Tolerance and
Tolerance and
regulation
regulation
of immune response.
of immune response.
Consequences in
Consequences in
immunopathology.
immunopathology.
Joanna Makowska
Monika Jędrzejczak
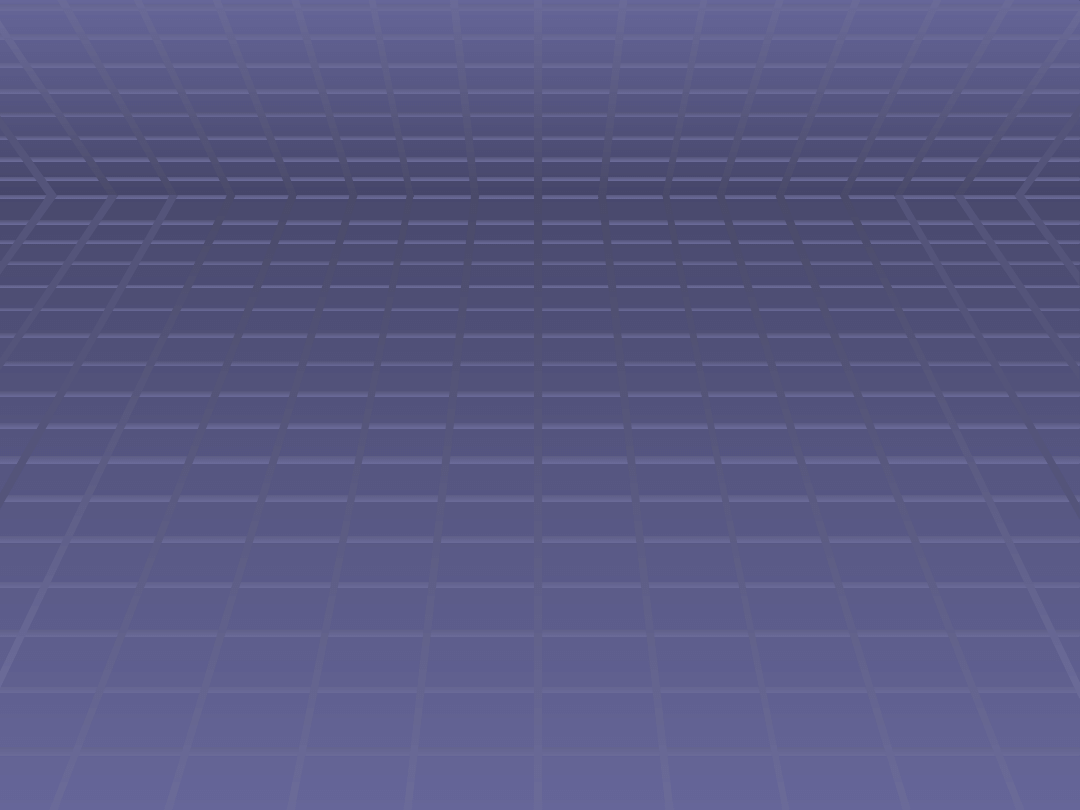
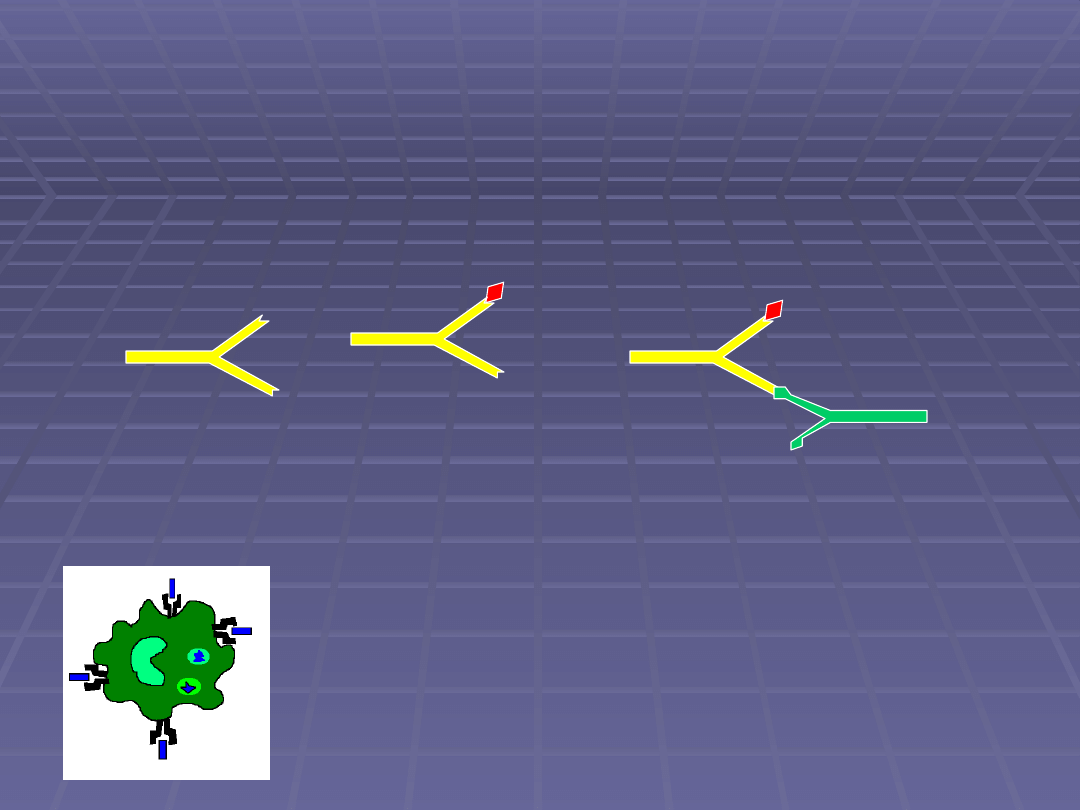
Cellular response
Cellular response
Time from exposition to allergen
T-
d
e
p
e
n
d
e
n
t
re
s
p
o
n
s
e
i
n
te
n
s
it
y
limphocytes T expansion
limphocytes T activation
Apoptosis
activation
Humoral response - IgE
Humoral response - IgE
synthesis
synthesis
B
Y
Th2
Ag
B
Y
CD4
TCR
CD40L
IL4
IL13
MC
IL4
APC
MHC II
CD21 IL4R
CD21
FcERII
CD40
IgM
IgE
Plazmocyt
Y
Y
Y
Y
Y
Y
Y
B
B
B
B
Th
CD40
CD40L
B
Activation
proliferation and
differatiation
HUMORAL
RESPONSE
Il-4
IL-2
IL-5
Cells cooperation in immune
Cells cooperation in immune
response
response
Humoral
Humoral
Lymph Th2 (MHC II)
Lymph Th2 (MHC II)
Surface molecules
Surface molecules
Cytokines (mostly
Cytokines (mostly
Th2)
Th2)
Cellular
Cellular
Lymph Th1
Lymph Th1
Macrofages
Macrofages
Lymph cytotoxic
Lymph cytotoxic
Immunological reaction
Immunological reaction
to antigens has ability to
to antigens has ability to
self-limitation and
self-limitation and
disappears in parallel
disappears in parallel
with antigen elimination
with antigen elimination
and immunological
and immunological
system comes back
system comes back
to its balance.
to its balance.
Regulation
Regulation
Costimulating molecules
Costimulating molecules
Anti-idiotypic antibodies
Anti-idiotypic antibodies
Soluble cytokines receptors
Soluble cytokines receptors
T reg lymphocytes
T reg lymphocytes
CELLULAR RESPONSE
CELLULAR RESPONSE
Against intracellular microorganisms
Against intracellular microorganisms
Against neoplasmatic cells
Against neoplasmatic cells
Th cytokines activity
Th cytokines activity
Tc activity (mostly CD8+, MHC I)
Tc activity (mostly CD8+, MHC I)
CELLULAR RESPONSE
CELLULAR RESPONSE
Develops 24-48 h = late response
Develops 24-48 h = late response
Early response – 2 h
Early response – 2 h
(many cells –
(many cells –
lymphocytes,
lymphocytes,
macrofages
macrofages
produce factors –
produce factors –
RANTES, MCP-1, MCP-2, MIP-
RANTES, MCP-1, MCP-2, MIP-
1
1
α
α
inducing histamine release by mast
inducing histamine release by mast
cells)
cells)
Response amplification – cellular
Response amplification – cellular
infiltration
infiltration
Immature lymphocyte T
APC
CD28
CD80/CD86
For lymphocyte T activation 2 signals are needed:
MHCII- antigen-TCR binding
Costimualtory proteins CD28 and CD80/CD86 binding
TCR
MHCII
antigen
APC
CD28
CD80/CD86
Lymphocyt T produces IL-2 and IL-2 receptor expression appears
IL-2
Immature lymphocyte T
APC
CD80/CD86
Immature lymphocyte T
CD28 expression downregulation on activated lymphocyte T
Immature lymphocyte T
APC
Ligand for CD80/CD86 -
CTLA4
increased expression on activated
lymphocytes T.
This molecule is responsible for inhibitory signal transmition.
Lymphocyte T activation is inhibited.
