation counter measures radioactivity after
Scintillation counter measures radioactivity after
I
I
123
123
administration.
administration.
Uptake varies greatly by iodine status
Uptake varies greatly by iodine status
–
Indigenous diet (normal uptake 10% vs. 90%)
Indigenous diet (normal uptake 10% vs. 90%)
–
Amiodarone, Contrast study, Topical betadine
Amiodarone, Contrast study, Topical betadine
Elevated RAIU with hyperthyroid symptoms
Elevated RAIU with hyperthyroid symptoms
–
Graves’
Graves’
–
Toxic goiter
Toxic goiter
Low RAIU with hyperthyroid symptoms
Low RAIU with hyperthyroid symptoms
–
Thyroiditis (Subacute, Active Hashimoto’s)
Thyroiditis (Subacute, Active Hashimoto’s)
–
Hormone ingestion (Thyrotoxicosis factitia, Hamburger
Hormone ingestion (Thyrotoxicosis factitia, Hamburger
Thyrotoxicosis)
Thyrotoxicosis)
–
Excess I
Excess I
-
-
intake in Graves’ (Jod-Basedow effect)
intake in Graves’ (Jod-Basedow effect)
–
Ectopic thyroid carcinoma (Struma ovarii)
Ectopic thyroid carcinoma (Struma ovarii)
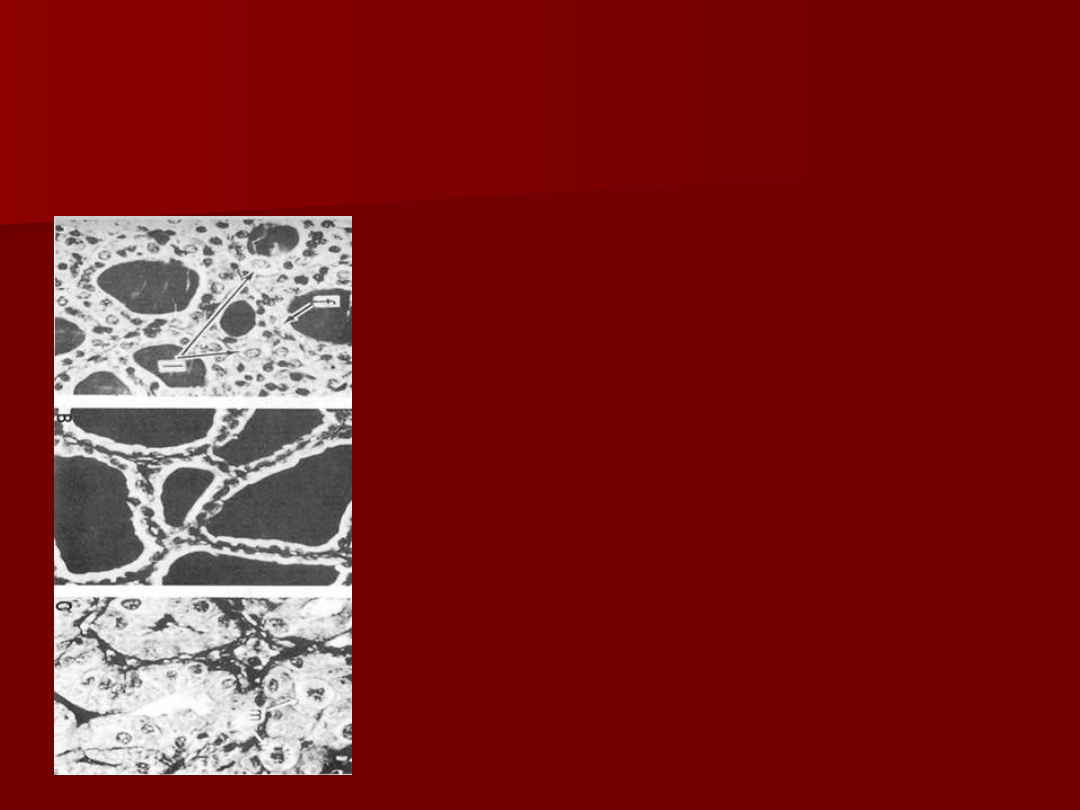
Iodine states
Iodine states
Normal Thyroid
Normal Thyroid
Inactive Thyroid
Inactive Thyroid
Hyperactive Thyroid
Hyperactive Thyroid

