885
demonstrated minimal posterior changes
without sequestrum-like formation;
group II hips demonstrated a central se-
questrum-like change but maintenance
of epiphyseal height; group III hips
showed preservation of the posterior
head only; group IV hips demonstrated
total head involvement.
Control subjects for all coagulation as-
says included 169 otherwise healthy chil-
dren aged 1 through 16 years (inclusive)
who were admitted for elective same-day
surgery at Children’s Hospital Medical
Center. The appropriate informed con-
sent was obtained for all the subjects.
This study was approved by the Review
Board on Investigations Involving
Human Beings of the Children’s Hospi-
tal Medical Center. Levels of protein C,
protein S, antithrombin III, plasminogen
activator inhibitor, plasminogen, and
lipoprotein (a) were determined as pre-
viously described.
3
The anticoagulant re-
sponse to APC was performed with a
modification of the commercial method
using the Coatest for APC Resistance
(Chromogenix AB, Mölndal, Sweden).
8
The assay used a predilution of one vol-
ume sample plasma with four volumes
factor V-deficient plasma (V-DEF Plas-
ma, Chromogenix AB, Mölndal, Swe-
den.) For the determination of the factor
V Leiden mutation, genomic DNA was
prepared on the propositus, parents, and
family members. A 224-base pair frag-
ment of the factor V gene was amplified
and then digested with Mnl-1 restriction
The cause of Legg-Perthes disease, a dis-
order of the hip in children resulting
from avascular necrosis of the femoral
head, is unclear. Circulatory impairment
of the affected bone has been postulated
to be the common denominator.
1
Typi-
cally occurring between 2 and 12 years
of age, Legg-Perthes disease primarily
affects boys, with a sex ratio of 4 to 5:1.
1
The condition can be bilateral in up to
10% to 20% of affected children.
1
There
is an increased incidence among families
of involved children.
2
Recent evidence
suggests that familial thrombophilia
and/or hypofibrinolysis may play a
causative role in up to 60% to 80% of
children with Legg-Perthes disease.
3-6
The most common thrombophilic defect
described in these children has been the
L
L
egg-Perthes disease in three siblings, two
heterozygous and one homozygous for the factor V
Leiden mutation
Ralph Gruppo,
MD
, Charles J. Glueck,
MD
, Eric Wall,
MD
, Dennis Roy,
MD
, and Ping Wang,
P
h
D
presence of the factor V Leiden muta-
tion, a genetic disorder associated with
resistance to activated protein C.
5,6
It has
been postulated that thrombophilia and
hypofibrinolysis predispose the children
to thrombotic venous occlusion in bone,
which leads to intramedullary hyperten-
sion, anoxia, and ischemic bone death.
3-6
The current report describes a novel
family with heritable resistance to APC
in which transmission of the factor V
Leiden gene mutation occurred across
three generations. Three siblings had
Legg-Perthes disease in association with
the factor V Leiden mutation. Two chil-
dren were heterozygous for the muta-
tion, and one (with bilateral hip involve-
ment) was homozygous. The association
of aseptic necrosis of the hip with resis-
tance to APC in this family provides
compelling evidence for the pathoetio-
logic role of familial thrombophilia in
Legg-Perthes disease in children.
M
ETHODS
Radiographs of both the involved and
uninvolved hips of each patient were re-
viewed and assigned to a category of the
Catterall classification.
7
Group I hips
From the Divisions of Hematology/Oncology and Orthope-
dics, Children’s Hospital Medical Center, and the Choles-
terol Center, Jewish Hospital, Cincinnati, Ohio.
Supported in part by a grant from the Jewish Hos-
pital Medical Research Council.
Submitted for publication Apr. 15, 1997; revision
received Aug. 27, 1997; accepted Sept. 18, 1997.
Reprint requests: Ralph A. Gruppo, MD, Division
of Hematology/Oncology, 3333 Burnet Ave.,
Cincinnati, OH 45229.
Copyright © 1998 by Mosby, Inc.
