
doi: 10.2522/ptj.20070179
Originally published online July 10, 2008
2008; 88:947-955.
PHYS THER.
Biricolti and Lucio A Rinaldi
Marco Baccini, Matteo Paci, Luca Nannetti, Claudia
Validity
Diagnosing ''Pusher Behavior'' and Construct
Scale for Contraversive Pushing: Cutoff Scores for
http://ptjournal.apta.org/content/88/8/947
found online at:
The online version of this article, along with updated information and services, can be
Collections
in the following collection(s):
This article, along with others on similar topics, appears
e-Letters
"Responses" in the online version of this article.
"Submit a response" in the right-hand menu under
To submit an e-Letter on this article, click
E-mail alerts
Scale for Contraversive Pushing:
Cutoff Scores for Diagnosing “Pusher
Behavior” and Construct Validity
Marco Baccini, Matteo Paci, Luca Nannetti, Claudia Biricolti, Lucio A Rinaldi
Background and Purpose.
Considerable disagreement exists among research-
ers with regard to the prevalence, pathophysiology, and treatment of “pusher be-
havior” (PB), partly because of different testing procedures. This study was primarily
aimed at establishing cutoff scores for and the construct validity of the Scale for
Contraversive Pushing (SCP). The prevalence of PB in people with right- and left-brain
lesions also was investigated.
Subjects and Methods.
The study subjects were 105 consecutive patients
with recent stroke. Two methods were used to diagnose PB: clinical examination and
SCP score with 3 different cutoff points—an SCP total score of greater than 0 (Crit_1),
subscores in each section of the scale of greater than 0 (Crit_2), and subscores in each
section of the scale of
ⱖ1 (Crit_3). Clinical and SCP diagnoses were independently
made by different examiners. The Cohen
coefficient was used to determine the
agreement between clinical and SCP diagnoses. The construct validity of the SCP was
estimated by calculation of Spearman rank correlation coefficients for SCP and
balance, mobility, and functional scores.
Results.
The agreement between clinical and SCP diagnoses was low (
⫽.212)
when Crit_1 was used. Crit_2 led to the highest agreement with the clinical diagnosis
(
⫽.933). However, only Crit_3, although globally less accurate (⫽.754), ensured
no false-positive results. The construct validity of the SCP was demonstrated by
significant (P
⬍.001) moderate to high correlations with mobility (rho⫽.595), func-
tional (rho
⫽.632), and balance (rho⫽.666) scores. The prevalence of PB was not
influenced by the side of the lesion. A limitation of the study was that the reliability
of the clinical examination method was not investigated.
Discussion and Conclusion.
The results support the validity of the SCP and
suggest the need to choose different SCP cutoff criteria (Crit_2 or Crit_3) according
to the aim of the evaluation.
M Baccini, PT, MSc, is Physical
Therapist, Unit of Functional Re-
education, Azienda Sanitaria di
Firenze, and Director, Motion
Analysis Laboratory, Piero Palagi
Hospital, Florence, Italy. He also is
a consultant for the Rehabilitation
Center of the Filippo Turati Foun-
dation, Gavinana Pistoia, Italy,
and a contractor professor in
physical therapy (first and second
degrees) at Florence University,
Florence, Italy. Institution mailing
address:
Azienda
Sanitaria
di
Firenze, Laboratorio di Analisi del
Movimento,
Ospedale
Piero
Palagi, Viale Michelangiolo 41,
50125 Florence, Italy. Address all
correspondence to Mr Baccini at:
marco.baccini@asf.toscana.it.
M Paci, PT, MSc, is Physical Ther-
apist, Villa Fiorita Hospital, Prato,
Italy, and is a contractor professor
in physical therapy (first degree) at
Florence University.
L Nannetti, MD, is Specialist in Ge-
riatrics and Geriatrician, Azienda
Sanitaria, 4 di Prato, Prato, Italy.
C Biricolti, PT, MSc, is Physical
Therapist, Unit of Functional Re-
education, Azienda Sanitaria di
Firenze, Piero Palagi Hospital, and
Bobath Instructor (I.B.I.T.A.) and a
contractor professor in physical
therapy (first degree) at Florence
University.
LA Rinaldi, PT, MSc, is Assistant
Professor and Director, Motion
Analysis and Neurorehabilitation
Laboratory, Department of Critical
Care Medicine and Surgery, Unit
of
Gerontology
and
Geriatric
Medicine, Florence University.
[Baccini M, Paci M, Nannetti L,
et al. Scale for Contraversive Push-
ing: cutoff scores for diagnosing
“pusher behavior” and construct
validity.
Phys
Ther.
2008;88:
947–955.]
© 2008 American Physical Therapy
Association
Research Report
Post a Rapid Response or
find The Bottom Line:
www.ptjournal.org
August 2008
Volume 88
Number 8
Physical Therapy
f
947

“P
usher behavior” (PB) is a
poorly understood disorder
exhibited by some people
with stroke. This behavior has 3 typ-
ical features: (1) contralesional tilted
posture
with
severe
imbalance,
(2) tendency to push strongly to-
ward the paretic side with the non-
affected limbs, and (3) resistance to
external correction of the tilted pos-
ture.
1
Researchers have reported dif-
ferent findings with regard to the
prevalence of PB in the acute phase
after stroke. Some authors found that
5% to 10% of people receiving reha-
bilitation for stroke exhibited the be-
havior,
2– 4
but others reported nota-
bly higher values, from 40% to 50%
5
and 63%.
6
Most likely, this large dis-
crepancy is mainly attributable to the
use of different criteria for diagnosis,
although it also may be a function of
the interval between stroke onset
and examination. Other terms that
occasionally have been used to indi-
cate postural control problems simi-
lar to PB in people who have had a
stroke are “listing phenomenon”
3,7
and “lateropulsion,”
8
but these terms
have not been used with a unique
meaning. Recently, Karnath
9
made a
useful terminological distinction by
indicating precisely that active push-
ing and resistance to correction of
posture are the main features that
distinguish PB from other postural
disorders in stroke.
Although few data are available, PB
may hinder or at least delay func-
tional recovery, especially balance
and gait functions.
2
Therefore, in re-
cent years, this behavior has re-
ceived increasing interest. There is
growing agreement that PB reflects
some misrepresentation of verticali-
ty,
10,11
but the exact mechanism is
still unclear. The orientation of the
body relative to the gravito-inertial
force requires an implicit represen-
tation of verticality that is critical for
balance control. This representation
is based on visual, somesthetic, and
vestibular
information.
11
Because
people who have had a stroke may
show a biased perception of upright-
ness,
12
it has been suggested that PB
may emerge as an extreme form of
this misrepresentation; that is, peo-
ple with PB may tend to align their
body posture with a contralesionally
tilted perceived vertical.
11
Indeed,
Perennou et al
11
measured the seg-
mental body orientation in people
who had PB and who were seated on
a laterally unstable, rocking platform
and were asked to keep their bodies
aligned to the vertical. The authors
found that these people were able to
align the head correctly to the verti-
cal but showed a remarkable tilting
of the pelvis toward the contra-
lesional side. In contrast to these re-
sults, Karnath et al
10
found that peo-
ple with PB, in the absence of vision,
felt that their bodies were oriented
upright when they were tilted an
average of 18 degrees to the ipsi-
lesional, rather than to the contra-
lesional, side; moreover, the per-
ceived vertical of these people was
within normal limits when they were
allowed to view the structured sur-
roundings. Therefore, the authors
hypothesized that the disorder may
be the consequence of a conflict be-
tween 2 reference systems, that is,
a normal visual vertical and an ipsi-
lesionally tilted postural vertical.
Not surprisingly, the rehabilitation
approaches suggested on the basis
of these pathophysiological findings
are quite different.
10,13
Valid and reliable assessment instru-
ments are necessary to identify the
presence and the severity of the
behavior, to study the underlying
mechanisms, to compare the effec-
tiveness of different treatment strat-
egies, and to define the prevalence
and the prognosis of the disorder.