Common Thyroid
Common Thyroid
Disorders
Disorders

Goiter
Goiter
Goiter
Goiter
: Chronic enlargement of the thyroid gland
: Chronic enlargement of the thyroid gland
not due to neoplasm
not due to neoplasm
Endemic goiter
Endemic goiter
–
Areas where > 5% of children 6-12 years of age have
Areas where > 5% of children 6-12 years of age have
goiter
goiter
–
Common in China and central Africa
Common in China and central Africa
Sporadic goiter
Sporadic goiter
–
Areas where < 5% of children 6-12 years of age have
Areas where < 5% of children 6-12 years of age have
goiter
goiter
–
Multinodular
Multinodular
goiter
goiter
in sporatic areas often denotes the
in sporatic areas often denotes the
presence of multiple nodules rather than gross gland
presence of multiple nodules rather than gross gland
enlargement
enlargement
Familial
Familial

Goiter
Goiter
Etiology
Etiology
–
Hashimoto’s thyroiditis
Hashimoto’s thyroiditis
Early stages only, late stages show atrophic changes
Early stages only, late stages show atrophic changes
May present with hypo, hyper, or euthyroid states
May present with hypo, hyper, or euthyroid states
–
Graves’ disease
Graves’ disease
Due to chronic stimulation of TSH receptor
Due to chronic stimulation of TSH receptor
–
Diet
Diet
Brassica (cabbage, turnips, cauliflower, broccoli)
Brassica (cabbage, turnips, cauliflower, broccoli)
Cassava
Cassava
–
Chronic Iodine excess
Chronic Iodine excess
Iodine excess leads to increased colloid formation and can prevent
Iodine excess leads to increased colloid formation and can prevent
hormone release
hormone release
If a patient does not develop iodine leak, excess iodine can lead to
If a patient does not develop iodine leak, excess iodine can lead to
goiter
goiter
–
Medications
Medications
Lithium prevents release of hormone, causes goiter in 6% of chronic
Lithium prevents release of hormone, causes goiter in 6% of chronic
users
users
–
Neoplasm
Neoplasm

Goiter
Goiter
Pathogenesis
Pathogenesis
–
Iodine deficient areas
Iodine deficient areas
Heterogeneous response to TSH
Heterogeneous response to TSH
Chronic stimulation leads to multiple nodules
Chronic stimulation leads to multiple nodules
–
Iodine replete areas
Iodine replete areas
Thyroid follicles are heterogeneous in their growth and
Thyroid follicles are heterogeneous in their growth and
activity potential
activity potential
Autopsy series show MNG >30%.
Autopsy series show MNG >30%.
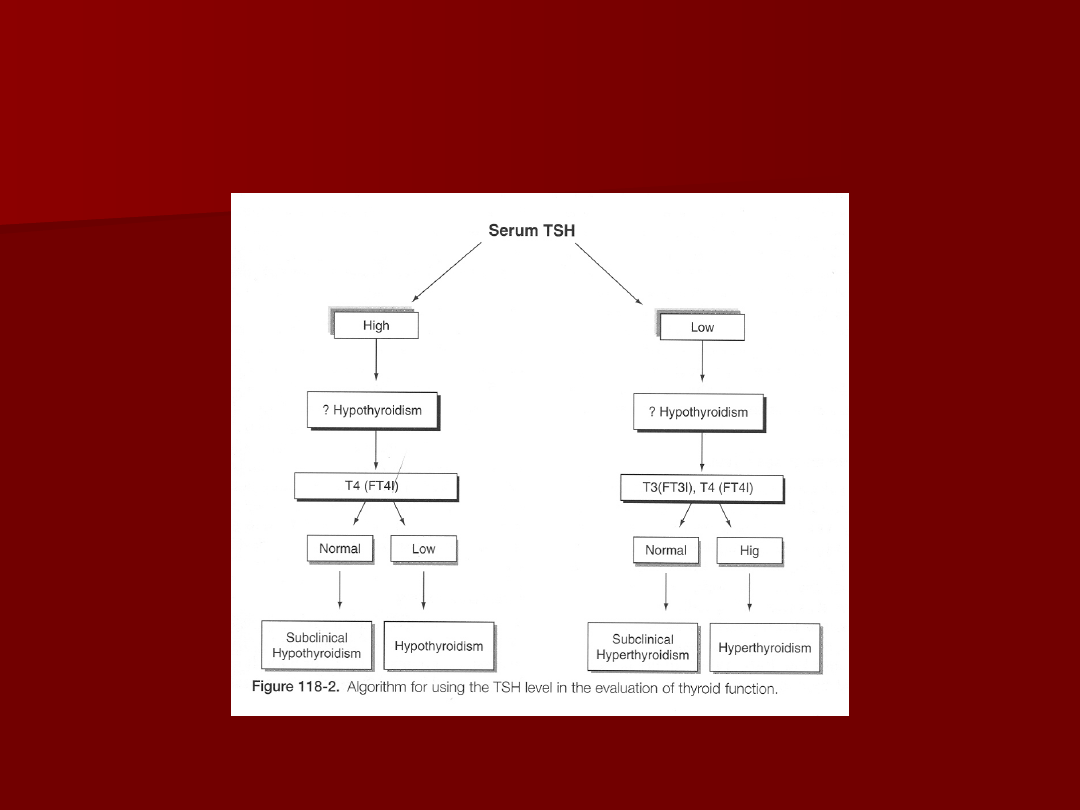
Thyroid function evaluation
Thyroid function evaluation
–
TSH, T4, T3
TSH, T4, T3
–
Overt hyperthyroidism (TSH low, T3/T4 high)
Overt hyperthyroidism (TSH low, T3/T4 high)
–
Subclinical hyperthyroidism (TSH low, T3/T4 normal)
Subclinical hyperthyroidism (TSH low, T3/T4 normal)
Determination of thyroid state is key in determining
Determination of thyroid state is key in determining
treatment
treatment