0022-3476/$5.00 + 0
9/22/86310
APC
Activated protein C
n-FDAPC-SR
Normalized factor V-deficient acti-
vated protein C sensitivity ratio
A family is described with three-generation transmission of factor V Leiden (a
thrombophilic mutation that causes resistance to activated protein C). Legg-
Perthes disease developed in three siblings in this family. The male proband and
his sister were heterozygous for the mutation and had unilateral hip disease at
age 2 years. The brother, who had bilateral hip disease, was homozygous. This
novel family provides compelling evidence for the pathoetiologic role of familial
thrombophilia in Legg-Perthes disease. (J Pediatr 1998;132:885-8)
G
RUPPO ET AL
.
T
HE
J
OURNAL OF
P
EDIATRICS
M
AY
1998
enzyme, with separation of the fragments
on a 2% agarose gel, as previously de-
scribed.
5
C
ASE
R
EPORT
The proband, a 9-year-old boy, was di-
agnosed at age 2 years 8 months with
Legg-Perthes disease of the left hip when
he presented with the sudden onset of
limp and no history of trauma. At pre-
sentation he had 100% involvement of
the femoral head (Fig. 1). He was treat-
ed with home traction at night and ab-
duction casting for 7 months. Because of
persistent stiffness of the hip, he under-
went surgery consisting of an innominate
osteotomy with an acetabular augmenta-
tion procedure. He was shown to be het-
erozygous for the G to A point mutation
at position 1691 of the factor V gene
(factor V Leiden gene mutation) with an
abnormal normalized factor V-deficient
activated protein C sensitivity ratio (III-
1, Fig. 2).His mother (II-3) and father
(II-4) were heterozygous for the factor V
Leiden gene mutation with low n-
FDAPC-SR (Fig. 2). A three-generation
transmission of the factor V Leiden mu-
tation exists within the family (Fig. 2).
A painless limp developed in the
proband’s brother (III-2) at age 2 years 1
month. At that time there was no definite
evidence of Legg-Perthes disease. Subse-
quently, at age 4 years 7 months he expe-
rienced right leg pain and had a limp. Ra-
diographic studies showed bilateral
femoral head involvement consistent with
Legg-Perthes disease of both hips, with
50% involvement on the right and 15%
involvement on the left (Fig. 1). He has
been followed up with observation only.
He is homozygous for the mutant factor
V gene with low n-FDAPC-SR (Fig. 2).
Studies on the proband and his brother
were included in a previous report.
5
The proband’s sister (III-3) was not yet
born when her male siblings were first
studied. Testing for the factor V Leiden
mutation or radiographic studies were not
done until she presented with a limp at age
2 years 10 months. At that time, radi-
ographs showed irregularity of the right
ossification center of the femur. A magnet-
ic resonance imaging scan confirmed
Legg-Perthes disease of the right hip, with
75% involvement (not shown). She has
been followed up with observation only.
She was found to be heterozygous for the
mutant factor V Leiden gene with low n-
FDAPC-SR (Fig. 2). The proband’s ma-
ternal grandmother (I-1, Fig. 2), who had
a pulmonary embolus at age 51 years, had
a normal n-APC-SR, but was found to
have hypofibrinolysis, with high activity of
plasminogen activator inhibitor and low
stimulated tissue plasminogen activator
activity. The proband’s maternal grandfa-
ther (I-2), who was homozygous for the
factor V Leiden mutant allele, had a my-
ocardial infarction at age 51 years (Fig. 2).
Protein C, protein S, antithrombin III,
plasminogen activator inhibitor, plasmino-
gen and lipoprotein (a) levels were found
to be normal in the three siblings when
compared with age-adjusted normal con-
trol levels.
D
ISCUSSION
In 1993, Dahlbäck et al.