Karnath et al
10
developed an assess-
ment tool, the Scale for Contraver-
sive Pushing (SCP), aimed at diag-
nosing the presence of PB and
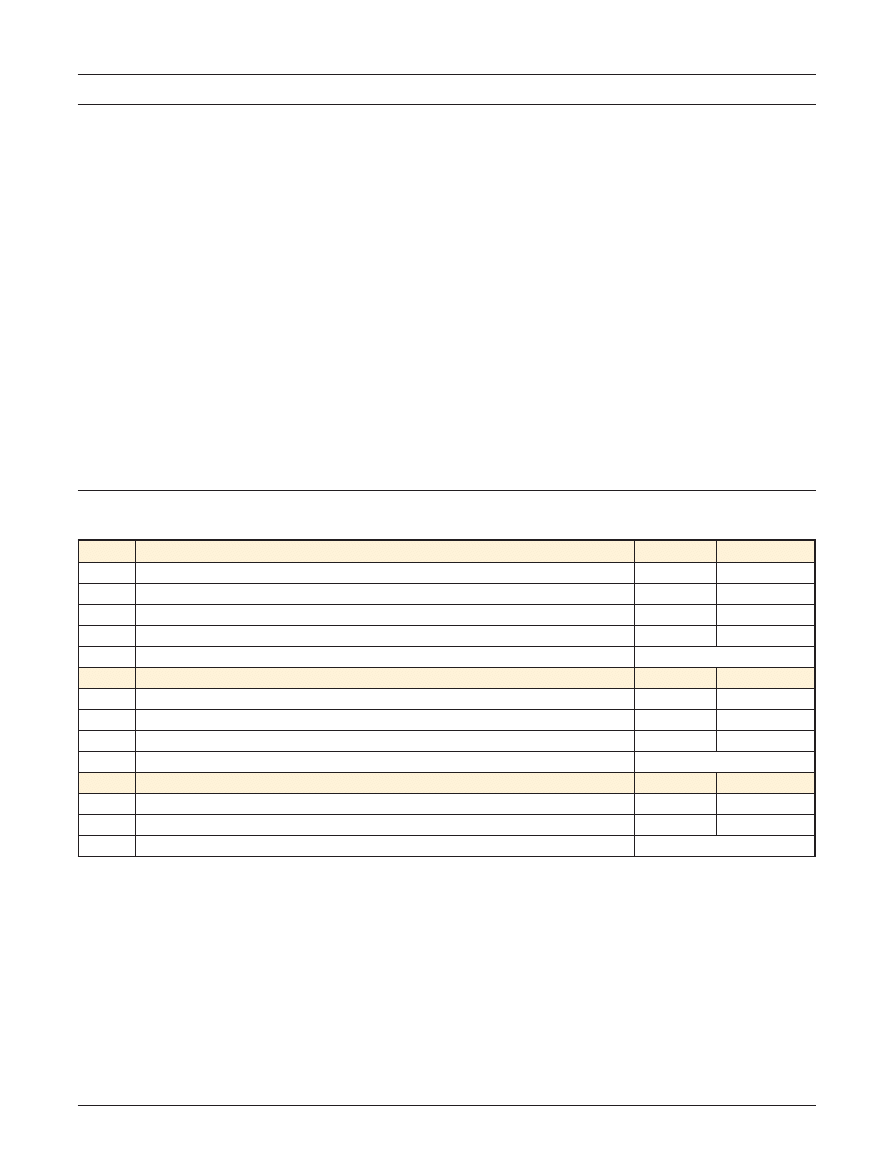
quantifying its severity. The SCP
comprises 3 sections, each assessing
a particular feature of the syndrome,
namely, the symmetry of spontane-
ous body posture (section A), the use
of nonaffected extremities (leg or
arm) to push by abduction and ex-
tension thrust (section B), and the
resistance to passive correction of
the tilted posture (section C). For
each item, the score ranges from 0 to
1. Because each feature is examined
in both sitting and standing posi-
tions, the maximum score in each
section is 2. Recently, the authors
completed and integrated instruc-
tions and task definitions for SCP ad-
ministration and scoring.
14
The SCP
is shown in the Appendix. We eval-
uated some psychometric character-
istics of the SCP, namely, interrater
reliability, internal consistency, and
diagnostic accuracy, in a sample of
26 people who had recently had a
stroke and who were selected on
the basis of the presence of postural
impairment.
15
We found that the
interobserver reliability of the SCP
was very high for both subscores
(intraclass correlation coefficients
⫽
.944, .929, and .939 for sections A, B,
and C, respectively) and total score
(intraclass correlation coefficient
⫽
.971). The scale also showed excel-
lent internal consistency (Cronbach
alpha
⫽.919).
With regard to the validity of the SCP
as a diagnostic tool for PB, we ad-
dressed the issue of the appropriate
cutoff scores for the scale. Cutoff
scores for the SCP have not been
definitively established, and contro-
versy currently exists regarding the
most appropriate way to interpret
SCP scores. On the basis of their clin-
ical experience, in their first article
on the topic, Karnath et al
10
sug-
gested a score of
ⱖ1 in each section
of the scale as the cutoff criterion for
making the diagnosis of PB. In their
study on the natural history of PB
after stroke, however, Danells et al
6
used a much less conservative crite-
rion and assigned a diagnosis of PB to
Validity of Scale for Contraversive Pushing
948
f
Physical Therapy
Volume 88
Number 8
August 2008
all people who had an SCP total
score of greater than 0, but they did
not assess the validity of this cutoff
score. We investigated the validity of
the original criteria of Karnath et al
10
by calculating the agreement be-
tween the clinical diagnosis, accord-
ing to the recommendations of Da-
vies,
1
and the SCP diagnosis. We
found that the criteria of Karnath
et al
10
led to many false-negative re-
sults when applied to a sample of
people with stroke and postural
impairment. Consequently, we pro-
posed the use of a different criterion,
that is, a score of
ⱖ0 in each section
of the SCP; this criterion improved
substantially the validity of the scale
as a diagnostic tool for PB in that
selected sample of people with
stroke.
15
This criterion, however, as
well as the other suggested cutoff
points for the SCP, needs to be tested
in an unselected, more heteroge-
neous, and larger sample of people
with hemiplegia, in whom the rate of
true-negative results (people without
a diagnosis of PB) could be expected
to be very high.
The construct validity of the SCP has
not been formally investigated yet.
Because PB is a distinctive disorder
of postural control in which the per-
ception of body orientation is se-
verely disturbed,
10,11
it may be ex-
pected that the disorder will impair
activities that require managing grav-
itational force when moving the
body to an upright posture and bal-
ancing. In the acute stage of recov-
ery from stroke, balance impairment
is a strong predictor of function in
terms of activities of daily living and
mobility,
16
and the severity of bal-
ance impairment correlates with the
severity of disability.
17
On the basis
of these findings, we believed that
the construct validity of the SCP
would be supported by a moderate
correlation between SCP scores and
balance,
mobility,
and
disability
scores.
The present study was primarily
aimed at investigating the validity of
the suggested cutoff scores for the
SCP and at evaluating the construct
validity of the scale. A further objec-
tive was to estimate the prevalence
of PB and its relationship to the side
of the lesion in people receiving neu-
rorehabilitation for stroke.
Method
Participants
All consecutive patients admitted for
stroke to 2 inpatient rehabilitation
hospitals
(Villa
Fiorita
Hospital,
Prato, Italy, and Piero Palagi Hospi-
tal, Florence, Italy) from January
2006 to December 2006 were in-
cluded in the study, provided that
they met the following 4 criteria:
first stroke; monolateral stroke, as in-
dicated by computed tomography
scans or magnetic resonance imag-
ing; recent stroke (
ⱕ30 days from
onset); and presence of at least min-
imal unilateral motor impairment at
upper or lower limbs or presence of
balance deficit (or presence of both),
as indicated by impaired perfor-
mance on the motricity and balance
sections of the Fugl-Meyer Assess-
ment Scale (FM).