Non-Toxic Goiter
Non-Toxic Goiter
Cancer screening in non-toxic MNG
Cancer screening in non-toxic MNG
–
Longstanding MNG has a risk of malignancy identical to
Longstanding MNG has a risk of malignancy identical to
solitary nodules (<5%)
solitary nodules (<5%)
–
MNG with nodules < 1.5 cm may be followed clinically
MNG with nodules < 1.5 cm may be followed clinically
–
MNG with non-functioning nodules > 4cm should be excised
MNG with non-functioning nodules > 4cm should be excised
No FNA needed due to poor sensitivity
No FNA needed due to poor sensitivity
Incidence of cancer (up to 40%)
Incidence of cancer (up to 40%)
–
FNA in MNG
FNA in MNG
Sensitivity 85% - 95%
Sensitivity 85% - 95%
Specificity 95%
Specificity 95%
Negative FNA can be followed with annual US
Negative FNA can be followed with annual US
Insufficient FNA’s should be repeated
Insufficient FNA’s should be repeated
Incoclusive FNA or papillary cytology warrants excision
Incoclusive FNA or papillary cytology warrants excision
–
Hyperfunctioning nodules may mimic follicular neoplasm on
Hyperfunctioning nodules may mimic follicular neoplasm on
FNA
FNA

Non-Toxic Goiter
Non-Toxic Goiter
Treatment options
Treatment options
(no compressive symptoms)
(no compressive symptoms)
–
US follow-up to monitor for progression
US follow-up to monitor for progression
–
Thyroid suppression therapy
Thyroid suppression therapy
May be used for progressive growth
May be used for progressive growth
May reduce gland volume up to 50%
May reduce gland volume up to 50%
Goiter regrowth occurs rapidly following therapy cessation
Goiter regrowth occurs rapidly following therapy cessation
–
Surgery
Surgery
Suspicious neck lymphadenopathy
Suspicious neck lymphadenopathy
History of radiation to the cervical region
History of radiation to the cervical region
Rapid enlargement of nodules
Rapid enlargement of nodules
Papillary histology
Papillary histology
Microfollicular histology (?)
Microfollicular histology (?)

Non-Toxic Goiter
Non-Toxic Goiter
Treatment options
Treatment options
(compressive symptoms)
(compressive symptoms)
–
RAI ablation
RAI ablation
Volume reduction 33% - 66% in 80% of patients
Volume reduction 33% - 66% in 80% of patients
Improvement of dysphagia or dyspnea in 70% - 90%
Improvement of dysphagia or dyspnea in 70% - 90%
Post RAI hypothyroidism 60% in 8 years
Post RAI hypothyroidism 60% in 8 years
Post RAI Graves’ disease 10%
Post RAI Graves’ disease 10%
Post RAI lifetime cancer risk 1.6%
Post RAI lifetime cancer risk 1.6%
–
Surgery
Surgery
Most commonly recommended treatment for healthy
Most commonly recommended treatment for healthy
individuals
individuals

