
Associations among adolescent risk behaviours
and self-esteem in six domains
Lauren G. Wild,
1
Alan J. Flisher,
1
Arvin Bhana
2
and Carl Lombard
3
1
University of Cape Town, South Africa;
2
Human Sciences Research Council, Durban, South Africa;
3
Medical Research Council, Cape Town, South Africa
Background: This study investigated associations among adolescents’ self-esteem in 6 domains (peers,
school, family, sports/athletics, body image and global self-worth) and risk behaviours related to
substance use, bullying, suicidality and sexuality. Method: A multistage stratified sampling strategy
was used to select a representative sample of 939 English-, Afrikaans- and Xhosa-speaking students in
Grades 8 and 11 at public high schools in Cape Town, South Africa. Participants completed the mul-
tidimensional Self-Esteem Questionnaire (SEQ; DuBois, Felner, Brand, Phillips, & Lease, 1996) and a
self-report questionnaire containing items about demographic characteristics and participation in a
range of risk behaviours. It included questions about their use of tobacco, alcohol, cannabis, solvents
and other substances, bullying, suicidal ideation and attempts, and risky sexual behaviour. Data was
analysed using a series of logistic regression models, with the estimation of model parameters being
done through generalised estimation equations. Results: Scores on each self-esteem scale were sig-
nificantly associated with at least one risk behaviour in male and female adolescents after controlling for
the sampling strategy, grade and race. However, specific self-esteem domains were differentially related
to particular risk behaviours. After taking the correlations between the self-esteem scales into account,
low self-esteem in the family and school contexts and high self-esteem in the peer domain were signi-
ficantly independently associated with multiple risk behaviours in adolescents of both sexes. Low body-
image self-esteem and global self-worth were also uniquely associated with risk behaviours in girls, but
not in boys. Conclusions: Overall, the findings suggest that interventions that aim to protect adoles-
cents from engaging in risk behaviours by increasing their self-esteem are likely to be most effective and
cost-efficient if they are aimed at the family and school domains. Keywords: Adolescence, bullying,
self-esteem, sexual behaviour, substance use, suicidal behaviour.
In recent years, researchers have begun to pay
increasing attention to adolescent risk behaviours.
The primary reason for this is that the major causes of
adolescent morbidity and mortality are not diseases
but preventable behaviours, in interaction with social
and environmental factors. Adolescent health prob-
lems are mainly related to sexual and reproductive
health and the use of substances such as tobacco,
alcohol and psychoactive drugs. Accidents (especially
traffic incidents), suicide and violence from others are
the leading causes of death in individuals aged be-
tween 10 and 19 (World Health Organization, 1993).
Risk behaviours do not only jeopardise physical
health, however. They also have psychological and
social outcomes, in that they can interfere with the
accomplishment of normal developmental tasks and
the fulfilment of expected social roles (Jessor, 1991).
There is considerable evidence that adolescent risk
behaviours
are
interrelated
(Flisher,
Ziervogel,
Chalton, Leger, & Robertson, 1996; Jessor, 1991;
McGee & Williams, 2000). This suggests that health-
compromising behaviours in adolescents may have
common underlying factors, and that the identifica-
tion of these aetiological factors is likely to have
important implications for designing effective inter-
vention programmes.
One possible antecedent of risk behaviours in
adolescence is low self-esteem. Self-esteem is gen-
erally used to refer to an individual’s evaluation of
him- or herself, including feelings of self-worth
(Coopersmith, 1967; Rosenberg, 1979). Several the-
orists have argued that individuals with low self-
esteem are predisposed to adopt risk behaviours,
although the reasons given for this vary. Kaplan
(1975) proposes that adolescents whose experiences
in their conventional, normative membership groups
have led to feelings of self-rejection lose motivation to
conform to the conventional group’s norms. This
increases the likelihood that they will turn instead to
delinquent peers and adopt risk behaviours that are
valued and considered to be appropriate within these
deviant groups (Jang & Thornberry, 1998). Other
theorists have argued that people low in self-esteem
may turn to risk behaviours such as substance
abuse as a way to cope with or escape from the neg-
ative feelings associated with low self-worth (Bau-
meister, 1990; Jessor, Van den Bos, Vanderryn,
Costa, & Turbin, 1995), because these are the only
means available to them to deal with stress (Koval &
Pederson, 1999), or because they are easily influ-
enced by others through ‘peer pressure’ (McGee &
Williams, 2000). Such theories suggest that raising
adolescents’ self-esteem will help to protect them
against adopting risk behaviours.
Empirical evidence for a relationship between self-
esteem and adolescent risk behaviours is, however,
Journal of Child Psychology and Psychiatry 45:8 (2004), pp 1454–1467
doi: 10.1111/j.1469-7610.2004.00330.x
Ó Association for Child Psychology and Psychiatry, 2004.
Published by Blackwell Publishing, 9600 Garsington Road, Oxford OX4 2DQ, UK and 350 Main Street, Malden, MA 02148, USA

inconclusive. Several cross-sectional and longitud-
inal studies have linked low self-esteem with current
and/or future risk behaviours. For example, low
self-esteem (assessed as an overall tone of self-dis-
approval) has been significantly associated with
substance abuse (Gordon & Caltabiano, 1996), in-
cluding a greater frequency and quantity of alcohol
use and problem drinking (Scheier, Botvin, Griffin, &
Diaz, 2000), smoking (Carvajal, Wiatrek, Evans,
Knee, & Nash, 2000), using cannabis (Ho
¨fler et al.,
1999) and using inhalants (Howard & Jenson, 1999;
Howard, Walker, Walker, Cottler, & Compton, 1999).
Low self-esteem has also been linked with other
health risk behaviours such as problem eating
(McGee & Williams, 2000) and suicidal ideation or
behaviours (McGee & Williams, 2000; Neumark-
Sztainer, Story, French, & Resnick, 1997; Vella,
Persic, & Lester, 1996; Yoder, 1999).
Other researchers have found that associations
between low self-esteem and risk behaviours are
limited to certain demographic groups. For example,
four studies have linked smoking, problem drinking
and/or unhealthy weight loss behaviours with low
self-esteem for girls, but not for boys (Abernathy,
Massad, & Romano-Dwyer, 1995; Koval, Pederson,
Mills, McGrady, & Carvajal, 2000; Neumark-Sztain-
er et al., 1997; Pitka
¨nen, 1999). Berry, Shillington,
Peak, and Hohman (2000) found that lower self-
esteem in adolescence appeared to increase the odds
of a teen pregnancy for blacks and Hispanics, but
not for whites and Native Americans.
Still other studies have found that after controlling
for other highly correlated child and family back-
ground variables, low self-esteem is unrelated to
later alcohol intake or problem drinking (Poikolai-
nen, Tuulio-Henriksson, Aalto-Seta
¨la, Marttunen,
& Lo
¨nnqvist, 2001; Scheier et al., 2000), increased
smoking (Carvajal et al., 2000), substance use
in general (Koval & Pederson, 1999; McGee &
Williams, 2000; Neumark-Sztainer et al., 1997; West
& Sweeting, 1997), suicidality (Beautrais, Joyce, &
Mulder, 1999; Kingsbury, Hawton, Steinhardt, &
James, 1999; Roberts, Roberts, & Chen, 1998) or
early sexual activity and adolescent pregnancy
(Hockaday, Crase, Shelley, & Stockdale, 2000;
McGee & Williams, 2000; Neumark-Sztainer et al.,
1997; West & Sweeting, 1997). In fact, one study
(Paul, Fitzjohn, Herbison, & Dickson, 2000) found
that higher self-esteem was an independent predic-
tor of early sexual intercourse in females, but not in
males.
One probable reason for the inconsistencies in
these findings is that researchers have used different
operational definitions of self-esteem, and have var-
ied in the extent to which they have controlled for its
covariates. A study by Kawabata, Cross, Nishioka,
and Shimai (1999) suggests that one way of
approaching this issue might be to replace the uni-
dimensional measures of global self-esteem used in
most studies with a more specific, multidimensional
measure. These researchers found a trend for Jap-
anese adolescents who had ever smoked to report
lower perceived cognitive competence and lower
family self-esteem but higher perceived physical
competence than those who had never smoked.
Since interventions that address specific domains or
components of self-esteem appear to be more suc-
cessful than programmes that attempt to enhance
global self-esteem directly (Harter, 1998), further
exploration of possible differential relationships
between adolescent risk behaviours and different
domains of self-esteem is important.
Inconsistencies in previous research results might
also reflect sampling characteristics. The research
reviewed above has been conducted in a number of
different countries in North America, Europe and
Australasia, and the research findings might be
influenced by cultural variations in conceptions of,
and responses to, risk behaviours and mental health
(Poikolainen et al., 2001). Further research is
therefore needed to investigate links between specific
domains of self-esteem and a variety of risk behav-
iours in other cultures. In particular, we are not
aware of any published studies that examine these
relationships in developing countries.
