Update for chapter 23: How evidence-based is our clinical examination of the ankle?
C. Niek van Dijk, Heleen Sonneveld
Supination injuries of the ankle ligament are among the most common injuries. They account for about
25% of all injuries in the musculoskeletal system. The most commonly injured part of the lateral ligament
complex is the anterior talofibular ligament. In case of a multiligament rupture apart from the anterior talofibular
ligament the calcaneofibular ligament is ruptured concomitantly. The calcaneofibular ligament apart from
stabilising the ankle joint is a primary stabiliser of the subtalar joint as well. Theoretically a subtalar instability is
present in this situation.
Subtalar instability
In case of a multiligament rupture apart from the ATFL the calcaneofibular ligament is ruptured
concomitantly. Theoretically a subtalar instability is present in this situation. Apart from this combined problem
subtalar instability can also be an isolated problem.
In the acute phase the combined ligment rupture resembles the isolated ATFL rupture with swelling, haematoma
discoloration, pain on palpation and positive ADT. The chronic subtalar instability presents late with complaints
of persistent instability. The clinical examination includes local pain over the sinus tarsi and increased inversion
to the hindfoot and increased external rotation or medial translation of the calcaneus only described by very
experienced examiners.
There are several methods described for imaging subtalar instability, like stress tomografy, subtalar
arthrography, Broden stress view, CT scanning and more recently MRI and diagnostic subtalar arthroscopy.
Arthrography and arthroscopy are invasive procedures with accompanying risks at complications. The stress
radiography is still in favor because subtalar instability is a dynamical problem. However in recent literature no
gold standard has been described.
Acute multiligamentair leasions are treated the same way as ATFL leasions. There is no evidence for
primary surgery. Like other hindfoot injuries, many patients improve with conservative measures. Proprioceptive
training and peroneal strengthening gave better results than casting or taping and ROM exercises.
1
There is not enough evidence in the literature for clinical and radiological diagnostics of subtalar
instability, but because the treatment and final results resemble those of the isolated ATFL rupture diagnostics in
the acute situation can be limited to diagnostics for the ATFL.
Discussion
In recent literature we didn’t find any new evidence about physical examination of the ankle or
diagnosis of the sprained ankle.
Delayed physical examination still provides a diagnostic modality with a high sensitivity and
specificity. This strategy has been confirmed to be the strategy of choice in an editorial in the British Journal of
Bone and Joint Surgery.
References:
1. Keefe DT, Haddad SL. Subtalar instability. Etiology, diagnosis, and management. Foot Ankle Clin. 2002
;7(3):577-609.
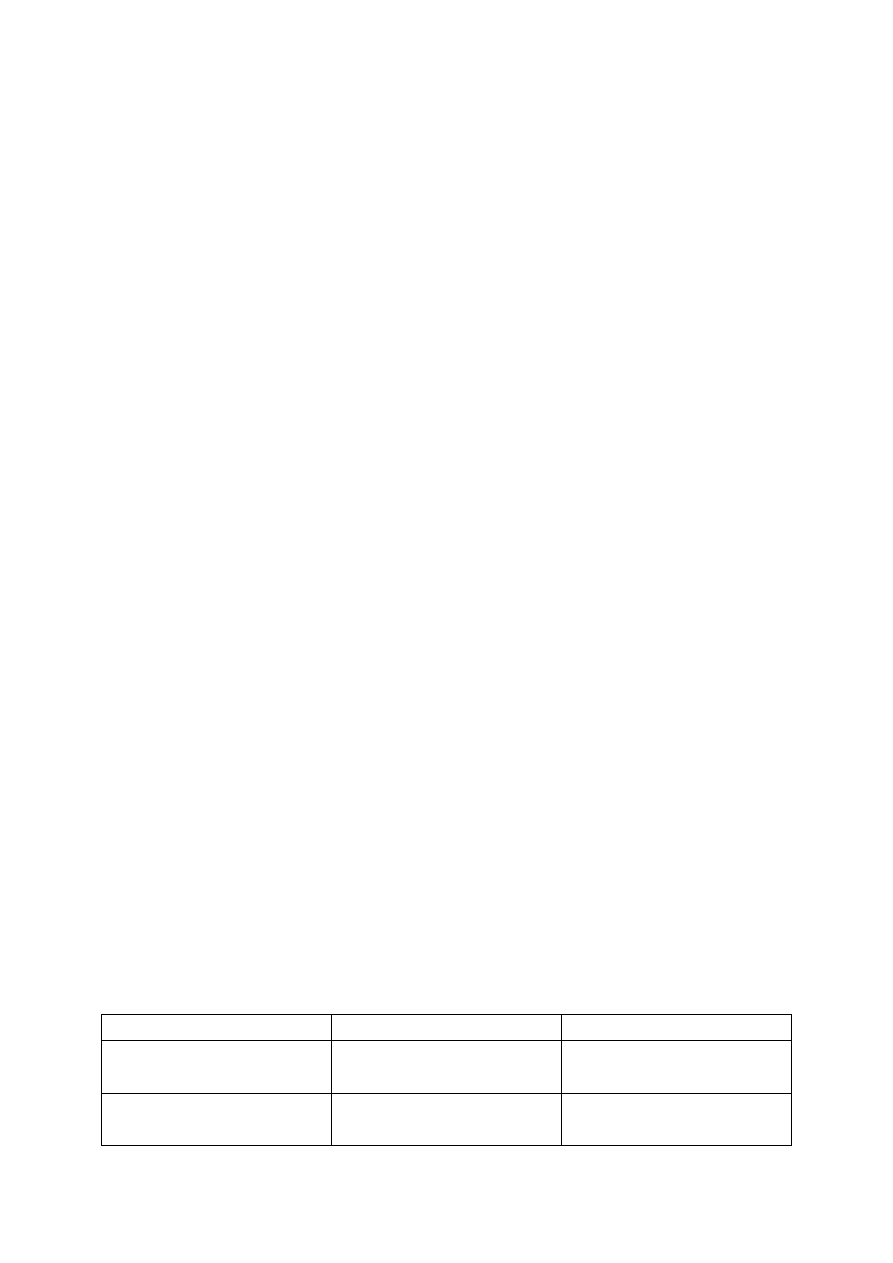
Summarizing the evidence
Comparison
Results
Level of evidence
Delayed physical examination
versus arthrography
3 CTs all of moderate or large size
proved no diffeence in outcome
Grade A1
Physical examination <48 hours
versus arthrography
5 CTs 2 of large size pooled in
favor of arthrography
Grade A4

3 Multiple Choice Questions
1. The diagnosis of acute lateral ankle ligament rupture is based on:
a. result of physical examination
b. result of physical exam + stress X-rays
c. result of physical exam + arthrography
d. result of physical exam + echography
e. stress X-rays, arthrography or echography
2. The outcome of physical examination for detection of an acute lateral ankle ligament rupture is based on:
a. inspection
b. palpation
c. manual anterior drawer test
d. A+B+C
e. Talar tilt test
3. The best available treatment for an acute lateral ankle ligament rupture is:
a. supervised neglect (=no treatment)
b. elastic support
c. inelastic tape bandage
d. brace
e. operative treatment

The right answers are: 1 – a, 2 – d, 3 - e
Document Outline
- Subtalar instability
- There are several methods described for imaging subtalar instability, like stress tomografy, subtalar arthrography, Broden stress view, CT scanning and more recently MRI and diagnostic subtalar arthroscopy. Arthrography and arthroscopy are invasive proce
- Acute multiligamentair leasions are treated the same way as ATFL leasions. There is no evidence for primary surgery. Like other hindfoot injuries, many patients improve with conservative measures. Proprioceptive training and peroneal strengthening gave
- There is not enough evidence in the literature for clinical and radiological diagnostics of subtalar instability, but because the treatment and final results resemble those of the isolated ATFL rupture diagnostics in the acute situation can be limited to
- Delayed physical examination still provides a diagnostic modality with a high sensitivity and specificity. This strategy has been confirmed to be the strategy of choice in an editorial in the British Journal of Bone and Joint Surgery.
- 3 Multiple Choice Questions
Wyszukiwarka
Podobne podstrony:
updatejpegprocessing(1)
cpu364 update instructions
BW ch23
Bluetooth update AVIC Fxxx Ver330
Instrukcja Aktualizacji modelu KDL 32EX720 TV Firmware update
cpu363 update instructions
5 4 5 Lab Create Accounts and Update
Ch23 pg753 774
mpdm upDATE
SOP, Sop-wyklady Brzezinski update!, Programowanie współbieżne
Instalacja ROMów KDZ Updater LG L9 P760
Wykład 3 updated
D&D 3 5 PHB, DMG, & Monster Manual, Update 3 0 to 3 5
fgtech galletto v54 ecu passing test(06 16 2015 update)
Intr to Stud of Lit updated 119 09
Installing Windows 7 or Windows Server 2008 R2 from USB Stick Jaxidian Update
G500 GPS firmware Update Instruction Guide
więcej podobnych podstron