The relationship of depressive symptoms to symptom reporting,
self-care and glucose control in diabetes
Paul S. Ciechanowski, M.D.,MPH
a,
*, Wayne J. Katon, M.D.
a
, Joan E. Russo, Ph.D
a
,
Irl B. Hirsch, M.D.
b
a
Department of Psychiatry and Behavioral Sciences, University of Washington, Seatlle, WA 98195, USA
b
Department of Medicine, University of Washington, Seattle, WA, USA
Abstract
Depressive symptoms are common among patients with diabetes and may have a significant impact on self-management and health
outcomes. In this study we predicted that: 1) there would be a significant association between depressive symptoms and diabetes symptom
burden, physical functioning, diabetes self-care, and HbA1c levels; and, 2) that the association between depressive symptoms and HbA1c
levels would be significantly greater in type 1, as compared to type 2 diabetic patients. This cross-sectional observational study of 276 type
1 and 199 type 2 diabetes patients took place in a tertiary care specialty clinic. We collected self-reported data on depressive symptoms,
complications, medical comorbidity, diabetes symptoms, diabetes self-care behaviors, physical functioning, and demographics. From
automated data we determined mean HbA1c levels over the prior year. We performed linear regression analyses to assess the association
between depressive symptoms and diabetes symptom perception, diabetes self-care behaviors, physical functioning, and glycemic control.
Among patients with type 1 and 2 diabetes, depressive symptoms were associated with greater diabetes symptom reporting, poorer physical
functioning, and less adherence to exercise regimens and diet. There was a significant association between depressive symptoms and HbA1c
levels in type 1, but not type 2 diabetic patients. Because of their association with clinical aspects of diabetes care such as diabetes symptom
reporting and adherence to diabetes self-care, depressive symptoms are important to recognize in treating patients with diabetes. © 2003
Elsevier Inc. All rights reserved.
Keywords: Depression; Diabetes; Diabetes symptoms; Self-care; Glucose control
1. Introduction
A recent meta-analysis has shown that among patients
with diabetes, the prevalence of major depression and sig-
nificant depressive symptoms was 11% and 31%, respec-
tively [1]. The presence of comorbid depressive symptoms
can have a significant impact on health outcomes, health
care utilization, and overall functioning in patients with
diabetes [2,3]. In a recent study of predominantly type 2
primary care diabetes patients (N
⫽367), we found that de-
pressive symptoms were associated with significantly
poorer physical and mental functioning, decreased adher-
ence to dietary recommendations, less adherence to oral
hypoglycemic medications, higher health care costs and
nonsignificant increases in HbA1c levels [4].
While a number of cross-sectional studies have shown
that depression is significantly associated with hyperglyce-
mia in type 2 diabetic patients, as many studies have found
that this association is not significant [5]. When examined
meta-analytically, the association between poorer glucose
control and depression has been found to be more signifi-
cant in type 1 as compared to type 2 diabetic patients across
studies, particularly when standardized interviews were
used (Effect Size 0.28 vs. 0.15) [5]. A recent cross-sectional
study also found the correlation between Beck Depression
Inventory scores and HbA1c levels in type 1 diabetic pa-
tients was moderately high (r
⫽.44) as compared to that in
type 2 diabetic patients (r
⫽⫺.06) [6]. A number of differ-
ences in type 1 and 2 diabetes – such as different etiologies,
age of onset and treatment regimens – may lead to different
mechanisms operating to cause hyperglycemia in depressed
type 1 and 2 diabetic patients. In type 1 diabetes, patients
develop complete insulin deficiency due to an autoimmune
destruction of the beta cells of the pancreas. In type 2
* Corresponding author. Tel.:
⫹1-206-543-8848; fax: ⫹1-206-221-
5414.
E-mail address: pavelcie@u.washington.edu (P. Cliechanowski).
General Hospital Psychiatry 25 (2003) 246 –252
0163-8343/03/$ – see front matter © 2003 Elsevier Inc. All rights reserved.
doi:10.1016/S0163-8343(03)00055-0

diabetes there is a relative lack of insulin based in part on
resistance to this hormone at both the liver and the muscle.
The complete insulin deficiency in type 1 diabetes may
result in greater lability in glycemic control in response to
behavioral or neuro-hormonal effects of depression, than
may be the case in type 2 diabetes. There is also typically
more treatment heterogeneity in type 2 patients who may be
treated with diet and exercise only, oral hypoglycemics,
insulin or a combination of these. The main – and essential
– treatment in type 1 diabetes is insulin, though diet and
exercise also play an important secondary role in achieving
glucose control. Such differences in diabetes treatment may
result in differential treatment outcomes given changes in
self-care behavior resulting from depression. For example,
in a type 2 diabetic patient treated with diet only, lack of
treatment adherence is not likely to cause as significant an
increase in glucose levels as lack of adherence to an insulin
regimen in a type 1 diabetic patient.
Another important feature of the coexistence of diabetes
and depression is the increased potential for symptom re-
porting among depressed diabetic patients. While there is
overlap of symptoms associated with both disorders (e.g.,
fatigue, hyperphagia), depression is known to cause non-
specific symptom amplification in patients with chronic
medical illnesses [7]. Thus, patients with depression may
have a lower threshold in reporting all physical symptoms
including common diabetes symptoms such as thirst, poly-
uria, and blurry vision. This tendency to amplify physical
symptoms may result in higher health care use and in-
creased laboratory testing by providers [8].
In the current study, we assessed the impact of depres-
sive symptoms on patients with diabetes in a tertiary care
university-based clinic. We sought to determine if diabetes
self-care behaviors, physical functioning, diabetes symptom
reporting and glucose control correlated significantly with
depressive symptoms in both type 1 and 2 diabetes. We
hypothesized that higher levels of depression would be
significantly associated with greater diabetes symptom re-
porting, lower diabetes self-care, lower physical functioning
in both type 1 and 2 diabetes, and we predicted that there
would be effect modification so that higher levels of depres-
sion would be significantly associated with higher HbA1c
levels in type 1, but not type 2 diabetes.