As a first step towards addressing this gap, Wild,
Flisher, Bhana, and Lombard (2002a) conducted a
pilot study examining links between the multidi-
mensional Self-Esteem Questionnaire (SEQ; DuBois,
Felner, Brand, Phillips, & Lease, 1996) and indica-
tors of substance use and suicidality in a sample of
116 adolescents enrolled in Grade 8 and Grade 11 at
independent (private) schools in Cape Town, South
Africa. Results of this study provided preliminary
evidence that specific domains of self-esteem are
differentially associated with particular risk behav-
iours. Family self-esteem showed the strongest
overall pattern of correlations with the risk behav-
iours assessed, and made a significant unique con-
tribution to predicting whether a student had ever
smoked a whole cigarette, used illicit drugs, and
thought about or attempted suicide. Lower school
self-esteem was also significantly associated with
smoking, and lower global self-esteem was signific-
antly associated with suicidality. In contrast, higher
sports/athletics self-esteem was significantly asso-
ciated with an increased probability of using alcohol
in the past month and smoking. Self-esteem with
respect to peers and body image did not make a
unique contribution to predicting any of the risk
behaviours assessed.
Adolescents attending independent schools are
not representative of high school students in Cape
Town since they have high socioeconomic status,
and it is not clear to what extent these findings can
be generalised to all adolescents. Moreover, the
sample size in this study was too small to stratify the
data by gender, although previous research has
suggested that predictors of risk behaviour may dif-
fer for boys and girls (Abernathy et al., 1995; Koval
Self-esteem and adolescent risk behaviours
1455

et al., 2000; Neumark-Sztainer et al., 1997; Pitka
¨nen,
1999). The present study was therefore designed to
extend this pilot work to a considerably larger,
representative sample of English-, Afrikaans- and
Xhosa-speaking public high-school students in Cape
Town. In particular, it aimed to explore associations
among adolescents’ self-evaluations in the contexts
of peers, school, family, sports/athletics and body
image and their feelings of global self-worth, and risk
behaviours related to substance use, bullying, suicid-
ality and sexuality.
Method
Participants
The study population was all students in Grades 8 and
11 attending public high schools in Cape Town. These
grade levels were selected in order to include as wide an
age range as possible, given that it was not financially
feasible to sample students in all grade levels. Grade 8
is the first year of high school in South Africa, and
Grade 11 is the penultimate year. Researchers are not
usually permitted access to Grade 12 students as they
are preparing for their final examinations.
Schools were stratified by postal code groupings, as
areas with the same postal code tend to be relatively
homogenous with regard to socio-economic status and
racial composition. We selected 39 schools such that
the proportion of the selected schools in a particular
stratum was directly proportional to the number of
students in that stratum. Within each stratum, the
selection probability of a school was proportional to the
number of students in that school. Two classes were
randomly selected from each participating grade, and
40 students were randomly selected from their com-
bined class lists. An additional 5 students were selected
as replacements for a maximum of 5 absent students.
This procedure yielded a total sample of 2,946 stu-
dents, of whom every third student in each class com-
pleted
the
self-esteem
measure.
The
remaining
students completed questionnaires assessing other
potential predictors of adolescent risk behaviour that
are not included in this report.
Of the participating students (N
¼ 939), 480 (51%)
were in Grade 8. The mean age of the 478 Grade 8
students who reported this information was 14.1 years
(range
¼ 12–24, SD ¼ 1.22), while the mean age of the
457 Grade 11s who provided this information was
17.4 years (range
¼ 15–26, SD ¼ 1.70). Five hundred
and nineteen of the 920 participants (56%) who pro-
vided information on their gender were female.
Of the 908 students who reported their racial classi-
fication, 459 (51%) described themselves as coloured
(derived from Asian, European and African ancestry),
241 (26%) as black, 205 (23%) as white, and 3 as Asian.
These race groups are as defined by the repealed popu-
lation registration act of 1950, and do not have
anthropological or scientific validity. However, they are
used because there are differences between the groups
for many indicators of health, mediated by political and
economic factors (Ellison, De Wet, Ijsselmuiden, &
Richter, 1996). Census figures suggest that blacks may
have been underrepresented in this sample, while
whites were overrepresented. Estimates of the racial
breakdown of 10- to 19-year-olds in Cape Town in 2001
were 53% coloured, 32% black, 14% white and 1%
Asian, although preliminary independent demographic
analyses suggest that these figures underestimate the
white population (Statistics South Africa, 2003). The
original English-language version of the questionnaire
was completed by 399 adolescents (42%), the Afrikaans
version by 384 adolescents (41%), and the Xhosa
version by 156 adolescents (17%).
Measures
Self-esteem.
Adolescents’ self-esteem was assessed
using the multidimensional Self-Esteem Questionnaire
(SEQ) developed by DuBois et al. (1996). The measure
consists of 42 items, each of which is rated on a 4-point
scale ranging from strongly disagree to strongly agree.
Each item is scored 1 to 4, with higher values indicating
higher self-esteem. In order to guard against possible
bias associated with response style, ten items are
negatively worded and reverse scored.
The SEQ is divided into six subscales. One of these
contains items directly assessing adolescents’ global
self-worth (e.g., ‘I am happy with myself as a person’).
The remaining subscales assess adolescents’ self-evalu-
ations with respect to five salient contexts or domains of
adolescents’ experience: peers (e.g., ‘I am as popular
with kids my own age as I want to be’), school (e.g., ‘I am
good enough at math’), family (e.g., ‘I am happy with
how much my family loves me’), sports/athletics (e.g., ‘I
am as good at sports/physical activities as I want to be’)
and body image (e.g., ‘I like my body just the way it is’).
The SEQ was selected in preference to other possible
self-esteem measures for several reasons. DuBois
et al.’s (1996) use of an ecological-transactional theor-
etical framework greatly assists in the interpretation of
self-esteem data in relation to various risk behaviours,
and the scale is designed to measure self-esteem in the
domains centrally related to adolescent adaptation and
risk. The measure was also considered to be highly
suitable because it was developed on adolescents in the
age ranges for the current study.
In addition, few other measures of self-esteem have
been subjected to adequate programmes of validation
research, including social desirability bias. DuBois
et al. (1996) provide such data in the form of two studies
that examine the psychometric properties of the Self-
Esteem scale. They found that scores obtained on the
SEQ had good internal consistency (coefficient alphas
for each subscale ranging from .81 to .91) and test–
retest reliability (rs ranging from .74 to .84) for a com-
munity sample of American adolescents. They also
provided evidence for the factorial validity of the sub-
scale structure, and for the SEQ’s convergent and dis-
criminant validity across self-report, interview and
parent-report forms.
Wild, Flisher, Bhana, and Lombard (2002b) invest-
igated the reliability and factorial validity of the SEQ
with two samples of adolescents enrolled in Grade 8
and 11 at schools in Cape Town. Participants were 900
students attending public schools, and 116 students
attending independent (private) schools. Results pro-
vided general support for the 6-factor structure pro-
posed by DuBois et al. (1996) and indicated that the
1456
Lauren G. Wild et al.

SEQ scale scores have good internal consistency
(Cronbach alphas ranging from .75 to .92) and ade-
quate test–retest reliability (Pearson rs ranging from .73
to .83) for English-speaking South Africans. When
Afrikaans and Xhosa translations of the questionnaire
were included in the analyses, internal consistency re-
mained above the minimum level of .70 recommended
for research use (Nunnally & Bernstein, 1994) for all
subscales except the sports/athletics scale (a
¼ .67).
One item (28) which had an item-total correlation of .06
and a nonsignificant factor loading on the sports/ath-
letics self-esteem factor was consequently omitted from
the scale for this study, raising the alpha coefficient for
this scale to an acceptable .73. Since there is no abso-
lute cut-off point to identify ‘low’ self-esteem, we di-
chotomised
self-esteem
scores
by
distinguishing
between those adolescents with scores below the med-
ian in each domain and those with higher scores.
Demographic information and risk behaviours.
The
participants completed a self-report risk questionnaire
containing items about demographic characteristics
and asking about their participation in a range of health
risk behaviours. It included questions about their use of
tobacco, alcohol, cannabis (‘dagga’), solvents and other
substances, bullying, suicidality and sexuality. The full
items used to assess these risk behaviours are included
as an appendix. While it is recognised that these items
do not cover the full range of adolescent risk behaviours
(e.g., extreme eating behaviour, road-related beha-
viour), they were selected because they represent
behaviours that are of particular concern in the popu-
lation under study. The risk behaviours were defined as
clearly as possible to reduce the likelihood of ambiguity,
and the level of language was appropriate for both
Grades 8 and 11. This questionnaire was subject to
extensive pilot testing both in small groups and a
classroom context, and similar versions of this ques-
tionnaire have been used in other school-based epi-
demiological studies in South Africa (Flisher, 1998).
