Contents
lists
available
at
Resuscitation
j o
u
r n
a l
h o m
e p a g e
:
w w w . e l s e v i e r . c o m / l o c a t e / r e s u s c i t a t i o n
Clinical
paper
Acute
coronary
angiography
in
patients
resuscitated
from
out-of-hospital
cardiac
arrest—A
systematic
review
and
meta-analysis
夽
Jacob
Moesgaard
Larsen
,
Jan
Ravkilde
Department
of
Cardiology
and
Centre
for
Cardiovascular
Research,
Aalborg
University
Hospital,
Hobrovej
18-22,
9000
Aalborg,
Denmark
a
r
t
i
c
l
e
i
n
f
o
Article
history:
Received
22
June
2012
Received
in
revised
form
30
August
2012
Accepted
30
August
2012
Keywords:
Coronary
angiography
Heart
arrest
Outcome
a
b
s
t
r
a
c
t
Introduction:
Out-of-hospital
cardiac
arrest
has
a
poor
prognosis.
The
main
aetiology
is
ischaemic
heart
disease.
Aim:
To
make
a
systematic
review
addressing
the
question:
“In
patients
with
return
of
spontaneous
circulation
following
out-of-hospital
cardiac
arrest,
does
acute
coronary
angiography
with
coronary
intervention
improve
survival
compared
to
conventional
treatment?”
Methods:
Peer
reviewed
articles
written
in
English
with
relevant
prognostic
data
were
included.
Compar-
ison
studies
on
patients
with
and
without
acute
coronary
angiography
were
pooled
in
a
meta-analysis.
Results:
Thirty-two
non-randomised
studies
were
included
of
which
22
were
case-series
without
patients
with
conservative
treatment.
Seven
studies
with
specific
efforts
to
control
confounding
had
statistical
evidence
to
support
the
use
of
acute
coronary
angiography
following
resuscitation
from
out-of-hospital
cardiac
arrest.
The
remaining
25
studies
were
considered
neutral.
Following
acute
coronary
angiography,
the
survival
to
hospital
discharge,
30
days
or
six
months
ranged
from
23%
to
86%.
In
patients
without
an
obvious
non-cardiac
aetiology,
the
prevalence
of
significant
coronary
artery
disease
ranged
from
59%
to
71%.
Electrocardiographic
findings
were
unreliable
for
identifying
angiographic
findings
of
acute
coronary
syndrome.
Ten
comparison
studies
demonstrated
a
pooled
unadjusted
odds
ratio
for
survival
of
2.78
(1.89;
4.10)
favouring
acute
coronary
angiography.
Conclusion:
No
randomised
studies
exist
on
acute
coronary
angiography
following
out-of-hospital
cardiac
arrest.
An
increasing
number
of
observational
studies
support
feasibility
and
a
possible
survival
benefit
of
an
early
invasive
approach.
In
patients
without
an
obvious
non-cardiac
aetiology,
acute
coronary
angiography
should
be
strongly
considered
irrespective
of
electrocardiographic
findings
due
to
a
high
prevalence
of
coronary
artery
disease.
© 2012 Elsevier Ireland Ltd. All rights reserved.
1.
Introduction
Out-of-hospital
cardiac
arrest
(OHCA)
has
a
poor
prognosis
and
is
a
leading
cause
of
death.
The
incidence
of
OHCA
treated
by
the
emergency
medical
service
in
Europe
has
been
estimated
to
be
approximately
275,000
persons
per
year
with
a
survival
of
10.7%
for
all
rhythms
and
21.2%
for
ventricular
fibrillation
arrest.
most
frequent
cause
of
OHCA
is
ischaemic
heart
disease.
coro-
nary
angiography
(CAG)
with
percutaneous
coronary
intervention
(PCI)
is
the
treatment
of
choice
in
patients
with
acute
coronary
syn-
drome
(ACS)
with
ST-segment
elevation
(STEMI)
or
new
left
bundle
branch
block
(LBBB)
in
the
electrocardiogram
(ECG)
without
pre-
ceding
cardiac
arrest.
prognostic
value
of
acute
CAG
following
夽 A
Spanish
translated
version
of
the
abstract
of
this
article
appears
as
Appendix
in
the
final
online
version
at
http://dx.doi.org/10.1016/j.resuscitation.2012.08.337
.
∗ Corresponding
author.
address:
(J.M.
Larsen).
return
of
spontaneous
circulation
(ROSC)
after
OHCA
is
less
clear,
especially
in
comatose
survivors.
The
topic
was
evaluated
in
the
2010
International
Consensus
on
Cardiopulmonary
Resuscitation
and
Emergency
Cardiovascular
Care
Science
with
Treatment
Rec-
ommendations
(2010
recommendation
was:
acute
CAG
should
be
considered
in
STEMI
or
clinical
suspicion
of
coro-
nary
ischaemia
as
a
likely
cause
of
the
arrest,
and
that
it
may
be
reasonable
to
be
included
in
a
systematic
standardised
post
cardiac
arrest
protocol.
Several
new
studies
have
emerged.
The
aim
of
this
study
was
to
make
an
updated
systematic
review
of
the
evidence
on
performing
acute
CAG
following
ROSC
after
OHCA.
2.
Methods
The
study
was
conducted
in
accordance
with
the
principles
stated
by
the
Meta-analysis
Of
Observational
Studies
in
Epi-
demiology
(MOOSE)
group
and
the
Preferred
Reporting
Items
for
Systematic
Reviews
and
Meta-analysis
(PRISMA)
short,
we
defined
a
structured
question
describing
the
Population,
0300-9572/$
–
see
front
matter ©
2012 Elsevier Ireland Ltd. All rights reserved.

1428
J.M.
Larsen,
J.
Ravkilde
/
Resuscitation
83 (2012) 1427–
1433
Intervention,
Comparison
and
Outcome
(PICO).
This
was
followed
by
literature
search
and
critical
appraisal
of
the
evidence.
The
eli-
gible
studies
were
summarised
in
tables,
and
the
outcome
was
evaluated
in
a
meta-analysis.
2.1.
PICO
question
“In
patients
with
ROSC
following
OHCA
(P),
does
acute
CAG
with
coronary
intervention
(I),
compared
to
conventional
treatment
(C),
improve
survival
(O)?
2.2.
Literature
search
The
literature
search
was
performed
on
May
1st,
2012,
in
collab-
oration
with
experienced
research
librarians.
PubMed
search
terms
were:
“Heart
arrest”
[Mesh]
AND
(“Coronary
Angiography”
[Mesh]
OR
“Angioplasty,
Balloon,
Coronary”
[Mesh]).
Embase
search
terms
were:
“exp
heart
arrest”
AND
(“exp
angiocardiography”
OR
“exp
transluminal
coronary
angioplasty”).
SveMed+
search
terms
were:
“exp
Heart-Arrest”
AND
(“exp
Coronary-Angiography”
OR
“exp
Angioplasty,-Transluminal,
Percutaneous
Coronary”).
The
identi-
fied
records
were
managed
using
reference
management
software
(RefWorks
2.0,
ProQuest
LLC,
USA).
Duplicates
were
identified
and
deleted.
Screening
of
the
records
was
done
by
one
author
(Larsen
JM).
Reviews,
case
reports,
editorials,
letters,
comments,
conference
abstracts,
records
with
clearly
no
relevance
to
the
PICO
question,
and
articles
not
written
in
English
were
excluded.
Full
text
arti-
cles
were
evaluated
for
eligibility
by
both
authors.
Articles
without
prognostic
data
at
hospital
discharge,
30
days
or
six
months
for
patients
with
acute
CAG
or
with
double
publication
of
prognostic
data
were
excluded.
