
Case Report
Hip Arthroscopy in Legg-Calve-Perthes Disease
Timothy R. Kuklo, M.D., J.D., William G. Mackenzie, M.D., F.R.C.S.C,
and Kathryn A. Keeler, B.S.
Summary: The case of a 7-year-old boy with Legg-Calve-Perthes disease is
presented. He had a prominent island of superficial epiphyseal ossification in his
right femoral head, an unusual finding in Legg-Calve-Perthes disease. Hip
arthroscopy was used successfully to identify and treat the lesion. After the
procedure, the patient had a reduction in pain and an increase in range of hip
motion. We believe that this case demonstrates the effective use of hip arthroscopy
in the treatment of this unusual sequela of Legg-Calve-Perthes disease. Key
Words: Hip arthroscopy—Legg-Calve-Perthes disease.
L
egg-Calve-Perthes disease is a disorder of the hip
in children. It is characterized by segmental
necrosis of the femoral head.
1
Late residual deformi-
ties include coxa magna, premature physeal arrest,
deformation of the femoral head, and osteochondritis
dissecans.
2
Goals in the treatment of Legg-Calve-
Perthes disease are to prevent deformity, limit growth
disturbances, and to ultimately prevent degenerative
joint disease. Today, more than 60% of patients with
Legg-Calve-Perthes disease can be successfully treated
nonoperatively.
2
Arthroscopy has been found to be
valuable in treating osteochondritis dissecans, loose
bodies, and chondral flaps, which can occur as late
sequelae in Legg-Calve-Perthes disease.
3-6
In this case,
we describe arthroscopic findings and treatment in the
early management of a symptomatic island of epiphy-
seal ossification.
MATERIALS AND METHODS
A 7-year-old boy with a 2-year history of Legg-
Calve-Perthes disease involving the right hip pre-
sented with difficult ambulation and increasing groin
pain. He recalled no history of trauma or other
antecedent event. He also denied fever, chills, sweats,
or recent illness. He did complain of a significant
amount of grinding in the right hip. He was an
extremely active boy who had markedly reduced his
activities in the past several months, often crawling
instead of walking around the house to reduce the pain.
Physical examination of the right hip revealed a
globally decreased range of motion, most notably in
internal rotation and abduction. Crepitus was noted
with hip motion. Trendelenburg’s sign was negative,
but a trunk shift was present when walking. The right
lower extremity was 1 cm shorter than the left lower
extremity.
Anteroposterior and frog-lateral pelvic radiographs
were consistent with Legg-Calve-Perthes disease of
the right hip in the reossification phase (Fig 1). There
was moderate lateral subluxation (48%) of the femoral
head. A small area of bone on the superior aspect of the
proximal femoral epiphysis was present on both antero-
posterior and frog-lateral radiographs. The hip joint
From Walter Reed Army Medical Center, Washington, D.C.
(T.R.K.); and Alfred I. duPont Hospital for Children, Wilmington,
Delaware (W.G.M., K.A.K.), U.S.A.
Address correspondence and requests for reprints to William G.
Mackenzie, M.D., Department of Orthopaedics, Alfred I. duPont
Hospital for Children, P.O. Box 269, Wilmington, DE 19899, U.S.A.