9
first de-
scribed the association of familial throm-
886
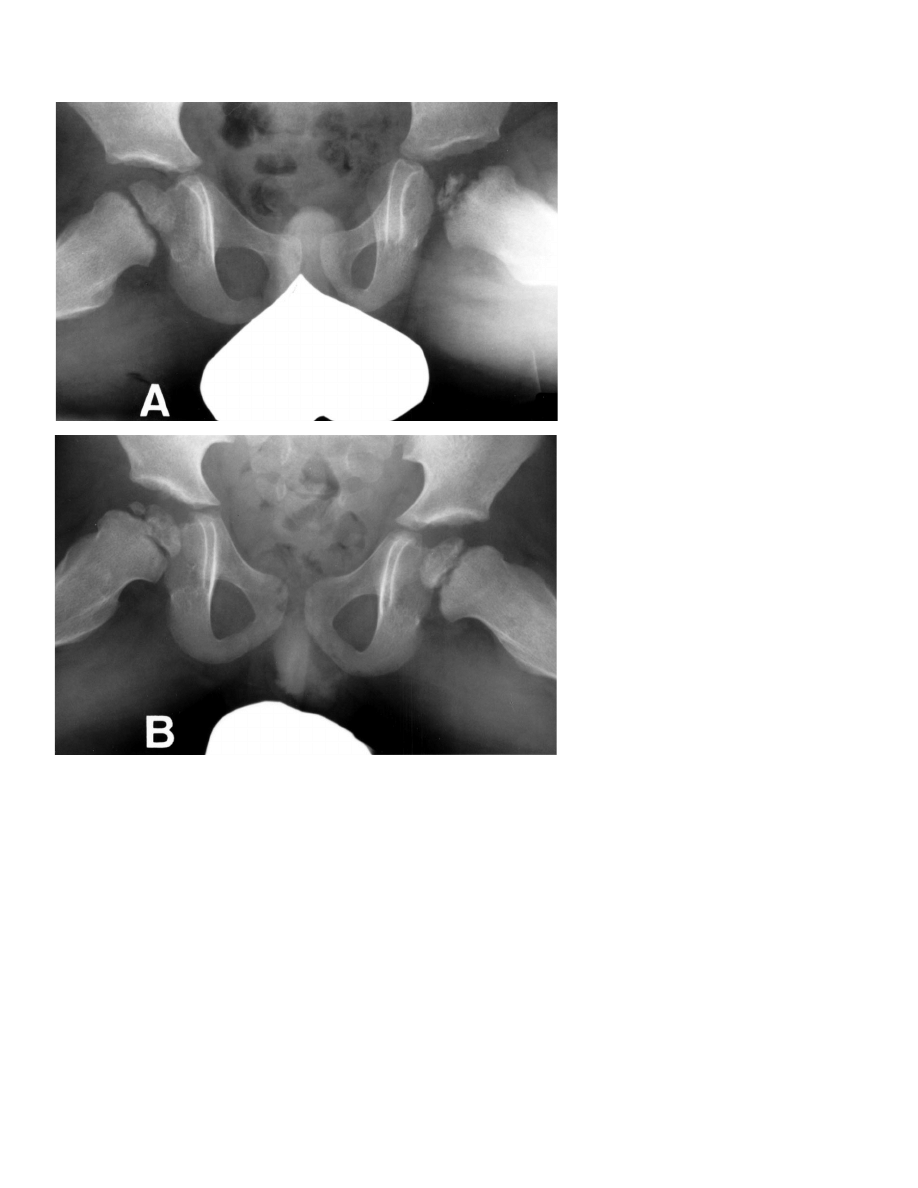
Fig. 1.
Frogleg radiographs of the hips of the proband (A) and brother (B). Legg-Perthes changes include
femoral head fragmentation and small size of ossification. A, The left hip showed 100% femoral head in-
volvement; Catterall group IV at age 3 years.The right hip was normal. B, At 4
1
⁄
2
years, the right hip in-
volvement was 50%; Catterall group II.The left hip was 15% involved; Catterall group I.
T
HE
J
OURNAL OF
P
EDIATRICS
G
RUPPO ET AL
.
V
OLUME
132, N
UMBER
5
bophilia with a poor anticoagulant re-
sponse to APC. The molecular alteration
underlying this phenomenon was identi-
fied by Bertina et al.
10
as an amino acid
substitution at the cleavage site of factor
V (Arg
506
to Gln, factor V Leiden). This
is the result of a single point mutation (G
to A) at position 1691 of the factor V
gene.
10
This mutation results in the resis-
tance of activated factor V to cleavage by
APC. APC resistance has been found to
be the most frequent inherited cause of
thrombosis, with an incidence of APC
resistance ranging from 17.5% to 64% in
cohorts of patients reported from various
studies of venous thrombosis.
11
The
prevalence of carriers of the APC resis-
tance/factor V Leiden trait has been de-
termined to be 2% to 7% in the general
adult population.
11
In 169 healthy chil-
dren studied at our institution, the preva-
lence of heterozygosity for the mutant
factor V Leiden mutation using PCR was
7 (4.1%) of 169.