2. Materials and methods
This cross-sectional observational study was carried out
at the University of Washington Diabetes Care Center
(DCC), Seattle, Washington. Eligible participants included
all English-speaking DCC patients already enrolled in both
1998 and 1999, age 18 or over. Potential subjects with
severe cognitive or language deficits were excluded. In July
1999, 826 potential subjects were sent an approach letter
briefly describing the study. Two weeks later subjects were
sent a questionnaire and consent form which fully explained
the study and requested permission for a review of their
automated records. Subjects not returning the questionnaire
within three weeks were sent an identical second question-
naire and consent form. Subjects received a $3 compensa-
tion for their time in participating in the study. The ques-
tionnaire and all patient correspondence were approved by
the University of Washington institutional review board.
2.1. Self report instruments
2.1.1. Depression
The Hopkins Symptom Checklist-90, Revised (SCL-
90-R) [9] is a self-report instrument, that has been validated
in previous studies of medical patients and has been found
to be highly reliable [10,11]. The twenty items from the
depression and additional symptom subscales (SCL-20)
were used in the current study.
2.1.2. Diabetes complications
Patients were given a score from 0 –3 to reflect the
number of self-reported diabetes-related complications from
the following: retinopathy, nephropathy, and peripheral
neuropathy [12]. This method has been shown to be highly
correlated with ratings of severity of diabetes from indepen-
dent physicians (r
⫽.72, P⬍.001) [12].
2.1.3. Medical comorbidity
Based on the methods of Wells et al. [13], we estimated
medical comorbidity by having patients check whether they
did or did not have each of eighteen medical conditions
(e.g., asthma, hypertension, ulcer) on a checklist. The total
number of conditions was calculated by summing positive
responses and for analyses each patient was given a score of
0, 1, 2 or more than 2 medical conditions.
2.1.4. Diabetes self-care
The Summary of Diabetes Self-Care Activities [14] is a
12-item questionnaire that measures absolute levels of self-
care behavior and the percentage of activities recommended
by the physician that were actually performed. This ques-
tionnaire has been shown to be a valid and reliable measure
of diabetes self-management in multiple trials. In this study,
diet amount, diet type, exercise, and glucose testing were
assessed, and since items within each domain have different
scales, raw scores for each were converted to standard
scores having a mean of 0 and an SD of 1. Standardized
scores were averaged to form a composite z score for each
regimen behavior. A higher z score indicates better adher-
ence to the self-care behavior.
2.1.5. Functional impairment
The Short-Form 12 Health Survey (SF-12) [15] is a
generic measure of health status that is a shorter version and
valid alternative to the SF-36 [16]. The SF-12 measures
functioning in medical populations and assesses physical
functioning, role limitations due to physical health prob-
247
P. Ciechanowski et al. / General Hospital Psychiatry 25 (2003) 246 –252

lems, bodily pain, general health, and social functioning,
which are represented in mental and physical component
scores. We report only the physical component score since
there is typically strong collinearity between depression and
the mental functioning score.
2.1.6. Symptom reporting
To assess diabetes symptoms, we used the Self-Comple-
tion Patient Outcome [17] instrument to measure the fol-
lowing diabetes symptoms: blurred vision, thirst, polyuria,
excessive hunger, shakiness, fatigue, parasthesias, and feel-
ing faint. Items were rated on a Likert scale and we calcu-
lated the total number of symptoms that were experienced at
least “several days” in the past month.
Demographic and clinical data were determined from
questionnaire responses (race, education, income, and mar-
ital status) and from automated data (age, gender and dia-
betes type). We also used automated data to determine mean
glycosylated hemoglobin (HbA1c) values for each subject
from the preceding twelve months. Mean number of HbA1c
tests in this population was 2 per year (range 0 – 6). To
analyze HbA1c levels, the University of Washington DCC
uses a Bayer DCA2000, which is certified by the National
Glycohemoglobin Standardization Program as having doc-
umented traceability to the Diabetes Control and Compli-
cations Trial Reference Method.
2.2. Diabetes classification
Subjects were classified in this clinic based on their
clinical characteristics. In general, individuals with type 1
diabetes presented in childhood, adolescence, or as young
adults with acute symptoms, often ketoacidosis. Those with
type 2 diabetes usually presented later in life and were
overweight. Since 1991 the clinic staff has had access to the
measurement of islet antibodies (islet cell antibody, glu-
tamic acid decarboxylase, insulinoma-associated-2 autoan-
tibodies, and insulin autoantibodies) and in those cases
where the diagnosis was not obvious, these antibodies were
measured. If one of these antibodies was positive the patient
was considered to have type 1 diabetes.
2.3. Statistical analysis
Data were analyzed using SPSS 10.0 for Windows. Two-
tailed t tests or
2
tests with corrections for continuity were
used to compare respondents and nonrespondents on age
and gender. Appropriate human subjects approval to utilize
aggregate data of nonrespondents on these variables was
obtained.
Multiple regression modeling with a combination of hi-
erarchical and stepwise techniques was used to determine if
depressive symptoms were associated with the following
dependent variables: HbA1c levels, diabetes symptoms,
self-care behaviors [diet type, diet amount, exercise, glu-
cose monitoring] and physical functioning. In each model
the significance of the demographic variables [age, gender,
marital status, education, race and income] was tested using
backward and forward stepwise techniques in the first step.
Only significant demographic variables were retained in the
models. In the second step, medical comorbidity and num-
ber of diabetes complications was forced into each model.