Flisher, Evans, Muller, and Lombard (in press) have
shown that this instrument has an adequate level of
test–retest reliability. Kappa values for the eight indi-
vidual items included in the analysis were moderate to
almost perfect, ranging from 52.0 (for telling someone
they intended to commit suicide) to 85.4 (for having ever
smoked a whole cigarette). It was not possible to cal-
culate kappa coefficients for the remaining seven items,
either because the marginal proportions were not
homogenous or because the prevalence rates were too
low. However, the observed agreement for each of these
items was higher than 92%.
The following health-compromising behaviours were
included as binary outcome measures in this study: (a)
having used alcohol (other than a few sips) in the pre-
vious month; (b) having smoked cigarettes in the pre-
vious month; (c) ever having used any illicit drug or
inhalants; (d) having bullied somebody at school during
the previous 12 months; (e) having been bullied at
school during the previous 12 months; (f) having
thought about committing suicide, threatened to do so,
or attempted to do so in the previous 12 months; (g)
having had more than 2 sexual partners in the previous
12 months, known their most recent partner for less
than 7 days before intercourse, and/or not used any
form of contraception or protection against disease on
the last occasion they had sexual intercourse (risky
sexual behaviour).
Procedure
The questionnaires were translated from English into
Xhosa and Afrikaans, and then back-translated into
English by other people who had these languages as
home language.
The back-translated versions were compared with the
original version, and any discrepancies were resolved
by negotiation between the original translators and
those doing the back-translations. Translated versions
of the questionnaire were then piloted in small groups
and classrooms in order to ensure that the translations
were adequate.
Permission to conduct the study was obtained from
the Western Cape Education Department and the
principals of the selected schools. Questionnaires were
administered in the classroom by members of the re-
search team, and participants were assured that their
responses would be anonymous and confidential. No
members of the school staff were present during the
administration of the questionnaires, and care was
taken to ensure that the students were seated such that
they could not see the responses of their classmates.
Students were informed that they could choose not to
participate in the study as a whole or to omit selected
questions.
Statistical analysis
Preliminary analyses were conducted using the Survey
Data Analysis (SUDAAN) program. We calculated
means and proportions with 95% confidence intervals
(CI’s) taking the multistage stratified design into ac-
count. We used the without replacement design option.
The design stages were postal code area, school and
grade. We computed sampling weights using the num-
ber of students in the school, the number of students in
the grade (in a specific school) and the number of stu-
dents sampled from the grade. We compared the results
for each gender (within each grade) and for each grade
(within each gender). In comparing two groups, if the
95% CI’s do not overlap, there is a significant (p < .025)
difference between the groups. If the CI’s overlap but
not to the extent that the point estimate of one group is
contained within the CI of the other group, there is a
significant (p < .05) difference between the groups. If
they overlap to the extent that the point estimate of one
group is contained within the CI of the other group, we
cannot draw any conclusions as to whether there is a
significant difference between the groups.
The relationships between the independent variables
and the adolescent risk behaviours were investigated
through a series of logistic regression models, using
generalized estimation equations (GEE; Zeger & Liang,
1986) to estimate the model parameters. The GEE ap-
proach takes account of the clustering due to students
being sampled within schools. The binary dependent
variable for each model was modelled with the logit link
function. Results are presented as odds ratios (with
95% Confidence Intervals) that compare the odds
of reporting an outcome for the different levels of a
Self-esteem and adolescent risk behaviours
1457
particular independent variable, all other factors being
held constant. Two sets of regression results are
reported for each of the seven risk behaviour outcomes,
using the following predictor variables: (1) the relevant
self-esteem scale and the covariates of sex, grade and
race; and (2) all the self-esteem scales and demographic
variables. The data were stratified by gender for all
these analyses.
Biases associated with excluding participants with
incomplete responses were reduced by replacing miss-
ing data on the SEQ subscales with the mean of the
participants’ scores on the remaining items in that
subscale, provided that at least one half of the subscale
items had been completed. Following this procedure,
226 adolescents (24%) were still missing data on at
least one variable. Preliminary analyses indicated that
black adolescents were nearly twice as likely as the
reference group of coloureds to be missing data
(p < .01). However, the presence of missing responses
was unrelated to self-esteem or to any of the risk be-
haviours assessed. It was also unrelated to gender,
grade level or the adolescent’s average mark at school in
the previous year. Because the patterns of missing data
appeared to be unrelated to the primary study vari-
ables, listwise deletion procedures were therefore ap-
plied when the outcome or predictor variables were not
completed, resulting in a 4–17% loss in participants per
GEE model employed. Alpha was set at .05 for all
statistical analyses.
Results
Self-esteem subscales
Table 1 presents means and 95% confidence inter-
vals for the SEQ scales, stratified by gender and
grade, and using appropriate sampling weights.
Grade 8 boys scored significantly higher than grade
8 girls on the body image, sports/athletics and glo-
bal self-esteem scales, and Grade 11 boys scored
significantly higher than Grade 11 girls on all sub-
scales except school self-esteem. Grade 8 girls
scored significantly higher than Grade 11 girls on all
the self-esteem scales, and Grade 8 boys scored
significantly higher than Grade 11 boys on the
school self-esteem scale.
Prevalence of risk behaviours
Prevalence rates for the risk behaviours selected as
criterion variables for this study are displayed in
Table 2. Prevalence rates are presented in the form of
percentages (and 95% confidence intervals), strati-
fied by gender and grade and using appropriate
sampling weights. Grade 8 boys were significantly
more likely than Grade 8 girls to report having bul-
lied another student or been bullied at school and
having engaged in risky sexual behaviour, but were
significantly less likely to report suicidal ideation or
behaviour. Smoking, drinking alcohol, using drugs,
bullying another student and risky sexual behaviour
were all significantly more prevalent in Grade 11
boys than Grade 11 girls. However, Grade 11 girls
were more likely than Grade 11 boys to report
suicidal ideation or behaviour.
Grade 11 girls were significantly more likely than
Grade 8 girls to report alcohol and drug use, suicid-
ality, and risky sexual behaviour. Smoking, alcohol
and drug use, risky sexual behaviour and suicidality
were all significantly more common in Grade 11 boys
than Grade 8 boys. However, Grade 11 boys were
significantly less likely than Grade 8 boys to report
having been bullied at school in the previous year.
Associations between self-esteem and risk
behaviours
Peer self-esteem. Odds Ratios (and 95% Confidence
Intervals) between the risk behaviours and the SEQ
scales are presented in Table 3, and displayed
graphically in Figure 1. Odds ratios adjusted for the
clustering according to school, grade and race indic-
ated that for both sexes, individuals who scored be-
low the median on the peer self-esteem scale were
significantly more likely than those with higher self-
Table 1 Means (and 95% Confidence Intervals) for Self-Esteem Questionnaire (SEQ) scale scores, stratified by gender and grade
SEQ scale
Females
Males
Grade 8
Grade 11
Grade 8
Grade 11
n
M (CI)
n
M (CI)
n
M (CI)
n
M (CI)
Peers (8 items)
250
22.18
239
21.14
185
22.83
175
23.68
(21.73–22.63)
(20.68–21.60)
(21.93–23.73)
(23.33–24.03)
School (8 items)
250
21.65
239
19.81
186
21.83
175
20.64
(20.92–22.37)
(19.28–20.33)
(20.90–22.76)
(19.58–21.71)
Family (8 items)
251
23.89
238
23.14
185
24.68
175
25.00
(23.46–24.33)
(22.50–23.78)
(23.74–25.63)
(24.14–25.85)
Body image (4 items)
253
10.75
239
9.89
186
11.95
175
11.69
(10.26–11.24)
(9.44–10.34)
(11.57–12.32)
(11.28–12.10)
Sports/athletics (5 items)
248
12.75
239
11.56
184
14.18
175
14.02
(12.27–13.22)
(11.09–12.02)
(13.67–14.69)
(13.63–14.41)
Global (8 items)
251
22.09
238
21.09
185
23.62
175
23.35
(21.53–22.64)
(20.49–21.68)
(22.86–24.39)
(22.67–24.04)
1458
Lauren G. Wild et al.

esteem in the peer domain to report having been
bullied at school in the previous 12 months. For
girls, low peer self-esteem was also significantly
associated with an increased likelihood of suicidal
ideation or behaviour, and marginally significantly
(p < .06) associated with a decreased likelihood of
risky sexual behaviour.
After controlling for the other self-esteem scales as
well as grade and race, low peer self-esteem was no
longer significantly associated with an increased
likelihood of any of the risk behaviours for either sex.
However, it was independently associated with a
decreased likelihood of cigarette use for both sexes
and of risky sexual behaviour and alcohol use for
girls. There was also a marginally significant
association (p < .06) between low peer self-esteem
and a decreased likelihood of having bullied another
student at school for boys.