Other
literature
sources
were
screening
of
the
reference
lists
of
the
included
articles
and
2010
CoSTR
and
the
peer
review
process.
2.3.
Evidence
appraisal
The
level
of
evidence
(LOE)
was
evaluated
by
both
authors:
LOE
1—randomised
controlled
trials
or
meta-analyses
of
randomised
controlled
trials;
LOE
2—studies
using
concurrent
controls
without
randomisation
for
comparison;
LOE
3—studies
using
retrospective
controls
for
comparison;
LOE
4—studies
without
a
control
group
for
comparison;
and
LOE
5—studies
not
directly
related
to
the
spe-
cific
population.
studies
without
matched
concurrent
controls
were
classified
as
LOE
4.
The
studies
were
categorised
as
prospective
or
retrospective
as
a
simple
evaluation
of
quality.
Stud-
ies
favouring
acute
CAG
in
a
propensity
score
analysis
or
reporting
a
significant
adjusted
odds
ratio
in
favour
of
acute
CAG
or
acute
PCI
were
classified
as
“supporting”
PICO.
Studies
with
non-significant
adjusted
results
were
classified
as
“neutral”
to
PICO.
Studies
with
significant
adjusted
results
favouring
conservative
treatment
were
classified
as
“opposing”.
To
be
conservative,
case-series
without
comparison
groups
were
classified
as
“neutral”
despite
high
sur-
vival
rates
due
to
possible
selection
bias.
2.4.
Statistics
The
statistical
analysis
was
performed
with
a
significance
level
of
p
<
0.05
(Stata
11,
StataCorp
LP,
USA).
Data
was
collected
from
the
result
sections
of
the
included
articles.
Comparison
studies
were
included
in
a
meta-analysis
estimating
an
unadjusted
pooled
OR
for
survival
using
a
random-effect
model.
The
heterogeneity
of
the
studies
was
evaluated
by
the
I-squared
measure,
which
describes
the
percentage
of
variation
across
the
studies
due
to
heterogeneity
rather
than
chance.
3.
Results
3.1.
Eligible
studies
The
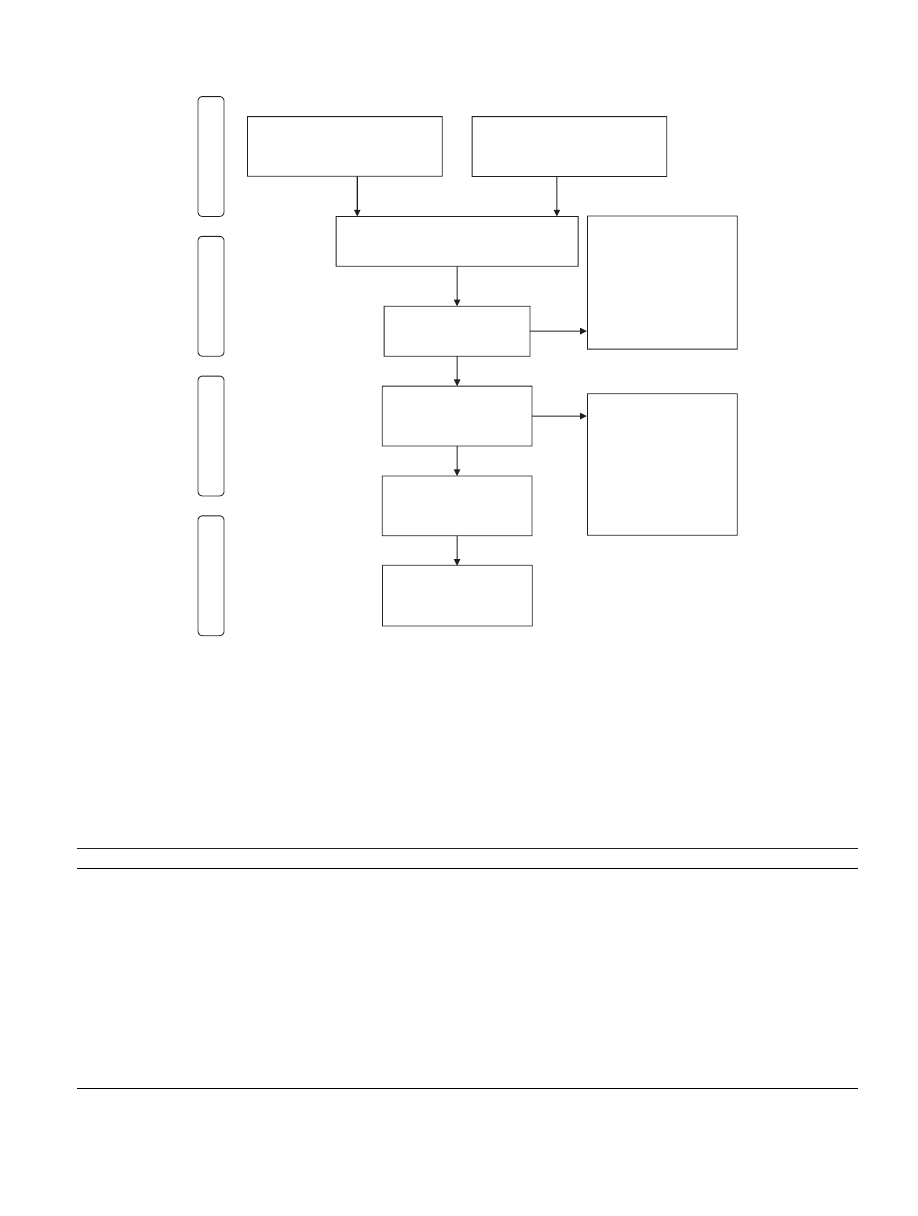
literature
search
is
illustrated
in
the
flow
diagram
in
Thirty-two
studies
met
the
criteria
for
inclusion
in
the
review.
Ten
were
included
in
the
meta-analysis.
Seven
studies
were
clas-
sified
as
supporting
acute
CAG
following
ROSC
after
OHCA,
and
the
remaining
25
studies
were
neutral.
Twelve
studies
were
not
considered
in
the
2010
CoSTR,
primarily
due
to
publication
after
completion
of
the
2010
CoSTR
evaluation
process.
marises
the
LOE
and
design
of
the
included
studies:
LOE
2
(one
study),
LOE
4
(22
studies)
and
LOE
5
(nine
studies).
In
all
cases,
LOE
5
was
due
to
inclusion
of
patients
with
in-hospital
cardiac
arrest
or
cardiac
arrest
without
specification
of
location.
Seventeen
studies
were
retrospective.
3.2.
Studies
on
acute
coronary
angiography
in
ST-segment
elevation
myocardial
infarction
summarises
the
characteristics
of
the
15
studies
on
acute
CAG
in
patients
with
STEMI
following
ROSC.
survival
ranged
from
41%
to
92%.
Common
characteristics
were
male
sex,
witnessed
cardiac
arrest,
OHCA
and
shockable
rhythm.
The
inclu-
sion
periods
were
generally
before
or
in
the
early
era
of
therapeutic
hypothermia
(TH),
and
the
use
of
TH
was
therefore
low
despite
a
high
prevalence
of
comatose
survivors
on
arrival
to
hospital.
The
largest
study
is
a
retrospective
case
series
of
186
consecutive
patients
undergoing
acute
CAG
due
to
ST-segment
elevation
or
Table
1
Evidence
level
and
design
of
the
studies
included
in
the
systematic
review.