In the third and fourth steps diabetes type (type 1
⫽1; type
2
⫽0) and depression score were entered, respectively. In
the model assessing the association between depression and
HbA1c levels, the a priori hypothesis that diabetes type
would modify this association was tested by forcing in, as
the fifth step, the interaction of diabetes type and depres-
sion.
3. Results
Of 826 patients, 475 (58%) responded to the survey, of
which 276 (58%) had type 1 diabetes and 199 (42%) had
type 2 diabetes. There were no significant differences be-
tween respondents and nonrespondents in age (48.8
⫾15.9
vs. 50.0
⫾16.4, respectively; t⫽1.13, df⫽825, P⫽.26) and
gender (52.5% in both groups;
2
(df
⫽1)⫽0.04, P⫽.95).
All subsequent analyses are based on those respondents who
had at least one HbA1c level documented in the electronic
records within a twelve-month period (N
⫽407). Clinical
and demographic characteristics of the respondents are out-
lined in Table 1.
3.1. Glycemic control
In the multiple regression model (Table 2), being married
was associated with a lower HbA1c level, whereas number
of complications was strongly positively associated with
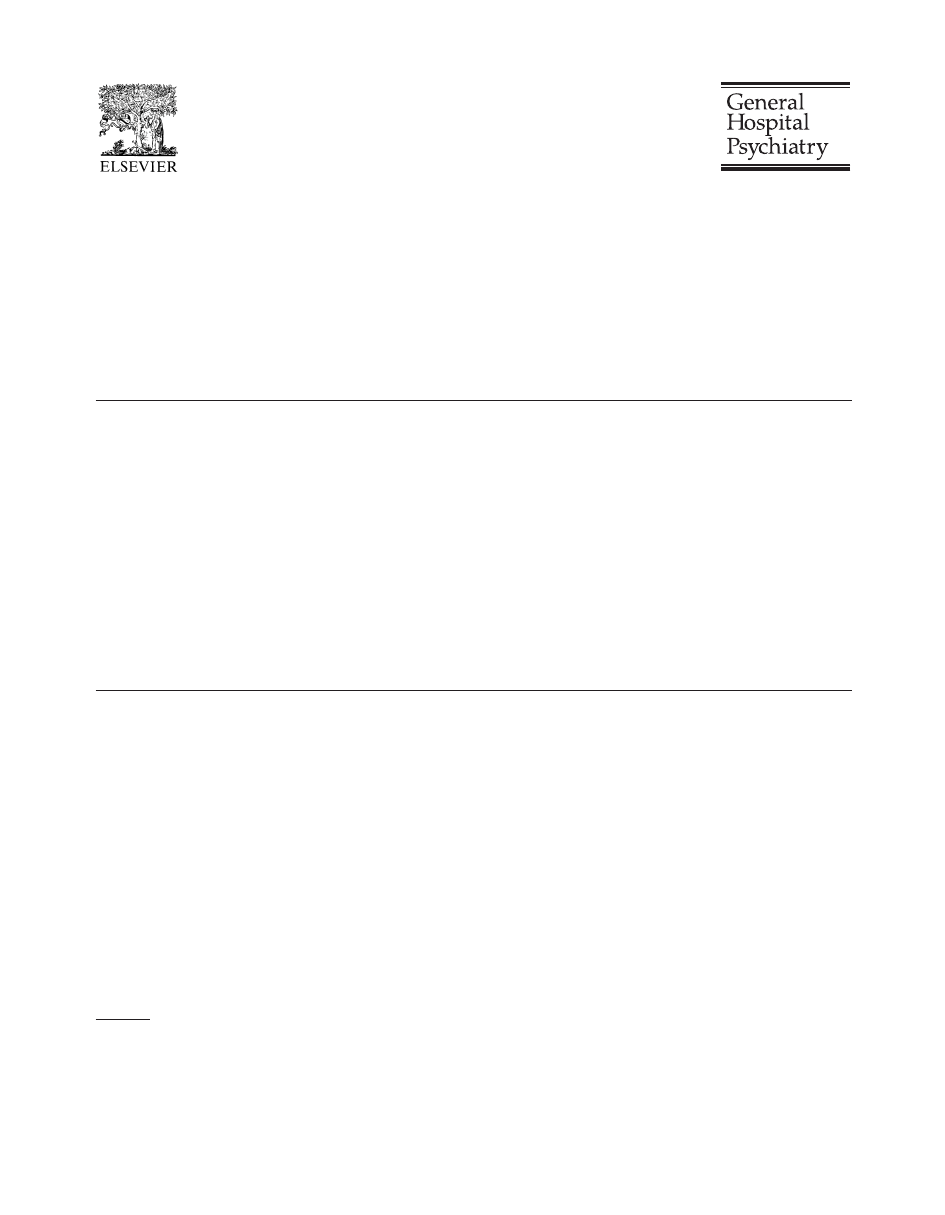
HbA1c level. There was a significant statistical interaction
of diabetes type and depression with respect to HbA1c level.
We chose clinically meaningful cut-scores to illustrate this
interaction in Fig. 1. A cut-score of 1.72 on the SCL-20 is
associated with the highest positive predictive value for the
diagnosis of major depression [18]. A cut-score of 8% for
HbA1c levels was chosen since current clinical guidelines
recommend additional clinical action for patients whose
HbA1c levels are above this range [19]. The proportion of
subjects with HbA1c levels over 8% was significantly
higher among patients with type 1 diabetes who were de-
pressed (66.7%) compared to those with type 1 who were
not depressed (38.6%) as well as compared to both de-
pressed and nondepressed type 2 diabetes patients (37.5%
and 40.3%, respectively) (
2
(df
⫽3)⫽9.6, P⫽.02).