Toxic Goiter
Toxic Goiter
Evaluate for
Evaluate for
–
Graves’ disease
Graves’ disease
Clinical findings (Pretibial myxedema, Opthalmopathy)
Clinical findings (Pretibial myxedema, Opthalmopathy)
Anti-TSH receptor Ab
Anti-TSH receptor Ab
High RAUI
High RAUI
–
Thyroiditis
Thyroiditis
Clinical findings (painful thyroid in Subacute thyroiditis)
Clinical findings (painful thyroid in Subacute thyroiditis)
Low RAUI
Low RAUI
–
Recent Iodine administration
Recent Iodine administration
Amiodarone
Amiodarone
IV contrast
IV contrast
Change in diet
Change in diet
FNA evaluation
FNA evaluation
–
Not indicated in hyperthyroid nodules due to low incidence of
Not indicated in hyperthyroid nodules due to low incidence of
malignancy
malignancy
–
FNA of hyperthyroid nodules can mimic follicular neoplasms
FNA of hyperthyroid nodules can mimic follicular neoplasms

Toxic Goiter
Toxic Goiter
Risks of hyperthyroidism
Risks of hyperthyroidism
–
Atrial fibrillation
Atrial fibrillation
–
Congestive Heart Failure
Congestive Heart Failure
–
Loss of bone mineral density
Loss of bone mineral density
–
Risks exist for both clinical or subclinical disease
Risks exist for both clinical or subclinical disease
Toxic Goiter
Toxic Goiter
–
Toxicity is usually longstanding
Toxicity is usually longstanding
–
Acute toxicity may occur in hyperthyroid states (Jod
Acute toxicity may occur in hyperthyroid states (Jod
Basedow effect) with
Basedow effect) with
Relocation to iodine replete area
Relocation to iodine replete area
Contrast administration
Contrast administration
Amiodarone (37% iodine)
Amiodarone (37% iodine)

Toxic Goiter
Toxic Goiter
Treatment for Toxic MNG
Treatment for Toxic MNG
–
Thionamide medications
Thionamide medications
Not indicated for long-term use due to complications
Not indicated for long-term use due to complications
May be used for symptomatic individuals until definitive
May be used for symptomatic individuals until definitive
treatment
treatment
.
.
–
Radioiodine
Radioiodine
Primary treatment for toxic MNG
Primary treatment for toxic MNG
Large I
Large I
131
131
dose required due to gland size
dose required due to gland size
Goiter size reduction by 40% within 1 year
Goiter size reduction by 40% within 1 year
Risk of hypothyroidism
Risk of hypothyroidism
11% - 24%
11% - 24%
May require second dose
May require second dose
–
Surgery
Surgery
Used for compressive symptoms
Used for compressive symptoms
Hypothyroidism occurs in up to 70% of subtotal
Hypothyroidism occurs in up to 70% of subtotal
thyroidectomy patients
thyroidectomy patients
Pre-surgical stabilization with thionamide medications
Pre-surgical stabilization with thionamide medications
Avoid SSKI due to risk for acute toxic symptoms
Avoid SSKI due to risk for acute toxic symptoms

Graves’ Disease
Graves’ Disease
Most common cause of thyrotoxicosis in the industrialized
Most common cause of thyrotoxicosis in the industrialized
world
world
Autoimmune condition with anti-TSHr antibodies
Autoimmune condition with anti-TSHr antibodies
Onset of disease may be related to severe stress which
Onset of disease may be related to severe stress which
alters the immune response
alters the immune response
Diagnosis
Diagnosis
–
TSH, T
TSH, T
4
4
, T
, T
3
3
to establish toxicosis
to establish toxicosis
–
RAIU scan to differentiate toxic conditions
RAIU scan to differentiate toxic conditions
–
Anti-TPO, Anti-TSAb, fT
Anti-TPO, Anti-TSAb, fT
3
3
if indicated
if indicated
RAIU in Hyperthyroid States
RAIU in Hyperthyroid States
High Uptake
High Uptake
Low Uptake
Low Uptake
Graves’
Graves’
Subacute Thyroiditis
Subacute Thyroiditis
Toxic MNG
Toxic MNG
Iodine Toxicosis
Iodine Toxicosis
Toxic Adenoma
Toxic Adenoma
Thyrotoxicosis factitia
Thyrotoxicosis factitia