Study
design
LOE
1
LOE
2
LOE
3
LOE
4
LOE
5
Studies
supporting
acute
CAG
following
OHCA
Prospective
–
–
–
Cronier
–
Dumas
Gräsner
Tömte
Spaulding
Retrospective
–
–
–
Merchant
Studies
neutral
to
acute
CAG
following
OHCA
Prospective
–
–
–
Bendz
Quintero-Moran
Kahn
Lettieri
Mooney
Möllmann
Nielsen
Peels
Pleskot
Retrospective
–
–
–
Anyfantakis
Garot
Hosmane
Knafelj
Hovdenes
Mager
Keelan
Reynolds
Markusohn
Richling
McCullough
Sideris
Wolfrum
Studies
opposing
acute
CAG
following
OHCA
Prospective
–
–
–
–
–
Retrospective
–
–
–
–
–
LOE
=
level
of
evidence
(1
– randomised
controlled
trials
or
meta-analyses
of
randomised
controlled
trials;
2
–
studies
using
concurrent
controls
without
ran-
domisation
for
comparison;
3
–
studies
using
retrospective
controls
for
comparison;
4
–
studies
without
a
control
group
for
comparison;
and
5
–
studies
not
directly
related
to
the
specific
population;
CAG
=
coronary
angiography;
OHCA
=
out-of-
hospital
cardiac
arrest.
a
Studies
not
evaluated
in
the
2010
International
Consensus
on
Cardiopulmonary
Resuscitation
and
Emergency
Cardiovascular
CareScience
with
Treatment
Recom-
mendations
document.
J.M.
Larsen,
J.
Ravkilde
/
Resuscitation
83 (2012) 1427–
1433
1429
Records identified through
database searching
(n = 1484)
Screening
Included
Eligibility
Identification
Additional records identified
through other sources
(n = 5)
Records after duplicates removed
(n = 1313)
Records screened
(n = 1313)
Records excluded
(n = 1249)
Reviews; case reports;
editorials; letters;
comments; conference
abstracts; studies not
relevant to PICO; non-
English writing.
Full-text articles
assessed for eligibility
(n = 64)
Full-text articles
excluded
(n = 32)
Necessary prognostic
information not
available; double-
publication of prognostic
data; studies not
relevant to PICO.
Studies included in
the systematic review
(n = 32)
Studies included in
the meta-analysis
(n = 10)
Fig.
1.
Flow
chart
of
the
selection
of
articles
for
the
systematic
review
and
meta-analysis.
The
database
search
included
PubMed
(n
=
613
records),
Embase
(n
=
866
records)
and
SveMed+
(n
=
5).
The
records
from
other
sources
were
obtained
by
screening
reference
lists
of
the
included
studies
and
the
2010
International
Consensus
on
Cardiopulmonary
Resuscitation
and
Emergency
Cardiovascular
Care
Science
with
Treatment
Recommendations
document
and
the
peer
review
process.
PICO
=
patient,
intervention,
comparison,
outcome.
presumed
new
LBBB
after
ROSC,
mainly
after
OHCA.
coronary
occlusion
was
found
in
74%.
The
remaining
patients
had
severe
chronic
stenosis.
The
survival
to
hospital
discharge
was
55%.
The
survival
at
six
months
was
54%,
primarily
with
a
good
neuro-
logical
status.
A
comparably
good
long-term
prognosis
was
seen
in
two
other
study,
comparing
direct
admittance
to
a
PCI
centre
and
transfer
from
a
referral
hospital,
demon-
strated
no
significant
difference
in
survival,
but
the
proportion
of
non-transferred
patients
with
preserved
left
ventricular
ejection
fraction
was
higher
(61%
vs
25%,
p
=
0.02).
comparison
of
Table
2
Characteristics
of
studies
on
acute
coronary
angiography
in
patients
with
ST-segment
elevation
myocardial
infarction.
Study
Inclusion
of
patients
N
OHCA
(%)
Witnessed
(%)
VF/VT
(%)
Unconscious
(%)
TH
(%)
Survival
Kahn
et
1989–1994
11
100
NA
100
64
0
51
McCullough
et
al.,
1989–1996
22
100
100
91
NA
0
41
Bendz
et
al.,
1998–2001
100
100
90
90
0
73
Quintero-Moran
et
al.,
2000–2003
63
43
100
81
NA
NA
68
(30
days)
Markusohn
et
al.,
1998–2006
25
100
92
84
72
8
76
Garot
et
1995–2005
186
84
67
NA
NA
18
55
Knafelj
et
al.,
2000–2005
72
NA
100
100
100
56
61
Richling
et
al.,
1991–2003
98
98
100
NA
37
55
(6
months)
Pleskot
et
al.,
Republic
2002–2004
100
NA
100
90
NA
70
Peels
et
Netherlands
2004–2005
44
100
NA
NA
NA
NA
50
Mager
et
al.,
2001–2006
21
NA
NA
NA
43
5
86
(30
days)
Wolfrum
et
2003–2006
33
100
NA
100
100
48
70
(6
months)
Lettieri
et
2005
100
70
90
NA
12
78
Szymanski
et
al.,
NA
NA
NA
100
NA
NA
92
(30
days)
Hosmane
et
al.,
2002–2006
98
68
90
NA
75
NA
64
Total
NA
792
NA
NA
NA
NA
NA
64
(mean)
N
=
number
of
patients;
OHCA
=
out-of-hospital
cardiac
arrest;
VF/VT
=
ventricular
fibrillation
or
tachycardia;
TH
=
therapeutic
hypothermia;
NA
=
not
available.
a
Survival
to
hospital
discharge
unless
otherwise
stated.
b
Only
data
on
patients
with
acute
coronary
angiography
following
cardiac
arrest
is
reported
from
the
study.
1430
J.M.
Larsen,
J.
Ravkilde
/
Resuscitation
83 (2012) 1427–
1433
Table
3
Characteristics
of
studies
on
patients
with
systematic
acute
coronary
angiography
following
out-of-hospital
cardiac
arrest
without
an
obvious
non-cardiac
aetiology.
Study
Inclusion
of
patients
n
ST-segment
elevation
or
LBBB
(%)
Significant
CAD
(%)
Angiographic
ACS
(%)
PCI
(%)
VF/VT
(%)
Unconscious
(%)
TH
(%)
Survival
Spaulding
et
al.,
1994–1996
84
63
71
69
33
93
NA
0
38
Anyfantakis
et
al.,
2001–2006
72
49
64
45
33
50
94
NA
49
Dumas
et
2003–2008
435
70
46
41
68
NA
86
39
Sideris
et
2002–2008
165
50
59
36
30
51
99
76
31
Möllmann
et
al.,
2003–2005
65
NA
NA
58
NA
NA
NA
81
(6
months)
Total
1994–2008
821
42
NA
NA
39
NA
NA
NA
41
(mean)
N
=
number
of
patients;
LBBB
=
left
bundle
branch
block;
CAD
=
coronary
artery
disease;
angiographic
ACS
=
recent
occlusion
or
irregular
lesion
at
angiography
in
resuscitated
patients;
PCI
=
percutaneous
coronary
intervention;
VF/VT
=
ventricular
fibrillation
or
tachycardia;
TH
=
therapeutic
hypothermia;
NA
=
not
available.
a
Survival
to
hospital
discharge
unless
otherwise
stated.
b
Only
data
on
patients
with
acute
coronary
angiography
following
cardiac
arrest
is
reported
from
the
study.
c
Unconscious
and
intubated.
d
ST-segment
elevation
but
not
left
LBBB
was
reported
in
study.
thrombolysis
and
acute
CAG
demonstrated
no
significant
difference
in
survival
at
six
months
(68%
vs
55%,
p
=
Two
studies
indicated
TH
to
be
feasible
in
STEMI
patients
undergo-
ing
acute
CAG
with
a
probable
positive
effect
on
good
neurological
3.3.