School self-esteem. Odds ratios controlling for the
clustering according to school, grade and race indic-
ated that low self-esteem with respect to school was
associated with an increased risk of alcohol and
cigarette use and of suicidality for both sexes, and
with an increased risk of drug use for girls. Boys with
scores below the median on the school self-esteem
scale were also more likely than those with higher
scores on this scale to report having bullied another
student, been bullied, and engaged in risky sexual
behaviour.
After controlling for the other self-esteem scales as
well as the demographic variables, low self-esteem in
the school context remained independently associ-
ated with an increased likelihood of cigarette use and
having been bullied for boys, and was marginally
significantly associated with an increased likelihood
of risky sexual behaviour and having bullied another
student at school. For girls, low school self-esteem
remained independently associated with an in-
creased likelihood of cigarette, drug and alcohol use.
Family self-esteem. After controlling for the clus-
tering of data according to school, grade and race,
low self-esteem in the family context was associated
with an increased likelihood of suicidality, alcohol
use and risky sexual behaviour for both sexes. It was
also associated with an increased likelihood of hav-
ing been bullied at school for boys, and with an in-
creased likelihood of cigarette and drug use for girls.
When the other self-esteem scales were also taken
into account, low family self-esteem was independ-
ently associated with an increased likelihood of sui-
cidality, risky sexual behaviour, and alcohol and
cigarette use for both sexes, and showed a margin-
ally significant association with an increased risk of
drug use for girls.
Body-image self-esteem. After controlling for the
clustering according to school, grade and race, boys
with low self-esteem with respect to their body-image
were significantly more likely to be suicidal and to
have been bullied at school than boys with higher
scores on the body-image self-esteem scale. How-
ever, body-image self-esteem was not independently
related to any of the risk behaviours for boys after
controlling for the other self-esteem scales.
For girls, low self-esteem with respect to body-
image was significantly associated with an increased
likelihood of suicidality, drug, alcohol and cigarette
use and risky sexual behaviour after controlling for
the clustering according to school, grade and race.
After controlling for the other self-esteem scales, girls
with scores below the median on the body image self-
esteem scale remained significantly more likely than
those with higher scores to report drug and cigarette
use, and marginally significantly (p < .06) more
likely to report alcohol use and suicidality.
Sports/athletics self-esteem. Low self-esteem with
respect to sports/athletics was significantly associ-
ated with an increased risk of having been bullied for
boys when the clustering according to school, grade
and race were controlled for. When the other self-
esteem scales were taken into account, low sports/
athletics self-esteem was significantly independently
associated only with a decreased likelihood of
cigarette use in boys.
For girls, low sports/athletics self-esteem was
associated with an increased risk of suicidality,
alcohol use and having been bullied after controlling
for the clustering according to school, grade and
race. However, after controlling for the other self-
esteem scales low sports/athletics self-esteem was
not independently associated with any of the risk
behaviours for girls.
Global self-worth. When the clustering according to
school, grade and race were controlled for, low global
self-worth was significantly associated with an in-
creased likelihood of suicidality in both sexes, of
having been bullied and used alcohol in boys, and of
risky sexual behaviour in girls.
When the other self-esteem scales were taken into
account, however, low global self-esteem did not make
a significant independent contribution to predicting
any of the risk behaviours for boys. Girls with low
Table 2 Prevalence rates (and 95% Confidence Intervals) for
risk behaviours, stratified by gender and grade
Risk
behaviour
Females
Males
Grade 8
M (CI)
Grade 11
M (CI)
Grade 8
M (CI)
Grade 11
M (CI)
Smoke
27 (19–34) 30 (23–37) 28 (20–35) 45 (35–54)
Alcohol
21 (15–26) 32 (24–39) 22 (16–28) 52 (43–62)
Drugs
10 (5–15)
16 (11–20) 12 (9–16)
38 (30–46)
Bullied
16 (11–20) 15 (10–21) 31 (22–40) 28 (20–35)
Been bullied 28 (24–33) 24 (18–31) 45 (37–53) 26 (21–31)
Suicide
30 (24–35) 41 (35–46) 16 (10–21) 25 (20–30)
Risky sex
5 (3–8)
19 (14–24) 18 (12–25) 39 (31–47)
Self-esteem and adolescent risk behaviours
1459

Table 3 Results of generalized estimating equations predicting risk behaviours from self-esteem
SEQ scale
Gender
Risk
behaviour
Adjusted for grade and race
Adjusted for grade, race and
other SEQ scales
n
OR
(95% CI )
n
OR
(95% CI )
Peers (<23)
Male
Smoke
342
.67
(.41–1.09)
339
.35**
(.19–.67)
Alcohol
337
1.37
(.84–2.24)
333
.93
(.51–1.69)
Drugs
348
.87
(.50–1.53)
344
.58
(.29–1.15)
Bullied
336
.82
(.50–1.35)
332
.54
(.29–1.01)
Been bullied
336
1.88**
(1.17–3.01)
332
1.24
(.69–2.21)
Suicide
346
1.70
(.97–3.00)
342
1.04
(.52–2.09)
Risky sex
337
1.34
(.79–2.29)
333
1.05
(.54–2.01)
Female
Smoke
466
.88
(.58–1.35)
463
.56*
(.33–.93)
Alcohol
454
.95
(.62–1.46)
451
.51*
(.30–.86)
Drugs
466
1.25
(.71–2.21)
463
.89
(.46–1.71)
Bullied
458
.96
(.59–1.59)
455
.82
(.46–1.46)
Been bullied
457
1.60*
(1.05–2.43)
454
1.44
(.89–2.34)
Suicide
466
2.19***
(1.47–3.27)
463
1.19
(.74–1.92)
Risky sex
451
.56
(.31–1.01)
448
.25***
(.12–.52)
School (<21)
Male
Smoke
343
2.11**
(1.32–3.37)
339
2.85***
(1.64–4.96)
Alcohol
338
1.61*
(1.00–2.59)
333
1.34
(.77–2.34)
Drugs
349
1.57
(.93–2.65)
344
1.68
(.91–3.09)
Bullied
337
1.64*
(1.00–2.69)
332
1.75
(.99–3.10)
Been bullied
337
2.56***
(1.57–4.17)
332
2.04*
(1.16–3.59)
Suicide
347
1.76*
(1.00–3.10)
342
1.24
(.64–2.39)
Risky sex
338
1.74*
(1.03–2.92)
333
1.83
(.99–3.36)
Female
Smoke
466
2.54***
(1.64–3.93)
463
2.52***
(1.51–4.20)
Alcohol
454
2.37***
(1.52–3.68)
451
2.03**
(1.21–3.41)
Drugs
466
2.45**
(1.37–4.38)
463
2.12*
(1.09–4.13)
Bullied
458
1.33
(.81–2.20)
455
1.30
(.72–2.35)
Been bullied
457
.99
(.65–1.49)
454
.73
(.45–1.18)
Suicide
466
1.95**
(1.32–2.89)
463
.93
(.57–1.49)
Risky sex
451
1.15
(.64–2.08)
448
.76
(.36–1.59)
Family (<24)
Male
Smoke
342
1.51
(.94–2.43)
339
1.82*
(1.03–3.22)
Alcohol
337
2.14**
(1.31–3.49)
333
2.02*
(1.14–3.56)
Drugs
348
1.39
(.81–2.36)
344
1.45
(.78–2.70)
Bullied
336
1.45
(.89–2.38)
332
1.42
(.80–2.52)
Been bullied
336
1.99**
(1.24–2.30)
332
1.34
(.77–2.35)
Suicide
346
2.87***
(1.64–5.05)
342
2.29*
(1.20–4.37)
Risky sex
337
1.84*
(1.09–3.11)
333
2.01*
(1.08–3.71)
Female
Smoke
466
1.84**
(1.20–2.81)
463
1.92*
(1.15–3.18)
Alcohol
454
2.50***
(1.61–3.87)
451
2.72***
(1.60–4.62)
Drugs
466
2.23**
(1.26–3.96)
463
1.94
(1.00–3.76)
Bullied
458
1.29
(.78–2.13)
455
1.15
(.65–2.05)
Been bullied
457
1.10
(.73–1.65)
454
.88
(.55–1.41)
Suicide
466
3.31***
(2.21–4.96)
463
2.23**
(1.41–3.51)
Risky sex
451
2.53**
(1.39–4.61)
448
3.19**
(1.52–6.69)
Body (<11)
Male
Smoke
343
1.01
(.62–1.64)
339
1.02
(.55–1.91)
Alcohol
338
1.32
(.79–2.19)
333
.99
(.53–1.85)
Drugs
349
1.11
(.63–1.95)
344
.95
(.48–1.87)
Bullied
337
1.19
(.72–1.99)
332
1.03
(.55–1.92)
Been bullied
337
1.64*
(1.01–2.68)
332
1.07
(.59–1.95)
Suicide
347
1.88*
(1.07–3.32)
342
1.48
(.74–2.95)
Risky sex
338
1.00
(.57–1.73)
333
.86
(.44–1.71)
Female
Smoke
469
1.88**
(1.22–2.89)
463
1.83*
(1.08–3.12)
Alcohol
457
1.88**
(1.22–2.92)
451
1.67
(.98–2.86)
Drugs
469
2.36**
(1.31–4.25)
463
2.24*
(1.11–4.49)
Bullied
461
1.32
(.80–2.16)
455
1.13
(.63–2.04)
Been bullied
460
1.08
(.71–1.63)
454
.88
(.53–1.44)
Suicide
469
2.53***
(1.71–3.76)
463
1.59
(.99–2.56)
Risky sex
454
1.82*
(1.01–3.29)
448
1.98
(.91–4.27)
Sports (<13)
Male
Smoke
341
.71
(.43–1.20)
339
.49*
(.26–.91)
Alcohol
336
1.03
(.61–1.74)
333
.71
(.38–1.32)
Drugs
347
1.17
(.66–2.08)
344
1.04
(.54–2.02)
Bullied
335
1.29
(.76–2.20)
332
1.07
(.57–2.01)
Been bullied
335
1.71*
(1.03–2.84)
332
.96
(.52–1.78)
Suicide
345
1.60
(.89–2.87)
342
.93
(.47–1.84)
Risky sex
336
.78
(.43–1.39)
333
.58
(.29–1.16)
Female
Smoke
464
1.36
(.88–2.11)
463
1.10
(.65–1.86)
Alcohol
452
1.69*
(1.08–2.63)
451
1.46
(.86–2.49)
1460
Lauren G. Wild et al.