Graves’ Disease
Graves’ Disease
Treatment
Treatment
–
Beta blockers for symptoms
Beta blockers for symptoms
–
Thionamide medications
Thionamide medications
May re-establish euthyroidism in 6-8 weeks
May re-establish euthyroidism in 6-8 weeks
40% - 60% incidence of disease remission
40% - 60% incidence of disease remission
20% incidence of allergy (rash, itching)
20% incidence of allergy (rash, itching)
0.5% incidence of potentially fatal agranulocytosis
0.5% incidence of potentially fatal agranulocytosis
–
Radioiodine ablation
Radioiodine ablation
10% incidence of hypothyroidism at 1 year
10% incidence of hypothyroidism at 1 year
55% - 75% incidence of hypothyroidism at 10 years
55% - 75% incidence of hypothyroidism at 10 years
Avoid RAI in children and pregancy
Avoid RAI in children and pregancy
–
Surgery
Surgery
Large goiters not amenable to RAI
Large goiters not amenable to RAI
Compressive symptoms
Compressive symptoms
Children, pregnancy
Children, pregnancy
50% - 60% incidence of hypothyroidism
50% - 60% incidence of hypothyroidism

Toxic Adenoma
Toxic Adenoma
Thyrotoxicosis
Thyrotoxicosis
–
Hyperfunctioning nodules <2 cm rarely lead to
Hyperfunctioning nodules <2 cm rarely lead to
thyrotoxicosis
thyrotoxicosis
–
Most nodules leading to thyrotoxicosis are >3
Most nodules leading to thyrotoxicosis are >3
cm.
cm.
Treatment Indications
Treatment Indications
–
Post-menopausal female
Post-menopausal female
Due to increased risk of bone loss
Due to increased risk of bone loss
–
Patients over 60
Patients over 60
Due to high risk of atrial fibrillation
Due to high risk of atrial fibrillation
–
Adenomas greater than 3 cm (?)
Adenomas greater than 3 cm (?)

Toxic Adenoma
Toxic Adenoma
Treatments
Treatments
–
Antithyroid medications
Antithyroid medications
Not used due to complications of long-term treatment
Not used due to complications of long-term treatment
–
Radioiodine
Radioiodine
Cure rate > 80% (20 mCi I131)
Cure rate > 80% (20 mCi I131)
Hypothyroidism risk 5% - 10%
Hypothyroidism risk 5% - 10%
Second dose of I131 needed in 10% - 20%
Second dose of I131 needed in 10% - 20%
Patients who are symptomatically toxic may require control
Patients who are symptomatically toxic may require control
with thionamide medications before RAI to reduce risk of
with thionamide medications before RAI to reduce risk of
worsening toxicity.
worsening toxicity.
–
Surgery
Surgery
Preferred for children and adolescents
Preferred for children and adolescents
Preferred for very large nodules when high I131 doses
Preferred for very large nodules when high I131 doses
needed
needed
Low risk of hypothyroidism
Low risk of hypothyroidism
–
Ethanol Injection
Ethanol Injection
Rarely done in the US
Rarely done in the US
May achieve cure in 80%
May achieve cure in 80%

Hypothyroidism
Hypothyroidism
Symptoms – fatigability, coldness, weight gain,
Symptoms – fatigability, coldness, weight gain,
constipation, low voice
constipation, low voice
Signs – Cool skin, dry skin, swelling of
Signs – Cool skin, dry skin, swelling of
face/hands/legs, slow reflexes, myxedema
face/hands/legs, slow reflexes, myxedema
Newborn – Retardation, short stature, swelling
Newborn – Retardation, short stature, swelling
of face/hands, possible deafness
of face/hands, possible deafness
Types of Hypothyroidism
Types of Hypothyroidism
–
Primary – Thyroid gland failure
Primary – Thyroid gland failure
–
Secondary – Pituitary failure
Secondary – Pituitary failure
–
Tertiary – Hypothalamic failure
Tertiary – Hypothalamic failure
–
Peripheral resistance
Peripheral resistance

Hypothyroidism
Hypothyroidism
Cause is determined by geography
Cause is determined by geography
–
Hashimoto’s in industrialized countries
Hashimoto’s in industrialized countries
–
May be due to iodine excess in some costal areas
May be due to iodine excess in some costal areas
Diagnosis
Diagnosis
–
Low FT
Low FT
4
4
, High TSH (Primary, check for antibodies)
, High TSH (Primary, check for antibodies)
–
Low FT
Low FT
4
4
, Low TSH (Secondary or Tertiary, TRH
, Low TSH (Secondary or Tertiary, TRH
stimulation test, MRI)
stimulation test, MRI)
Treatment
Treatment
–
Levothyroxine (T
Levothyroxine (T
4
4
) due to longer half life
) due to longer half life
–
Treatment prevents bone loss, cardiomyopathy,
Treatment prevents bone loss, cardiomyopathy,
myxedema
myxedema