Because we looked at HbA1c over the prior year, and the
self-report measure of depression asks about symptoms in
the past 2 weeks, we conducted a sensitivity analysis to
examine the correlation of depression and HbA1c levels
when only considering those HbA1c levels from the past 4
months (N
⫽253) and past 2 months (N⫽146), after control-
ling for the covariates from the linear model (married status
248
P. Ciechanowski et al. / General Hospital Psychiatry 25 (2003) 246 –252
and complications). In type 1 and 2 diabetic patients the
correlations were: 1) for 4 months, r
⫽.33, P⬍.001, r⫽.08,
NS, respectively; and, 2) for 2 months, r
⫽.42, P⬍.001,
r
⫽⫺.14, NS, respectively. Therefore, when SCL-20 scores
and HbA1c levels were more tightly associated in time of
measurement, there was a higher correlation in type 1 dia-
betes between the two measures. The mean SCL-20 depres-
sion score in this sample (0.9
⫾0.8) corresponds to a sub-
diagnostic range of depressive and anxiety symptoms,
which represent a mixture of dysthymic, and minor and
major depressed patients, as well as patients with adjust-
ment disorders with anxious and/or depressed mood [20 –
22].
3.2. Diabetes symptom reporting
In the multiple regression model assessing diabetes
symptom reporting, being married and higher education
Table 1
Demographic and clinical characteristics by diabetes type
Characteristic
Total (N
⫽ 407)
Diabetes Type
Analysis
Type 1 (N
⫽ 235)
Type 2 (N
⫽ 172)
Mean
SD
Mean
SD
Mean
SD
t
Age (years)
48.8
15.9
41.5
13.8
58.7
13.0
12.7***
HbAlc (%)
7.82
1.29
7.81
1.29
7.84
1.29
.29
SCL-20 score*
0.92
0.75
.85
0.74
1.01
0.77
2.25
N
%**
N
%**
N
%**
2
(df
⫽ 1)
Female gender
214
52.7
127
54.3
87
50.6
.54
Caucasian race
369
91.1
222
94.5
147
86.5
7.8**
At least 1 year college
363
89.4
212
90.2
151
88.3
.38
Married or cohabitating
278
68.8
162
69.2
116
68.2
.05
Income
⬎$40,000
255
65.9
155
69.2
100
61.3
2.6
At least 1 medical comorbidity
313
77.3
165
70.5
148
86.5
14.5***
At least 1 diabetes complication
189
47.3
108
46.6
81
48.2
.11
Diabetes treatment in type 2
diabetes patients
Insulin only
–
–
63
42.3
–
Oral hypoglycemics only
–
–
53
35.6
–
Insulin and oral hypoglycemics
–
–
22
14.8
–
Diet only
–
–
11
7.4
–
* Range of SCL-20 values: type 1 diabetes: 0 –3.4; type 2 diabetes: 0 –3.3.
**Number of subjects on which percents are based varies because of missing data from some items. SCL
⫽ Symptom Checklist
Table 2
Multiple regression modeling of the association of depression and selected variables
HbAlc
Diabetes
Symptom
Reporting
Physical
Component
Score
Diet Amount
Diet Type
Exercise
Glucose
monitoring

t

t

t

t

t

t

t
Demographic
covariates
age
⫺.17** ⫺3.50
.20**
3.23
.32
†
5.14
marital status
⫺.14** ⫺2.69
⫺.10*
⫺2.21
income
.12**
2.78
education
⫺.10*
⫺2.14
Clinical covariates
comorbidity
.01
.20
.01
.12
⫺.36
†
⫺7.32 ⫺.05
⫺.79
⫺.003
⫺.05 ⫺.06
⫺1.00 ⫺.03
⫺.37
complications
.29
†
5.24
⫺.13*
2.46
⫺.12** ⫺2.68 ⫺.03
.59
⫺.04
.64
⫺.07
⫺1.29 ⫺.07
1.08
Diabetes type
⫺.18*
⫺2.24
⫺.03
⫺.60
.05
.99
.18
2.85
.11