CD80/CD86
CTLA4
ANERGY
T reg
T reg
Treg constutively produced
Treg induced
• CD4+CD25+
•FOXP3 molecule expression
•CTLA4 expression on cell
surface
•Supression effect by direct
contact
• Activated lymphocytes T
may inhibit unspecificaly
• IL10, TGFβ, IL9 production
Tr1
Tr1
Th3
Th3
•IL10
induction
• high amount
in bowels
•
TGF
TGF
β
β
induction
induction
•
high amount in
bowels
Anti-antibodies
Anti-antibodies
antigen
Antigen appearance in the body
Antibody can also be immunogenic
Giving antibody from one to other organism may produce anti-antibody
antibody
Anti-antibodies
Anti-antibodies
Reumatologic factors
Reumatologic factors
Anti-idiotypic antibody
Anti-idiotypic antibody
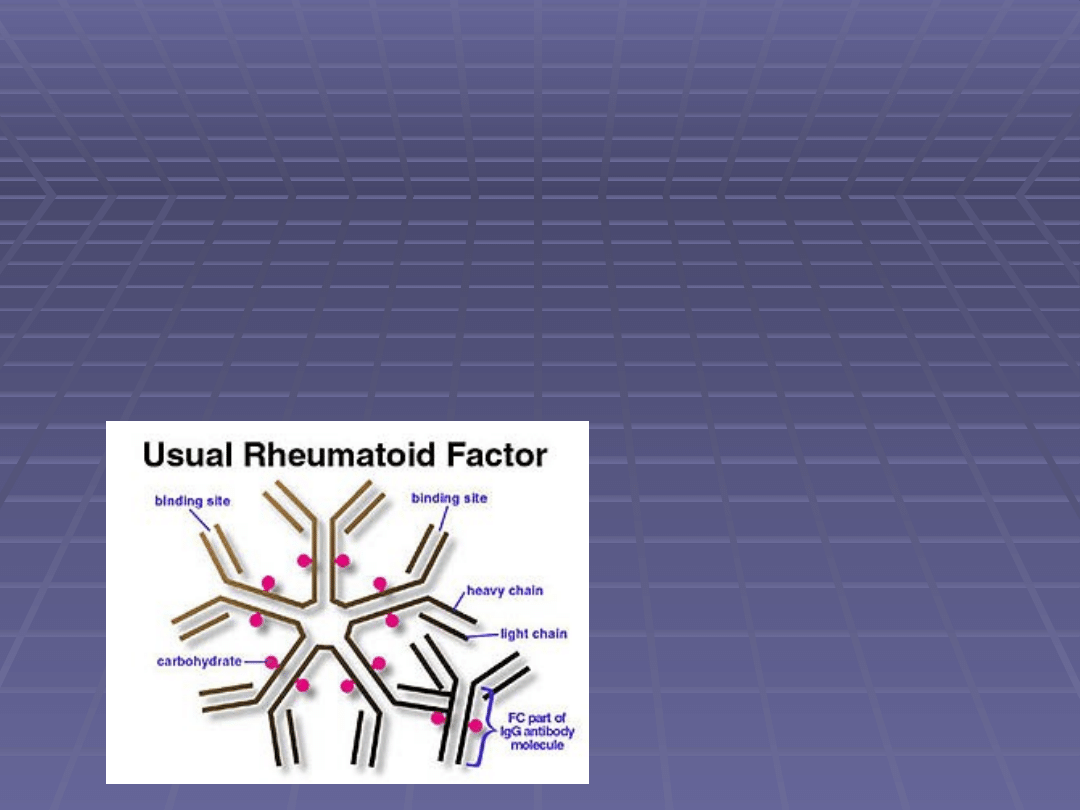
Reumatologic factor
Reumatologic factor
Antibody
Antibody
IgM
IgM
(85%)
(85%)
less frequently IgG, IgA or IgE
less frequently IgG, IgA or IgE
against Fc of own
against Fc of own
IgG
IgG
Detectable in serum,
Detectable in serum,
synovial fluid,
synovial fluid,
pleural fluid
pleural fluid
Reumatologic factor
Reumatologic factor
Autoimmunologc diseases – RZS
Acute bacterial, viral infections
Neoplasmatic disorders
Production induced by immunological complexes
Upregulate complement activity and IC removal
Bind to Fc – so bind to antibody with different
specificity
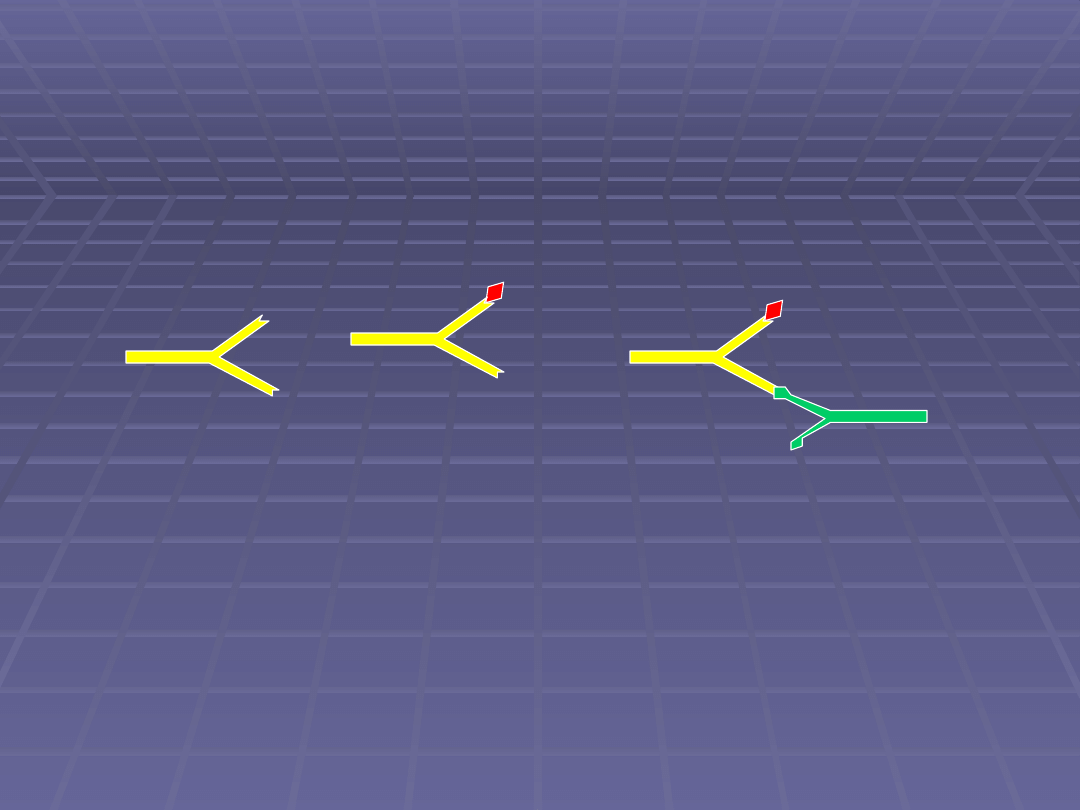
Anti-idiotypic antibody
Anti-idiotypic antibody
antigen
antibody
Ig are produced against antigen
Immunologic response initiation
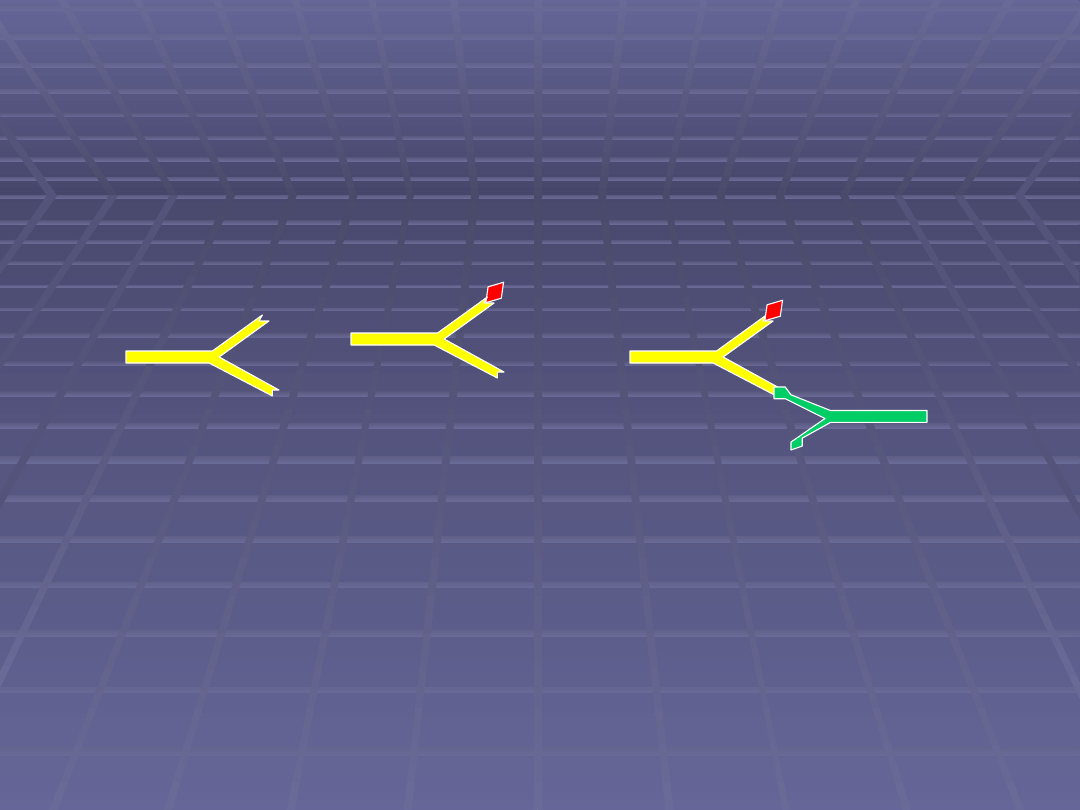
Anti-idiotypic antibody (Ab2)
Anti-idiotypic antibody (Ab2)
antigen
Anti-idiotypic
antibody
Jerne’a anti-idiotypic network theory
antibody
Within time anti-idiotypic antibody are produced
against Fab
on
antibodies.
