METHOD OF SHIPPING
Personal pick-up
CP stock
Courier service
METHOD OF PAYMENT
Cash/Check
Credit / Debit card
DELIVER TO
First name:
…………………………………………………………….............………….……………………………….…………
Last name:
……………................…........................................................................................................
Date of birth:
....................................................................……….
E-mail:
............................................................................................................................................................................................................................................……………………………….
Telephone:
……………………………….……………………………….………………………………………………….……………...
Address:
……………………………….…………..................…………………….…………………………………......................……....………………………....................................................................................................................................................................…………………………................................……………………………….
City:
……………………………….…………..................…………………….…………………………………......…......................................................
State:
....................................................................………………………................................….........…..……………….
ZIP code:
…………................……......…..................
Sponsoring person’s name:
..............................................................................................................................................................................................................................................……………………………….
ID number:
…………...............................…………….……………...
BILL TO (if different from delivery address)
Company name:
………………………………………………………………………............………………….……………………………….……….............................................................................
EIN:
.................................................................................................................................................................................
Address:
……………………………….…………..................…………………….…………………………………......................……....………………………....................................................................................................................................................................…………………………................................……………………………….
City:
……………………………….…………..................…………………….…………………………………......…......................................................
State:
....................................................................………………………................................….........…..……………….
ZIP code:
…………................……......…..................
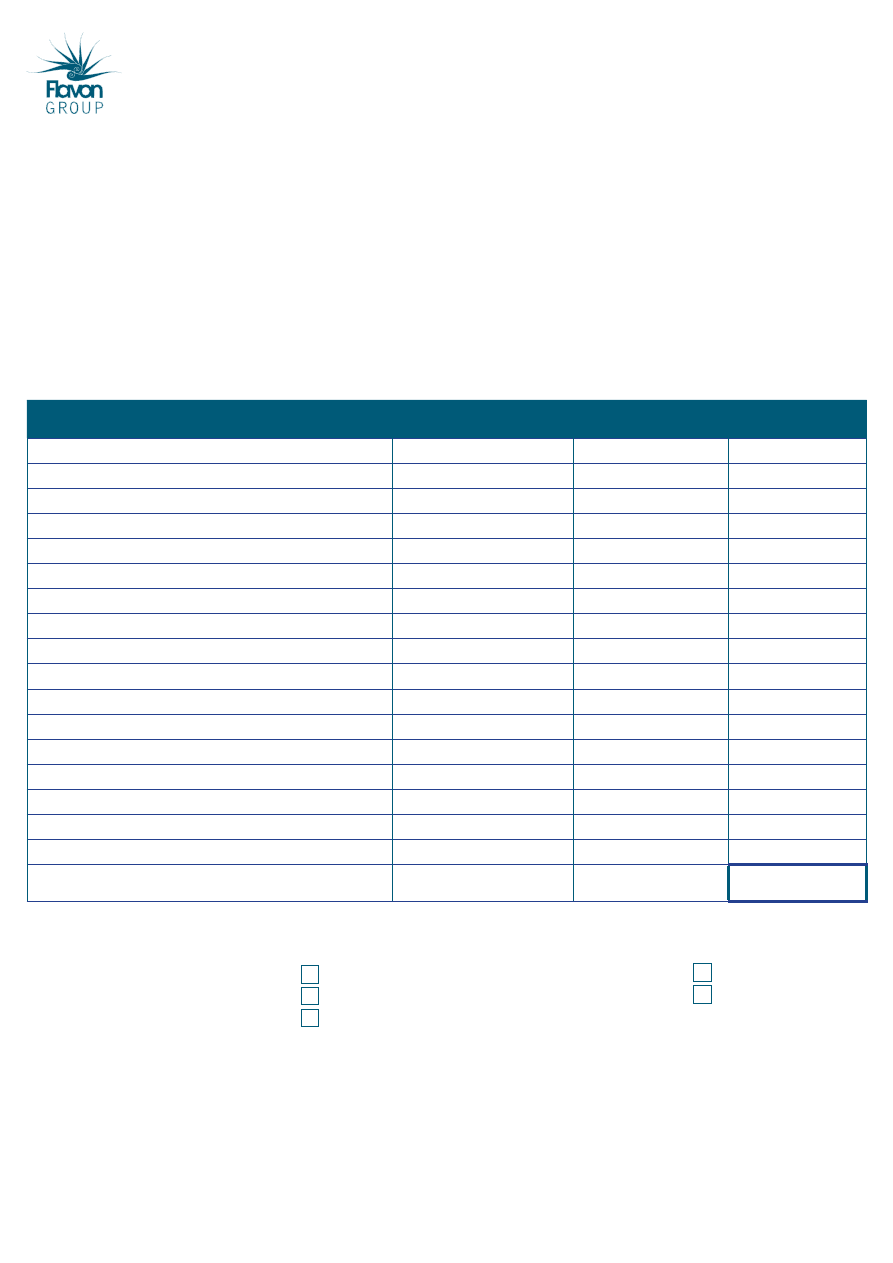
PRODUCT
Unit price
(excluding taxes)
Quantity
Total (USD)
Flavon max (4 jars)
$180.00
Flavon max (1 jar)
$45.00
Flavon Kids (4 jars)
$180.00
Flavon Kids (1 jar)
$45.00
Flavon max Plus+ (3 jars)
$180.00
Flavon Green (4 jars)
$180.00
Flavon Green (1 jar)
$45.00
Flavon Active (4 jars)
$180.00
Flavon Active (1 jar)
$45.00
Flavon Protect (4 jars)
$180.00
Flavon Protect (1 jar)
$45.00
Marketing (business) brochure
$0.25
Product brochure
$0.25
Introduction to flavonoids
$1.00
International handbook
$5.50
Shipping cost*
Purchase discount
TOTAL
* depends on weight and delivery address
__________________________________________________________
Signature
The provided data will be used only to fulfill orders, managed confidentially. These data will not be given to a third, unauthorized person.
For more information or to order, please call toll-free 855-352-8668
Please send this form signed and filled to one of the following addresses:
FLAVON USA LLC, 1370 N. US 1, SUITE 206, ORMOND BEACH, FL 32174
florida@flavongroup.com
Product Order Form
ID number:
…………………....…………….……………………….
(provided by Flavon Group)
Wyszukiwarka
Podobne podstrony:
Product order US 20120611
Product order US 20120611
US Patent 568,177 Apparatus For Producing Ozone
US Patent 577,670 Apparatus For Producing Electric Currents Of High Frequency
US Patent 568,179 Method Of And Apparatus For Producing Currents Of High Frequency
US Patent 583,953 Apparatus For Producing Currents Of High Frequency
US Patent 568,180 Apparatus For Producing Electrical Currents Of High Frequency
Product presentation XC100FC
~$Production Of Speech Part 2
Product presentation easyControl
Wykład nr 5 podstawy decyzji producenta
Us ugi internetu dla LTK i SRK
Transfer sk adki US
Manual Acer TravelMate 2430 US EN
AD Order Of Battle
Overview of Exploration and Production
Ek w 5, Producent, 25mar11 [t Nieznany
CM 52 ProductDefinition oct2011
więcej podobnych podstron