r
1999 by the Arthroscopy Association of North America
0749-8063/99/1501-1792$3.00/0
88
Arthroscopy: The Journal of Arthroscopic and Related Surgery, Vol 15, No 1 (January-February), 1999: pp 88–92
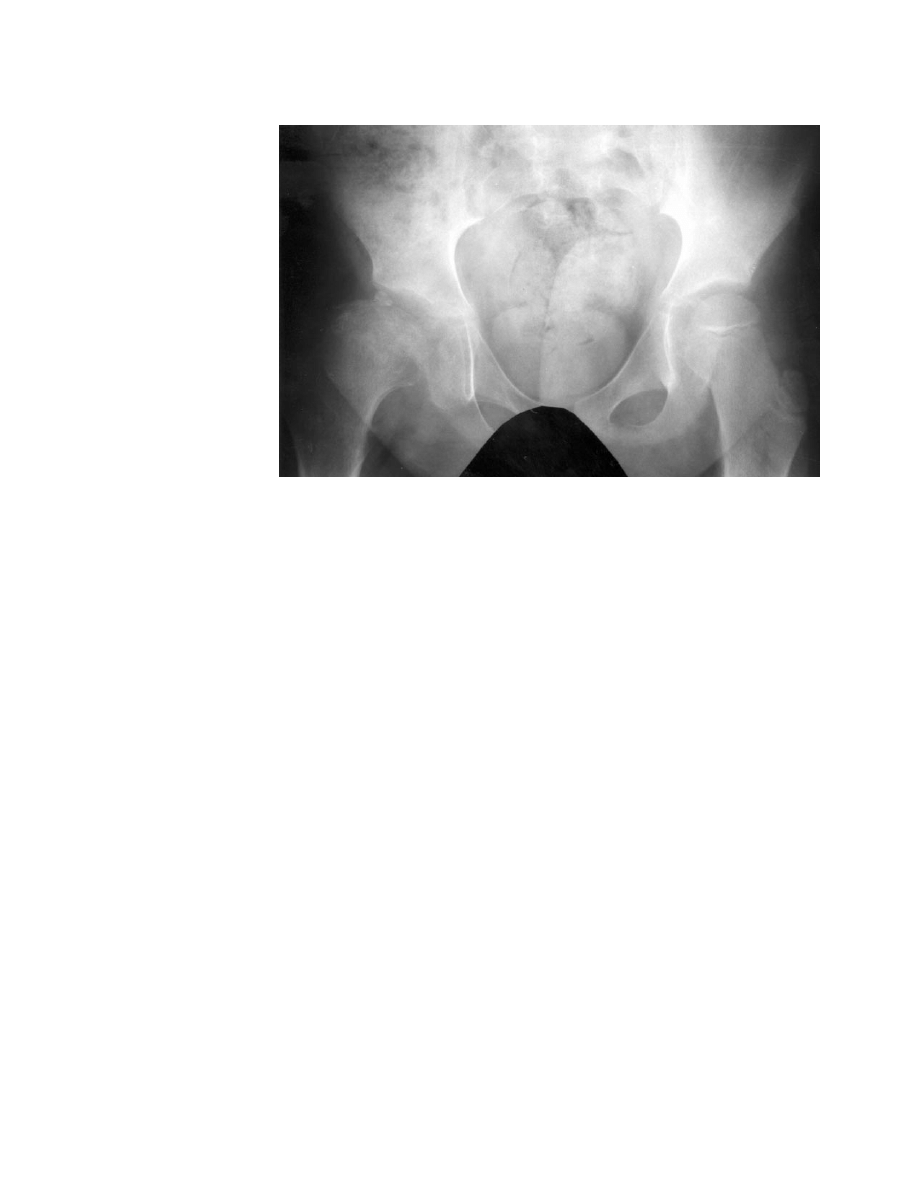
space was wider on the right affected side when
compared with the contralateral side.