Immunological complexes network is build up
(antibody - anti-idiotypic antibody)
Anti-idiotypic antibody
Anti-idiotypic antibody
antigen
Anti-idiotypic
antibody
Jerne’a anti-idiotypic network theory
antibody
Complexes are eliminated by
macrophages
Anti-idiotypic antibody
Anti-idiotypic antibody
Many idiothypic determinant are present in
Many idiothypic determinant are present in
Fab
Fab
Anti-idiotypic antibody may bind to antibody
Anti-idiotypic antibody may bind to antibody
of different classes both soluble and on cell
of different classes both soluble and on cell
surface (BCR, TCR)
surface (BCR, TCR)
1984 – Jerne – Nobel price
1984 – Jerne – Nobel price
Anti-idiotypic antibody
Anti-idiotypic antibody
Present in healthy subjects
Present in healthy subjects
Regulatory function for humoral and
Regulatory function for humoral and
cellular response
cellular response
Depending on:
Depending on:
Concentration
Concentration
Time when they appear
Time when they appear
Other factors like cytokines
Other factors like cytokines
Immunological tolerance
Immunological tolerance
For normal body functioning not only
For normal body functioning not only
effective pathogens and toxin
effective pathogens and toxin
elimination is needed
elimination is needed
but also ability to autoantigens
but also ability to autoantigens
tolerance as well as
tolerance as well as
antigens that are harmless.
antigens that are harmless.
Lack of tolerance leads to severe disorders
Immunological memory
Immunological memory
Ability to quicker and more effective
Ability to quicker and more effective
immunological response after second
immunological response after second
contact with antigen.
contact with antigen.
Positive memory (microorganism
Positive memory (microorganism
disorders)
disorders)
Negative memory (allergy)
Negative memory (allergy)
Immunological memory
Immunological memory
mechanisms
mechanisms
Increasing
Increasing
number of lymphocytes
number of lymphocytes
that can recognise antigen
that can recognise antigen
Lymphocytes with
Lymphocytes with
higher affinity
higher affinity
to
to
antigens
antigens
Survived
Survived
memory lymphocytes
memory lymphocytes
* 90% cells from primary response die in
* 90% cells from primary response die in
apoptosis induced by Apo-1/Fas or cytokines;
apoptosis induced by Apo-1/Fas or cytokines;
* memory cells survive because of increased Bcl-2
* memory cells survive because of increased Bcl-2
expression (antyapoptotic molecule)
expression (antyapoptotic molecule)
How is it possible?
How is it possible?
- hypothesis
- hypothesis
1.
1.
Memory lymphocytes can live for a long time
Memory lymphocytes can live for a long time
2.
2.
Antigen that induce primary immunological
Antigen that induce primary immunological
response is binded for a long time by dendritic
response is binded for a long time by dendritic
cells and can stimulate lyphocytes
cells and can stimulate lyphocytes
3.
3.
Memory lymphocytes are constitutively
Memory lymphocytes are constitutively
activated by cross-reacting antigens, mitogens
activated by cross-reacting antigens, mitogens
and superantigens
and superantigens
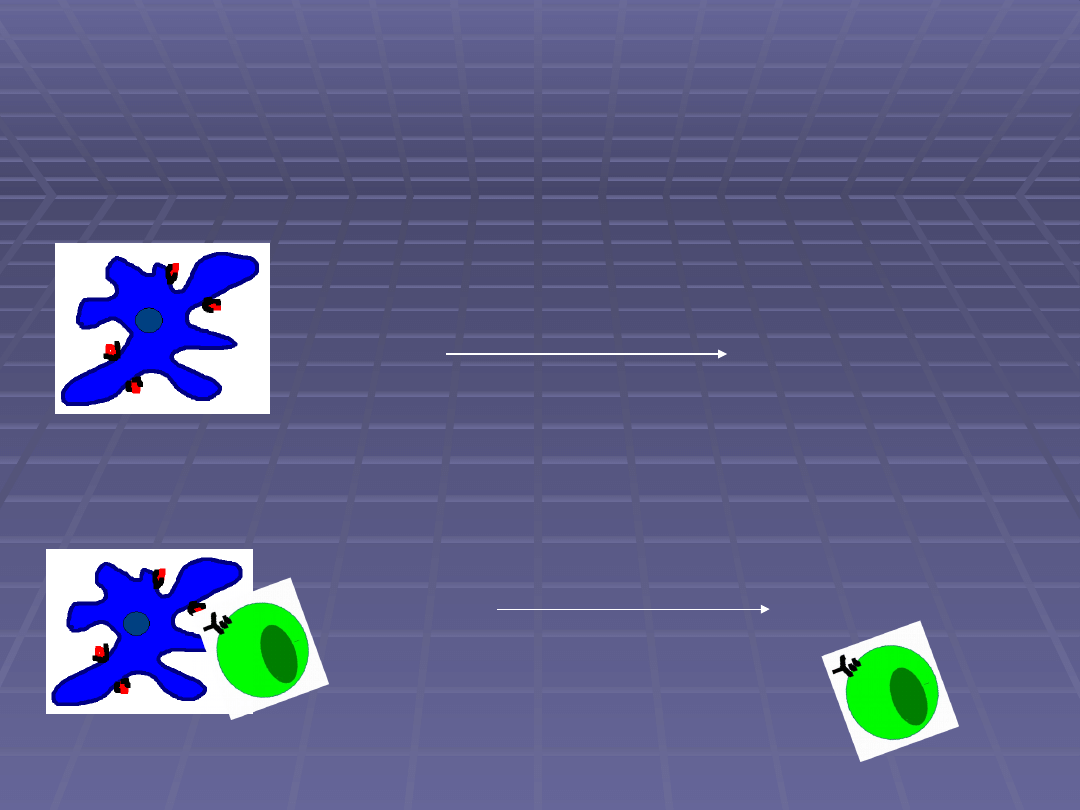
The role of nodules dendritic cell
The role of nodules dendritic cell
(FDC) in immunological memory
(FDC) in immunological memory
Y
Y
Y
Y
Y
Y
Y
Y
No immature lymphocytes
activation
Immunological reaction duration
Ig against antibody high concentration
Blocking of antigen binded on FDC surface
Immunological reaction inhibition
Ig downregulation,
antigens presentation – can activate immature lymphocytes B
Lymphocytes stimulation
Antibody production
Y
Y
Y
Memory lymphocytes B
Memory lymphocytes B
compared to immature
compared to immature
lymphocytes B
lymphocytes B
More
More
BCR have higher affinity to antigen
BCR have higher affinity to antigen
(mature Ig affinity – VDJ genes recombination)
(mature Ig affinity – VDJ genes recombination)
usually IgG, IgA, IgE
usually IgG, IgA, IgE
IgM, IgD
IgM, IgD
Have more MHCII
Have more MHCII
Are easier activated
Are easier activated
Live longer – often present in spleen, bone-marrow
Live longer – often present in spleen, bone-marrow
Memory lymphoctes T
Memory lymphoctes T
compared to immature
compared to immature
lymphocytes T
lymphocytes T
Same affinity
Same affinity
High CD45RO expression – phosphatase
High CD45RO expression – phosphatase
responsible for lymhocytes activation
responsible for lymhocytes activation
Adhesion molecules increased expression
Adhesion molecules increased expression
IL-2 receptor expression activation
IL-2 receptor expression activation
Costimulatory molecules role is smaller
Costimulatory molecules role is smaller
comparing to primary response
comparing to primary response
Other circulation: more frequently in
Other circulation: more frequently in
nonlymphatic organs, specially in inflammatory
nonlymphatic organs, specially in inflammatory
places
places
vaccination
Immunologic
Immunologic
al
al
tolerance
tolerance
Unresponsiveness of the immunologic
Unresponsiveness of the immunologic
al
al
system to an antigen that is induced by
system to an antigen that is induced by
previous exposure to that antigen
previous exposure to that antigen
(humoral and cellular)
(humoral and cellular)
.
.