Studies
on
systematic
acute
coronary
angiography
in
selected
patients
with
out-of-hospital
cardiac
arrest
of
mixed
aetiology
illustrates
five
studies
on
systematic
acute
CAG
in
patients
following
ROSC
after
OHCA
without
an
obvious
non-
cardiac
aetiology.
reported
survival
ranged
from
31%
to
81%.
The
patient
characteristics
were
more
varied
compared
to
the
pure
STEMI
studies.
TH
was
used
in
the
majority
of
the
patients
in
the
two
largest
prevalence
of
significant
coro-
nary
artery
disease
(CAD)
was
high
ranging
from
59%
to
71%.
Angiographic
signs
comparable
to
acute
myocardial
infarction
with
recent
occlusion
or
irregular
lesions
varied
from
36%
to
69%.
ST-
segment
elevation
or
LBBB
was
seen
in
31–63%.
Shockable
rhythms
ranged
from
50%
to
93%.
The
pioneering
prospective
study
by
Spaulding
et
al.
included
84
patients
with
systematic
acute
CAG
following
OHCA
without
obvious
non-cardiac
aetiology.
positive
and
negative
pre-
dictive
values
for
recent
coronary
occlusion
on
angiography
of
chest
pain
and/or
ST-segment
elevation
were
63%
and
74%,
respec-
tively.
Survival
to
hospital
discharge
was
38%.
Successful
PCI
was
an
independent
predictor
of
survival
(adjusted
OR
5.2,
p
=
0.04).
The
largest
study
including
435
patients
from
a
prospective
reg-
istry
also
demonstrated
suboptimal
but
slightly
better
diagnostic
predictive
values
of
ST-segment
elevation,
and
successful
PCI
was
an
independent
predictor
of
survival
(adjusted
OR
2.1,
p
=
0.01).
Similar
suboptimal
diagnostic
values
of
ST-segment
elevation
for
identifying
angiographic
lesions
comparable
to
ACS
were
also
seen
in
two
retrospective
newest
of
these
stud-
ies
suggested
an
extended
ECG
criterion
of
ST-segment
elevation
and/or
depression
and/or
LBBB
and/or
unspecific
wide
QRS
and/or
right
bundle
branch
block.
extended
criterion
demonstrated
a
lower
positive
predictive
value
of
48%
but
a
negative
predic-
tive
value
of
100%
with
a
potential
to
reduce
the
needed
acute
procedures.
Table
4
Studies
including
patients
with
and
without
acute
coronary
angiography
following
cardiac
arrest.
Study
Inclusion
of
patients
N
OHCA
(%)
ST-segment
elevation
or
LBBB
(%)
Acute
CAG
(%)
PCI
(%)
VF/VT
(%)
Unconscious
(%)
TH
(%)
Survival
with
and
without
acute
CAG
Bulut
et
al.,
Netherlands
NA
72
100
NA
14
11
69
69
0
40
vs
37
p
=
1.00
Merchant
et
al.,
2000–2005
110
0
12
27
15
100
NA
NA
80
vs
54
p
=
0.02
Nielsen
et
al.,
2004–2008
986
100
NA
49
30
70
100
100
63
vs
50
p
<
0.001
Reynolds
et
2005–2007
241
56
19
26
NA
39
NA
33
52
vs
p
=
0.004
Aurore
et
al.,
2000–2006
445
100
28
30
16
42
NA
NA
23
vs
10
p
<
0.001
Cronier
et
2003–2008
111
100
54
82
42
100
NA
70
59
vs
30
p
=
0.02
Gräsner
et
2004–2010
584
100
NA
26
NA
42
NA
31
52
vs
p
<
0.001
Mooney
et
al.,
2006–2009
140
100
49
72
40
76
100
100
62
vs
38
p
=
0.01
Tömte
et
al.,
2003–2009
174
100
NA
83
45
49
78
NA
52
vs
p
=
0.04
Strote
et
al.,
1999–2002
240
100
34
25
16
98
NA
0
72
vs
49
p
=
0.003
Total
NA
3103
92
NA
41
NA
62
NA
NA
56
vs
32
(means)
p
<
0.001
N
=
number
of
patients;
OHCA
=
out-of-hospital
cardiac
arrest;
LBBB
=
left
bundle
branch
block;
CAG
=
coronary
angiography;
PCI
=
percutaneous
coronary
intervention;
VF/VT
=
ventricular
fibrillation
or
tachycardia;
TH
=
therapeutic
hypothermia;
NA
=
not
available.
a
Survival
to
hospital
discharge
unless
otherwise
stated
with
calculated
p-values
by
Fischer’s
exact
test
or
Chi-square
test.
b
Survival
to
hospital
discharge
with
good
neurology.
J.M.
Larsen,
J.
Ravkilde
/
Resuscitation
83 (2012) 1427–
1433
1431
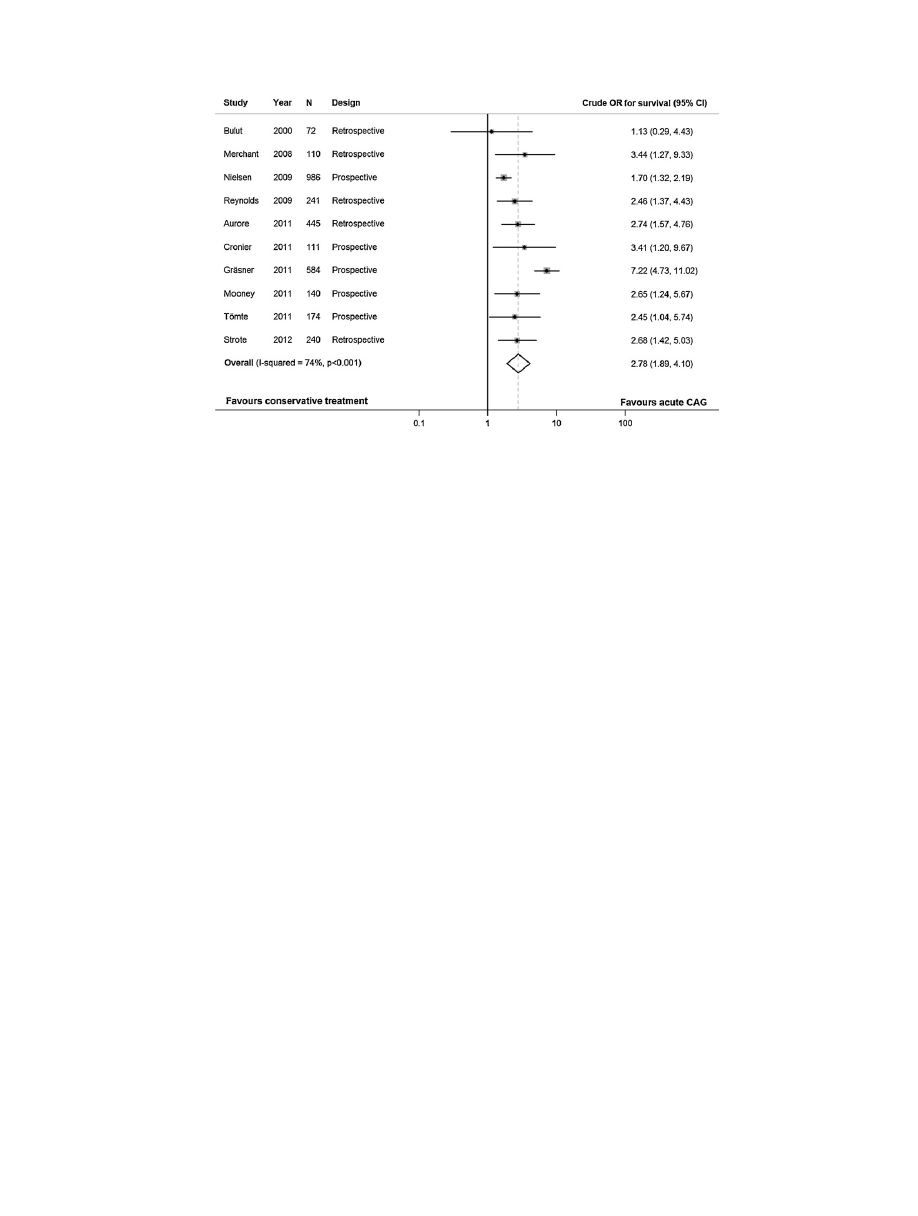
Fig.