1.68
.11*
2.14
⫺.03
⫺.44
Depression
⫺.08
⫺1.01
.41
†
8.50
⫺.23** ⫺5.13 ⫺.25
†
⫺4.53
⫺.14* ⫺2.58 ⫺.15** ⫺2.78 ⫺.07 ⫺1.10
Diabetes type
⫻
depression
.22*
2.47
Overall model
F(6,361)
⫽ 10.42,
R
2
⫽ 0.15,
p
⬍ .0001
F(6,362)
⫽ 23.23,
R
2
⫽ 0.28,
p
⬍ .0001
F(6,364)
⫽ 42.90,
R
2
⫽ 0.44,
p
⬍ .0001
F (5,351)
⫽ 9.58,
R
2
⫽ 0.12,
p
⬍ .0001
F(5,359)
⫽ 8.90,
R
2
⫽ 0.11,
p
⬍ .0001
F(5,361)
⫽ 6.24,
R
2
⫽ 0.07,
p
⬍ .0001
F(4,305)
⫽ .56,
R
2
⫽ 0.01,
p
⫽ .69
* p
⬍ .05, **p ⬍ .01,
†
p
⬍ .001
249
P. Ciechanowski et al. / General Hospital Psychiatry 25 (2003) 246 –252
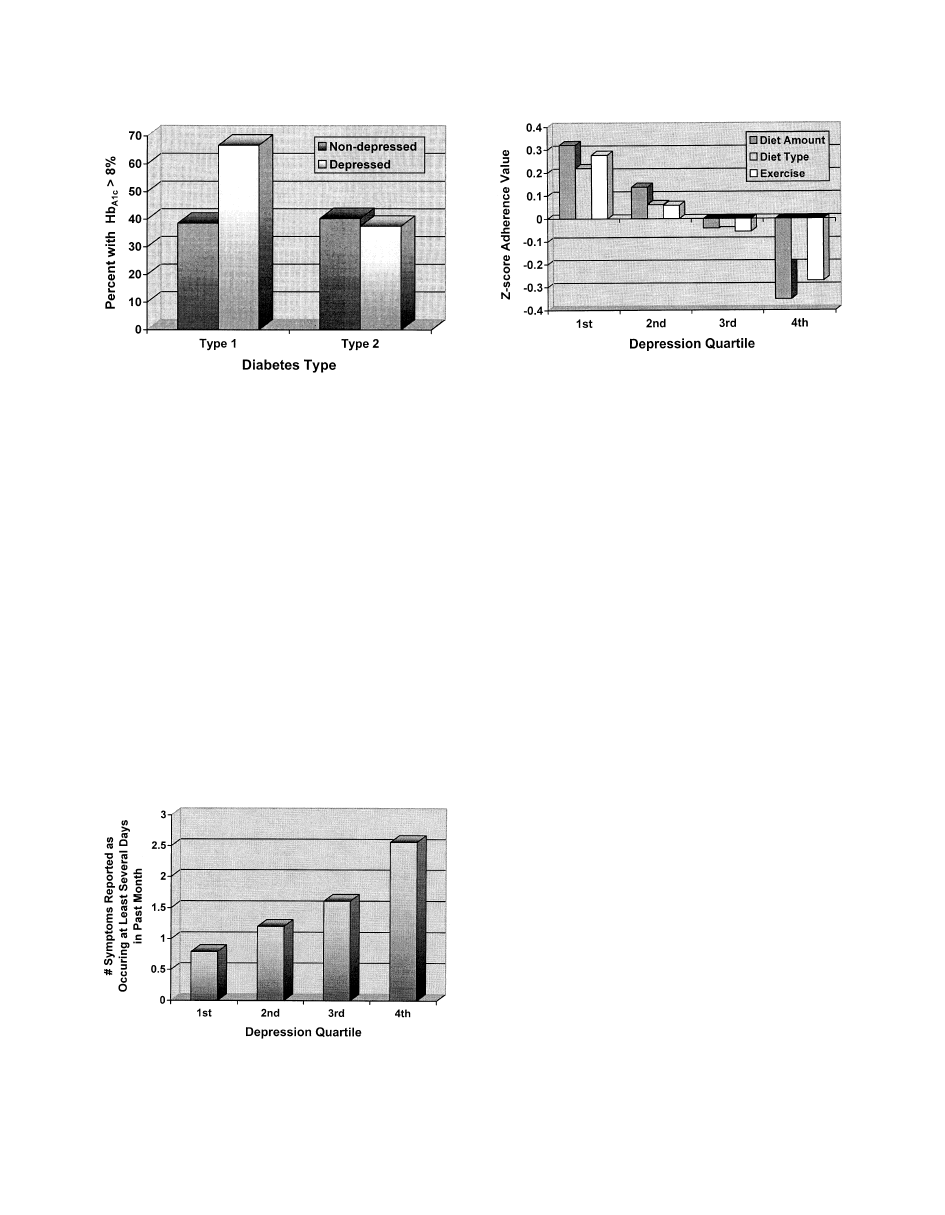
were significantly associated with lower symptom reporting
whereas higher levels of diabetes complications and depres-
sion were significantly and independently associated with
more diabetes symptom reporting (Table 2). To illustrate
this relationship graphically, quartiles of depression were
used to derive means of symptom reporting in each quartile.
Fig. 2 shows the mean number of diabetes symptoms re-
ported as occurring at least several days in the prior month
by quartiles of SCL-20 depression scores.
3.3. Physical functioning
Increasing age, and higher levels of medical comorbid-
ity, diabetes complications and depression were all signifi-
cantly associated with poorer physical functioning in our
sample, while higher income was associated with better
physical functioning (Table 2).
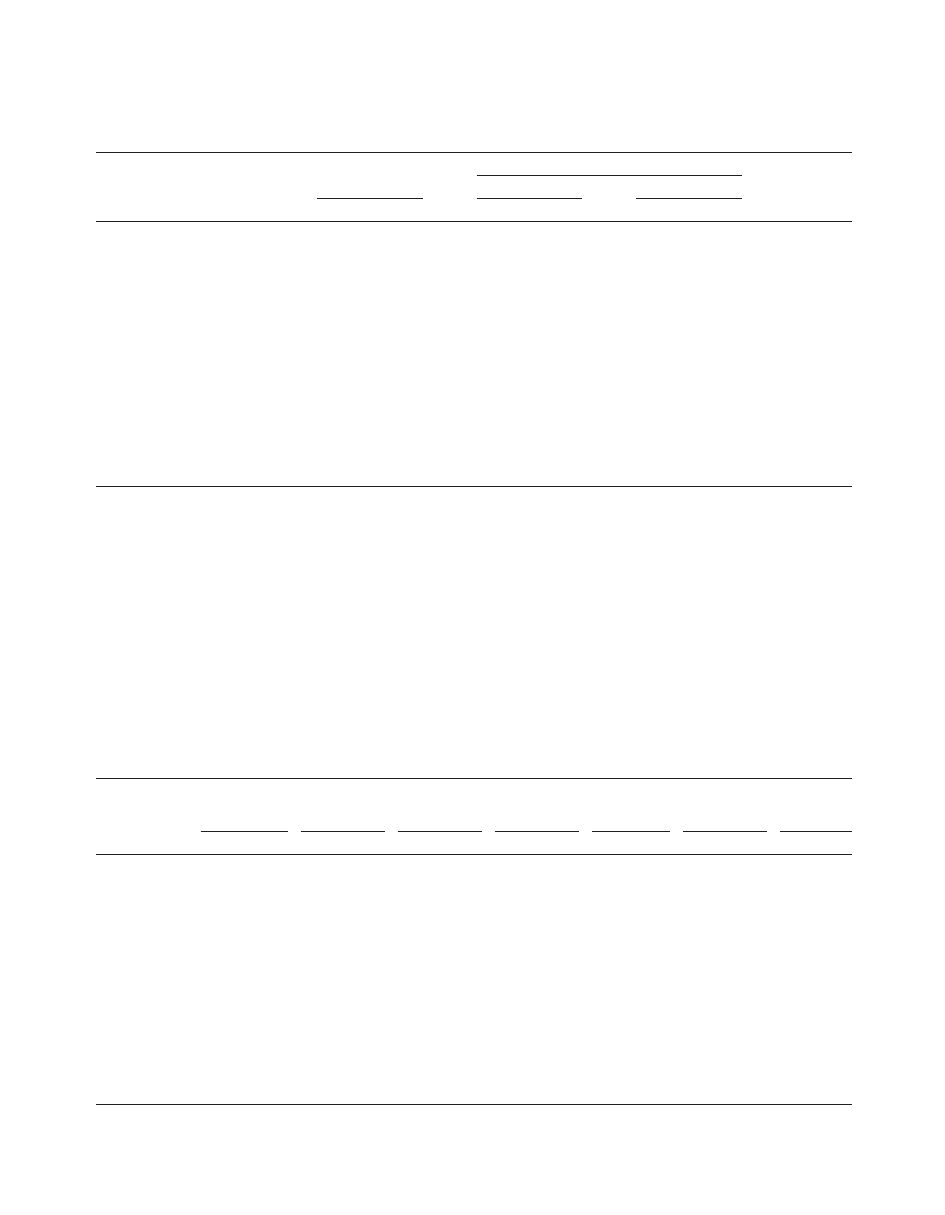
3.4. Diabetes self-care
Increasing age was significantly associated with higher
self-reported adherence to diet amount and type, while a
higher level of depression was associated with lower self-
reported adherence to diet amount, diet type and exercise.
Type 1 diabetes was significantly associated with higher
self-reported adherence with exercise. Glucose monitoring
was not associated with any of the variables in our model.
Fig. 3 illustrates the association between self-care and de-
pression for those domains of self-care that have been
shown to be significantly associated with depression (diet
type, diet amount and exercise). Again, depression severity
was grouped into quartiles and mean z-score for each do-
main of self-care was obtained for each quartile. As shown
in the figure, as depression increased, levels of diet and
exercise adherence decreased.
4. Discussion
Depressive symptoms were found to be significantly
associated with lower adherence to dietary recommenda-
tions and exercise, poorer physical functioning, and higher
diabetes symptom reporting among patients with type 1 and
type 2 diabetes in a tertiary care diabetes specialty clinic.
These associations were robust after controlling for diabetes
type and complications. These results are consistent with
other studies. For example, in our previous study of a
primary care sample of predominantly type 2 diabetic pa-
tients, dietary recommendations were not followed as
closely in patients with greater levels of depression [4].
Common symptoms of depression such as changes in ap-