18
The characteris-
tics of the selected study participants
are shown in Table 1. Participants
gave their written informed consent
for collection, storage, and use of
personal data.
Assessment
At admission to the rehabilitation
unit, each participant was assessed
by a staff physical therapist, who ad-
ministered the FM, the mobility sec-
tion of the motor assessment chart
developed by Lindmark and Hamrin
(LIND-MOB),
19
and the Barthel Index
(BI).
20
These tests are routinely ad-
ministered to all people admitted to
the Villa Fiorita and Piero Palagi hos-
pitals for stroke rehabilitation. The
FM is a 226-point multiple-item scale
that evaluates balance and motricity,
sensation, range of joint motion, and
pain in the paretic arms. All items are
scored on a 3-point (0 –2) ordinal
scale, in which 0 indicates no func-
tion. The excellent psychometric
characteristics of the FM are well es-
tablished.
21
The LIND-MOB evalu-
ates an individual’s abilities in rolling
to the affected and nonaffected
sides, sitting up from a lying-down
position and the reverse, leaning for-
ward from a seated position to touch
the feet, standing up, and walking.
Items are scored according to the
need for assistance in order to com-
plete the task on a 4-point (0 –3) or-
dinal scale, in which 0 indicates the
inability to perform the task. In a
sample of 21 people with acute
stroke, the LIND-MOB showed good
intrarater reliability (kappa values
ranging from .68 to .84) and inter-
rater reliability (kappa values ranging
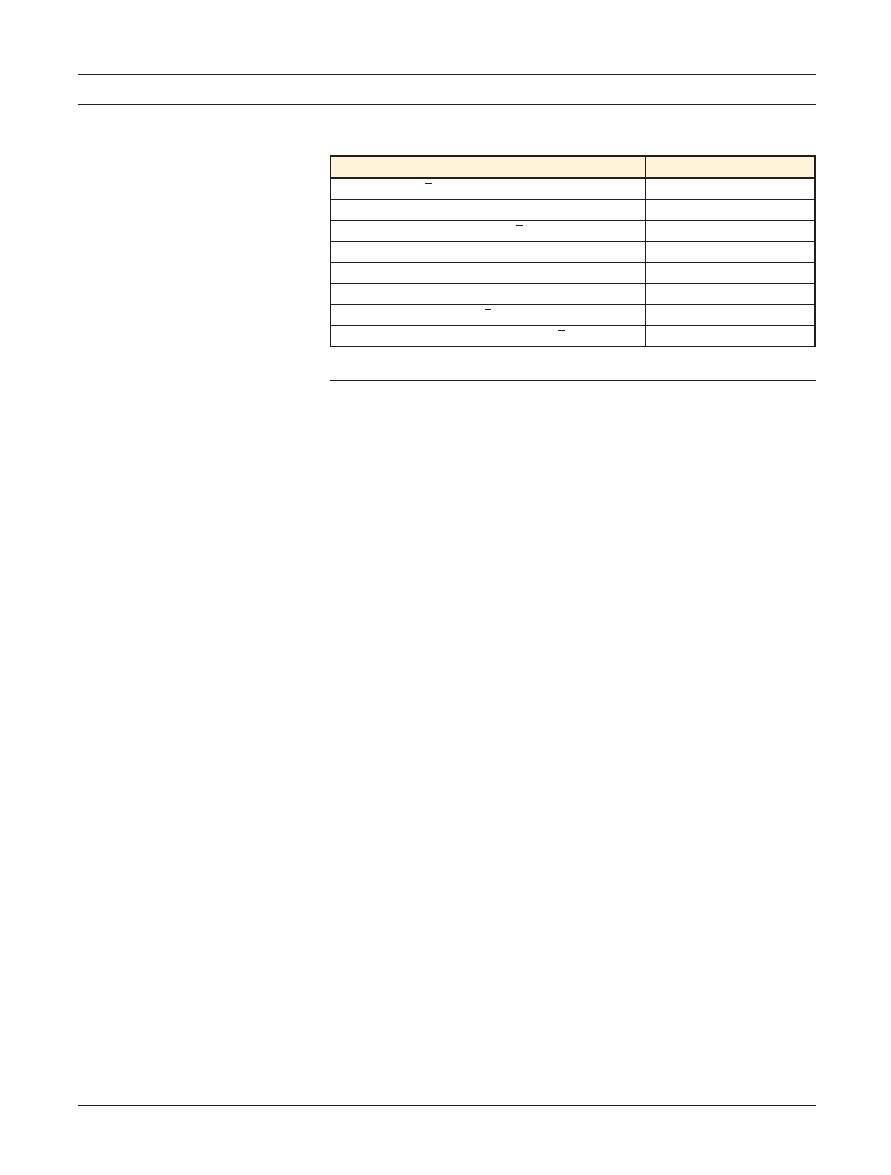
Table 1.
Characteristics of 105 Study Participants
Characteristic
Value
a
Age, y (X
⫾SD)
70.6
⫾11.2
Sex (M/F)
54/51
Time from stroke onset, d (X
⫾SD)
17.3
⫾6.2
Lesion side (R/L)
49/56
Neglect (yes/no)
13/92
Aphasia (yes/no)
38/67
Barthel Index score (X
⫾SD)
36.1
⫾24.2
Fugl-Meyer Assessment Scale score (X
⫾SD)
147.4
⫾48.9
a
Reported as number of participants, unless otherwise indicated.
Validity of Scale for Contraversive Pushing
August 2008
Volume 88
Number 8
Physical Therapy
f
949
from .68 to .76).
22
The BI, a 10-item
performance-based scale that evalu-
ates independence in basic activities
of daily living, has been shown to
have excellent reliability and validi-
ty.
23
Because the presence and the
severity of PB are expected to inter-
fere with balance, mobility, and
functional level, these evaluations
were used to estimate the construct
validity of the SCP.
Four examiners assessed the pres-
ence and severity of PB within 3 days
of admission. One examiner was a
geriatrician
with
experience
in
stroke
rehabilitation.
The
others
were physical therapists with many
years of experience with people
who have had a stroke. At each re-
habilitation unit, people were inde-
pendently evaluated by 2 examiners
within a few hours of each other.
One of the examiners (MP and CB at
Villa Fiorita and Piero Palagi hospi-
tals, respectively) selected partici-
pants and made the clinical diagnosis
of PB according to the recommenda-
tions of Davies.
1
The clinical exami-
nation in the 2 hospitals was based
on the same criteria and focused on
careful observation of people while
lying down, sitting, standing, weight
transferring, and walking. The exam-
iners
watched
for
characteristic
signs of the behavior, such as whole-
body incorrect alignment manifested
as typical lengthening or shortening
of the affected or unaffected side of
the trunk and active extension in the
unaffected extremities with resis-
tance to be moved toward the unaf-
fected side. However, the examiners
also watched for other signs, such as
difficulty in placing the unaffected
leg in the supine position, flexion of
the paretic leg while weight transfer-
ring toward the contralateral side
during standing, and adduction of
the paretic leg in the swing phase of
gait. People were diagnosed as hav-
ing PB when at least 2 of the above-
mentioned signs were present, with
one of them judged as severe.
The second examiner (LN or MB)
administered the SCP and diagnosed
the participant as having PB or not
having PB on the basis of 3 cutoff
criteria—a total SCP score of greater
than 0 (ie, the criterion used by
Danells et al,
6
defined as Crit_1); a
score of greater than 0 in each SCP
section, leading to a total SCP score
of
ⱖ1.75 (ie, the criterion suggested
by Baccini et al,
15
defined as Crit_2);
and a score of
ⱖ1 in each SCP sec-
tion, leading to a total SCP score of
ⱖ3 (ie, the original criterion sug-
gested by Karnath et al,
10
defined as
Crit_3). The second examiner was
unaware of all earlier assessments as
well as the clinical diagnosis of PB.
Data Analysis
The agreement between the SCP di-
agnosis resulting from the 3 different
cutoff criteria and the clinical diag-
nosis was estimated by calculation of
the Cohen kappa coefficient (
).