2.
Forest
plot
from
a
meta-analysis
of
studies
including
patients
with
and
without
acute
coronary
angiography.
The
odds
ratios
are
unadjusted
for
possible
selection
bias
and
should
be
interpreted
with
caution.
The
grey
boxes
covering
the
point
estimate
of
the
odds
ratio
illustrate
the
weight
of
the
individual
study
in
the
pooled
odds
ratio.
These
weights
were
defined
by
a
random
effect
model
due
to
heterogeneity
of
the
studies
as
illustrated
by
a
high
I-squared.
N
=
number
of
patients;
OR
=
odds
ratio;
CI
=
confidence
interval;
CAG
=
coronary
angiography.
Two
small
studies
with
systematic
acute
CAG
following
OHCA
with
ventricular
fibrillation
were
not
included
in
to
more
selective
inclusion
criteria.
One
of
the
studies
included
15
patients
with
a
survival
to
hospital
discharge
of
73%.
other
study
included
50
comatose
haemodynamic
unstable
patients
and
demonstrated
an
impressive
six-month
survival
of
82%.
3.4.
Comparison
studies
including
patients
with
and
without
acute
coronary
angiography
10
studies
on
patients
resuscitated
from
car-
diac
arrest
of
mixed
aetiology
with
acute
CAG
only
performed
in
selected
indication
for
performing
acute
CAG
was
not
specified
in
most
of
the
studies.
The
use
of
acute
CAG
was
very
heterogeneous
in
the
studies
ranging
from
14%
to
83%.
Overall,
the
patients
undergoing
acute
CAG
had
a
better
survival.
The
character-
istics
of
patients
in
the
studies
were
heterogeneous,
e.g.
shockable
rhythms
ranged
from
39%
to
100%.
The
prevalence
of
comatose
sur-
vivors
was
only
sparsely
reported,
but
TH
was
generally
used
more
common
than
in
the
pure
STEMI-studies.
The
largest
study
prospectively
included
986
patients
resus-
citated
from
OHCA
at
38
centres
in
seven
countries
admitted
to
intensive
care
units
treated
with
percent
of
the
patients
presented
with
acute
myocardial
infarction,
but
only
49%
underwent
acute
CAG,
30%
PCI,
5%
thrombolytic
treatment
and
1%
coronary
artery
bypass
grafting.
Initial
shockable
rhythm
was
predictive
of
a
favourable
outcome
if
acute
CAG
was
performed
(p
<
0.001),
whereas
asystole
was
only
predictive
of
a
bad
outcome
if
acute
CAG
was
not
performed
(p
<
0.001).
Bleeding
requiring
trans-
fusion
was
more
common
in
patients
with
acute
CAG
(6.2%
vs
2.8%,
p
=
0.02).
In
three
other
studies,
acute
CAG
was
found
to
be
an
inde-
pendent
predictor
of
survival
with
adjusted
OR
of
3.8
(p
<
0.05),
5.7
(p
<
0.001)
and
11.2
(p
<
0.001),
study
only
demonstrated
a
significant
independent
predictive
value
on
sur-
vival
with
good
neurology
of
performing
CAG
before
discharge,
but
not
acute
CAG.
study
found
a
significant
independent
predictive
value
of
acute
PCI,
but
not
acute
CAG.
The
newest
and
only
LOE2
study
by
Strote
et
al.
included
240
resuscitated
OHCA
patients
and
compared
acute
CAG
(
≤6
h)
to
later
CAG
(>6
h)
or
no
CAG
before
was
performed
in
61%
with
acute
CAG,
which
more
often
had
ST-segment
elevation
and
pre-arrest
symptoms
indicating
ACS.
PCI
before
discharge
was
only
performed
in
7%
of
patients
without
acute
CAG.
The
crude
survival
to
hospital
discharge
was
better
in
patients
with
acute
CAG
(72%
vs
49%,
p
=
0.003).
To
address
possible
selection
bias,
matching
with
propensity
score
analysis
was
done
indicating
a
survival
benefit
of
acute
CAG
in
the
patients
with
propensity
scores
with
middle
to
high
likelihood
of
undergoing
acute
CAG.
No
multivariate
analysis
of
the
prognostic
effect
of
acute
CAG
including
the
propensity
score
was
reported
in
the
study.
The
crude
prognostic
information
from
the
ten
studies
was
com-
piled
in
a
meta-analysis
as
illustrated
in
the
forest
plot
in
studies,
except
the
smallest
and
oldest,
had
a
significant
unadjusted
OR
for
survival
favouring
acute
CAG.
The
pooled
unadjusted
OR
was
2.78,
95%
confidence
interval
(1.89;
4.10).
The
high
I-squared
illustrates
heterogeneity
in
the
studies.
4.
Discussion
The
high
rate
of
mortality
associated
with
OHCA
calls
for
opti-
mised
treatment
both
before
and
after
ROSC.
No
randomised
trials
exist
evaluating
the
use
of
acute
CAG
following
successful
resusci-
tation
from
OHCA
(
4.1.
Acute
coronary
angiography
in
ST-segment
elevation
myocardial
infarction
following
resuscitation
from
out-of-hospital
cardiac
arrest
Acute
CAG
with
subsequent
PCI
compared
to
fibrinolysis
in
STEMI
patients
without
preceding
cardiac
arrest
is
favourable
for
survival
and
morbidity,
when
the
transfer
time
to
a
PCI
cen-
tre
is
short.
arrest
survivors
are
frequently
excluded
from
randomised
studies
because
of
unconsciousness
and
unsta-
ble
circulation
due
to
post-cardiac
arrest
syndrome
and
potential
irreversible
brain
optimal
management
of
espe-
cially
the
comatose
survivors
of
OHCA
with
a
proper
balance
between
action
and
withdrawal
of
treatment
is
very
challenging
both
for
the
interventional
cardiologist
and
the
intensivist.
The

1432
J.M.
Larsen,
J.
Ravkilde
/
Resuscitation
83 (2012) 1427–
1433
recommendation
in
the
2010
CoSTR
and
2010
European
guide-
lines
for
resuscitation
is
that
acute
CAG
should
be
considered
in
resuscitated
OHCA
patients
with
ST-segment
elevation
or
new
case
series
on
selected
resuscitated
patients
with
ST-segment
elevation
or
new
LBBB
demonstrate
acute
CAG
to
be
feasible
and
with
a
relatively
good
survival
(
The
studies
have
poor
evidence
levels
most
often
including
patients
with
wit-
nessed
arrests
and
shockable
rhythms.
This
selection
of
patients
probably
results
in
overoptimistic
survival
rates,
but
the
studies
do
demonstrate
that
acute
CAG
with
coronary
intervention
indeed
is
feasible
in
the
post
cardiac
arrest
setting.
A
small
retrospective
study
comparing
acute
fibrinolysis
and
acute
CAG
following
OHCA
demonstrated
no
significant
difference
in
survival,
but
actually
a
non-significant
trend
favouring
fibri-
nolysis
probably
due
to
time
delay
before
start
of
the
invasive
delay
can
also
explain
poorer
left
ventricu-
lar
ejection
fraction
in
patients
transfer
from
referral
hospital
compared
to
direct
admittance
to
a
PCI
centre
for
acute
CAG
fol-
lowing
emphasises
the
need
for
speed
in
treatment
of
patients
with
an
acute
coronary
occlusion.