Hypothyroidism
Hypothyroidism
Agenesis
Agenesis
Thyroid destruction
Thyroid destruction
–
Hashimoto’s thyroiditis
Hashimoto’s thyroiditis
–
Surgery
Surgery
–
I
I
131
131
ablation
ablation
–
Infiltrative diseases
Infiltrative diseases
–
Post-laryngectomy
Post-laryngectomy
Inhibition of function
Inhibition of function
–
Iodine deficiency
Iodine deficiency
–
Iodine administration
Iodine administration
–
Anti-thyroid medications (PTU, Methimazole, Lithium, Interferon)
Anti-thyroid medications (PTU, Methimazole, Lithium, Interferon)
–
Inherited defects
Inherited defects
Transient
Transient
–
Postpartum
Postpartum
–
Thyroiditis
Thyroiditis
Hashimoto’s
Hashimoto’s
(Chronic, Lymphocytic)
(Chronic, Lymphocytic)
Most common cause of hypothyroidism
Most common cause of hypothyroidism
Result of antibodies to TPO, TBG
Result of antibodies to TPO, TBG
Commonly presents in females 30-50 yrs.
Commonly presents in females 30-50 yrs.
Usually non-tender and asymptomatic
Usually non-tender and asymptomatic
Lab values
Lab values
–
High TSH
High TSH
–
Low T
Low T
4
4
–
Anti-TPO Ab
Anti-TPO Ab
–
Anti-TBG Ab
Anti-TBG Ab
Treat with Levothyroxine
Treat with Levothyroxine

Thyroiditis
Thyroiditis

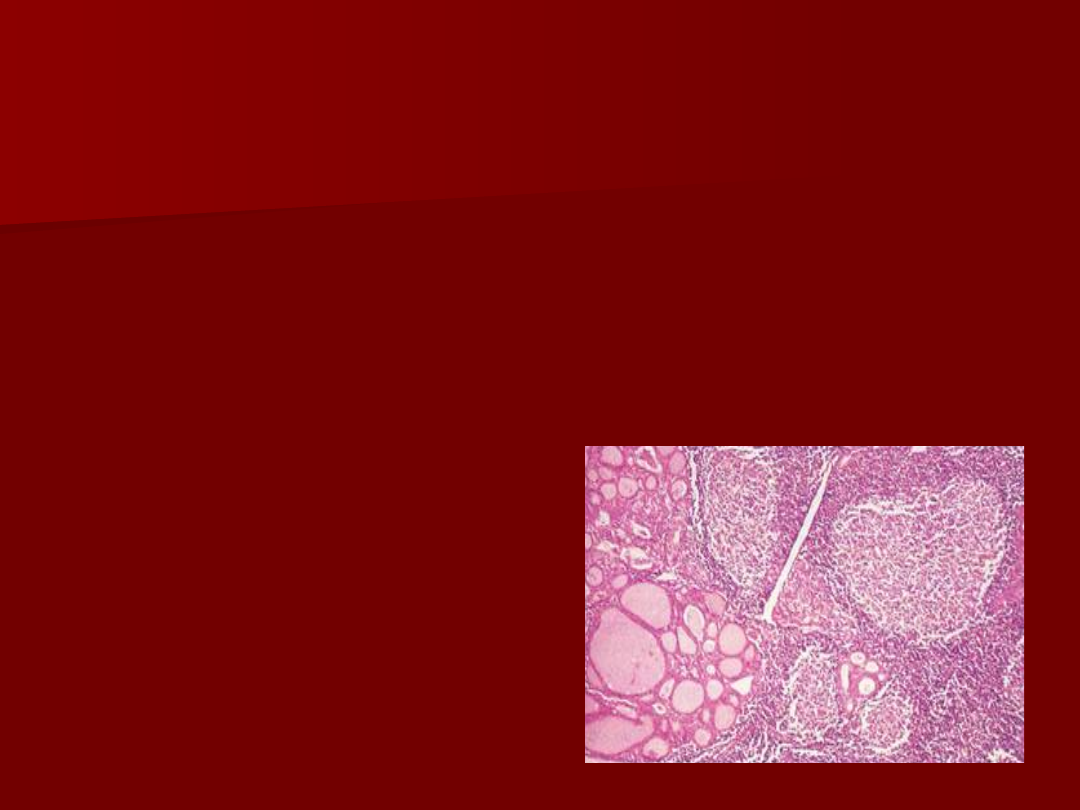
Hashimoto’s Thyroiditis
Hashimoto’s Thyroiditis
Most common cause of goiter and hypothyroidism in the U.S.
Most common cause of goiter and hypothyroidism in the U.S.
Physical
Physical
–
Painless diffuse goiter
Painless diffuse goiter
Lab studies
Lab studies
–
Hypothyroidism
Hypothyroidism
–
Anti TPO antibodies (90%)
Anti TPO antibodies (90%)
–
Anti Thyroglobulin antibodies (20-50%)
Anti Thyroglobulin antibodies (20-50%)
–
Acute Hyperthyroidism (5%)
Acute Hyperthyroidism (5%)
Treatment
Treatment
–
Levothyroxine if hypothyroid
Levothyroxine if hypothyroid
–
Triiodothyronine (for myxedema coma)
Triiodothyronine (for myxedema coma)
–
Thyroid suppression (levothyroxine) to decrease goiter size
Thyroid suppression (levothyroxine) to decrease goiter size
Contraindications
Contraindications
Stop therapy if no resolution noted
Stop therapy if no resolution noted
–
Surgery for compression or pain.
Surgery for compression or pain.