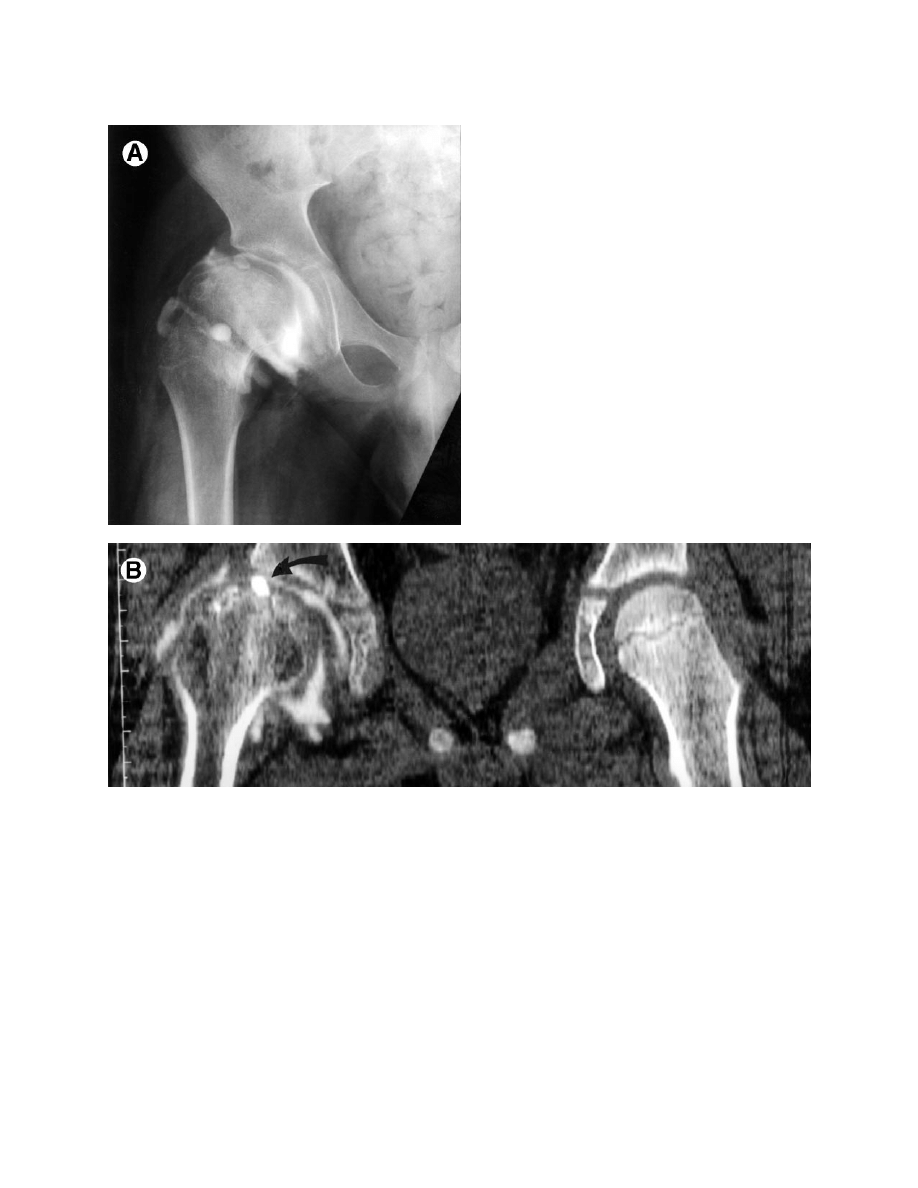
A computed tomography/arthrogram was obtained
to further evaluate the epiphyseal island of bone (Fig
2). The bone island did not appear to be mobile, but it
was surrounded by contrast indicating communication
with the joint. The bony surface of the lesion was
intra-articular with no apparent overlying cartilage.
Magnetic resonance imaging did not provide any
further information.
A right hip arthroscopy was performed with the
patient in a supine position in traction on a fracture
table. The joint was well-visualized on insertion of the
arthroscope through the lateral approach as described
by Glick et al.