petite and decreased energy and motivation may signifi-
cantly affect diet and exercise. While changes in motivation
and concentration that occur in depression can conceivably
affect frequency of glucose monitoring, no evidence for this
could be found in our sample. In our previous study, we also
Fig. 1. Association between depression and HbA1c levels by diabetes type.
Depressed group has SCL-20 score
ⱖ1.72, nondepressed group has
SCL-20 score
⬍1.72.
Fig. 2. Association between depression quartiles and diabetes-related
symptom reporting. Number of symptoms refers to total number of diabe-
tes symptoms reported as occurring at least several days in prior month.
Ranges of quartiles of SCL-20 depression scores are as follows: 1st: 0-.34;
2nd: .35-.69; 3rd: .70 –1.35; 4th: 1.36 –3.40.
Fig. 3. Association between depression quartiles and diabetes self-care.
Ranges of quartiles of SCL-20 depression scores are as follows: 1st: 0-.34;
2nd: .35-.69; 3rd: .70 –1.35; 4th:1.36 –3.40.
250
P. Ciechanowski et al. / General Hospital Psychiatry 25 (2003) 246 –252

observed an association between physical functioning and
depression [4].
There was also a strong and significant association be-
tween depression and diabetes symptom reporting even af-
ter controlling for diabetes severity and medical comorbid-
ity. This corresponds to previous research in which it was
shown that depression was associated with diabetes symp-
toms even after adjusting for HbA1c levels [8]. In post hoc
analyses, we found that by controlling for HbA1c, as a final
step in our linear regression model, depressive symptoms
still remained highly correlated with symptom reporting.
Furthermore, post hoc Pearson correlations showed that all
8 symptoms were significantly correlated (P
⬍.005) with
depression ranging from r
⫽.43 for sleepiness to r⫽.15 for
shakiness in the following order from highest to lowest
correlation: sleepiness, blurry vision, thirst, parasthesias,
hunger, polyuria, feeling faint, and shakiness. Research in
patients with other chronic medical illnesses such as hepa-
titis C, inflammatory bowel disease, coronary artery disease,
and patients with closed head injury have all shown that
depression comorbidity is associated with increased physi-
cal symptom reporting even after controlling for severity of
illness [23].
Depressive symptoms were associated with a significant
increase in glycosylated hemoglobin (HbA1c) in type 1, but
not type 2 diabetic patients. This is consistent with the
results of a recent study by Van Tilburg and colleagues [6].
These results suggest that whether the impact of depres-
sion on glucose control is mediated through its effect on
self-care behaviors, or via central effects such as by influ-
encing the hypothalamic-pituitary adrenal axis [24], that the
impact is considerably greater for type 1 diabetic patients.
This may be because of increased complexity of self-care
regimens in type 1 diabetes, or because of neurohormonal
differences in regulation of glucose between type 1 and 2
diabetes.