8
Although the associa-
tion of APC resistance and thrombosis
has been reported mainly in adults, APC
resistance has been recognized recently
as a cause of thrombosis in infants and
children, with manifestations including
venous and arterial thrombosis, purpura
fulminans, and stroke.
12-15
Thrombophilia and hypofibrinolysis
have previously been shown to be associ-
ated with up to 60% to 80% of cases of
Legg-Perthes disease in children.
3-6
Often, two or more thrombophilic fac-
tors may coexist in the same child, sug-
gesting multifactorial causes.
5,6
It has
been postulated that these thrombotic
disorders predispose the patient to ve-
nous thrombotic occlusion in bone,
which leads to intramedullary hyperten-
sion, anoxia, and ischemic bone death
characteristic of osteonecrosis.
3-6
Legg-Perthes disease has been report-
ed to be familial.
1,2
Hall
2
estimated the
incidence of Legg-Perthes disease to be
2.5% in siblings of male index cases. In
this family, all three siblings, two het-
erozygous and one homozygous for the
mutant factor V Leiden gene, had Legg-
Perthes disease. We speculate that the
heritable thrombophilic disorders (in-
cluding resistance to APC) may account,
to a large degree, for the familial occur-
rence of Legg-Perthes disease in chil-
dren.
3-6
Our current on-going studies
should help further define the proportion
of children with familial Legg-Perthes
disease that can be attributed to these
disorders.
Sites other than the hip may be affected
by osteonecrosis in children. Whether the
inherited hypercoagulable disorders are
associated with osteonecrosis in these
other areas is unknown. In our previous
report of 64 children with Legg-Perthes
disease, in which 8 children had the factor
V Leiden mutation, none had known os-
teonecrosis at sites other than the hip.
5
The major promise arising from the
documentation of coagulation abnormali-
ties in the pathogenesis of osteonecrosis
lies in the possibility for halting progres-
sion and facilitating repair of the femoral
head with anticoagulant therapy. Existing
evidence in adults with early-stage os-
teonecrosis suggests that anticoagulant
therapy may stop the progression of os-
teonecrosis and induce regression
6
. Anti-
coagulant therapy is not without risk,
however, especially in young children. We
suggest that a multi-institutional study be
conducted on anticoagulant therapy in se-
lected children expected to have the worst
prognosis for Legg-Perthes disease. Chil-
dren with greater degrees of femoral head
involvement or later onset (after age 5 or
6 years) have a less favorable long-term
prognosis for hip function.
16
Such chil-
dren frequently require total hip replace-
ment surgery as young adults, and would
be the best candidates for such a study on
anticoagulant therapy.
We thank Ann Becker, BS, Ann Pillow, RN,
Davis Stroop, MS, and Trent Tracy, PA, for their
technical assistance, and Alan E.Oestreich, MD,
for reviewing the radiographs.
R
EFERENCES
1. Thompson GH, Salter RB. Legg-Calve-
Perthes disease: current concepts and
controversies. Orthop Clin North Am
1987;18:617-35.
2. Hall DJ. Genetic aspects of Perthes’ dis-
ease: a critical review. Clin Orthop 1986;
209:100-14.
3. Glueck CJ, Crawford A, Roy D,
Freiberg R, Glueck H, Stroop D. Associ-
ation of antithrombotic factor deficien-
cies and hypofibrinolysis with Legg-
Perthes disease. J Bone Joint Surg Am
1996;78:3-13.