If
transfer
to
a
PCI
centre
is
not
possible
in
a
reasonable
time,
an
alternative
reperfusion
strat-
egy
with
acute
fibrinolysis
should
still
be
considered
in
resuscitated
patients
with
STEMI
despite
preceding
chest
compressions.
4.2.
Acute
coronary
angiography
in
patients
following
resuscitation
from
out-of-hospital
cardiac
arrest
The
2010
CoSTR
and
European
guidelines
on
resuscitation
rec-
ommend
acute
CAG
to
be
considered
in
selected
resuscitated
OHCA
patients
irrespective
of
ECG
findings,
if
coronary
ischaemia
is
suspected
to
be
the
aetiology
for
cardiac
arrest,
and
it
may
be
rea-
sonable
to
include
acute
CAG
as
part
of
a
standardised
post-cardiac
arrest
recommendation
is
based
on
observational
studies
with
poor
evidence
levels.
In
our
review,
we
identified
sev-
eral
mainly
newer
but
still
low
evidence
level
studies
on
patients
with
cardiac
arrest
of
mixed
aetiology
not
evaluated
in
the
2010
CoSTR,
adding
further
evidence
on
the
topic.
Systematic
acute
CAG
in
patient
without
an
obvious
non-cardiac
aetiology
has
demonstrated
a
high
prevalence
of
significant
CAD
and
a
favourable
survival
(
Studies
with
systematic
acute
CAG
in
patients
resuscitated
from
OHCA
with
shockable
rhythms
also
demonstrate
very
high
survival
studies
have
examined
the
diagnostic
properties
of
ST-segment
elevation
fol-
lowing
OHCA
compared
to
angiographic
findings
with
variable
results.
In
general,
the
diagnostic
values
were
suboptimal,
espe-
cially
the
negative
predictive
one
study,
the
negative
predictive
value
was
increased
to
100%
on
behalf
of
a
much
poorer
positive
predictive
value
by
using
an
extended
ECG
criterion
for
triage
with
ST-segment
elevation
and/or
depression
and/or
LBBB
and/or
unspecific
wide
QRS
and/or
right
bundle
branch
However,
the
author
is
cautious
to
recommend
implementation
of
this
strategy
for
triage
before
completion
of
prospective
studies,
as
it
is
well
known
that
the
ECG
can
be
without
ischaemic
findings
despite
an
acute
occlusion
in
patients
without
preceding
cardiac
arrest.
Our
meta-analysis
comparing
patients
with
and
without
acute
CAG
in
populations
with
mixed
aetiology
to
the
cardiac
arrest
demonstrated
a
significant
crude
positive
association
between
acute
CAG
and
survival.
Unfortunately,
no
data
is
available
for
an
adjusted
analysis
to
control
for
selection
bias
Therefore,
the
pooled
OR
in
the
meta-analysis
should
be
inter-
preted
with
caution.
The
risk
of
selection
bias
is
emphasised
by
the
only
LOE2
study
in
which
age,
bystander
cardiopulmonary
resus-
citation,
daytime
presentation,
history
of
PCI
or
stroke
and
acute
ST-segment
elevation
in
ECG
were
positively
associated
to
receiv-
ing
an
acute
CAG.
study
did
however
indicate
a
survival
benefit
of
acute
CAG
when
adjusting
for
selection
bias
by
propensity
score
analysis.
Six
other
studies
of
our
review
also
demonstrated
significant
adjusted
odds
ratios
in
favour
of
either
acute
CAG
or
acute
The
poor
diagnostic
properties
of
the
ECG
in
resuscitated
OHCA
patients
with
a
high
prevalence
of
CAD
emphasises
the
routine
use
of
systematic
acute
CAG
as
part
of
a
standard
post-cardiac-arrest
protocol.
The
use
of
routine
acute
CAG
in
conscious
survivors
is
not
very
controversial
as
most
interventional
cardiologists
will
con-
sider
this
as
high
risk
acute
coronary
syndrome.
Routine
acute
CAG
in
comatose
survivors
is
more
debatable
due
to
the
poor
evidence,
possible
irreversible
brain
injury
and
an
inherent
slightly
higher
risk
of
bleeding
complications
with
concurrent
TH.
the
studies
in
our
review
exclusively
including
comatose
survivors
mainly
treated
with
TH
and
acute
CAG
with
coronary
intervention
did
show
relatively
good
survival
recommend
future
randomised
studies
including
comatose
survivors
of
OHCA
without
STEMI
or
new
LBBB
undergoing
TH.
This
will
be
clinical
feasible
and
of
importance
both
for
the
intensive
care
and
inter-
ventional
cardiology
communities.
5.
Limitations
The
search
strategy
only
included
three
databases.
Non-English
articles
were
excluded.
Relevant
articles
could
be
missing
in
the
review,
but
this
is
less
likely
as
the
reference
lists
of
the
included
articles
and
the
2010
CoSTR
were
screened.
The
classification
of
the
studies
as
supporting,
neutral
and
opposing
PICO
is
debat-
able.
We
have
used
a
more
conservative
approach
than
in
the
2010
CoSTR
evaluation
process
by
only
allowing
studies
to
be
classified
as
supporting
if
adjusted
statistical
evidence
was
present
in
order
to
reduce
confounding.
The
definition
of
acute
CAG
differed
between
the
studies
from
less
than
6
h
up
to
less
than
24
h.
This
contributes
to
the
heterogeneity
of
the
reported
prognosis
in
the
studies.
It
would
have
been
clinically
relevant
to
make
a
separate
more
thorough
prognostic
analysis
of
conscious
and
comatose
survivors,
as
their
prognosis
differ.
This
was
not
feasible
with
the
available
data.
The
meta-analysis
was
based
on
prognostic
data
from
heterogeneous
studies.
This
was
evident
by
the
high
I-squared
value.
A
pooled
OR
seemed
fair
as
the
individual
odds
ratios
all
were
pointing
in
the
same
direction.
A
random
effect
model
was
used
due
to
the
hetero-
geneity.
The
meta-analysis
was
not
adjusted
for
possible
selection
bias
as
the
necessary
data
was
not
available.
Therefore,
the
meta-
analysis
should
be
interpreted
with
caution,
but
several
individual
studies
with
adjusted
analysis
do
support
the
use
of
acute
CAG
in
the
post
cardiac
arrest
setting.
6.
Conclusions
No
randomised
studies
exist
on
acute
CAG
following
OHCA.
An
increasing
number
of
observational
studies
support
feasibility
and
a
possible
survival
benefit
of
an
early
invasive
approach.
Acute
CAG
is
associated
to
a
better
survival
in
studies
on
resuscitated
patients
with
heterogeneous
aetiology
to
OHCA.
Systematic
acute
CAG
fol-
lowing
OHCA
without
an
obvious
non-cardiac
aetiology
should
be
strongly
considered
irrespective
of
electrocardiographic
findings
due
to
a
high
prevalence
of
CAD
and
unreliable
diagnostic
proper-
ties
of
the
electrocardiographic
findings.
Randomised
multicentre
studies
with
acute
CAG
following
OHCA
are
warranted
especially
in
comatose
survivors
for
optimising
the
diagnostic
and
therapeutic
strategy.
Conflict
of
interest
statement
None.

J.M.
Larsen,
J.