7
The portal for the arthroscope was
anterior to that used for the instrumentation. The
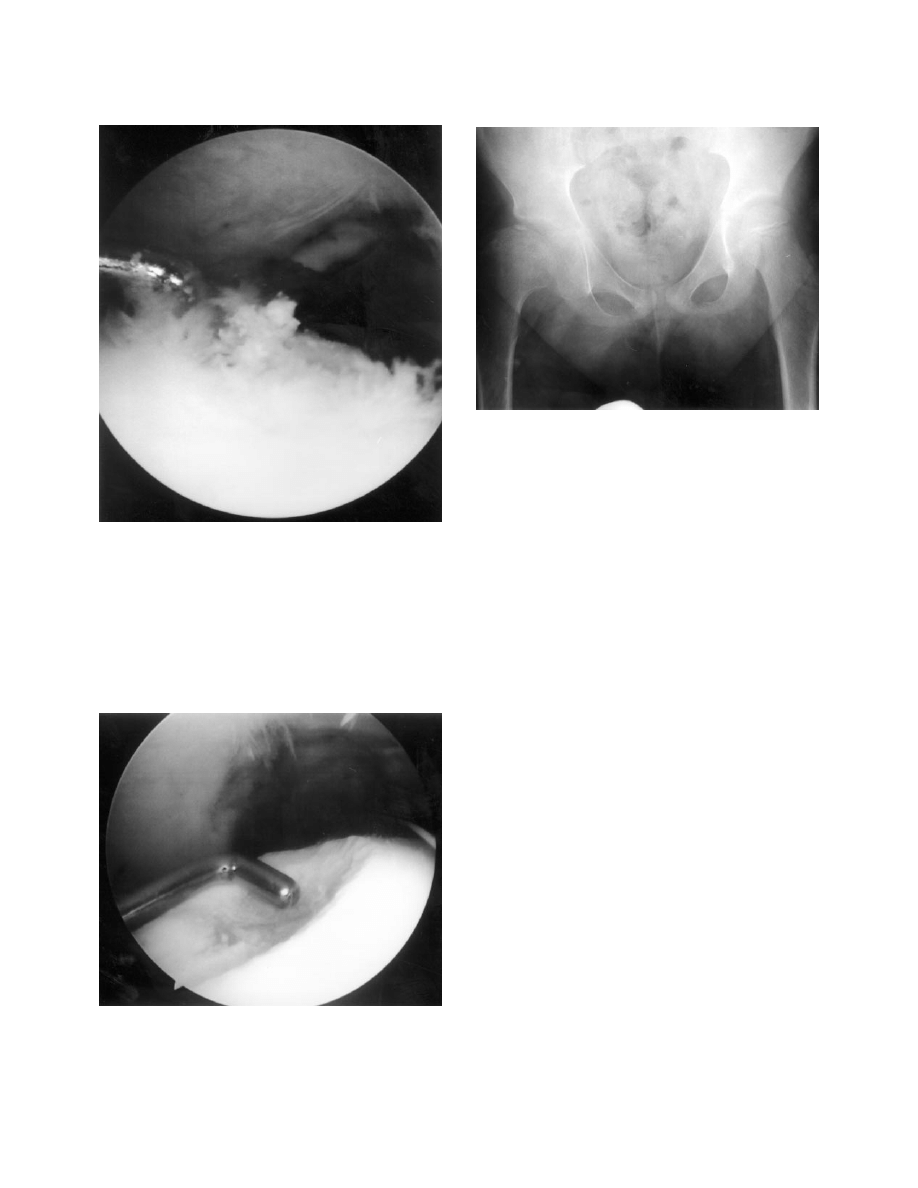
acetabular articular surface was intact except for a
small area of acetabular chondral fibrillation on the
surface opposite the epiphyseal island on the femoral
head (Fig 3). The area of epiphyseal ossification
projected above the femoral surface and was nonvascu-
lar bone (Fig 3). Manipulation with a probe did not
reveal any mobility of the epiphyseal island. A 4.0-mm
burr was used to debride the lesion and decrease its
prominence below the articular surface (Fig 4). No
bony bleeding was noted after burring.
RESULTS
The patient returned to school 2 days after the
operation and progressively increased his activities
over the next 2 weeks. At his 5-month follow-up
appointment, he had no pain and good range of
motion. Right hip flexion had improved from 105°
preoperatively to 120°, abduction had improved from
25° to 45°, and internal rotation from 25° to 60°. His
limp had resolved. Radiographs showed a remnant of
the epiphyseal ossification with no other abnormalities
(Fig 5).
DISCUSSION
This case details the unusual finding and arthro-
scopic evaluation of a superficial area of epiphyseal
ossification in Legg-Calve-Perthes disease. Orthopae-
dic surgeons have used arthroscopy as an alternative to
open surgery in the treatment of hip disorders.
3,8,9-12
When compared with open surgery, arthroscopy al-
lows for a less invasive method of exploring the hip
joint and less traumatic removal of loose or foreign
bodies.