4. Glueck CJ, Glueck HI, Greenfield D,
Freiberg R, Kahn A, Hamer T, et al. Pro-
887
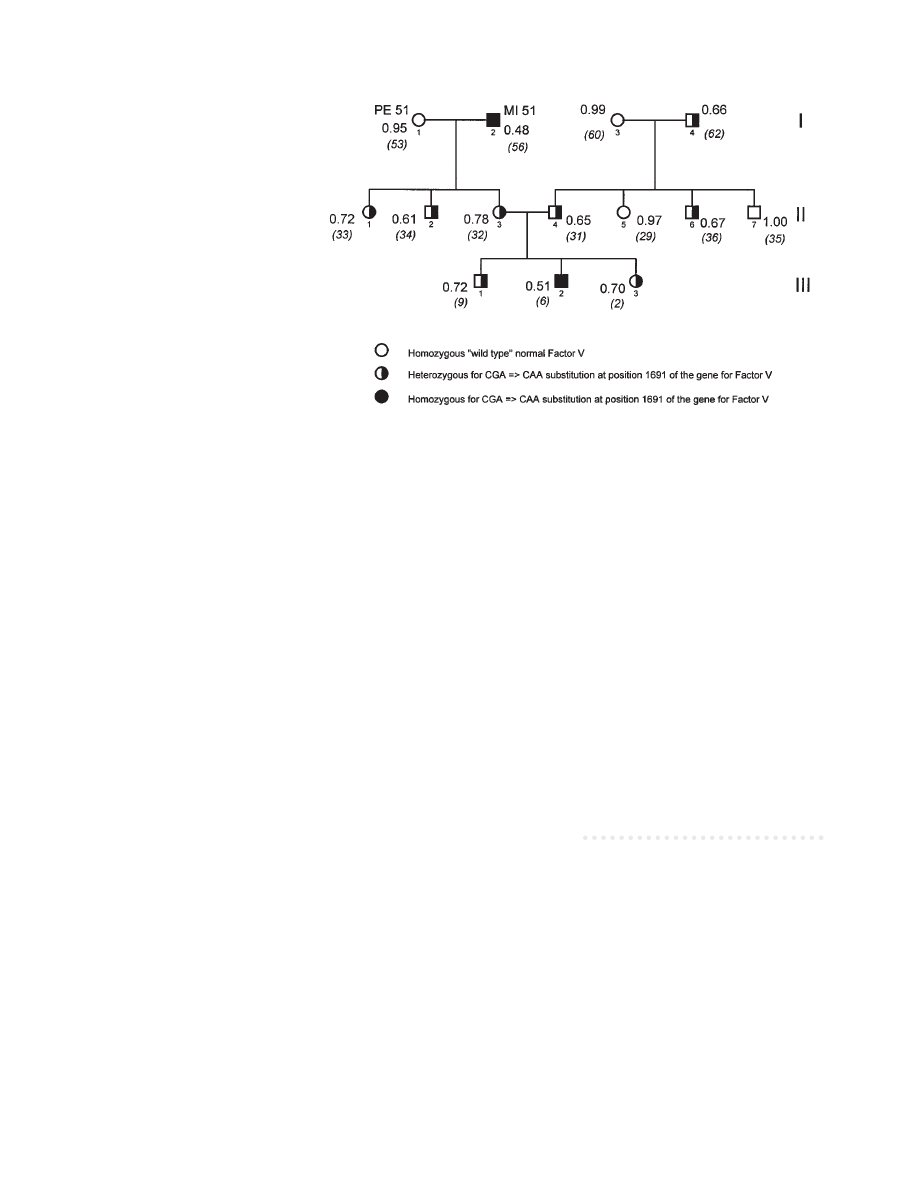
Fig. 2.
Three-generation vertical transmission of resistance to activated protein C, heterozygosity, and ho-
mozygosity for the mutant factor V Leiden trait.The three siblings (generation III) were identified sequen-
tially to have Legg-Perthes disease. Family member I-1 had high plasminogen activator inhibitor activity
(23.1 U/ml, normal range 5.2 to 19.9 U/ml), and low stimulated tissue plasminogen activator activity (0.013
IU/ml, normal range 2.28 to 11.3 IU/ml).
3
She had normal levels of protein C, protein S, antithrombin III,
lipoprotein (a), and fibrinogen. Current age (in years) is displayed in parentheses. nFDAPC-SR ratio is dis-
played next to the genetic symbol (normal 0.93 to 1.09). MI, Myocardial infarction (age of infarction dis-
played); PE, pulmonary embolism (age of embolism displayed).

G
RUPPO ET AL
.
T
HE
J
OURNAL OF
P
EDIATRICS
M
AY
1998
888
tein C and S deficiency, thrombophilia,
and hypofibrinolysis: pathophysiologic
causes of Legg-Perthes disease. Pediatr
Res 1994;35:383-8.
5. Glueck CJ, Brandt G, Gruppo R, Craw-
ford A, Roy D, Tracy T, et al. Resistance
to activated protein C and Legg-Perthes
Disease. Clin Orthop 1997;338:139-52.