Ravkilde
/
Resuscitation
83 (2012) 1427–
1433
1433
Acknowledgements
The
authors
thank
chief
librarian
Conni
Skrubbeltrang
and
librarian
assistant
Jacob
Borg
Andersen
from
the
Medical
Library
at
Aalborg
University
Hospital
for
valuable
help
on
performing
the
database
search.
We
thank
research
secretary
Hanne
Madsen
from
the
Department
of
Cardiology
at
Aalborg
University
Hospital
for
assisting
in
the
final
preparation
of
the
manuscript.
Funding:
No
external
funding
was
used
in
the
preparation
of
the
manuscript.
References
1. Atwood
C,
Eisenberg
MS,
Herlitz
J,
Rea
TD.
Incidence
of
EMS-treated
out-of-
hospital
cardiac
arrest
in
Europe.
Resuscitation
2005;67:75–80.
2. Davies
MJ.
Anatomic
features
in
victims
of
sudden
coronary
death.
Coronary
artery
pathology.
Circulation
1992;85:19–24.
3.
Van
de
Werf
F,
Bax
J,
Betriu
A,
et
al.
Management
of
acute
myocardial
infarction
in
patients
presenting
with
persistent
ST-segment
elevation:
the
task
force
on
the
management
of
ST-segment
elevation
acute
myocardial
infarction
of
the
European
Society
of
Cardiology.
Eur
Heart
J
2008;29:2909–45.
4.
Bossaert
L,
O’Connor
RE,
Arntz
HR,
et
al.
Part
9:
acute
coronary
syndromes:
2010
International
Consensus
on
Cardiopulmonary
Resuscitation
and
Emergency
Cardiovascular
Care
Science
with
Treatment
Recommendations.
Resuscitation
2010;81(Suppl.
1):175–212.
5.
Stroup
DF,
Berlin
JA,
Morton
SC,
et
al.
Meta-analysis
of
observational
studies
in
epidemiology:
a
proposal
for
reporting.
Meta-analysis
Of
Observational
Studies
in
Epidemiology
(MOOSE)
group.
JAMA
2000;283:2008–12.
6.
Moher
D,
Liberati
A,
Tetzlaff
J,
Altman
DG.
Preferred
reporting
items
for
sys-
tematic
reviews
and
meta-analyses:
the
PRISMA
statement.
J
Clin
Epidemiol
2009;62:1006–12.
7.
Morley
PT,
Atkins
DL,
Billi
JE,
et
al.
Part
3:
evidence
evaluation
process:
2010
International
Consensus
on
Cardiopulmonary
Resuscitation
and
Emergency
Cardiovascular
Care
Science
with
Treatment
Recommendations.
Resuscitation
2010;81(Suppl.
1):32–40.
8. Kahn
JK,
Glazier
S,
Swor
R,
Savas
V,
O’Neill
WW.
Primary
coronary
angioplasty
for
acute
myocardial
infarction
complicated
by
out-of-hospital
cardiac
arrest.
Am
J
Cardiol
1995;75:1069–70.
9.
McCullough
PA,
Prakash
R,
Tobin
KJ,
O’Neill
WW,
Thompson
RJ.
Application
of
a
cardiac
arrest
score
in
patients
with
sudden
death
and
ST
segment
elevation
for
triage
to
angiography
and
intervention.
J
Intervent
Cardiol
2002;15:257–61.
10.
Bendz
B,
Eritsland
J,
Nakstad
AR,
et
al.
Long-term
prognosis
after
out-of-hospital
cardiac
arrest
and
primary
percutaneous
coronary
intervention.
Resuscitation
2004;63:49–53.
11. Quintero-Moran
B,
Moreno
R,
Villarreal
S,
et
al.
Percutaneous
coronary
inter-
vention
for
cardiac
arrest
secondary
to
ST-elevation
acute
myocardial
infarction.
Influence
of
immediate
paramedical/medical
assistance
on
clinical
outcome.
J
Invasive
Cardiol
2006;18:269–72.
12. Markusohn
E,
Roguin
A,
Sebbag
A,
et
al.
Primary
percutaneous
coronary
inter-
vention
after
out-of-hospital
cardiac
arrest:
patients
and
outcomes.
Isr
Med
Assoc
J
2007;9:257–9.
13. Garot
P,
Lefevre
T,
Eltchaninoff
H,
et
al.
Six-month
outcome
of
emer-
gency
percutaneous
coronary
intervention
in
resuscitated
patients
after
cardiac
arrest
complicating
ST-elevation
myocardial
infarction.
Circulation
2007;115:1354–62.
14.
Knafelj
R,
Radsel
P,
Ploj
T,
Noc
M.
Primary
percutaneous
coronary
intervention
and
mild
induced
hypothermia
in
comatose
survivors
of
ventricular
fibrillation
with
ST-elevation
acute
myocardial
infarction.
Resuscitation
2007;74:227–34.
15.
Richling
N,
Herkner
H,
Holzer
M,
Riedmueller
E,
Sterz
F,
Schreiber
W.
Thrombolytic
therapy
vs
primary
percutaneous
intervention
after
ventricular
fibrillation
cardiac
arrest
due
to
acute
ST-segment
elevation
myocardial
infarc-
tion
and
its
effect
on
F
outcome.
Am
J
Emerg
Med
2007;25:545–50.
16.
Pleskot
M,
Babu
A,
Hazukova
R,
et
al.
Out-of-hospital
cardiac
arrests
in
patients
with
acute
ST
elevation
myocardial
infarctions
in
the
East
Bohemian
region
over
the
period
2002–2004.
Cardiology
2008;109:41–51.
17.
Peels
HO,
Jessurun
GA,
van
der
Horst
IC,
Arnold
AE,
Piers
LH,
Zijlstra
F.
Outcome
in
transferred
and
nontransferred
patients
after
primary
percutaneous
coronary
intervention
for
ischaemic
out-of-hospital
cardiac
arrest.
Catheter
Cardiovasc
Interv
2008;71:147–51.
18.
Mager
A,
Kornowski
R,
Murninkas
D,
et
al.
Outcome
of
emergency
percutaneous
coronary
intervention
for
acute
ST-elevation
myocardial
infarction
complicated
by
cardiac
arrest.
Coron
Artery
Dis
2008;19:615–8.
19.
Wolfrum
S,
Pierau
C,
Radke
PW,
Schunkert
H,
Kurowski
V.
Mild
therapeutic
hypothermia
in
patients
after
out-of-hospital
cardiac
arrest
due
to
acute
ST-
segment
elevation
myocardial
infarction
undergoing
immediate
percutaneous
coronary
intervention.
Crit
Care
Med
2008;36:1780–6.
20.
Lettieri
C,
Savonitto
S,
De
Servi
S,
et
al.
Emergency
percutaneous
coronary
inter-
vention
in
patients
with
ST-elevation
myocardial
infarction
complicated
by
out-of-hospital
cardiac
arrest:
early
and
medium-term
outcome.
Am
Heart
J
2009;157:569–75.
21.
Szymanski
FM,
Grabowski
M,
Karpinski
G,
Hrynkiewicz
A,
Filipiak
KJ,
Opolski
G.
Does
time
delay
between
the
primary
cardiac
arrest
and
PCI
affect
outcome?
Acta
Cardiol
2009;64:633–7.
22. Hosmane
VR,
Mustafa
NG,
Reddy
VK,
et
al.
Survival
and
neurologic
recovery
in
patients
with
ST-segment
elevation
myocardial
infarction
resuscitated
from
cardiac
arrest.
J
Am
Coll
Cardiol
2009;53:409–15.
23.
Spaulding
CM,
Joly
L,
Rosenberg
A,
et
al.
Immediate
coronary
angiography
in
survivors
of
out-of-hospital
cardiac
arrest.
N
Engl
J
Med
1997;336:1629–33.
24.