Antigens
Antigens
Tolerogence/
Tolerogence/
tolerogenic
tolerogenic
Induce tolerance
Induce tolerance
Immunogens
Immunogens
generate immunity
generate immunity
Autotolerance
Autotolerance
is a tolerance to own antigens.
is a tolerance to own antigens.
is a part of the normal immune
is a part of the normal immune
system
system
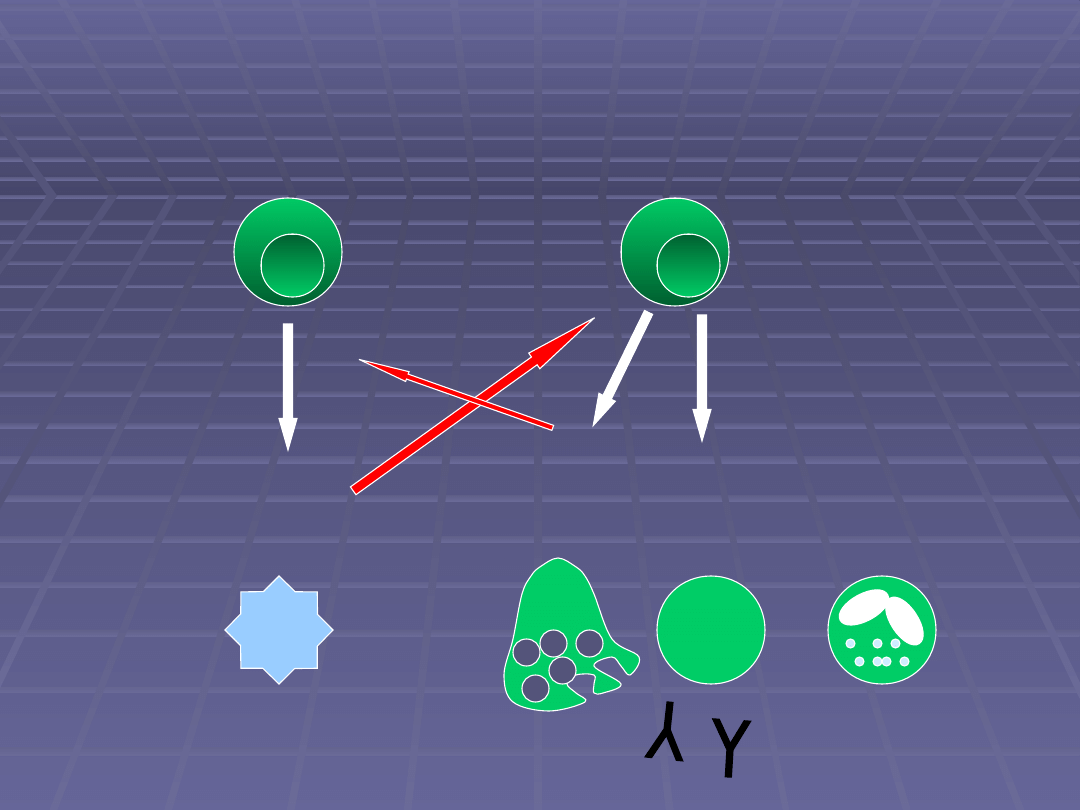
T
T
Immunogen
ic
antigen
Tolerogenic
antigen
T
T
T
Proliferation and
differentiation
T
Deletion (cell death)
Anergy (functional
unresponsiveness)
+
No
respons
e
Immunogen
ic
antigen
Why is it so important?
Why is it so important?
Tolerance to own antigens
Tolerance to own antigens
- we all have the same antigen receptors genes, later expressed in
- we all have the same antigen receptors genes, later expressed in
lymphocytes
lymphocytes
- self antigens are present on the cells and in the circulation
- self antigens are present on the cells and in the circulation
- self/nonself discrimination
- self/nonself discrimination
Foreign antigens may be administered in ways that
Foreign antigens may be administered in ways that
inhibit immune response
inhibit immune response
- immunisation methods to enhance the immunogenicity
- immunisation methods to enhance the immunogenicity
Therapeutic approach for preventing harmful
Therapeutic approach for preventing harmful
immune response
immune response
- organ transplant rejection
- organ transplant rejection
- autoimmune and allergic disorders treatment
- autoimmune and allergic disorders treatment
- tolerance in gene theraphy
- tolerance in gene theraphy
- proteins injection in protein deficienies (factor VIII in hemophiliacs)
- proteins injection in protein deficienies (factor VIII in hemophiliacs)
Mechanisms of tolerance
Mechanisms of tolerance
C
C
lonal
lonal
d
d
eletion
eletion
C
C
lonal
lonal
a
a
nergy
nergy
Autoantygen seqestration
Autoantygen seqestration
- anatomical
- anatomical
- molecular
- molecular
Active supression
Active supression
- anti-idiothypic antibody
- anti-idiothypic antibody
- regulatory lymphocytes
- regulatory lymphocytes
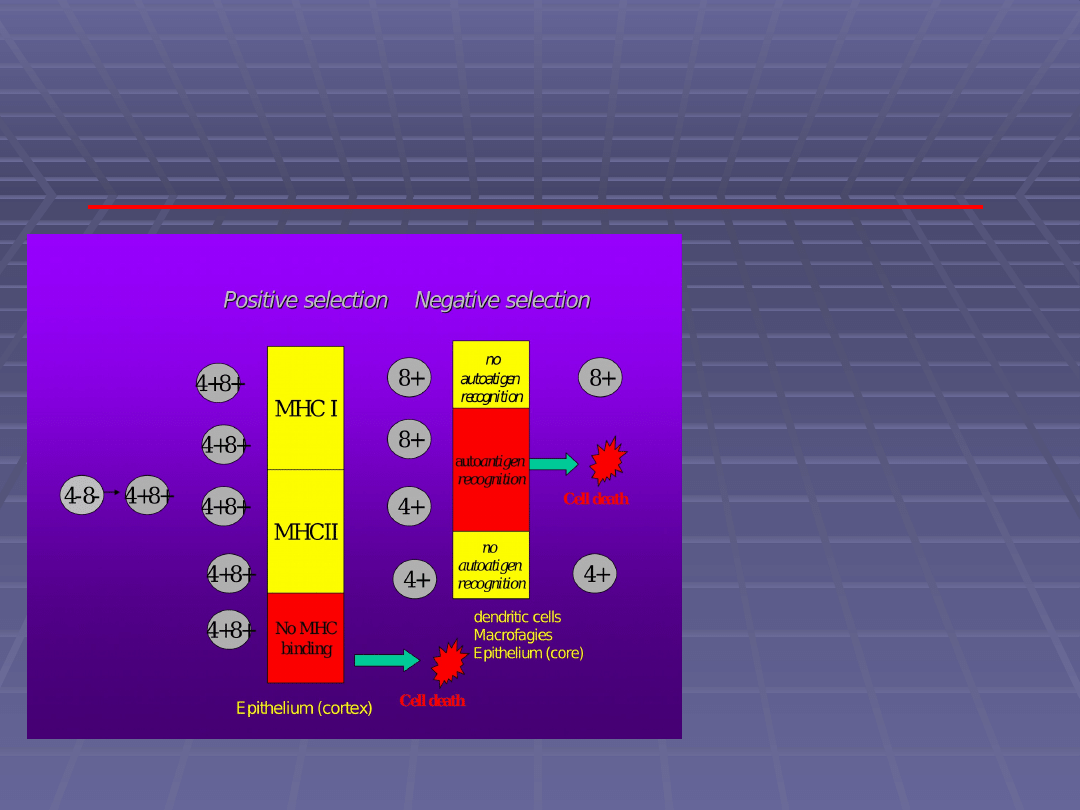
Clonal deletion
Clonal deletion
Process that leads to death
Process that leads to death
of
of
lymphocytes
lymphocytes
capable to autoantigen
capable to autoantigen
recognition
recognition
l
l
y
y
m
m
ph
ph
ocyt
ocyt
es
es
T
T
–
–
in thymus
in thymus
and in
and in
peripheral
peripheral
l
l
y
y
m
m
ph
ph
ocyt
ocyt
es
es
B
B
–
–
in bone marrow
in bone marrow
and
and
in peripheral
in peripheral
Positive selection Negative
Positive selection Negative
selection
selection
4-8- 4+8+
4+8+
4+8+
4+8+