Prior researchers have reported the effect of depression
on worsening adherence to medical regimens in general
[25], and to various self-care strategies (glucose monitoring,
exercise, diet, medications) in diabetes [26,27]. The im-
portance of improving adherence to treatment of diabetes
has been emphasized in both the Diabetes Control and
Complications Trial (DCCT) [28] and the UK Prospective
Diabetes Study [29] which both showed that strict ad-
herence to diabetes treatment (and lowering of blood sugar)
in type 1 and type 2 diabetic patients, respectively, resulted
in a decreased risk of long-term complications. Other
studies have shown that depression is associated longitudi-
nally with an increased risk of diabetic complications,
especially retinopathy and macrovascular complications
[30,31]. The implications of untreated depression on long-
term complications are even more significant when one
considers that depression tends to be recurrent or chronic in
most patients with diabetes, e.g., in one study, 79% of
patients reporting a history of major depression relapsed
over a 5-year follow-up period with a mean of four episodes
per patient [32]. One recent randomized controlled trial has
suggested that improved outcomes of depression with cog-
nitive behavioral therapy versus diabetic educational treat-
ment were associated with significantly improved HbA1c
levels at 6 months follow up [33]. Another randomized
controlled trial [34] has shown that a serotonin-selective
reuptake inhibitor was more effective than placebo in treat-
ing major depression in diabetic patients. The clinician
treating diabetic patients should strive to recognize depres-
sion among these patients because of the strong possibility
that diabetes symptoms, physical functioning, diabetes self-
care and HbA1c levels may all improve with depression
treatment.
There are several limitations of this study. Although this
was a population-based study of diabetic patients from a
tertiary care clinic, there is possibly a lack of generalizabil-
ity of this predominantly Caucasian, educated, employed
and insured health care population to other settings. Fur-
thermore, it is possible that the intensity of the care received
from a diabetologist and diabetes treatment team in this
sample, not to mention possible selection biases of patients
who chose to come to a tertiary care center, may make this
sample less generalizable to a typical primary care popula-
tion. As a result, there may be less variability in treatment
outcomes—particularly with type 2 diabetic patients—as
compared to similar patients in primary care.
Another possible limitation of this study is the use of
self-report questionnaires to derive levels of depressive
symptom severity rather than using structured interviews to
make a diagnosis of major depression. Similarly, self-re-
ported instruments were used to assess self-care behaviors,
and may be less accurate than objective measures of adher-
ence as a result of social desirability bias. Because this study
reports cross-sectional observational data, we cannot make
causal inferences about depressive symptoms on the re-
ported outcomes. Alternative explanations, such as that de-
pressive symptoms resulting from poorer diabetes outcomes
or the possibility that unmeasured third factors may be
responsible for this relationship, must be considered. Larger
scale randomized controlled trials need to be planned that
measure the effect of interventions that improve depressive
outcomes on symptom burden, functional impairment, self-
management and HbA1c levels.
Acknowledgments
The authors thank Anthony D’Amico and Larry
Mix for their assistance with collection of data for this
study.
Supported by Group Health Cooperative/Kaiser Perma-
nente Community Foundation Grant #66-0404 and Bayer
Institute for Health Care Communication Grant #98-439
and NIDDK grant K23 DK60652-01.
251
P. Ciechanowski et al. / General Hospital Psychiatry 25 (2003) 246 –252

References
[1] Anderson RJ, Freeland KE, Clouse RE, Lustman PJ. The prevalence
of comorbid depression in adults with diabetes: a meta-analysis.
Diabetes Care 2001;24(6):1069 –1078.
[2] Lustman PJ, Clouse RE, Freedland KE. Management of major de-
pression in adults with diabetes: implications of recent clinical trials.
Sem Clin Neuropsychiatry 1998;3:102–114.
[3] Egede LE, Zheng D, Simpson K. Comorbid depression is associated
with increased health care use and expenditures in individuals with
diabetes. Diabetes Care 2002;25(3):464 – 470.
[4] Ciechanowski PS, Katon WJ, Russo JE. Depression and diabetes:
impact of depressive symptoms on adherence, function, and costs.
Arch Intern Med 2000 Nov 27;60(21):3278 –3285.
[5] Lustman PJ, Anderson RJ, Freeland KE, de Groot M, Carney RM,
Clouse RE. Depression and poor glycemic control: a meta-analytic
review of the literature. Diabetes Care 2000;23(7):934 – 42.
[6] Van Tilburg MA, McCaskill CC, Lane JD, Edwards CL, Bethel A,
Feinglos MN, Surwit RS. Depressed mood is a factor in glycemic
control in type 1 diabetes. Psychosom Med 2001;63(4):551–555.
[7] Katon WJ. The effect of major depression on chronic medical illness.
Sem Clin Neuropsychiatry 1998;3:82– 86.
[8] Lustman PS, Clouse RE, Carney RM. Depression and the reporting of
diabetes symptoms. Int J Psychiatry Med 1988;18:295–303.
[9] Derogatis LR, Lipman RS, Rickels K, Uhlenhuth EH, Covi L. The
Hopkins Symptom Checklist (HSCL): a self-report symptom inven-
tory. Behav Sci 1974;19(1):1–15.
[10] Goldberg DP, Rickels K, Downing R, Hesbacher P. A comparison of
two psychiatric screening tests. Br J Psychiatry 1976;129:61– 67.
[11] Glass RM, Allan AT, Uhlenhuth EH. Psychiatric screening in a
medical clinic. Arch Gen Psychiatry 1978;35:1189 –1195.
[12] Jacobson AM, de Groot M, Sampson JA. The effects of psychiatric
disorders and symptoms on quality of life in patients with type I and
type II diabetes mellitus. Qual Life Res 1997;6:11–20.