Anyfantakis
ZA,
Baron
G,
Aubry
P,
et
al.
Acute
coronary
angiographic
findings
in
survivors
of
out-of-hospital
cardiac
arrest.
Am
Heart
J
2009;157:312–8.
25.
Dumas
F,
Cariou
A,
Manzo-Silberman
S,
et
al.
Immediate
percutaneous
coro-
nary
intervention
is
associated
with
better
survival
after
out-of-hospital
cardiac
arrest:
insights
from
the
PROCAT
(Parisian
Region
Out
of
Hospital
Cardiac
Arrest)
registry.
Circ
Cardiovasc
Interv
2010;3:200–7.
26.
Sideris
G,
Voicu
S,
Dillinger
JG,
et
al.
Value
of
post-resuscitation
electrocardio-
gram
in
the
diagnosis
of
acute
myocardial
infarction
in
out-of-hospital
cardiac
arrest
patients.
Resuscitation
2011;82:1148–53.
27.
Mollmann
H,
Szardien
S,
Liebetrau
C,
et
al.
Clinical
outcome
of
patients
treated
with
an
early
invasive
strategy
after
out-of-hospital
cardiac
arrest.
J
Int
Med
Res
2011;39:2169–77.
28.
Keelan
PC,
Bunch
TJ,
White
RD,
Packer
DL,
Holmes
DR.
Early
direct
coro-
nary
angioplasty
in
survivors
of
out-of-hospital
cardiac
arrest.
Am
J
Cardiol
2003;91:1461–3.
29. Hovdenes
J,
Laake
JH,
Aaberge
L,
Haugaa
H,
Bugge
JF.
Therapeutic
hypother-
mia
after
out-of-hospital
cardiac
arrest:
experiences
with
patients
treated
with
percutaneous
coronary
intervention
and
cardiogenic
shock.
Acta
Anaesthesiol
Scand
2007;51:137–42.
30. Bulut
S,
Aengevaeren
WRM,
Luijten
HJE,
Verheugt
FWA.
Successful
out-
of-hospital
cardiopulmonary
resuscitation:
What
is
the
optimal
in-hospital
treatment
strategy?
Resuscitation
2000;47:155–61.
31.
Merchant
RM,
Abella
BS,
Khan
M,
et
al.
Cardiac
catheterization
is
underutilized
after
in-hospital
cardiac
arrest.
Resuscitation
2008;79:398–403.
32.
Nielsen
N,
Hovdenes
J,
Nilsson
F,
et
al.
Outcome,
timing
and
adverse
events
in
therapeutic
hypothermia
after
out-of-hospital
cardiac
arrest.
Acta
Anaesthesiol
Scand
2009;53:926–34.
33. Reynolds
JC,
Callaway
CW,
El
Khoudary
SR,
Moore
CG,
Alvarez
RJ,
Rittenberger
JC.
Coronary
angiography
predicts
improved
outcome
following
cardiac
arrest:
propensity-adjusted
analysis.
J
Intensive
Care
Med
2009;24:179–86.
34.
Aurore
A,
Jabre
P,
Liot
P,
Margenet
A,
Lecarpentier
E,
Combes
X.
Predictive
factors
for
positive
coronary
angiography
in
out-of-hospital
cardiac
arrest
patients.
Eur
J
Emerg
Med
2011;18:73–6.
35.
Cronier
P,
Vignon
P,
Bouferrache
K,
et
al.
Impact
of
routine
percutaneous
coronary
intervention
after
out-of-hospital
cardiac
arrest
due
to
ventricular
fibrillation.
Crit
Care
2011;15:R122.
36. Grasner
JT,
Meybohm
P,
Caliebe
A,
et
al.
Postresuscitation
care
with
mild
therapeutic
hypothermia
and
coronary
intervention
after
out-of-hospital
cardiopulmonary
resuscitation:
a
prospective
registry
analysis.
Crit
Care
2011;15:R61.
37.
Mooney
MR,
Unger
BT,
Boland
LL,
et
al.
Therapeutic
hypothermia
after
out-of-
hospital
cardiac
arrest:
evaluation
of
a
regional
system
to
increase
access
to
cooling.
Circulation
2011;124:206–14.
38.
Tomte
O,
Andersen
GO,
Jacobsen
D,
Draegni
T,
Auestad
B,
Sunde
K.
Strong
and
weak
aspects
of
an
established
post-resuscitation
treatment
protocol—a
five-
year
observational
study.
Resuscitation
2011;82:1186–93.
39.
Strote
JA,
Maynard
C,
Olsufka
M,
et
al.
Comparison
of
role
of
early
(less
than
six
hours)
to
later
(more
than
six
hours)
or
no
cardiac
catheterization
after
resuscitation
from
out-of-hospital
cardiac
arrest.
Am
J
Cardiol
2012;109:
451–4.
40.
Andersen
HR,
Nielsen
TT,
Rasmussen
K,
et
al.
A
comparison
of
coronary
angio-
plasty
with
fibrinolytic
therapy
in
acute
myocardial
infarction.
N
Engl
J
Med
2003;349:733–42.
41.
Nolan
JP,
Neumar
RW,
Adrie
C,
et
al.
Post-cardiac
arrest
syndrome:
epi-
demiology,
pathophysiology,
treatment,
and
prognostication.
Resuscitation
2008;79:350–79.
42.
Arntz
HR,
Bossaert
LL,
Danchin
N,
Nikolaou
NI.
European
Resuscitation
Coun-
cil
Guidelines
for
Resuscitation
2010
Section
5.
Initial
management
of
acute
coronary
syndromes.
Resuscitation
2010;81:1353–63.
Document Outline
- Acute coronary angiography in patients resuscitated from out-of-hospital cardiac arrest—A systematic review and meta-analysis
- 1 Introduction
- 2 Methods
- 3 Results
- 3.1 Eligible studies
- 3.2 Studies on acute coronary angiography in ST-segment elevation myocardial infarction
- 3.3 Studies on systematic acute coronary angiography in selected patients with out-of-hospital cardiac arrest of mixed aet...
- 3.4 Comparison studies including patients with and without acute coronary angiography
- 4 Discussion
- 5 Limitations
- 6 Conclusions
- Conflict of interest statement
- Acknowledgements
- References
Wyszukiwarka
Podobne podstrony:
Acute Coronary Thrombosis in Boston Marathon Runners
Konstatinos A Land versus water exercise in patients with coronary
Effects of Clopidogrel?ded to Aspirin in Patients with Recent Lacunar Stroke
Cementless Ceramic Hip Arthroplasties in Patients Less Than 30 Years Old
Difficult airway management in a patient with traumatic asphyxia
ACUTE ABDOMEN DISORDERS IN PREGNANCY MAT DOD
Impaired Sexual Function in Patients with BPD is Determined by History of Sexual Abuse
A Ser49Cys Variant in the Ataxia Telangiectasia, Mutated, Gene that Is More Common in Patients with
Muscle Mass Gain Observed in Patients with Short Bowel Syndrome
Difficult airway management in a patient with traumatic asphyxia
Proton Magnetic Resonance Spectroscopy of the Medial Prefrontal Cortex in Patients With Deficit Schi
Serum cytokine levels in patients with chronic low back pain due to herniated disc
The Effects of Probiotic Supplementation on Markers of Blood Lipids, and Blood Pressure in Patients
Rapid Blood Pressure Lowering in Patients
Personality Constellations in Patients With a History of Childhood Sexual Abuse
Effect of high dose intravenous ascorbic acid on the level of inflammation in patients with rheumato
The relationship of Lumbar Flexion to disability in patients with low back pain
Continuous mechanical chest compression during in hospital cardiopulmonary resuscitation of patients
więcej podobnych podstron