4+8+
4+8+
MHC I
MHCII
No
MHC
binding
Cell death
8+
8+
4+
4+
Epithelium (cortex)
no
autoantigen
recognition
autoatigen
recognition
no
autoantigen
recognition
Cell death
8+
4+
Dendritic cells
Macrophages
Epithelium (core)
Clonal anergy
Clonal anergy
Inactivation of autoreactive lymphocytes
Inactivation of autoreactive lymphocytes
that avoided clonal deletion
that avoided clonal deletion
„
„
second
signal”
is
needed
for
second
signal”
is
needed
for
lymphocytes activation ( CD28 i CD80)
lymphocytes activation ( CD28 i CD80)
Only one signal leads to lymphocyte
Only one signal leads to lymphocyte
anergy – in this situation lymphocyte
anergy – in this situation lymphocyte
can produce some cytokines but can not
can produce some cytokines but can not
proliferate
proliferate
Immature lymphocyte T
APC
CD28
CD80/CD86
TCR
MHCII
antigen
Lack of
II signal leads to anergy
APC
B7
CTLA4
T
The role of costimualting molecules
The role of costimualting molecules
CD28 and CTLA4
CD28 and CTLA4
APC
CD28
B7
T
IL2
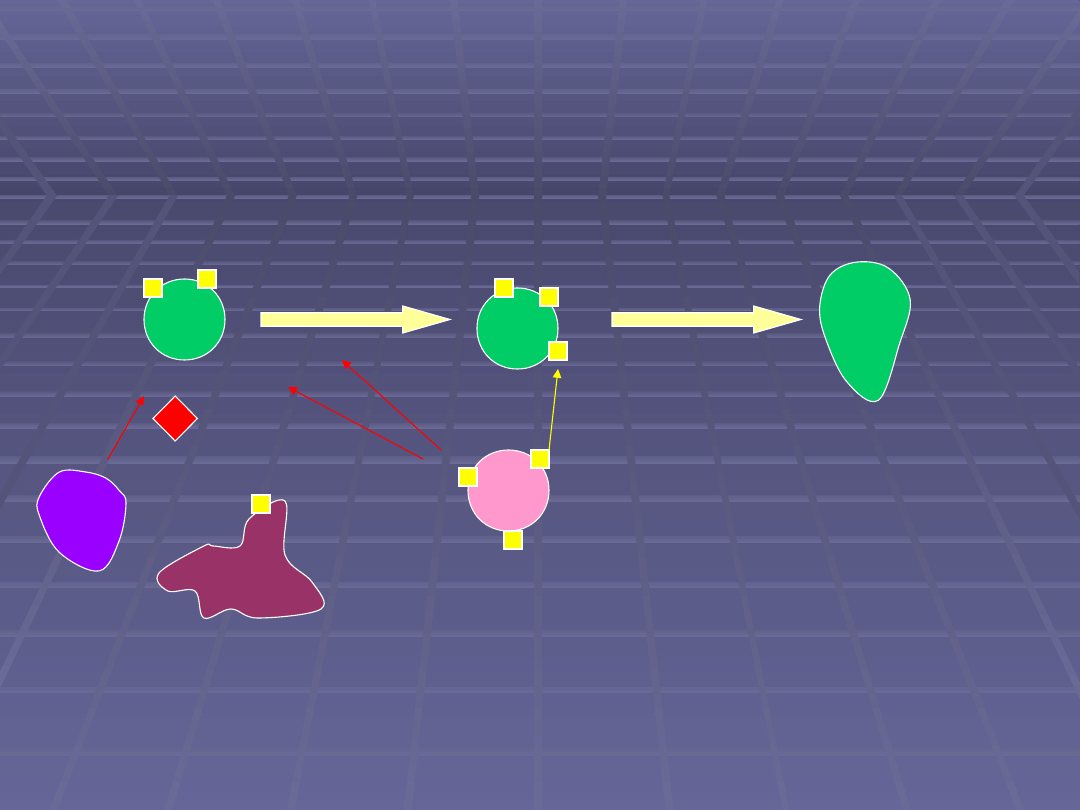
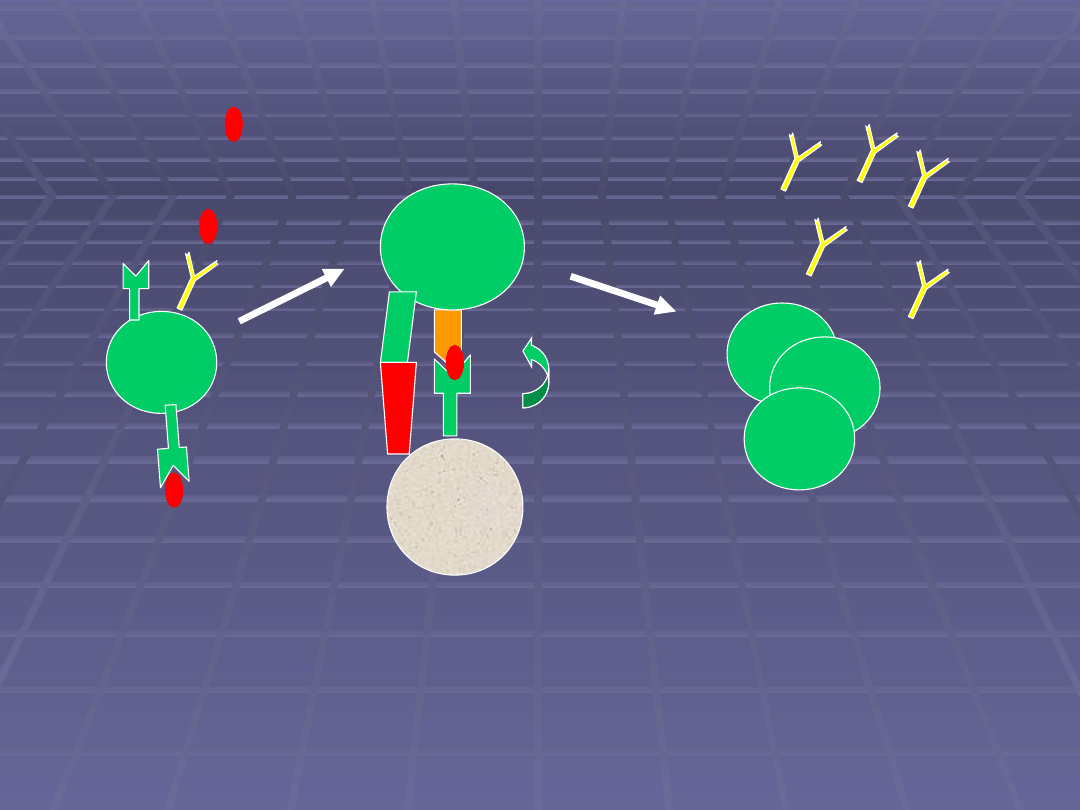
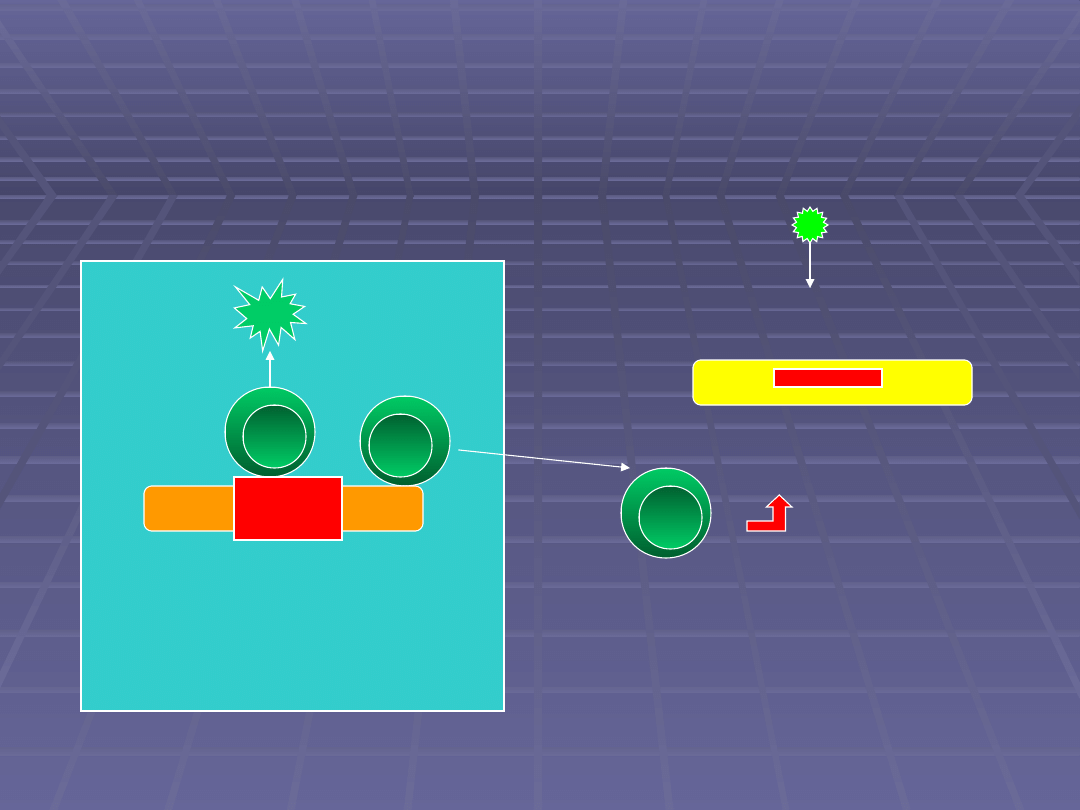
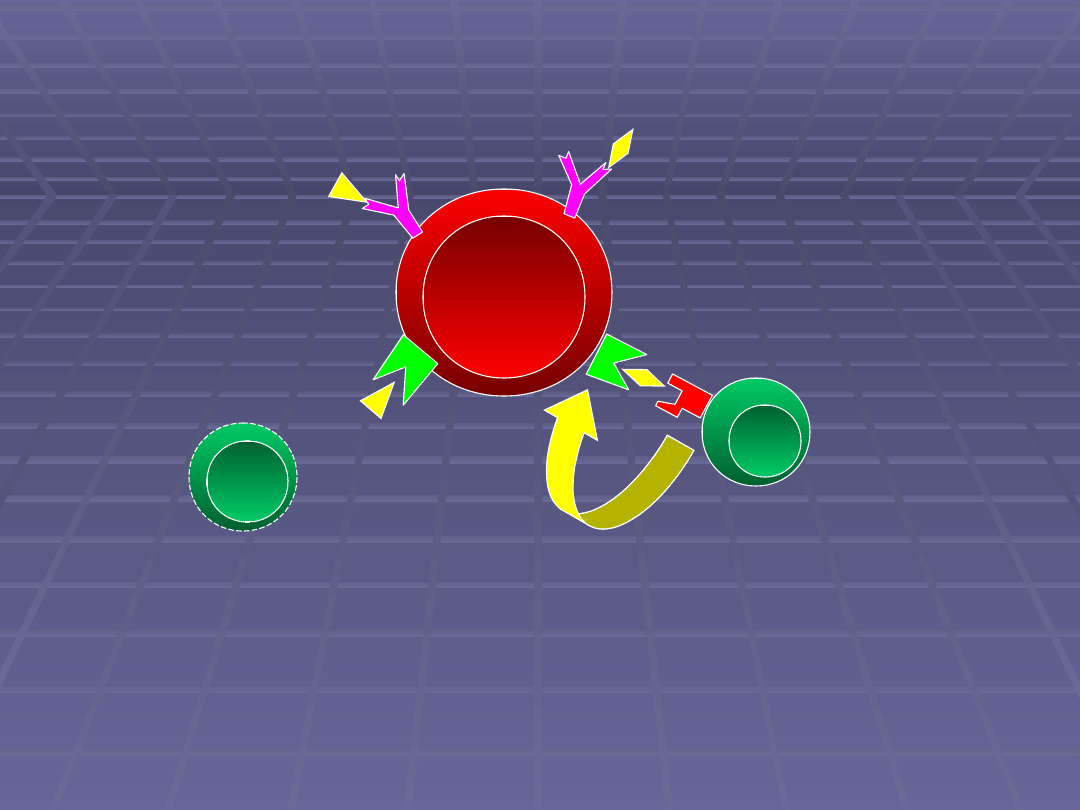
Tolerance mechanisms of lymphocytes B
Tolerance mechanisms of lymphocytes B
B
YY
Y
IgM
Polivalent antigens;
peptidoglikans
Clonal deletion
Anergy
Poly IgM binding
Apopotosis
Fagocytosis
B
B
Y Y
Y
Mature
lymphocytes B
B
Y
Y Y
soluble
autoantigens
high concentration
B
Y
IgM
ekspression
B
O
N
E
M
A
R
R
O
W
P
E
R
IP
H
E
R
A
L
S
PA
C
E
AUTO-ANTIGEN
AUTO-ANTIGEN
SEQUESTRATION
SEQUESTRATION
Anatomical
Anatomical
Molecular
Molecular
Molecular sequestration model
Molecular sequestration model
thymus
Th
Th
Lymphocyt that
recognise
„hidden” epitop
„dominating
” epitop
„hidden”
epitop
Virus
IFN γ
Disclosure of
„hidden”
autoantigen
Th
Recognition of
„hidden” autoantigen
Lymphocyt that
recognise
„dominating”
epitop
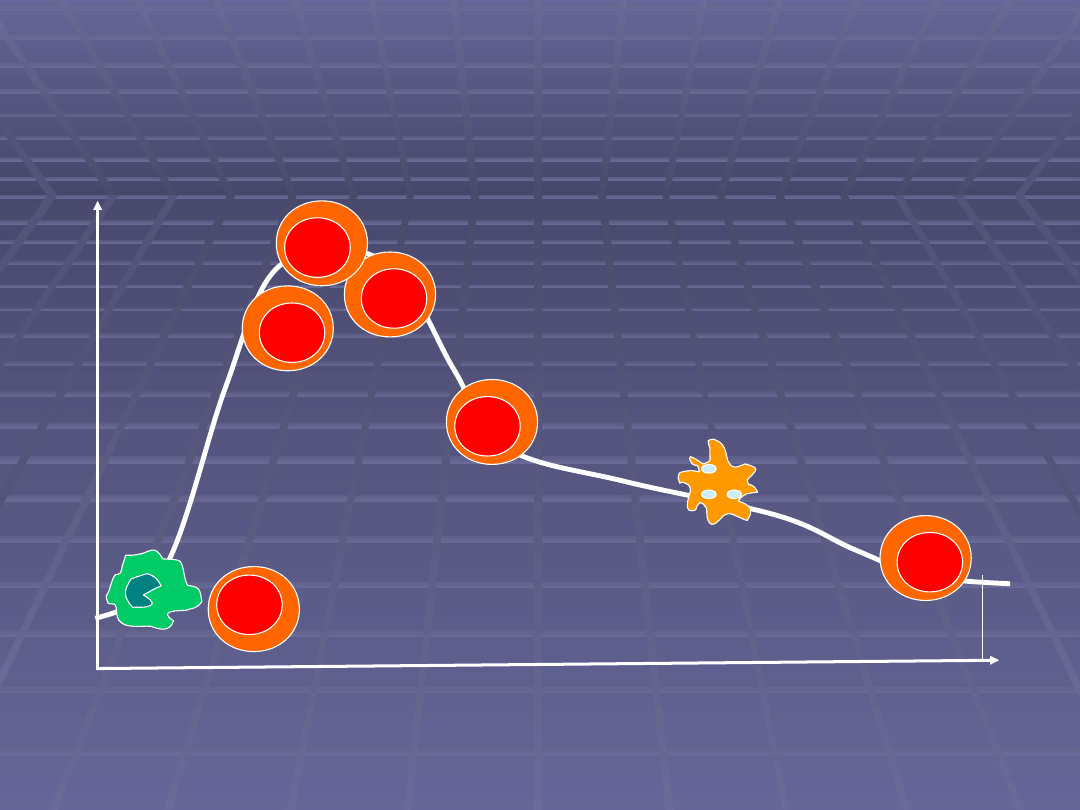
Active supression
Active supression
Limphocytes T reg
Limphocytes T reg
Anti-idiotypic antibodies
Anti-idiotypic antibodies
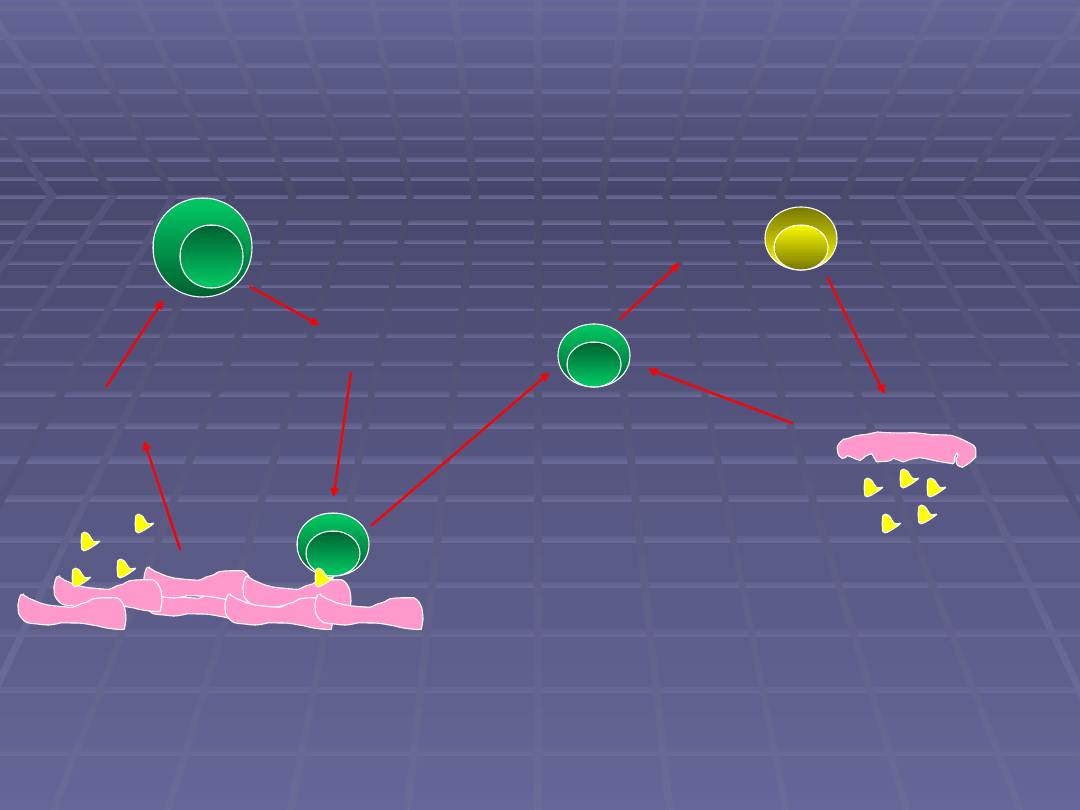
Anti-idiotypic antibody
antigen
Anti-idiotypic
antibody
Jerne’a anti-idiotypic network theory
antibody
* Can mimic autoantigens
* Can mimic autoantigens
for example tyreotropin in Graves-Basedove disease
for example tyreotropin in Graves-Basedove disease
* Defficiency may lead to clinical manifestation – lack of regulation
* Defficiency may lead to clinical manifestation – lack of regulation
Factors that can influence
Factors that can influence
autoregulation
autoregulation
immunological
immunological
genetical
genetical