global self-worth were more likely to report sui-
cidal ideation or behaviours than girls with higher
global self-esteem scores, but were less likely to
report smoking and (marginally significantly) using
alcohol.
Discussion
This study aimed to explore associations among
adolescents’ self-esteem in the context of peers,
school, family, sports/athletics and body image,
feelings of global self-worth, and risk behaviours
related to substance use, bullying, suicidality and
sexuality. Results indicated that after controlling for
the clustering according to school, grade and race,
scores on each self-esteem scale were significantly
associated with at least one risk behaviour in male
and female adolescents. However, specific domains
of self-esteem were differentially related to particular
risk behaviours.
Low global self-esteem was significantly associated
with an increased likelihood of suicidality in both
sexes, of having been bullied and used alcohol in
boys, and of risky sexual behaviour in girls after
controlling for the clustering of schools, grade, and
race. These findings provide some support for sev-
eral recent cross-sectional and prospective studies
conducted in North America, Europe and Austral-
asia which have linked low self-esteem (assessed as
a global, unidimensional measure) with risk behav-
iours such as suicidality (Neumark-Sztainer et al.,
1997; Vella et al., 1996; Yoder, 1999) and substance
abuse (Gordon & Caltabiano, 1996), including a
greater frequency and quantity of alcohol use and
problem drinking (Scheier et al., 2000).
In contrast to some of these studies, however
(Carvajal et al., 2000; Ho
¨fler et al., 1999; Howard &
Jenson, 1999; Howard et al., 1999), we did not find
any significant associations between global self-
esteem and an increased likelihood of cigarette or
drug use for either sex. Moreover, when the corre-
lations between global self-worth and the other self-
esteem scales were taken into account, low global
self-worth did not make a significant independent
contribution to predicting any of the risk behav-
iours in boys. For girls, it was independently asso-
ciated only with an increased risk of suicidality and
a decreased risk of cigarette and (marginally signi-
ficantly) alcohol use.
This does not mean that self-esteem is unimpor-
tant in predicting adolescent risk behaviours. Ra-
ther, the results of this study suggest that different
risk behaviours are more strongly related to certain
domains of self-esteem than others. Overall, the
findings of this study suggest that low self-esteem
with respect to family and school are the most per-
tinent predictors of risk behaviours in adolescents.
After controlling for the clustering according to
school, grade and race and the other self-esteem
scales, low family self-esteem was independently
associated with an increased likelihood of suicid-
ality, risky sexual behaviour, and alcohol and
cigarette use for both sexes, and with a marginally
significant increased risk of drug use for girls. This
finding is interesting in light of the widespread
assumption that peer relationships increasingly re-
place family relationships in adolescence, at least in
Western societies (Grotevant, 1998). However, it is
consistent with a body of recent theory and research
which recognizes that while time spent with family
Table 3 Continued
SEQ scale
Gender
Risk
behaviour
Adjusted for grade and race
Adjusted for grade, race
and other SEQ scales
n
OR
(95% CI )
n
OR
(95% CI )
Drugs
464
1.03
(.58–1.82)
463
.61
(.31–1.21)
Bullied
456
.88
(.53–1.47)
455
.73
(.40–1.33)
Been bullied
455
1.59*
(1.04–2.43)
454
1.52
(.93–2.47)
Suicide
464
2.04**
(1.36–3.06)
463
1.15
(.71–1.87)
Risky sex
449
1.21
(.66–2.20)
448
1.18
(.55–2.52)
Global (<22)
Male
Smoke
343
1.37
(.84–2.21)
339
1.45
(.75–2.78)
Alcohol
337
1.65*
(1.01–2.71)
333
1.26
(.66–2.40)
Drugs
348
1.26
(.73–2.19)
344
1.15
(.55–2.41)
Bullied
336
1.32
(.80–2.19)
332
1.15
(.60–2.18)
Been bullied
336
2.10**
(1.29–3.41)
332
1.28
(.69–2.40)
Suicide
346
2.02*
(1.15–3.55)
342
1.06
(.50–2.25)
Risky sex
336
1.17
(.68–2.02)
333
.89
(.44–1.80)
Female
Smoke
466
1.10
(.72–1.67)
463
.52*
(.29–.93)
Alcohol
454
1.31
(.86–2.01)
451
.57
(.32–1.02)
Drugs
466
1.60
(.92–2.81)
463
.77
(.36–1.63)
Bullied
458
1.36
(.83–2.24)
455
1.30
(.68–2.46)
Been bullied
457
1.42
(.95–2.14)
454
1.35
(.81–2.26)
Suicide
466
3.36***
(2.24–5.04)
463
1.85*
(1.12–3.06)
Risky sex
451
2.14*
(1.17–3.90)
448
1.74
(.78–3.91)
Note: OR
¼ odds ratio; CI ¼ confidence interval. All odds ratios are adjusted for the clustering of data according to school.
p < .06; *p < .05; **p < .01; ***p < .001.
Self-esteem and adolescent risk behaviours
1461
typically decreases during adolescence and that
spent with friends increases, family relationships
remain important, and are significantly associated
with adolescents’ emotional health and competent
behaviour (e.g., Sweeting, West, & Richards, 1998;
for a review see Grotevant, 1998).
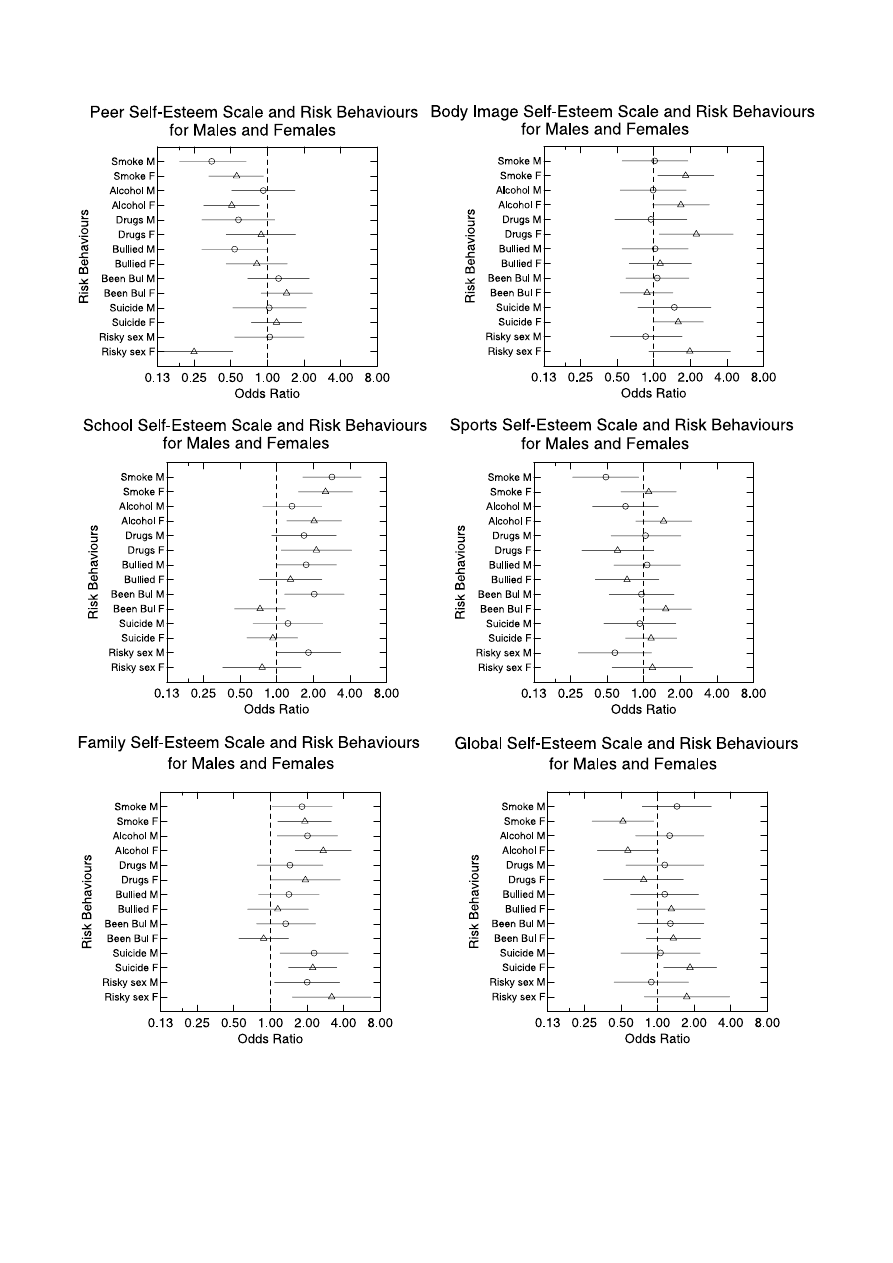
Figure 1 Odds ratios for males and females adjusted for clustering according to school, grade, race and other SEQ
scales
1462
Lauren G. Wild et al.