From SCP scores and clinical evalua-
tions, sensitivity, specificity, predic-
tive value of a positive test, predic-
tive value of a negative test, positive
and negative likelihood ratios, and
global diagnostic accuracy of the
scale were calculated for each crite-
rion, along with 95% confidence
intervals. The construct validity of
the SCP was estimated by calculation
of the Spearman rank correlation co-
efficients for the SCP total score and
subscores and the balance subscore
of the FM (FM-BAL), the LIND-MOB
subscore, and the BI score.
Comparisons of the prevalence of a
clinical diagnosis of PB in people
with right- and left-brain lesions and
in people with stroke who were re-
ferred to the 2 rehabilitation units
were carried out with the chi-square
test.
The level of statistical significance
was set at .05. Data analyses were
performed with the statistical pack-
age SPSS Version 12.0 for Windows.*
Validity indexes and 95% confidence
intervals were calculated with Mi-
crosoft Excel 2003.
†
Results
Validity of Different
Cutoff Criteria
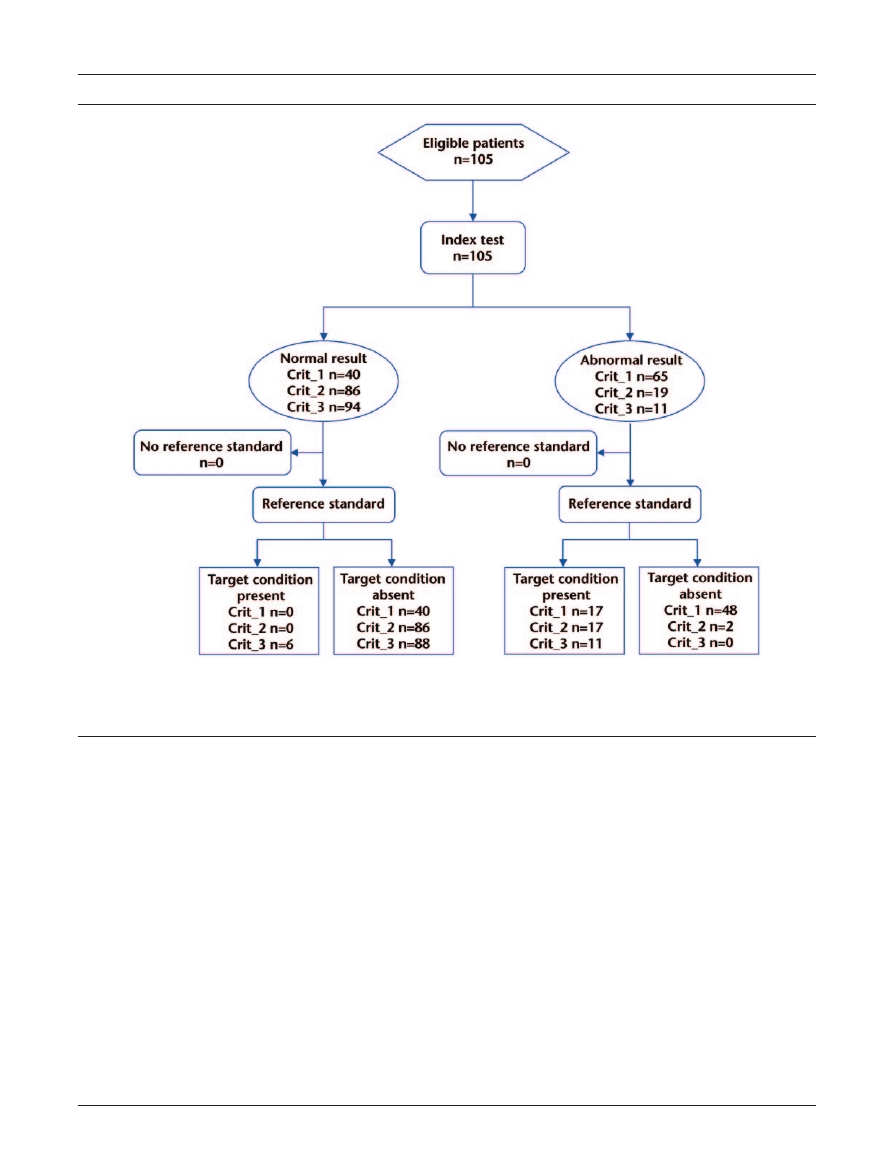
The Figure shows the flow diagram
for the study. In the population stud-
ied, 17 of 105 participants (16.2%)
were diagnosed as having PB on the
basis of the clinical examination. The
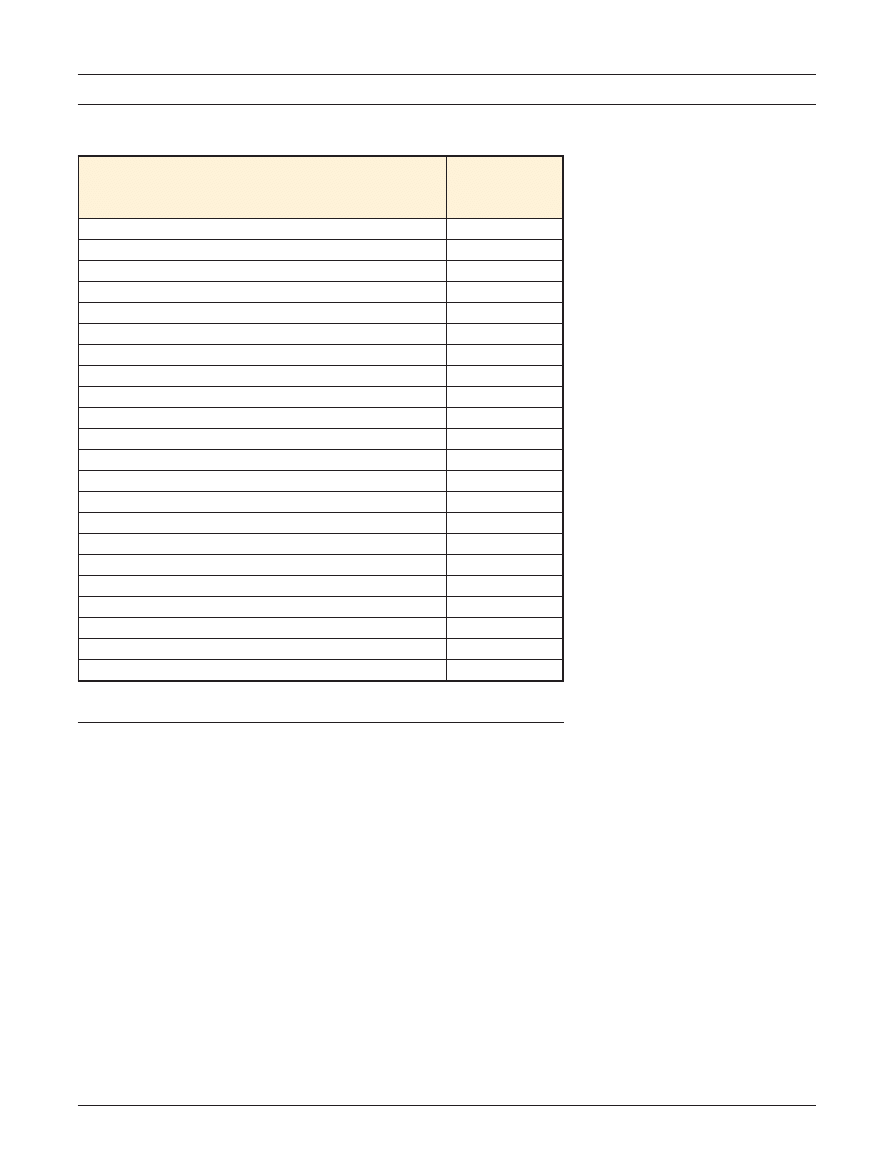
core features of PB in these partici-
pants are summarized in Table 2. On
the basis of the SCP scores, however,
a diagnosis of PB was made for 65,
19, and 11 participants when Crit_1,
Crit_2, and Crit_3, respectively, were
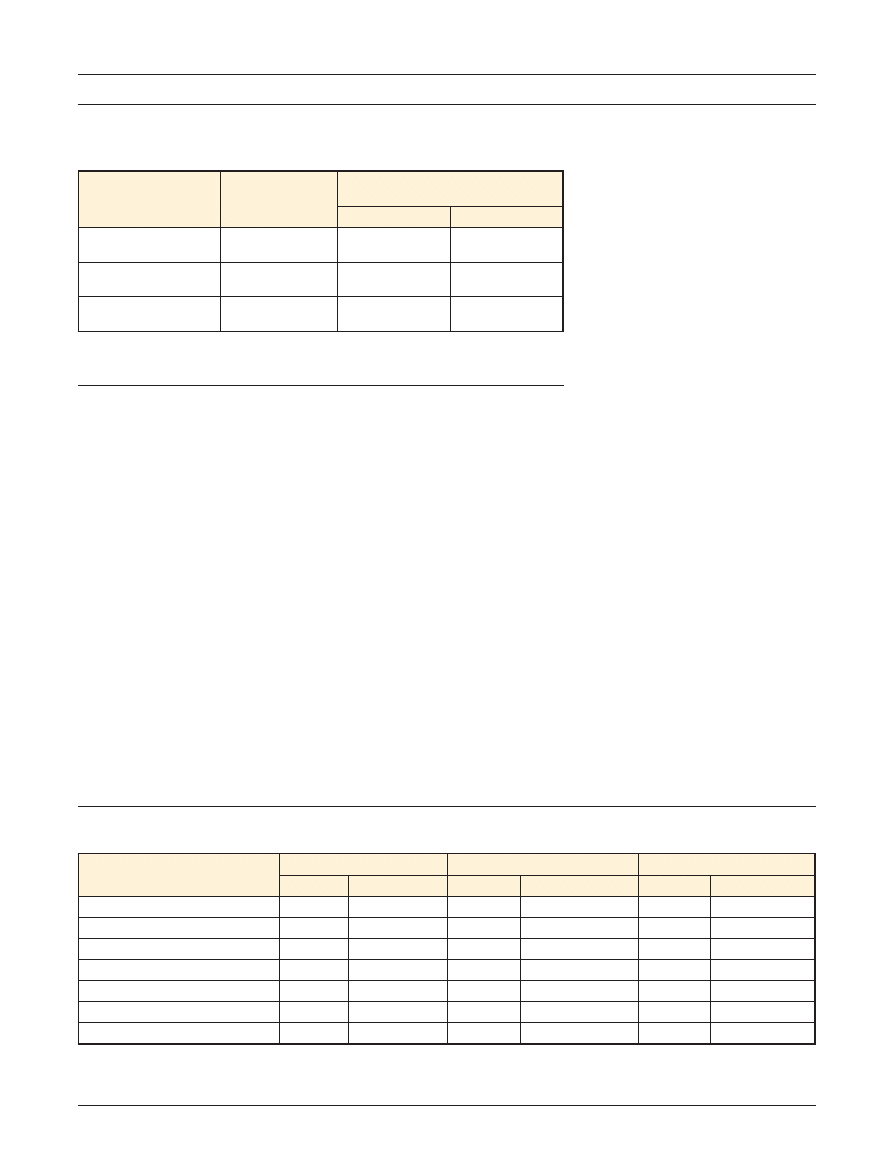
used. Consequently, when different
cutoff criteria were used, the clin-
ical and SCP diagnoses differed
(Tab. 3), as did the validity indexes
of the scale (Tab. 4). When Crit_1
was used, the diagnostic agreement
between the SCP and the clinical ex-
amination was poor: agreement was
found for only 54.3% of participants
(57/105; Cohen
⫽.212, SE⫽.052).
Forty were diagnosed as not having