environmental
environmental
hormonal
hormonal
Immunological factors
Immunological factors
Clonal deletion disturbances
Clonal deletion disturbances
Autoantigen depending factors
Autoantigen depending factors
Lyphocytes T depending factors
Lyphocytes T depending factors
Lyphocytes B depending factors
Lyphocytes B depending factors
Anti-idiotypic regulation
Anti-idiotypic regulation
disturbances
disturbances
Clonal deletion disturbances
Clonal deletion disturbances
• Autoreactive lymphocytes
getting out of
to peripheral space
• mutation of genes coding
APO1/Fas i APO1/FasL
-
SLE- circulating of mutated Fas
- apoptosis antagonists
- Hashimoto- Fas expression on
thyreocytes
Autoantigen depending factors
Autoantigen depending factors
Auroantigen sequestration removal
Auroantigen sequestration removal
np. heart infarctus, posttraumal eye inflammation
np. heart infarctus, posttraumal eye inflammation
Increased autoantigen presentation
Increased autoantigen presentation
- influenced by IFNγ increased MHC II expression
- influenced by IFNγ increased MHC II expression
collitis ulcerosa, diabetes,
collitis ulcerosa, diabetes,
autoimmune inflammatory thyroid disease
autoimmune inflammatory thyroid disease
Change of autoantigen structure
Change of autoantigen structure
drug-dependent SLE, inflammatory and traumal
drug-dependent SLE, inflammatory and traumal
influence
influence
Lyphocytes T depending
Lyphocytes T depending
factors
factors
Immunological deviation
Immunological deviation
Cross-reactivity between autoantigen
Cross-reactivity between autoantigen
and egzogenic antigen
and egzogenic antigen
Supression disturbances
Supression disturbances
miasthenia, thymus inflammation, SM, DM
miasthenia, thymus inflammation, SM, DM
no Ts production for DNA in S LE
no Ts production for DNA in S LE
Cytokine depending disturbances
Cytokine depending disturbances
IL2 and IL2R - SLE,
IL2 and IL2R - SLE,
sclerodermia
sclerodermia
, SM
, SM
Th
Th
Autoreaktywna
komórka B
Autoantigen
Egzogenic, cross-reactive
antigen
No Th cell
Th lymphocyte specific
for egzogenic antigen
HELP
Cross-reactivity between autoantigen
Cross-reactivity between autoantigen
and egzogenic antigen
and egzogenic antigen
*
adenovirus A2 and mielin protein -
SM
* ant p69 kom.β pancreas and cow’s milk albumin -
DM t I
IMPORTANT:
correlation with relative HLA haplotyp!
Th1
Th2
IFNγ
Macrophages
activation
IL4
IL5
IL10
B
eosinophil
Mast cell
Immunological deviation
Immunological deviation
RZS
SM
DM t I
SLE
miasthenia gravis
Lyphocytes B depending
Lyphocytes B depending
factors
factors
Policlonal activation
Policlonal activation
-lipopolisacharyd