6. Glueck CJ, Freiberg R, Gruppo R,
Crawford A, Roy D, Brandt G, et al.
Thrombophilia and hypofibrinolysis: re-
versible pathogenetic etiologies of os-
teonecrosis in adults and children (Legg-
Perthes disease). In: Urbaniak JR,
Jones JP, editors. Osteonecrosis: etiolo-
gy, diagnosis, and treatment. Rosemont
(IL): American Academy of Orthopedic
Surgeons; 1997. p. 105-10.
7. Catterall A. The natural history of
Perthes’ disease. J Bone Joint Surg Br
1971;538:37-53.
8. Brandt G, Gruppo R, Glueck CJ, Stroop
D, Becker A, Pillow A, et al. Sensitivity,
specificity and predictive value of modi-
fied assays for activated protein C resis-
tance in children. Thromb Haemost
1998;79:567-70.
9. Dahlbäck B, Carlsson M, Svensson PJ.
Familial thrombophilia due to a previ-
ously unrecognized mechanism charac-
terized by poor anticoagulant response to
activated protein C: prediction of a cofac-
tor to activated protein C. Proc Natl
Acad Sci U S A 1993;90:1004-8.
10. Bertina RM, Koeleman BPC, Koster T,
Rosendaal FR, Dirven RJ, de Ronde H,
et al. Mutation in blood coagulation fac-
tor V associated with resistance to acti-
vated protein C. Nature 1994;369:64-7.
11. Bertina RM, Reitsma PH, Rosendaal
FR, Vandenbroucke JP. Resistance to
activated protein C and Factor V Leiden
as risk factors for venous thrombosis.
Thromb Haemost 1995;74:449-53.
12. Kodish E, Potter C, Kirschbaum NE,
Foster PA. Activated protein C resis-
tance in a neonate with venous thrombo-
sis. J Pediatr 1995;127:645-8.
13. Nowak-Gottl U, Koch HG, Aschka I,
Kohlhase B, Vielhaber H, Kurlemann G,
et al. Resistance to activated protein C
(APCR) in children with venous or arte-
rial thromboembolism. Br J Haematol
1996;92:992-8.
14. Sifontes MT, Nuss R, Jacobson LJ,
Griffin JH, Manco-Johnson MJ.
Thrombosis in otherwise well children
with the factor V Leiden mutation. J Pe-
diatr 1996;128:324-8.
15. Pipe SW, Schmaier AH, Nichols WC,
Ginsburg D, Bozynski ME, Castle VP.
Neonatal purpura fulminans in associa-
tion with factor V R506Q mutation. J
Pediatr 1996;128:706-9.
16. Wenger DR, Ward T, Herring JA. Cur-
rent concepts review: Legg-Calve-
Perthes disease. J Bone Joint Surg Am
1991;73:778-88.
Wyszukiwarka
Podobne podstrony:
Legg Calvé Perthes Disease in Czech Archaeological Material
Multicenter study for Legg Calvé Perthes disease in Japan
A recurrent mutation in type II collagen gene causes Legg Calvé Perthes disease in a Japanese family
IEEE Finding Patterns in Three Dimensional Graphs Algorithms and Applications to Scientific Data Mi
Osteochondritis dissecans in association with legg calve perthes disease
Intertrochanteric osteotomy in young adults for sequelae of Legg Calvé Perthes’ disease—a long term
Modified epiphyseal index for MRI in Legg Calve Perthes disease (LCPD)
Hip Arthroscopy in Legg Calve Perthes Disease
Legg Calve Perthes disease The prognostic significance of the subchondral fracture and a two group c
Computerized gait analysis in Legg Calve´ Perthes disease—Analysis of the frontal plane
Femoral head vascularisation in Legg Calvé Perthes disease comparison of dynamic gadolinium enhanced
Coxa magna quantification using MRI in Legg Calve Perthes disease
Osteochondritis dissecans in association with legg calve perthes disease
Interruption of the blood supply of femoral head an experimental study on the pathogenesis of Legg C
Legg Calvé Perthes disease multipositional power Doppler sonography of the proximal femoral vascular
Zoledronic acid improves femoral head sphericity in a rat model of perthes disease
Legg Calve Perthes’ disease
Legg Calve Perthes’ disease
więcej podobnych podstron