PB and 17 were diagnosed as having
PB by both methods. With this cutoff
criterion, 48 participants were incor-
rectly diagnosed by the SCP as hav-
ing PB. Consequently, despite per-
fect sensitivity, the scale had very
low specificity, and the predictive
value of a positive test was very low
as well.
Both Crit_2 and Crit_3 led to much
better agreement between SCP and
clinical diagnoses. The best SCP di-
agnostic accuracy was found with
Crit_2, which correctly diagnosed
98.1% of participants (103/105; Co-
hen
⫽.933, SE⫽.047). With this cri-
terion, the specificity of the scale
was greatly enhanced, without any
decrease in sensitivity or the predic-
* SPSS Inc, 233 S Wacker Dr, Chicago, IL
60606.
†
Microsoft Corp, One Microsoft Way, Red-
mond, WA 98052-6399.
Validity of Scale for Contraversive Pushing
950
f
Physical Therapy
Volume 88
Number 8
August 2008
tive value of a negative test. How-
ever, Crit_2 led to false-positive re-
sults in 2 participants. Crit_3 led to
correct diagnoses in 94.3% of partic-
ipants
(99/105;
Cohen
⫽.754,
SE
⫽.094). No false-positive results
were obtained with the scale when
this more conservative criterion was
used, but 6 participants were classi-
fied as not having PB, contrary to the
clinical diagnosis. Therefore, when
Crit_3 was used, the scale was highly
specific, but its sensitivity was rela-
tively low.
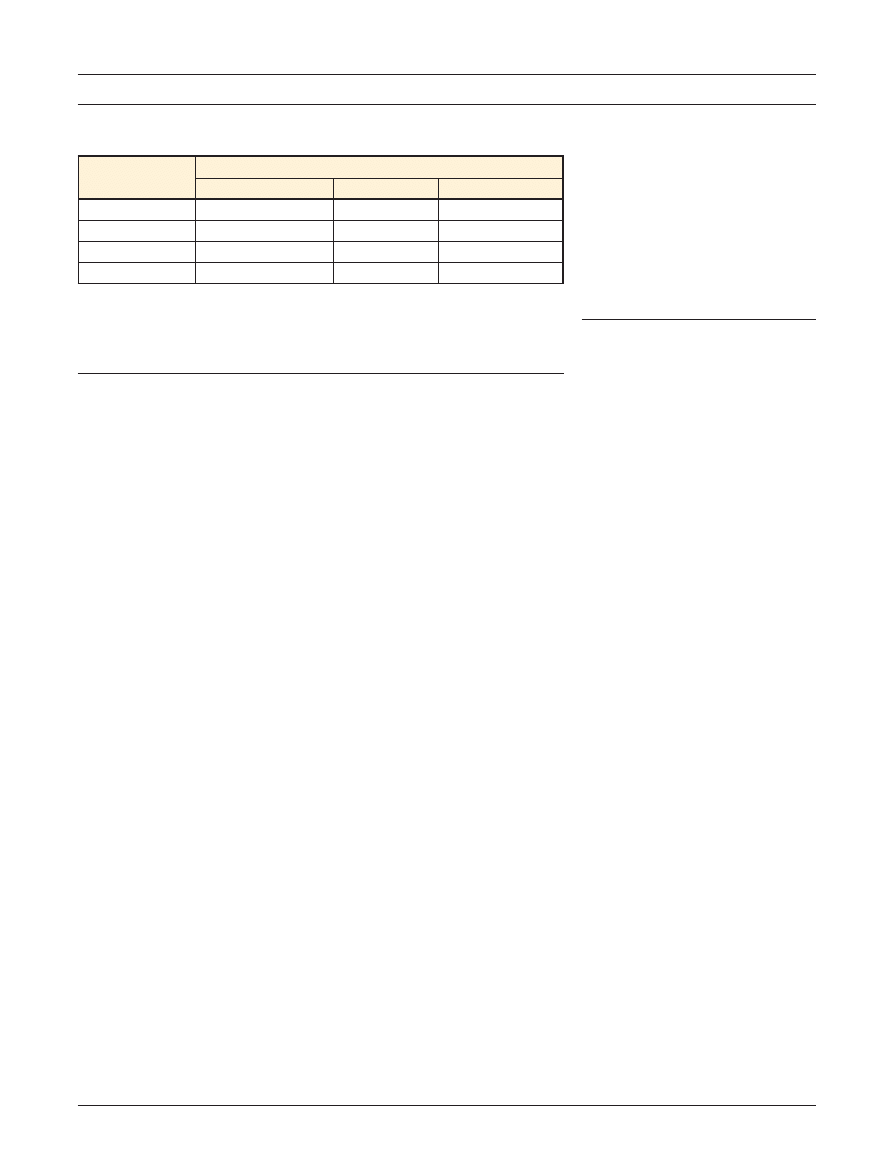
SCP Construct Validity
Table 5 shows the Spearman rank
correlation
coefficients
for
SCP
scores and functional (BI), mobility
(LIND-MOB), and balance (FM-BAL)
examinations. For the SCP total
score, the correlations were moder-
ate to high, and all were significant at
the .001 level. The values are nega-
tive because, for the SCP, lower
values
indicate
better
function,
whereas for the other instruments,
the opposite is true. Section A scores
showed distinctly higher correla-
tions with the other measures than
section B and C scores.