After controlling for the other self-esteem scales as
well as the demographic variables, low school self-
esteem remained independently associated with an
increased likelihood of cigarette use and having been
bullied for boys, and was marginally significantly
associated with an increased likelihood of risky
sexual behaviour and having bullied another stu-
dent at school. For girls, low school self-esteem re-
mained independently associated with an increased
likelihood of cigarette, drug and alcohol use. This
finding contrasts with McGee and Williams’ (2000)
study, in which academic self-esteem assessed in
preadolescence was unrelated to risk behaviour at
age 15 amongst adolescents in New Zealand. On the
other hand, it is consistent with Kawabata et al.’s
(1999) finding of an association between lower per-
ceived cognitive competence and ever having smoked
for young Japanese adolescents. Although the
reasons for these differences are unclear, it may be
that academic or school self-esteem is more closely
associated with current rather than future risk
behaviours, or that school self-esteem becomes a
stronger predictor of risk behaviour in adolescence
(when academic performance is often salient and
associated with class placement, selection of courses
and future career plans) than is the case in preado-
lescence. Alternatively, the strength of these associ-
ations may be affected by cultural variations in the
meaning and importance given both to academic
achievement and to the use of various psychoactive
substances in different countries.
When the other self-esteem scales were controlled
for, low self-esteem with respect to body-image did
not make a significant independent contribution to-
wards explaining any of the risk behaviours for boys,
but was significantly associated with an increased
likelihood of cigarette and drug use for girls, and
marginally significantly associated with alcohol use
and suicidality. This finding is consistent with evid-
ence that female adolescents react more negatively to
increases in body fat and weight gain and are typic-
ally more dissatisfied with their appearance than are
males (Harter, 1998). According to Harter, this
probably reflects the fact that although society and
the media tend to emphasise the importance of
physical attractiveness for both sexes, standards
regarding desirable bodily characteristics (such as
thinness) are particularly narrow and unrealistic for
women.
In contrast to the general pattern of results linking
low self-esteem with an increased likelihood of risk
behaviours, low self-esteem in some domains was
associated with a decreased likelihood of risk
behaviours when the remaining self-esteem scales
were held constant. Low peer self-esteem was inde-
pendently associated with a decreased likelihood of
cigarette use for both sexes and of risky sexual
behaviour and alcohol use for girls. There was also a
marginally significant association (p < .06) between
low peer self-esteem and a decreased likelihood of
having bullied another student at school for boys.
Low sports/athletics self-esteem was also associated
with a decreased likelihood of smoking in boys, while
low global self-worth was independently associated
with a decreased risk of cigarette and (marginally
significantly) alcohol use in girls.
One possible explanation for this apparent pro-
tective effect of low self-esteem in some domains is
that given equivalent levels of self-esteem with re-
spect to domains such as the school and family,
adolescents who are lower in self-esteem, and par-
ticularly those who perceive themselves as less
accepted by their peer group, may be less likely to
spend time with peers and to become involved in
romantic partnerships. They may therefore be less
likely to experience opportunities, temptation or
pressure to engage in behaviours such as smoking,
drinking and sexual intercourse. This explanation
would be consistent with West and Sweeting’s (1997)
finding that although global self-esteem was unre-
lated to risk behaviours in Glaswegian 15-year-olds,
adolescents who spent more time in unsupervised,
‘street-oriented’ peer activities were more likely to
smoke, drink, have used drugs and to be more sex-
ually experienced than their peers who were not in-
volved in this lifestyle. An alternative possibility (also
suggested by West & Sweeting, 1997) is that if be-
haviours such as smoking, drinking, sexual inter-
course and even bullying peers are valued or
admired by the peer group, engaging in these beha-
viours and adopting an identity as a ‘rebel’ may
actually increase adolescents’ self-esteem, partic-
ularly in the peer domain.
This raises an important limitation of the study
that must be taken into account when interpreting
the results. Although the analyses provide evidence
that certain domains of self-esteem are associated
with adolescent risk behaviours, the cross-sectional
nature of the data means that we cannot infer
causal or even temporal relationships among these
variables. It may be that in at least some cases,
adolescents’ risk behaviours affect their self-esteem
in particular domains as well as vice versa. For
example, substance use may lead to conflict with
parents and school authorities and to poorer aca-
demic performance at school, and hence to lower
feelings of self-esteem in these domains. Prospect-
ive, longitudinal studies in which measures of self-
esteem are taken prior to the risk behaviours in
question would be better equipped to examine the
direction of effect.
A second caveat with respect to these results is
that they were based on information provided by the
adolescent only. This raises the possibility that some
of the findings may be overstated because of shared
method variance. Although adolescents are likely to
be the most reliable reporters of both their feelings of
self-esteem and their risk behaviours, further re-
search obtaining information from multiple sources
would help to boost confidence in these results.
Self-esteem and adolescent risk behaviours
1463

A further limitation of this study is that the
measures of risk behaviour used do not take the
quantity or severity of the risk behaviour into ac-
count. For example, the measure of alcohol use
made no distinction between drinking that may be
normative and that which constitutes a health risk.
Similarly, the suicidality index did not distinguish
between adolescents who had made serious and life-
threatening attempts, youngsters whose attempts
are very mild or of limited lethality potential, and
those who have thought or talked about committing
suicide, but never actually attempted to do so.
Buster and Rodgers (2000) reported that self-esteem
accounted for a significant proportion of the variance
in heavy drinking behaviour in adolescents, but was
not significantly associated with light drinking.
Thus, future research is needed to examine the
possibility of differential relationships between self-
esteem and different levels of the risk behaviours
included in this study. Further research is also
needed to determine whether there is a cut-off point
beyond which changes in self-esteem are no longer
associated with increased risk or protection, in order
to determine which adolescents should be targeted
in intervention programmes.
Finally, it is important to note that low self-esteem
alone is unlikely to provide an adequate aetiological
explanation for the range of risk behaviours adoles-
cents may engage in. As Jessor (1991) argues, any
complete and responsible explanation of adolescent
risk behaviour needs to be complex, and to incor-
porate multiple domains (for example, the social
environment, the perceived environment, biology/
genetics, personality and [other] behaviour) as well
as their interactions. Moreover, this research was
conducted in the Cape Town metropolitan area, and
black adolescents may have been underrepresented
in the sample. As a result, generalisations to ado-
lescents in rural areas, other parts of South Africa
and other countries must be made with appropriate
caution.
Despite these caveats, this study has made a sig-
nificant contribution to the research literature in
demonstrating that investigating links between spe-
cific domains of self-esteem and adolescent risk
behaviours is likely to provide information that
cannot be obtained from global measures of self-
worth alone. First, it has shown that the likelihood of
adolescents engaging in a particular risk behaviour
(e.g., smoking cigarettes) may increase with low self-
esteem in particular domains (e.g., family and
school) and decrease with low self-esteem in other
areas (e.g., peers). Second, it has shown that the
links between self-esteem domains and risk behav-
iours may vary to some extent according to gender,
with body-image and global self-worth being inde-
pendent predictors of risk behaviours among girls,
but not boys. These findings are not only of theor-
etical interest, but have important implications for
designing effective interventions aimed at preventing
adolescents
from
adopting
dysfunctional
risk
behaviours.