Silent Thyroiditis
Silent Thyroiditis
Post-partum Thyroiditis
Post-partum Thyroiditis
Silent thyroiditis is termed post-partum thyroiditis if it
Silent thyroiditis is termed post-partum thyroiditis if it
occurs within one year of delivery.
occurs within one year of delivery.
Clinical
Clinical
–
Hyperthyroid symptoms at presentation
Hyperthyroid symptoms at presentation
–
Progression to euthyroidism followed by hypothyroidism for up
Progression to euthyroidism followed by hypothyroidism for up
to 1 year.
to 1 year.
–
Hypothyroidism generally resolves
Hypothyroidism generally resolves
Diagnosis
Diagnosis
–
May be confused with post-partum Graves’ relapse
May be confused with post-partum Graves’ relapse
Treatment
Treatment
–
Beta blockers during toxic phase
Beta blockers during toxic phase
–
No anti-thyroid medication indicated
No anti-thyroid medication indicated
–
Iopanoic acid (Telopaque) for severe hyperthyroidism
Iopanoic acid (Telopaque) for severe hyperthyroidism
–
Thyroid hormone during hypothyroid phase. Must withdraw in
Thyroid hormone during hypothyroid phase. Must withdraw in
6 months to check for resolution.
6 months to check for resolution.

Subacute Thyroiditis
Subacute Thyroiditis
DeQuervain’s, Granulomatous
DeQuervain’s, Granulomatous
Most common cause of
Most common cause of
painful thyroiditis
painful thyroiditis
Often follows a URI
Often follows a URI
FNA may reveal
FNA may reveal
multinuleated giant cells or
multinuleated giant cells or
granulomatous change.
granulomatous change.
Course
Course
–
Pain and thyrotoxicosis (3-
Pain and thyrotoxicosis (3-
6 weeks)
6 weeks)
–
Asymptomatic
Asymptomatic
euthyroidism
euthyroidism
–
Hypothyroid period (weeks
Hypothyroid period (weeks
to months)
to months)
–
Recovery (complete in
Recovery (complete in
95% after 4-6 months)
95% after 4-6 months)

Subacute Thyroiditis
Subacute Thyroiditis
DeQuervain’s, Granulomatous
DeQuervain’s, Granulomatous
Diagnosis
Diagnosis
–
Elevated ESR
Elevated ESR
–
Anemia (normochromic, normocytic)
Anemia (normochromic, normocytic)
–
Low TSH, Elevated T4 > T3, Low anti-TPO/Tgb
Low TSH, Elevated T4 > T3, Low anti-TPO/Tgb
–
Low RAI uptake (same as silent thyroiditis)
Low RAI uptake (same as silent thyroiditis)
Treatment
Treatment
–
NSAID’s and salicylates.
NSAID’s and salicylates.
–
Oral steroids in severe cases
Oral steroids in severe cases
–
Beta blockers for symptoms of hyperthyroidism, Iopanoic acid
Beta blockers for symptoms of hyperthyroidism, Iopanoic acid
for severe symptoms
for severe symptoms
–
PTU not indicated since excess hormone results from leak
PTU not indicated since excess hormone results from leak
instead of hyperfunction
instead of hyperfunction
–
Symptoms can recur requiring repeat treatment
Symptoms can recur requiring repeat treatment
–
Graves’ disease may occasionally develop as a late sequellae
Graves’ disease may occasionally develop as a late sequellae