Prevalence of PB in Right- and
Left-Brain Lesions
According to the clinical examina-
tion, the overall prevalence of PB in
the population studied was 16.2%.
Prevalence did not differ signifi-
cantly between the 2 rehabilitation
units (16.1% and 16.3% at Villa
Fiorita Hospital and at Piero Palagi
Hospital, respectively; P
⫽.972). With
regard to the side of the lesion, no
significant differences were found
between participants with right- and
left-brain lesions (18.4% and 14.3%,
respectively; P
⫽.571).
Discussion
The main purpose of the present
study was to determine the validity
of 3 cutoff criteria suggested for us-
ing the SCP as a diagnostic tool for
PB. The results confirmed that the
Figure.
Flow diagram for the study of the validity of different cutoff scores for the Scale for Contraversive Pushing (SCP). Crit_1
⫽cutoff
criterion 1 (ie, total SCP score of
⬎0), Crit_2⫽cutoff criterion 2 (ie, score of ⬎0 in each of the 3 sections of the SCP), Crit_3⫽cutoff
criterion 3 (ie, score of
ⱖ1 in each of the 3 sections of the SCP), index test⫽SCP, reference standard⫽clinical examination method.
Validity of Scale for Contraversive Pushing
August 2008
Volume 88
Number 8
Physical Therapy
f
951
cutoff score used by Danells et al,
6
which assigned a diagnosis of PB to
all people with an SCP score of
greater than 0, is absolutely inade-
quate, leading to a large number of
false-positive diagnoses. This result is
not surprising, because most people
who have had a stroke show an
asymmetric
posture,
with
less
weight bearing by the affected leg
than by the unaffected leg.
24,25
A lat-
eral tilting in itself, however, does
not indicate the presence of clear
PB. As indicated in our earlier arti-
cle,
15
the presence of all of the typ-
ical features of the syndrome seems
to be necessary for correctly diagnos-
ing PB in people after stroke. The
findings in the present study strongly
support this assumption.
The results also indicated that the
criterion we suggested in previous
research
15
seems to be the most suit-
able for making a correct diagnosis,
even when applied in an unselected,
more representative sample of peo-
ple with hemiplegia. However, al-
though correctly classifying 98.1% of
people, this cutoff score misdiag-
nosed 2 participants as having PB.
Therefore, when this criterion is
used, the presence of a minimal
number of false-positive diagnoses
cannot be excluded. Conversely,
when the original cutoff score sug-
gested by Karnath et al
10
was used,
no false-positive diagnoses emerged.
This more conservative criterion
proved to be less accurate than the
former because it failed to detect the
presence of the behavior in 6 of 17
people (35%). However, in this
larger and heterogeneous sample of
people with stroke, it was signifi-
cantly more suitable than we found
it to be in our previous research.
15
This result also was expected be-
cause in the general population of
people with stroke and receiving re-
habilitation, the rate of true-negative
results is expected to be much
higher than that in a sample of peo-
ple with stroke and selected for the
presence of postural disorders.
On the basis of these findings, we
suggest that SCP cutoff criteria be
selected according to the aim of the
evaluation. For epidemiological pur-
poses, we believe that the cutoff cri-
terion that proved to be the most
accurate, that is, a score of greater
than 0 in each section of the scale
(Crit_2), is the most suitable. This
criterion may be useful for studies
aimed at investigating the preva-
lence of the syndrome or its associa-
tion with other features, such as the
side of a cerebral lesion or the pres-
ence of neglect. There is consider-
able disagreement among research-
ers about these topics,
2,4 – 6
and it
may be argued that conflicting find-
ings may be partially attributable to
different criteria for diagnosing PB.
On the other hand, in research about
the pathophysiology of PB, a correct
diagnosis is a prerequisite to drawing
correct inferences. For example,
there is much debate about a hypo-
thetical bias in the perceived pos-
tural or visual vertical and whether
the bias is contralesional or ipsile-
sional.
10,11,24,25
We suggest that, in
studies aimed at investigating these
issues, the use of both Crit_2 and
Crit_3 for diagnosing the syndrome
would be advisable. The more con-
Table 2.
Features of Pusher Behavior in 17 Participants With a Positive Clinical Diagnosis
Feature
a
No. of
Participants
Showing the
Feature
Unaffected arm overactivity
3
Head rotation/lateral flexion toward US
7
Supine
Faulty alignment
5
Impaired placement of the unaffected leg
5
Sitting
b
Faulty alignment
11
Weight bearing on AS; unaffected hand leans against the bed
8
Resistance; trunk US shortening during weight transfer toward US
14
Pushing during bed-chair transfer toward US
15
Standing
b
Pushing and trunk US shortening during sit-to-stand movement
16
Faulty alignment
17
Unaffected upper-limb pushing
12
Unaffected lower-limb pushing
17
Resistance; trunk US shortening during weight transfer toward US
17
Affected leg flexion during weight transfer toward US
7
Walking
b
Faulty alignment
13
Resistance; trunk US shortening during weight transfer toward US
13
Hip adduction (swing phase)
5
Early sitting when approaching a chair
9
a
US
⫽unaffected side, AS⫽affected side.
b
Aids, support, or both allowed when necessary.
Validity of Scale for Contraversive Pushing
952
f
Physical Therapy
Volume 88
Number 8
August 2008
servative Crit_3 should be used for
selecting people who definitely ex-
hibit PB, whereas Crit_2 should be
used to include people without PB.
In this way, people with an uncer-
tain diagnosis would be excluded,
and the risk of an incorrect alloca-
tion of people to the PB group or the
non-PB group would be minimized.
The preceding discussion is based on
the assumption that the clinical diag-
noses were correct. A limitation of
the present study was that we did
not formally assess the reliability of
the method used to make the clinical
diagnoses. Therefore, possible bias
related to slightly different criteria
used in the clinical examinations
cannot be excluded.
Our findings also provide evidence
regarding SCP construct validity, be-
cause SCP scores correlated signifi-
cantly with functional, mobility, and
balance evaluations. Not surpris-
ingly, the strongest correlation was
found with balance scores, because
balance is directly affected by PB.
People with PB, in fact, use their
nonaffected extremities to push to-
ward the contralateral side and
eventually fall.
9
Differences in the
strength of the correlations found
for the 3 sections of the SCP most
likely reflected the particular as-
pects of the disorder being investi-
gated. As mentioned above, active
pushing and resistance to passive
correction of posture (assessed in
sections B and C) are distinguishing
features of PB,
9
whereas laterally
tilted posture and falling (assessed in
section A) are not.