9,12,13
Hip arthroscopy allows the surgeon to
obtain adequate visualization of the joint surfaces
without dislocation of the hip, potentially reducing the
risk of avascular necrosis of the femoral head.
6
In
addition, patients experience minimal postoperative
morbidity and shorter rehabilitation with hip arthros-
copy.
3,7,13
Hip arthroscopy has been used in the treatment of
children with hip disorders such as acetabular labral
tears, loose bodies, chondral injuries, and septic arthri-
tis, as well as in the diagnosis of other disorders.
4,6,13,14
In 1977, Gross
13
described his early experience with
F
IGURE
1.
Anteroposterior
pelvic radiograph revealing a
superficial area of epiphyseal
ossification on the right femoral
head.
89
HIP ARTHROSCOPY IN PERTHES DISEASE
hip arthroscopy in patients with congenital dislocation
of the hip, Legg-Calve-Perthes disease, slipped capital
femoral epiphysis, and neuropathic subluxation. Holg-
ersson et al.
14
described diagnostic arthroscopy in 13
children (15 hips) with chronic juvenile rheumatoid
arthritis.
Several authors have discussed the use of hip
arthroscopy in Legg-Calve-Perthes disease.
3,4,6,13
Gross
performed 20 arthroscopies on 17 children with Legg-
Calve-Perthes disease. Although he did not make
specific treatment recommendations, he reported ob-
serving flattening of the femoral head in all cases and
femoral cartilage fibrillation in two thirds of the hips.
Several of the hips also had defects in the articular
cartilage of the femoral head at the lateral lip of the
acetabulum.
13
In 1993, Lechevallier and Bowen
4
de-
scribed the successful use of arthroscopy in the
treatment of children with loose osteochondral frag-
ments, which are late sequelae of Legg-Calve-Perthes
disease. In addition, Bowen et al.
3
used hip arthros-
copy in treating adults with osteochondritis dissecans,
another late sequela of Legg-Calve-Perthes disease.
Arthroscopic intervention for our patient was simi-
lar to the use of arthroscopy in the treatment of loose
bodies and osteochondritis dissecans.
3,4
However, the
reported lesion differs from the previously described
conditions. Unlike a loose body, the area of epiphyseal
ossification was intimately associated with the articu-
F
IGURE
2.
(A) Arthrogram showing the area of epiphyseal
ossification extending to the articular surface. (B) Computed
tomography/arthrogram of the right hip showing the lesion
extending to the articular surface surrounded by contrast.
90
T. R. KUKLO ET AL.
lar cartilage. Unlike osteochondritis dissecans, the
bony area that extended superficial to the cartilage did
not have overlying articular cartilage or evidence of an
underlying subchondral bone defect from which it had
originated. The lesion appeared to originate from the
epiphysis and not to have been embedded there by
compressive forces. Perhaps it was a remnant of
necrotic bone from the process of the Legg-Calve-
Perthes disease.
Indications for treatment of our patient included
increasing pain with radiographic evidence of an
island of superficial epiphyseal ossification, an un-
usual finding in Legg-Calve-Perthes disease. Arthro-
scopic findings included acetabular articular fibrilla-
tion opposite the bone embedded in the femoral
cartilage, indicating mechanical wear. Although the
lesion was not completely removed, the bony promi-
nence was reduced below the level of the surrounding
articular cartilage. Five months after surgery, the
patient was much improved with an almost full range
of motion.
REFERENCES
1. Lee DM. Disorders of the hip. Philadelphia: JB Lippincott,
1983.
2. Weinstein SL. Legg-Calve-Perthes disease. In: Morrissey RT,
Weinstein SL, eds. Lovell and Winter’s pediatric orthopaedics.
Ed 4. Philadelphia: Lippincott-Raven, 1996;951-991.
3. Bowen JR, Kumar VP, Joyce JJ 3d, Bowen JC. Osteochondritis
dissecans following Perthes’ disease. Arthroscopic-operative
treatment. Clin Orthop 1986;209:49-56.