Acute Thyroiditis
Acute Thyroiditis
Causes
Causes
–
68% Bacterial (S. aureus, S. pyogenes)
68% Bacterial (S. aureus, S. pyogenes)
–
15% Fungal
15% Fungal
–
9% Mycobacterial
9% Mycobacterial
May occur secondary to
May occur secondary to
–
Pyriform sinus fistulae
Pyriform sinus fistulae
–
Pharyngeal space infections
Pharyngeal space infections
–
Persistent Thyroglossal remnants
Persistent Thyroglossal remnants
–
Thyroid surgery wound infections (rare)
Thyroid surgery wound infections (rare)
More common in HIV
More common in HIV

Acute Thyroiditis
Acute Thyroiditis
Diagnosis
Diagnosis
–
Warm, tender, enlarged thyroid
Warm, tender, enlarged thyroid
–
FNA to drain abscess, obtain culture
FNA to drain abscess, obtain culture
–
RAIU normal (versus decreased in DeQuervain’s)
RAIU normal (versus decreased in DeQuervain’s)
–
CT or US if infected TGDC suspected
CT or US if infected TGDC suspected
Treatment
Treatment
–
High mortality without prompt treatment
High mortality without prompt treatment
–
IV Antibiotics
IV Antibiotics
Nafcillin / Gentamycin or Rocephin for empiric therapy
Nafcillin / Gentamycin or Rocephin for empiric therapy
–
Search for pyriform fistulae (BA swallow, endoscopy)
Search for pyriform fistulae (BA swallow, endoscopy)
–
Recovery is usually complete
Recovery is usually complete

Riedel’s Thyroiditis
Riedel’s Thyroiditis
Rare disease involving fibrosis of the thyroid gland
Rare disease involving fibrosis of the thyroid gland
Diagnosis
Diagnosis
–
Thyroid antibodies are present in 2/3
Thyroid antibodies are present in 2/3
–
Painless goiter “woody”
Painless goiter “woody”
–
Open biopsy often needed to diagnose
Open biopsy often needed to diagnose
–
Associated with focal sclerosis syndromes (retroperitoneal,
Associated with focal sclerosis syndromes (retroperitoneal,
mediastinal, retroorbital, and sclerosing cholangitis)
mediastinal, retroorbital, and sclerosing cholangitis)
Treatment
Treatment
–
Resection for compressive symptoms
Resection for compressive symptoms
–
Chemotherapy with Tamoxifen, Methotrexate, or steroids
Chemotherapy with Tamoxifen, Methotrexate, or steroids
may be effective
may be effective
–
Thyroid hormone only for symptoms of hypothyroidism
Thyroid hormone only for symptoms of hypothyroidism
Document Outline
- Benign Thyroid Diseases
- History
- Surgical advances
- Slide 4
- Slide 5
- Slide 6
- Medical Advances
- Thyroid Physiology
- Iodine transport
- Thyroid hormone formation
- Slide 11
- Wolff-Chaikoff Effect
- Jod-Basedow Effect
- Thyroid Hormone Control
- TRH
- TSH
- TSH Response
- Thyroid Hormone
- Hormone Binding Factors
- Thyroid Evaluation
- Slide 22
- RAIU
- Iodine states
- Common Thyroid Disorders
- Goiter
- Slide 27
- Slide 28
- Non-Toxic Goiter
- Slide 30
- Slide 31
- Toxic Goiter
- Slide 33
- Slide 34
- Graves’ Disease
- Slide 36
- Toxic Adenoma
- Slide 38
- Hypothyroidism
- Slide 40
- Slide 41
- Hashimoto’s (Chronic, Lymphocytic)
- Thyroiditis
- Hashimoto’s Thyroiditis
- Silent Thyroiditis Post-partum Thyroiditis
- Subacute Thyroiditis DeQuervain’s, Granulomatous
- Slide 47
- Acute Thyroiditis
- Slide 49
- Riedel’s Thyroiditis
Wyszukiwarka
Podobne podstrony:
Positron emission tomography slides
EurRad Ultrasound of thyroid, parathyroid glands and neck lymph nodes
jj slides tex
credit slides 1
2007 4 JUL The Thyroid
slides01
Criando Bons Slides
Munsell Slides
Chaos Deterministyczny p19 slides
Vision Slides
Criando Slides
lecture slides 05
F99 Carley slides
Electrocardiograms slides
hai burden slides notes 2002
ZW Pol pien PP 2011 2012 odcinek 1 dla studentów slides z wykładów w dniach 02 16 10 2011
lecture slides
więcej podobnych podstron