15
Indeed, symme-
try of posture and ability to sit and
stand upright were impaired in a sig-
nificant proportion of people with-
out PB. These people performed
poorly in the balance, mobility, and
functional tests but usually scored 0
in sections B and C of the SCP. Over-
all, it may be speculated that PB in-
fluences performance insofar as it af-
fects the ability to balance. However,
a direct effect of active pushing on
performance, such as the ability to
roll and rise from a lying-down posi-
tion or to transfer, may be present as
well.
Recently, a modified form of the SCP
was published and validated.
26
In a
small sample of people with hemi-
plegia (N
⫽19), the authors found
low to moderate correlations be-
tween the revised SCP scores and
balance and functional scores at
both admission (r
⫽.52 and r⫽.43,
respectively) and discharge (r
⫽.49
and r
⫽.45, respectively). These val-
ues are distinctly lower than the
values that we found for the original
scale. Indeed, the modified version
of the SCP is different enough from
the original scale to be rather a com-
pletely new assessment tool. Our
results indicate that the original ver-
Table 3.
Clinical Diagnosis and Scale for Contraversive Pushing (SCP) Diagnosis Made With 3
Different Cutoff Criteria
a
for 105 Participants
SCP Criterion
Diagnosis
No. of Participants With the
Following Clinical Diagnosis:
Negative
Positive
Crit_1
Negative
Positive
40
48
0
17
Crit_2
Negative
Positive
86
2
0
17
Crit_3
Negative
Positive
88
0
6
11
a
Crit_1
⫽cutoff criterion 1 (ie, total SCP score of ⬎0), Crit_2⫽cutoff criterion 2 (ie, score of ⬎0 in each
of the 3 sections of the SCP), Crit_3
⫽cutoff criterion 3 (ie, score of ⱖ1 in each of the 3 sections of the
SCP).
Table 4.
Validity Indexes of the Scale for Contraversive Pushing (SCP) With 3 Different Cutoff Criteria
a
for 105 Participants
Parameter
Crit_1
Crit_2
Crit_3
Value
95% CI
Value
95% CI
Value
95% CI
Sensitivity
1.000
0.805–1.000
1.000
0.805–1.000
0.647
0.383–0.856
Specificity
0.455
0.348–0.564
0.977
0.920–0.997
1.000
0.959–1.000
Predictive value of a positive test
0.262
0.160–0.385
0.895
0.669–0.987
1.000
0.715–1.000
Predictive value of a negative test
1.000
0.912–1.000
1.000
0.958–1.000
0.936
0.866–0.976
Positive likelihood ratio
1.833
1.515–2.219
44.053
11.180–173.171
Infinity
NaN–Infinity
Negative likelihood ratio
0.000
0.000–NaN
0.000
0.000–NaN
0.353
0.185–0.672
Accuracy
0.543
0.443–0.640
0.981
0.933–0.998
0.943
0.880–0.979
a
Crit_1
⫽cutoff criterion 1 (ie, total SCP score of ⬎0), Crit_2⫽cutoff criterion 2 (ie, score of ⬎0 in each of the 3 sections of the SCP), Crit_3⫽cutoff
criterion 3 (ie, score of
ⱖ1 in each of the 3 sections of the SCP). CI⫽confidence interval, NaN⫽not a number (ie, the calculation cannot be performed
because the values entered include one or more instances of zero).
Validity of Scale for Contraversive Pushing
August 2008
Volume 88
Number 8
Physical Therapy
f
953
sion of the SCP seems to be pref-
erable because it correlates better
with functional and postural abili-
ties. Moreover, the cutoff score
for diagnosing PB with the modi-
fied scale has not been empirically
investigated.
The validity of the SCP also seems to
be slightly higher than the validity of
a lateropulsion scale (LS) developed
by D’Aquila et al.
8
In a convenience
sample of 85 people with stroke
evaluated at admission to a rehabili-
tation unit, the authors reported
r
⫽.57 for LS and FM-BAL scores
and r
⫽.56 for LS and mobility
(Functional Independence Measure)
scores. Overall, the 13 motor or mo-
bility items of the Functional Inde-
pendence Measure that assess self-
care, sphincter control, transfer, and
locomotion are quite similar to the
items of the BI. Both of these values
are lower than the values found in
the present study. In addition to re-
liability and validity, however, evalu-
ation instruments should demon-
strate good responsiveness, that is,
the ability to detect changes over
time.
27,28
Further research should be
aimed at comparing the SCP and the
LS with regard to this important psy-
chometric feature.
Finally, the similar prevalences of PB
found in people with right- and left-
brain lesions are consistent with
other findings. The mean interval
from stroke onset in the sample stud-
ied was 13.7 (SD
⫽6.2) days, and
other research has shown that in this
subacute phase, the syndrome af-
fects people with right hemiplegia
and left hemiplegia equally.
2,5
The
clinical impression that PB is more
frequently exhibited by people with
right-brain injury is most likely attrib-
utable to the fact that the behavior
may persist longer in people with
right-brain lesions than in those with
left-brain lesions. When assessed sev-
eral weeks from stroke onset, in fact,
PB was found to be significantly
more frequent in people with left
hemiparesis.
5
Conclusion
The data presented here indicate
that the SCP cutoff score suggested
in our previous study
15
is superior to
other criteria for correctly classifying
nearly all people with stroke as hav-
ing PB or not having PB. However,
the use of the more conservative
original criterion of Karnath et al
10
is
advisable when the absolute cer-
tainty of no false-positive diagnoses
is requested. The construct validity
of the SCP seems to be slightly
higher than that of other published
scales for PB. The sensitivity to
change of the SCP and of the other
scales still needs to be addressed.
Mr Baccini, Mr Paci, and Mr Rinaldi provided
concept/idea/research design. Mr Baccini
provided writing and data analysis. Mr Bac-
cini, Mr Paci, Dr Nannetti, and Ms Biricolti
provided data collection. Mr Baccini and Mr
Rinaldi provided project management. Mr
Rinaldi provided facilities/equipment. All au-
thors provided consultation (including re-
view of manuscript before submission).
This article was received June 21, 2007, and
was accepted April 17, 2008.
DOI: 10.2522/ptj.20070179
References
1 Davies PM. Steps to Follow: A Guide to the
Treatment of Adult Hemiplegia
. Heidel-
berg, Germany: Springer; 1985.
2 Pedersen PM, Wandel A, Jorgensen HS,
et al. Ipsilateral pushing in stroke: inci-
dence, relation to neuropsychological
symptoms, and impact on rehabilitation.
The Copenhagen Stroke Study. Arch Phys
Med Rehabil.
1996;77:25–28.
3 Bohannon RW, Cook AC, Larkin PA, et al.
The listing phenomenon of hemiplegic pa-
tients. Neurol Rep. 1986;10:43– 44.
4 Premoselli S, Cesana L, Cerri C. Pusher
syndrome in stroke: clinical, neuropsycho-
logical and neurophysiological investiga-
tion. Eura Medicophys. 2001;37:143–151.
5 Lafosse C, Kerckhofs E, Troch M, et al.
Contraversive pushing and inattention of
the contralesional hemispace. J Clin Exp
Neuropsychol.
2005;27:460 – 484.
6 Danells CJ, Black SE, Gladstone DJ, et al.
Poststroke pushing: natural history and re-
lationship to motor and functional recov-
ery. Stroke. 2004;35:2873–2878.
7 Brunnstro
¨m S. Movement Therapy in
Hemiplegia: A Neurophysiological Ap-
proach
. New York, NY: Harper & Row;
1970.
8 D’Aquila MA, Smith T, Organ D, et al. Val-
idation of a lateropulsion scale for patients
recovering from stroke. Clin Rehabil.
2004;18:102–109.
9 Karnath HO. Pusher syndrome: a frequent
but little-known disturbance of body ori-
entation perception. J Neurol. 2007;25
4:415– 424.
10 Karnath HO, Ferber S, Dichgans J. The
origin of contraversive pushing: evidence
for a second graviceptive system in hu-
mans. Neurology. 2000;55:1298 –1304.
11 Perennou DA, Amblard B, Laassel EM,
et al. Understanding the pusher behavior
of some stroke patients with spatial defi-
cit: a pilot study. Arch Phys Med Rehabil.