Risky sexual behaviour among adolescents is of
particular concern in South Africa, as it contributes
towards the high prevalence of HIV/AIDS: data from
a national antenatal prevalence survey conducted in
1999 estimated that 16.5% of South African women
under the age of 20 were infected with HIV (Dickson-
Tetteh & Ladha, 2000). Previous research has found
that low self-esteem (assessed as a global construct)
may undermine abstinence, monogamy and condom
use amongst South African youth (for a review, see
Eaton, Flisher, & Aarø, 2003). The findings of this
study suggest that low self-esteem in the family
context is a stronger correlate of risky sexual beha-
viour for both boys and girls than low global self-
worth or low self-esteem in other domains. Improv-
ing the relationships and communication between
adults and adolescents in the home may therefore
have a role to play in helping to reduce sexual risk
behaviour amongst young people. Although current
interventions aimed at reducing the rates of HIV
infection pay little attention to the home setting, the
potential utility of targeting the family as a whole in
prevention programmes is supported by other re-
search reporting that many South African adoles-
cents experience poor communication with parents
about sexual matters, which in turn may contribute
to unsafe sexual behaviour (Eaton et al., 2003).
Overall, the results of this study suggest that
interventions that aim to protect adolescents from
engaging in risk behaviours by increasing their self-
esteem are likely to be most effective and cost-effi-
cient if they are aimed at the family and school do-
mains. Attempts to raise adolescents’ self-esteem by
providing them with opportunities and encourage-
ment to excel in other areas such as sports or peer
relationships may have several benefits for adoles-
cents, but the findings of this research suggest that
reducing the likelihood of engaging in risk behav-
iours is unlikely to be one of them.
Author notes
Lauren G. Wild and Alan J. Flisher, Department of
Psychiatry and Mental Health; Arvin Bhana, Child,
Youth and Family Development; Carl Lombard,
Biostatistics Unit.
Acknowledgements
Financial support for this research was provided by
the WHO Programme on Substance Abuse, the Uni-
ted Nations Development Programme, the South
African Medical Research Council, and the Medical
Faculty Research Committee of the University of
Cape Town. The authors would like to thank the
Western Cape Education Department, the prin-
cipals, staff and students of the schools that parti-
1464
Lauren G. Wild et al.
cipated in the study, Janet Evans and Lisa Wegner
for assistance with the fieldwork, and Martie Muller
for her contributions to data management.
Correspondence to
Lauren G. Wild, Department of Psychology, Univer-
sity of Cape Town, Rondebosch, 7701, South Africa;
Fax: (+2721) 650 4104; Email: lwild@humanities.
uct.ac.za
References
Abernathy, T.J., Massad, L., & Romano-Dwyer, L.
(1995). The relationship between smoking and self-
esteem. Adolescence, 30, 899–907.
Baumeister, R.F. (1990). Suicide as escape from self.
Psychological Review, 97, 90–113.
Beautrais, A.L., Joyce, P.R., & Mulder, R.T. (1999).
Personality traits and cognitive styles as risk factors
for serious suicide attempts among young people.
Suicide and Life-Threatening Behavior, 29, 37–47.
Berry, E.H., Shillington, A.M., Peak, T., & Hohman,
M.M. (2000). Multi-ethnic comparison of risk and
protective factors for adolescent pregnancy. Child and
Adolescent Social Work Journal, 17, 79–96.
Buster, M.A., & Rodgers, J.L. (2000). Genetic and
environmental influences on alcohol use: DF analysis
of NLSY kinship data. Journal of Biosocial Science, 32,
177–189.
Carvajal, S.C., Wiatrek, D.E., Evans, R.I., Knee, C.R.,
& Nash, S.G. (2000). Psychosocial determinants of
the onset and escalation of smoking: Cross-sec-
tional
and
prospective
findings
in
multiethnic
school samples. Journal of Adolescent Health, 27,
255–265.
Coopersmith, S. (1967). The antecedents of self-esteem.
San Francisco: Freeman.
Dickson-Tetteh, K., & Ladha, S. (2000). Youth health.
In A. Ntuli, N. Crisp, E. Clarke, & P. Barron (Eds.),
South African health review 2000. Durban: Health
Systems Trust.
DuBois, D., Felner, R.D., Brand, S., Phillips, R.S.C., &
Lease, A.M. (1996). Early adolescent self-esteem: A
developmental-ecological framework and assessment
strategy. Journal of Research on Adolescence, 6, 543–
579.
Eaton, L., Flisher, A.J., & Aarø, L. (2003). Unsafe sexual
behaviour in South African youth. Social Science and
Medicine, 56, 149–165.
Ellison, G.T.H., De Wet, T., Ijsselmuiden, C.B., &
Richter, L. (1996). Desegregating health statistics
and health research in South Africa. South African
Medical Journal, 86, 1257–1262.
Flisher, A.J. (1998). Guiding aspirations of epidemio-
logical research in adolescent risk behaviour in the
Department of Psychiatry, University of Cape Town.
Southern African Journal of Child and Adolescent
Mental Health, 10, 140–154.
Flisher, A.J., Evans, J., Muller, M., & Lombard, C. (in
press). Test–retest reliability of self-reported adoles-
cent risk behavior. Journal of Adolescence.
Flisher, A.J., Ziervogel, C.F., Chalton, D.O., Leger,
P.H., & Robertson, B.A. (1996). Risk-taking beha-
viour of Cape Peninsula high-school students: Part
IX. Evidence for a syndrome of adolescent risk
behaviour.
South
African
Medical
Journal,
86,
1090–1093.
Gordon, W.R., & Caltabiano, M.L. (1996). Urban–rural
differences
in
adolescent
self-esteem,
leisure
boredom, and sensation-seeking as predictors of
leisure-time usage and satisfaction. Adolescence,
31, 883–901.
Grotevant, H.D. (1998). Adolescent development in
family contexts. In N. Eisenberg (Ed.), Handbook of
child psychology (5th edn): Vol. 3. Social, emotional
and personality development (pp. 1097–1149). New
York: John Wiley & Sons.
Harter, S. (1998). The development of self-representa-
tions. In N. Eisenberg (Ed.), Handbook of child
psychology (5th edn): Vol. 3. Social, emotional and
personality development (pp. 553–617). New York:
John Wiley & Sons.
Hockaday, C., Crase, S.J., Shelley, M.C. II, & Stockdale,
D.F. (2000). A prospective study of adolescent preg-
nancy. Journal of Adolescence, 23, 423–438.
Ho
¨fler, M., Lieb, R., Perkonigg, A., Schuster, P., Sonn-
tag, H., & Wittchen, H.-U. (1999). Covariates of
cannabis use progression in a representative popula-
tion sample of adolescents: A prospective examina-
tion of vulnerability and risk factors. Addiction, 94,
1679–1694.
Howard, M.O., & Jenson, J.M. (1999). Inhalant use
among antisocial youth: Prevalence and correlates.
Addictive Behaviors, 24, 59–74.
Howard, M.O., Walker, R.D., Walker, P.S., Cottler, L.B.,
& Compton, W.M. (1999). Inhalant use among urban
American Indian youth. Addiction, 94, 83–95.
Jang, S.J., & Thornberry, T.P. (1998). Self-esteem,
delinquent peers, and delinquency: A test of the
self-enhancement
thesis.
American
Sociological
Review, 63, 586–598.
Jessor, R. (1991). Risk behavior in adolescence: A
psychosocial
framework
for
understanding
and
action. Journal of Adolescent Health, 12, 597–605.
Jessor, R., Van den Bos, J., Vanderryn, J., Costa, F.M.,
& Turbin, M.S. (1995). Protective factors in adoles-
cent problem behavior: Moderator effects and devel-
opmental change. Developmental Psychology, 31,
923–933.
Kaplan, H.B. (1975). Self-attitudes and deviant behav-
ior. Pacific Palisades, CA: Goodyear.
Kawabata, T., Cross, D., Nishioka, N., & Shimai, S.
(1999). Relationship between self-esteem and smok-
ing behavior among Japanese early adolescents:
Initial results from a three-year study. Journal of
School Health, 69, 280–284.
Kingsbury, S., Hawton, K., Steinhardt, K., & James, A.
(1999). Do adolescents who take overdoses have
specific psychological characteristics? A comparative
study with psychiatric and community controls.
Journal of the American Academy of Child and
Adolescent Psychiatry, 38, 1125–1131.
Koval, J.J., & Pederson, L.L. (1999). Stress-coping and
other psychosocial risk factors: A model for smoking
in Grade 6 students. Addictive Behaviors, 24, 207–
218.