[13] Wells KB, Sherbourne C, Schoenbaum M, Duan N, Meredith L,
Unu¨tzer J, Miranda J, Carney MF, Rubenstein LV. Impact of dissem-
inating quality improvement programs for depression in managed
primary care: a randomized controlled trial. JAMA. 2000;283(2):
212–220.
[14] Toobert DJ, Glasgow RE. Assessing diabetes self-management: the
summary of diabetes self-care activities questionnaire. In: Bradley C.,
editor. Handbook of Psychology and Diabetes. Berkshire, UK, Har-
wood Academic, 1994.
[15] Ware JE, Kosinski M, Keller SD. SF-12. How to score the SF-12
physical and mental health summary scales. Boston, MA, The Health
Insitiute, New England Medical Center, 1995.
[16] Ware JE, Kosinski M, Keller SD. A 12-Item Short-Form Health
Survey. Construction of scales and preliminary tests of reliability and
validity. Med Care 1996;34:220 –234.
[17] Whitty P, Steen N, Eccles M. A new completion outcome measure for
diabetes: is it responsive to change? Qual Life Res 1997;6:407– 413.
[18] Mulrow CD, Williams JS, Gerety MB, Ramirez G, Montiel OM,
Kerber C. Case-finding instruments for depression in primary care
settings. Ann Intern Med 1995;122(12):913–921.
[19] American Diabetes Association: Clinical practice recommendations.
Diabetes Care 2000;24 (Suppl. 1):S33–S44.
[20] Katon WJ, Von Korff M, Lin E, et al. Collaborative management to
achieve treatment guidelines: impact on depression in primary care.
JAMA 1995;273:1026 –1031.
[21] Hough R, Landsverk J, Stone J, et al. Comparison of psychiatric
screening questionnaires for primary care patients. Rockville, Md:
National Institute of Mental Health; 1983. Final report for NIMH
Contract No. 278-81-0036 (DB).
[22] Williams JW, Barrett J, Oxman T, et al. Treatment of dysthymia and
minor depression in primary care: a randomized controlled trial in
older adults. JAMA 2000;284:1519 –1526.
[23] Katon W, Ciechanowski P. Impact of major depression on chronic
medical illness. J Psychosom Research 2002;53:859 – 863.
[24] Winokur A, Maislin G, Phillips JL, Amsterdam JD. Insulin resistance
after oral glucose tolerance testing in patients with major depression.
Am J Psychiatry 1988;145:325–330.
[25] DiMatteo MR, Lepper HS, Croghan TW. Depression is a risk factor
for noncompliance with medical treatment: meta-analysis of the ef-
fects of anxiety and depression on patient adherence. Arch Intern Med
2000;160(14):2101–2107.
[26] McGill JB, Lustman PJ, Griffith LS, et al. Relationship of depression
to compliance with self-monitoring of blood glucose (abstract). Dia-
betes 1992;41:A84.
[27] Littlefield CH, Craven JL, Rodin GM, Daneman D, Murray MA,
Rydall AC. Relationship of self-efficacy and binging to adherence to
diabetes regimens among adolescents. Diabetes Care 1992;15:90 –94.
[28] The DCCT Research Group. Influence of intensive diabetes treatment
on quality of life outcomes in the Diabetes Control and Complications
Trial. Diabetes Care 1996;19:195–203.
[29] The United Kingdom Prospective Diabetes. Intensive blood-glucose
control with sulphonylureas or insulin compared with conventional
treatment and risk of complications in patients with type 2 diabetes.
Lancet 1998;3352:837– 853.
[30] Kovacs M, Obrosky DS, Goldston D, Drash A. Major depressive
disorder in youths with IDDM. A controlled prospective study of
course and outcome. Diabetes Care 1997;20:45–51.
[31] Carney RM, Freedland KE, Lustman PJ, Griffith LS. Depression and
coronary artery disease in diabetic patients: a 10-year follow-up.
Psychosom Med 1985;47:372–381.
[32] Lustman PJ, Griffith LS, Clouse RE: Depression in adults with
diabetes: results of a 5-year follow-up study. Diabetes Care 1988;11:
605– 612.
[33] Lustman PJ, Griffith LS, Freedland KE, Kissel S, Clouse RE. Cog-
nitive behavioral therapy for depression in type 2 diabetes mellitus: a
randomized controlled trial. Ann Intern Med 1998;129:613– 621.
[34] Lustman PJ, Freedland KE, Griffith LS, Clouse RE. Fluoxetine for
depression in diabetes: a randomized double-blind placebo-controlled
trial. Diabetes Care 2000;23(5):618 – 623.
252
P. Ciechanowski et al. / General Hospital Psychiatry 25 (2003) 246 –252
Document Outline
- The relationship of depressive symptoms to symptom reporting, self-care and glucose control in diabetes
Wyszukiwarka
Podobne podstrony:
Depresja cz II id 133646 Nieznany
Warsztaty samodoskonalace Program walki z lekiem i depresja Wydanie II 2
Warsztaty samodoskonalace Program walki z lekiem i depresja Wydanie II warsam
8 2010 Zab afektywne i depresje cz II
8 Zab afektywne i depresje WWL8 II
Warsztaty samodoskonalace Program walki z lekiem i depresja Wydanie II warsam
Warsztaty samodoskonalace Program walki z lekiem i depresja Wydanie II warsam
Warsztaty samodoskonalace Program walki z lekiem i depresja Wydanie II warsam
Warsztaty samodoskonalace Program walki z lekiem i depresja Wydanie II warsam
Depresja zimowa epidemiologia, etiopatogeneza, objawy i metody leczenia
depresja-psychopatologia, Pedagogika II rok
LECZENIE CUKRZYCY II
LECZENIE DEPRESJI
Leczenie pacjentów powypadkowych cz II
LECZENIE DEPRESJI
więcej podobnych podstron