4. Lechevallier J, Bowen JR. Arthroscopic treatment of the late
sequelae of Legg-Calve-Perthes disease. J Bone Joint Surg Br
1993;75:160 (suppl 2).
5. McCarthy JC, Day B, Busconi B. Hip arthroscopy: Applica-
tions and techniques. J Am Acad Orthop Surg 1995;3:115-122.
6. Schindler A, Lechevallier JJ, Rao NS, Bowen JR. Diagnostic
and therapeutic arthroscopy of the hip in children and adoles-
cents: evaluation of results. J Pediatr Orthop 1995;15:317-321
7. Glick JM, Sampson TG, Gordon RB, Behr JT, Schmidt E. Hip
arthroscopy by the lateral approach. Arthroscopy 1987;3:4-12.
F
IGURE
3.
Arthroscopic view of the right hip joint. The area of
epiphyseal ossification on the femoral head (right) was nonvascular
and had a ‘‘fluffy’’ appearance.
F
IGURE
4.
Arthroscopic view of the right hip joint shows the
femoral head following debridement (below) and chondral fibrilla-
tion of the acetabular surface opposite the lesion (above).
F
IGURE
5.
Anteroposterior pelvic radiograph taken 6 weeks after
surgery.
91
HIP ARTHROSCOPY IN PERTHES DISEASE

8. Goldman A, Minkoff J, Price A, Krinick R. A posterior
arthroscopic approach to bullet extraction from the hip. J
Trauma 1987;27:1294-1300.
9. Ide T, Akamatsu N, Nakajima I. Arthroscopic surgery of the hip
joint. Arthroscopy 1991;7:204-211.
10. Shifrin LZ, Reis ND. Arthroscopy of a dislocated hip replace-
ment: A case report. Clin Orthop 1980;146:213-214.
11. Vakili F, Salvati EA, Warren RF. Entrapped foreign body
within the acetabular cup in total hip replacement. Clin Orthop
1980;150:159-162.
12. Witwity T, Uhlmann RD, Fischer J. Arthroscopic management
of chondromatosis of the hip joint. Arthroscopy 1988;4:55-56.
13. Gross RH. Arthroscopy in hip disorders in children. Orthop
Rev 1977;6:43-49.
14. Holgersson S, Brattstrom H, Mogensen B, Lidgren L. Arthros-
copy of the hip in juvenile chronic arthritis. J Pediatr Orthop
1981;1:273-278.
92
T. R. KUKLO ET AL.
Wyszukiwarka
Podobne podstrony:
Modified epiphyseal index for MRI in Legg Calve Perthes disease (LCPD)
Computerized gait analysis in Legg Calve´ Perthes disease—Analysis of the frontal plane
Coxa magna quantification using MRI in Legg Calve Perthes disease
Osteochondritis dissecans in association with legg calve perthes disease
Osteochondritis dissecans in association with legg calve perthes disease
Interruption of the blood supply of femoral head an experimental study on the pathogenesis of Legg C
Legg Calve Perthes’ disease
Legg Calve Perthes’ disease
Legg Calve Perthes disease The prognostic significance of the subchondral fracture and a two group c
Femoral head vascularisation in Legg Calvé Perthes disease comparison of dynamic gadolinium enhanced
Interruption of the blood supply of femoral head an experimental study on the pathogenesis of Legg C
Intertrochanteric osteotomy in young adults for sequelae of Legg Calvé Perthes’ disease—a long term
Legg Calvé Perthes Disease in Czech Archaeological Material
Multicenter study for Legg Calvé Perthes disease in Japan
A recurrent mutation in type II collagen gene causes Legg Calvé Perthes disease in a Japanese family
Legg Calvé Perthes disease multipositional power Doppler sonography of the proximal femoral vascular
Cementless Ceramic Hip Arthroplasties in Patients Less Than 30 Years Old
Acute chondrolysis complicating Legg Calvé Perthes disease
Legg Perthes disease in three siblings, two heterozygous and one homozygous for the factor V Leiden
więcej podobnych podstron