Self-esteem and adolescent risk behaviours
1465

Koval, J.J., Pederson, L.L., Mills, C.A., McGrady, G.A.,
& Carvajal, S.C. (2000). Models of the relationship of
stress, depression, and other psychosocial factors to
smoking behavior: A comparison of a cohort of
students in Grades 6 and 8. Preventive Medicine,
30, 463–477.
McGee, R., & Williams, S. (2000). Does low self-esteem
predict health compromising behaviors among ado-
lescents? Journal of Adolescence, 23, 569–582.
Neumark-Sztainer, D., Story, M., French, S.A., &
Resnick, M.D. (1997). Psychosocial correlates of
health compromising behaviors among adolescents.
Health Education Research, 12, 37–52.
Nunnally, J.C., & Bernstein, I.H. (1994). Psychometric
theory (3rd edn). New York: McGraw-Hill.
Paul, C., Fitzjohn, J., Herbison, P., & Dickson, N.
(2000). The determinants of sexual intercourse before
age 16. Journal of Adolescent Health, 27, 136–147.
Pitka
¨nen, T. (1999). Problem drinking and psycholo-
gical well-being: A five-year follow-up study from
adolescence to young adulthood. Scandinavian Jour-
nal of Psychology, 40, 197–207.
Poikolainen, K., Tuulio-Henriksson, A., Aalto-Seta
¨la
¨, T.,
Marttunen, M., & Lo
¨nnqvist, J. (2001). Predictors of
alcohol intake and heavy drinking in early adulthood:
A 5-year follow-up of 15–19-year-old Finnish adoles-
cents. Alcohol and Alcoholism, 36, 85–88.
Roberts, R.E., Roberts, C.R., & Chen, Y.R. (1998).
Suicidal thinking among adolescents with a history
of attempted suicide. Journal of the American Aca-
demy of Child and Adolescent Psychiatry, 37, 1294–
1300.
Rosenberg, M. (1979). Conceiving the self. New York:
Basic Books.
Scheier, L.M., Botvin, G.J., Griffin, K.W., & Diaz, T.
(2000). Dynamic growth models of self-esteem and
adolescent alcohol use. Journal of Early Adolescence,
20, 178–209.
Statistics South Africa (2003). Census 2001 databases.
[On-line]. Retrieved October 10, 2003, from http://
www.statssa.gov.za/SpecialProjects/Census2001/
Census/Database/Census%202001/Municipality%20
Level/Persons/Persons.asp.
Sweeting, H., West, P., & Richards, M. (1998). Teenage
family life, lifestyles and life chances: Associations
with family structure, conflict with parents and joint
family activity. International Journal of Law, Policy
and the Family, 12, 15–16.
Vella, M.L., Persic, S., & Lester, D. (1996). Does self-
esteem predict suicidality after controls for depres-
sion? Psychological Reports, 79, 1178.
West, P., & Sweeting, H. (1997). ‘Lost souls’ and ‘rebels’:
A challenge to the assumption that low self-esteem
and unhealthy lifestyles are related. Health Educa-
tion, 5, 161–167.
Wild, L.G., Flisher, A.J., Bhana, A., & Lombard, C.
(2002a). Reliability of the Self-Esteem Questionnaire
for use with South African adolescents (Abstract).
South African Journal of Psychiatry, 8, 50–51.
Wild, L.G., Flisher, A.J., Bhana, A, & Lombard, C.
(2002b). Self-esteem and risk behaviours in South
African adolescents (Abstract). South African Journal
of Psychiatry, 8, 51.
World Health Organization (WHO). (1993). The health of
young people: A challenge and a promise. Geneva:
Author.
Yoder, K.A. (1999). Comparing suicide attemptors,
suicide ideators, and nonsuicidal homeless and
runaway adolescents. Suicide and Life-Threatening
Behavior, 29, 25–36.
Zeger, S.L., & Liang, K.Y. (1986). Longitudinal data
analysis for discrete and continuous outcomes. Bio-
metrics, 42, 121–130.
Manuscript accepted 23 October 2003
Appendix: Items assessing risk behaviours
This part of the questionnaire is concerned with the use of tobacco, alcohol, and other drugs.
1.
Have you ever smoked a whole cigarette?
IF YES:
a.
How old were you when you smoked a whole cigarette for the first time?
b.
In the past year have you smoked a whole cigarette?
c.
During the past month, on how many days did you smoke cigarettes?
d.
During the past month, on the days you smoked, how many cigarettes did you smoke per day?
2.
Have you ever used alcohol (including beer and wine), other than a few sips?
IF YES:
a.
How old were you when you used alcohol for the first time, other than a few sips?
b.
In the past year, did you use alcohol other than a few sips?
c.
During the past month, on how many days did you have at least one drink of alcohol?
d.
During the past 14 days, on how many days did you have 5 or more drinks on one occasion?
3.
Have you ever smoked dagga on its own?
IF YES:
a.
How old were you when you smoked dagga on its own for the first time?
b.
In the past year, did you smoke dagga on its own?
c.
During the past month, on how many days did you smoke dagga on its own?
4.
Have you ever smoked dagga and Mandrax together (‘white pipes’, ‘buttons’)?
IF YES:
1466
Lauren G. Wild et al.

a.
How old were you when you smoked dagga and Mandrax together for the first time?
b.
In the past year, did you smoke dagga and Mandrax together?
c.
During the past month, on how many days did you smoke dagga and Mandrax together?
5.
Have you ever sniffed glue, petrol or thinners?
IF YES:
a.
How old were you when you sniffed glue, petrol or thinners for the first time?
b.
In the past year, did you sniff glue, petrol or thinners?
c.
During the past month, on how many days did you sniff glue, petrol or thinners?
6.
Have you ever used crack cocaine?
IF YES:
a.
How old were you when you used crack cocaine for the first time?
b.
In the past year, did you ever use crack cocaine?
c.
During the past month, on how many days did you use crack cocaine?
7.
Have you ever used Ecstasy?
IF YES:
a.
How old were you when you used Ecstasy for the first time?
b.
In the past year, did you ever use Ecstasy?
c.
During the past month, on how many days did you use Ecstasy?
8.
Have you ever used any other type of illegal drug, such as cocaine, heroin, stimulants, hallucinogenics
such as LSD, Nexus, MMDA?
9.
Have you ever injected any illegal drug (i.e., mainlining)?
This part of the questionnaire is concerned with other things that some young people may do that may harm
their health.
10. During the past 12 months, have you bullied anybody at school?
11. During the past 12 months, have you ever been bullied at school?
12. During the past 12 months, did you ever seriously think about harming yourself in a way that may result
in your death?
13. During the past 12 months, did you ever tell someone that you intend putting an end to your life?
14. During the past 12 months, did you actually ever try to put an end to your life?
IF YES:
Did any attempt result in injury, poisoning, or overdose that had to be treated by a doctor or nurse?
15. Have you ever had sexual intercourse? [This means intimate contact with someone of the opposite sex
during which the penis enters the vagina (female private parts)]
IF YES:
a.
How old were you when you first had sexual intercourse?
b.
With how many different partners have you had sexual intercourse in the last 12 months?
c.
How long ago did you last have sexual intercourse?
d.
On the last occasion that you had sexual intercourse, had you known your partner for more than 7 days?
e.
On the last occasion that you had sexual intercourse, did you or your partner use anything to prevent
pregnancy (family planning) or prevent disease?
f.
On the last occasion that you had sexual intercourse, if you did do anything to prevent pregnancy (family
planning) or disease, what did you or your partner use? (Indicate more than one if necessary)
Condom (‘rubber’)
Injection
Contraceptive pill (‘the pill’)
Cap or diaphragm
Spermicidal gel or foam
IUCD, IUD, ‘Copper T’, loop
Withdrawal, coitus interruptus
Self-esteem and adolescent risk behaviours
1467
Wyszukiwarka
Podobne podstrony:
Variations in Risk and Treatment Factors Among Adolescents Engaging in Different Types of Deliberate
Risk for suicide attempts among adolescents who engage in NSSI
Association between cancer screening behavior and family history among japanese women
The Epidemiology and Phenomenology of NSSI Behaviour Among Adolescents A Critical Review of the Lit
grodzicka bww do wstępu
Pytania z zerówki do Wstępu do psychologii
opis do wstępu
do franszyz wazne
DO DRUKU WAZNE MEGA
Do wstępu, dane z 2003
odp na egz do Gauzy, Ważne dla sudenta, Studia pedagogika
grodzicka bww do wstępu
Kody do Gothic 3 WAŻNE NIE WYRZUCAĆ !!!
Orthognata itp sysmteatyka do wstepu
Associated Press chce wykorzystać algorytmy do automatycznego tworzenia artykułów
Delay in diphtheria, pertussis, tetanus vaccination is associated with a reduced risk of childhood a
więcej podobnych podstron