-lipopolisacharyd
-EBV
-EBV
-HSV
-HSV
-HIV
-HIV
-Trypanosoma cruzi
-Trypanosoma cruzi
Lymphocytes B function disturbances
Lymphocytes B function disturbances
Superantigens and policlonal limphocytes B activation
Superantigens and policlonal limphocytes B activation
Th
APC
Superantigen
* Superantigens- antigens that stimulate limphocytes T
with different antigen specificity
B
Y
B
Y
Policlonal
activation:
-
EBV
- H I V
- LPS
- HSV
TCR
MHC II
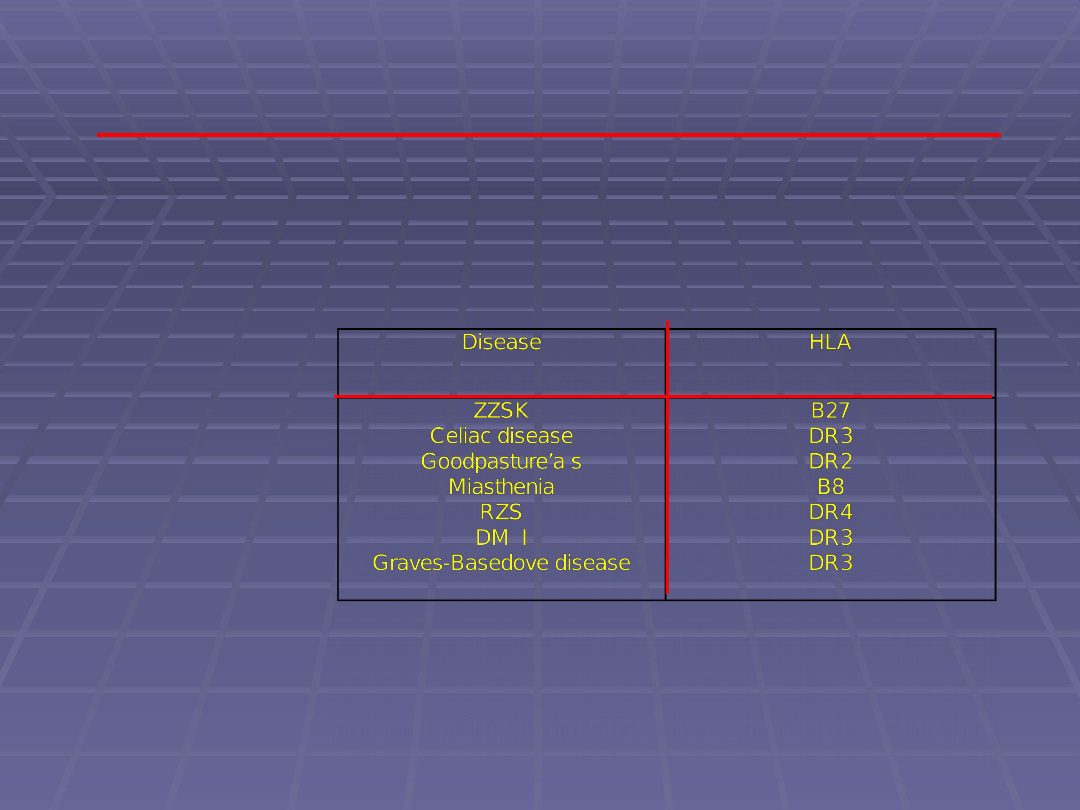
Genetical factors
Genetical factors
HLA
HLA
- allows autoreactive limphocytes elimination in thymus
- allows autoreactive limphocytes elimination in thymus
- influence antigen presentation to limphocytes T
- influence antigen presentation to limphocytes T
Other genes:
Other genes:
- genes oding TCR-
- genes oding TCR-
RZS, SLE
RZS, SLE
- genes for APO1/Fas i Fas L
- genes for APO1/Fas i Fas L
- genes coding complement proteins C2, C4
- genes coding complement proteins C2, C4
Environmental
Environmental
factors
factors
Bacterial infections
Bacterial infections
- cross-reactivity
- cross-reactivity
(streptoccoccal protein M and
(streptoccoccal protein M and
miosine
miosine
,
,
Clebsiella
Clebsiella
and HLA B 27)
and HLA B 27)
- bacterial superantigens
- bacterial superantigens
- staphylococcal toxins
- staphylococcal toxins
Viral infections
Viral infections
- cross-reactivity
- cross-reactivity
- policlonal lymphocytes B activation
- policlonal lymphocytes B activation
Cell infected by virus
IFNα/β
NK
IFN γ
Increased
expression of
MHC II and
autoantigen
presentation to
limphocytes Th
NK
Th
Th
Activated Th
limphocyte
do not need
professional APC
help
Tc
Cells damage and
Autoantigens removal
Cytokines increase
cytotoxicity
The role of viral infection in autoimmunisation induction
The role of viral infection in autoimmunisation induction
Virus
Cytotoxic effect
B
Y
Policlonal activation
Virus proteins expression on
cells
Cross-reactivity
* H BV and mielin
* Polio and AchR
The role of viral infection in autoimmunisation
The role of viral infection in autoimmunisation
induction
induction
Hormonal factors
Hormonal factors
Higher frequency of
Higher frequency of
autoimmunologic disorders in women
autoimmunologic disorders in women
Increased estrogens concentration in
Increased estrogens concentration in
women with autoimmunologic
women with autoimmunologic
disorders
disorders
Estrogens increase IFNγ synthesis –
Estrogens increase IFNγ synthesis –
increased MHC kl II expression
increased MHC kl II expression
Autotolerance
Autotolerance
is a tolerance to own antigens.
is a tolerance to own antigens.