2002;83:570 –575.
12 Pe
´rrennou DA, Amblard B, Leblond C,
et al. Biased postural vertical in humans
with hemispheric cerebral lesions. Neuro-
sci Lett.
1998;252:75–78.
13 Pe
´rennou D. Towards a better understand-
ing and quantitative assessment of push-
ing, a postural behaviour caused by some
strokes. Ann Readapt Med Phys. 2005;
48:198 –206.
Table 5.
Spearman Rank Correlation Coefficients
a
Score
Correlation Coefficient for:
Barthel Index
FM-BAL
LIND-MOB
SCP_A
⫺.620
b
⫺.704
b
⫺.632
b
SCP_B
⫺.447
b
⫺.463
b
⫺.429
b
SCP_C
⫺.416
b
⫺.370
b
⫺.345
c
SCP_TOT
⫺.632
b
⫺.666
b
⫺.595
b
a
FM-BAL
⫽balance subscore of the Fugl-Meyer Assessment Scale, LIND-MOB⫽subscore of the mobility
section of the motor assessment chart developed by Lindmark and Hamrin,
19
SCP_A
⫽section A
subscore of the Scale for Contraversive Pushing (SCP), SCP_B
⫽section B subscore of the SCP,
SCP_C
⫽section C subscore of the SCP, SCP_TOT⫽total score of the SCP.
b
P
⬍.001.
c
P
⬍.005.
Validity of Scale for Contraversive Pushing
954
f
Physical Therapy
Volume 88
Number 8
August 2008
14 Karnath HO, Bro
¨tz D. Letter to the Editor:
Instructions for the Clinical Scale for Con-
traversive Pushing (SCP). Neurorehabil
Neural Repair.
2007;4:370 –371.
15 Baccini M, Paci M, Rinaldi LA. The Scale
for Contraversive Pushing: a reliability and
validity study. Neurorehabil Neural Re-
pair.
2006;20:468 – 472.
16 Tyson SF, Hanley M, Chillala J, et al. The
relationship between balance, disability, and
recovery after stroke: predictive validity of
the Brunel Balance Assessment. Neuroreha-
bil Neural Repair.
2007;21:341–346.
17 Tyson SF, Hanley M, Chillala J, et al. Bal-
ance disability after stroke. Phys Ther.
2006;86:30 –38.
18 Fugl-Meyer AR, Jaasko L, Leyman I, et al. The
post-stroke hemiplegic patient, I: a method
for evaluation of physical performance.
Scand J Rehabil Med.
1975;7:13–31.
19 Lindmark B, Hamrin E. Evaluation of func-
tional capacity after stroke as a basis for
active intervention: presentation of a mod-
ified chart for motor capacity assessment
and its reliability. Scand J Rehabil Med.
1988;20:103–109.
20 Mahoney FI, Barthel DW. Functional eval-
uation: the Barthel Index. Md State Med J.
1965;14:61– 65.
21 Salter K, Jutai JW, Teasell R, et al. Issues
for selection of outcome measures in
stroke rehabilitation: ICF body functions.
Disabil Rehabil.
2005;27:191–207.
22 Kierkegaard M, Tollback A. Inter- and
intra-rater reliability of the B. Lindmark
Motor Assessment. Advances in Physio-
therapy.
2005;7:2– 6.
23 Barak S, Duncan PW. Issues in selecting
outcome measures to assess functional
recovery after stroke. NeuroRx. 2006;3:
505–524.
24 Saj A, Honore
´ J, Coello Y, et al. The visual
vertical in the pusher syndrome: influence
of hemispace and body position. J Neurol.
2005;252:885– 891.
25 Johannsen L, Fruhmann Berger M, Karnath
HO. Subjective visual vertical (SVV) deter-
mined in a representative sample of 15
patients with pusher syndrome. J Neurol.
2006;253:1367–1369.
26 Lagerqvist J, Skargren E. Pusher syndrome:
reliability,
validity
and
sensitivity
to
change of a classification instrument. Ad-
vances in Physiotherapy.
2006;8:154 –
160.
27 Fitzpatrick R, Ziebland S, Jenkinson C,
et al. Importance of sensitivity to change
as a criterion for selecting health status
measures. Qual Health Care. 1992;1:
89 –93.
28 Binkley JM, Stratford PW, Lott SA, Riddle
DL; North American Orthopaedic Rehabil-
itation Research Network. The Lower Ex-
tremity Functional Scale (LEFS): scale de-
velopment, measurement properties, and
clinical application. Phys Ther. 1999;79:
371–383.
Appendix.
Scale for Contraversive Pushing (SCP)
10,14,
a
A
Posture (symmetry of spontaneous posture)
Sitting
Standing
Score 1
⫽severe contraversive tilt with falling to the contralesional side
Score 0.75
⫽severe contraversive tilt without falling
Score 0.25
⫽mild contraversive tilt without falling
Score 0
⫽no tilt/upright body orientation
Total (maximum
⫽2)
B
Extension (use of the arm/leg to extend the area of physical contact to the ground)
Score 1
⫽performed already in rest
Score 0.5
⫽performed only until position is changed
b
Score 0
⫽no extension
Total (maximum
⫽2)
C
Resistance (resistance to passive correction of posture to an upright position)
c
Score 1
⫽resistance is shown
Score 0
⫽resistance is not shown
Total (maximum
⫽2)
a
Reprinted with permission of Lippincott Williams & Wilkins from: Karnath HO, Ferber S, Dichgans J. The origin of contraversive pushing: evidence for a
second graviceptive system in humans. Neurology. 2000;55:1298 –1304.
b
For sitting, ask the patient to glide the buttocks on the mattress toward the nonparetic side, to transfer from bed to wheelchair toward the nonparetic
side, or both. For standing, ask the patient to start walking. If pushing already occurs when the patient is rising from the sitting position, section B is given
the value of 1 for standing.
c
Touch the patient at the sternum and the back. Give the following instructions: “I will move your body sideward. Please permit this movement.”
Validity of Scale for Contraversive Pushing
August 2008
Volume 88
Number 8
Physical Therapy
f
955

doi: 10.2522/ptj.20070179
Originally published online July 10, 2008
2008; 88:947-955.
PHYS THER.
Biricolti and Lucio A Rinaldi
Marco Baccini, Matteo Paci, Luca Nannetti, Claudia
Validity
Diagnosing ''Pusher Behavior'' and Construct
Scale for Contraversive Pushing: Cutoff Scores for
References
http://ptjournal.apta.org/content/88/8/947#BIBL
for free at:
This article cites 26 articles, 8 of which you can access
Cited by
http://ptjournal.apta.org/content/88/8/947#otherarticles
This article has been cited by 2 HighWire-hosted articles:
Information
Subscription
http://ptjournal.apta.org/subscriptions/
Permissions and Reprints
http://ptjournal.apta.org/site/misc/terms.xhtml
Information for Authors
http://ptjournal.apta.org/site/misc/ifora.xhtml
Wyszukiwarka
Podobne podstrony:
2793 artykul 7 id 31748 Nieznany
2892 artykul 1 id 32057 Nieznany
artykul (1) id 69658 Nieznany
artykul 5 id 69654 Nieznany (2)
finanse artykuly id 172227 Nieznany
m2 artykul 1 id 275067 Nieznany
artykul 2 id 69662 Nieznany (2)
artykul 4 id 69537 Nieznany
artykul1 id 69679 Nieznany (2)
artykul 3 id 69652 Nieznany (2)
neurologia artykul 2 id 317511 Nieznany
Artykul 5 id 69561 Nieznany (2)
Bunkier Krysia Artykul id 9530 Nieznany (2)
ZKI artykul id 590848 Nieznany
artykul 4 id 69653 Nieznany (2)
2793 artykul 7 id 31748 Nieznany
2892 artykul 1 id 32057 Nieznany
artykul (1) id 69658 Nieznany
artykul profilaktyka cz2 id 695 Nieznany (2)
więcej podobnych podstron