is a part of the normal immune
is a part of the normal immune
system
system
Autoimmunological
Autoimmunological
mechanisms
mechanisms
Autoantigens
Autoantigens
(intracellular, secretogenous)
(intracellular, secretogenous)
Autoreactive lymphocytes T
Autoreactive lymphocytes T
(CD4+; MHC restriction)
(CD4+; MHC restriction)
Autoreactive lymphocytes B
Autoreactive lymphocytes B
(soluble antigens, APC)
(soluble antigens, APC)
Autoantibody
Autoantibody
(soluble or cellular surface antigens)
(soluble or cellular surface antigens)
Autoimmunological disordes
Autoimmunological disordes
Chronic disorders with
Chronic disorders with
remissions leading to
remissions leading to
disability and death
disability and death
70 diseases
70 diseases
5% of population
5% of population
Autoimmunological disordes
Autoimmunological disordes
Depending on autoantigen location
Depending on autoantigen location
*
*
organ specific
organ specific
* systemic
* systemic
Depending on patomechanism
Depending on patomechanism
* limph CD4+
* limph CD4+
* immunological complexes
* immunological complexes
* antibody
* antibody
Organ specific disorders
Organ specific disorders
Hashimoto
Hashimoto
Graves-Basedov
Graves-Basedov
Pernicious anaemia
Pernicious anaemia
Addison
Addison
Diabetes mellitus I
Diabetes mellitus I
Miasthenia gravis
Miasthenia gravis
Multiple sclerosis
Multiple sclerosis
Systemic disorders
Systemic disorders
Systemic lupus erythromatosus SLE
Systemic lupus erythromatosus SLE
Sclerodermia
Sclerodermia
Musculo-cutaneus inflammatory
Musculo-cutaneus inflammatory
diseaese
diseaese
Sjogren syndrome
Sjogren syndrome
Primary billary cirrhosis
Primary billary cirrhosis
Autoimmunohemolitic anemia
Autoimmunohemolitic anemia
Autoimmunological disordes
Autoimmunological disordes
Cellular response
Cellular response
Hashimoto
Hashimoto
MD I
MD I
Multiple sclerosis
Multiple sclerosis
albinism
albinism
Humoral response
Humoral response
Miasthenia gravis
Miasthenia gravis
Graves-Basedov
Graves-Basedov
Autoimmunohemoliti
Autoimmunohemoliti
c anemia
c anemia
Systemic lupus
Systemic lupus
erythromatosus
erythromatosus
SLE
SLE
Multiple sclerosis
Multiple sclerosis
myelin sheath destruction by:
myelin sheath destruction by:
Macrofages (NO, TNF, free radical)
Macrofages (NO, TNF, free radical)
CD8+ cytotoxic (MHC I, granzymes, perforynes)
CD8+ cytotoxic (MHC I, granzymes, perforynes)
Lymphocytes B (antibodies against complement)
Lymphocytes B (antibodies against complement)
Cytokines (IFN-
Cytokines (IFN-
γ
γ
, TNF)
, TNF)
Chemokines for Th1
Chemokines for Th1
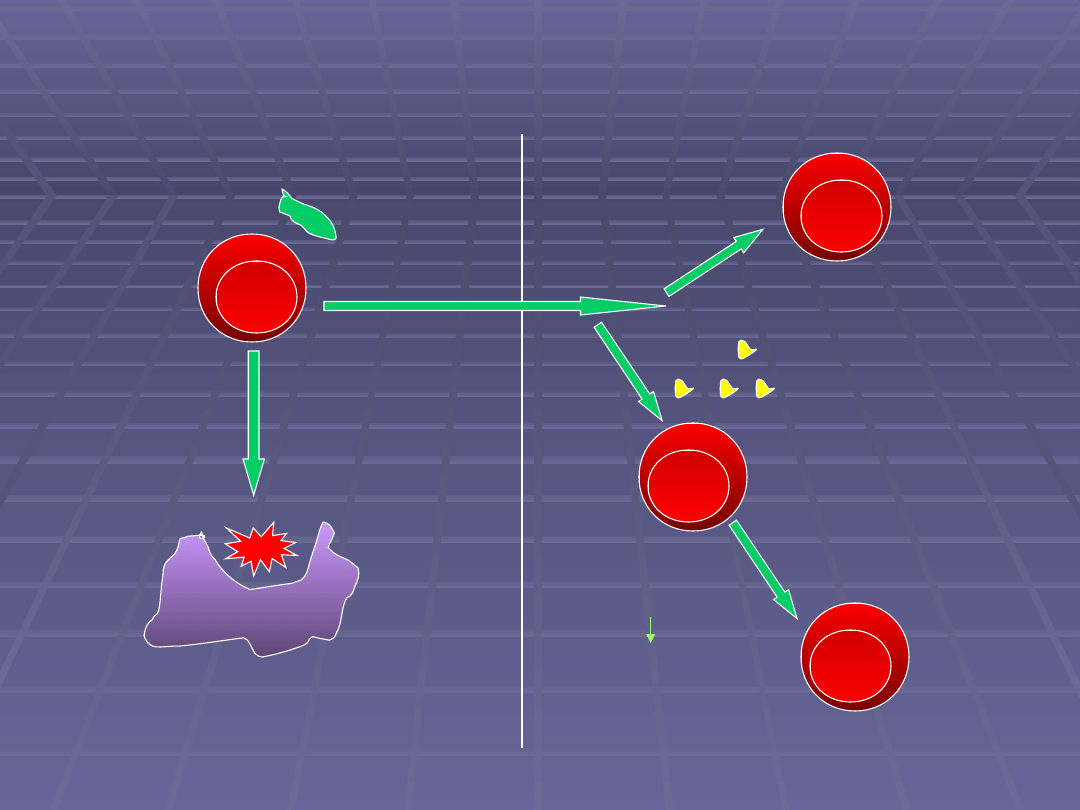
Humoral response
Humoral response
Antigen opsonisation
Antigen opsonisation
(fagocytosis,
(fagocytosis,
complement)
complement)
- erythrocytes in
- erythrocytes in
autoimmunohemolitic anemia or platelets
autoimmunohemolitic anemia or platelets
Autoantibody binded to cell surface antigens
Autoantibody binded to cell surface antigens
- complement activation, neutrophils, macrophages infiltration
- complement activation, neutrophils, macrophages infiltration
- Goodpasture’a syndrom
- Goodpasture’a syndrom
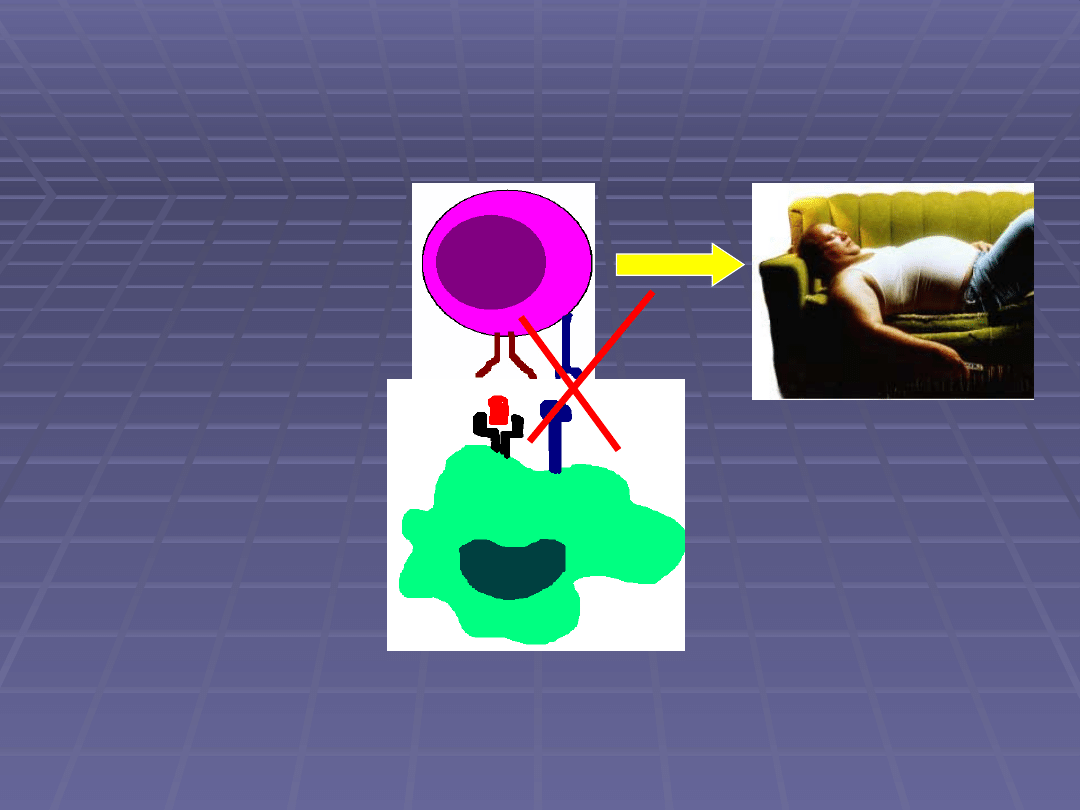
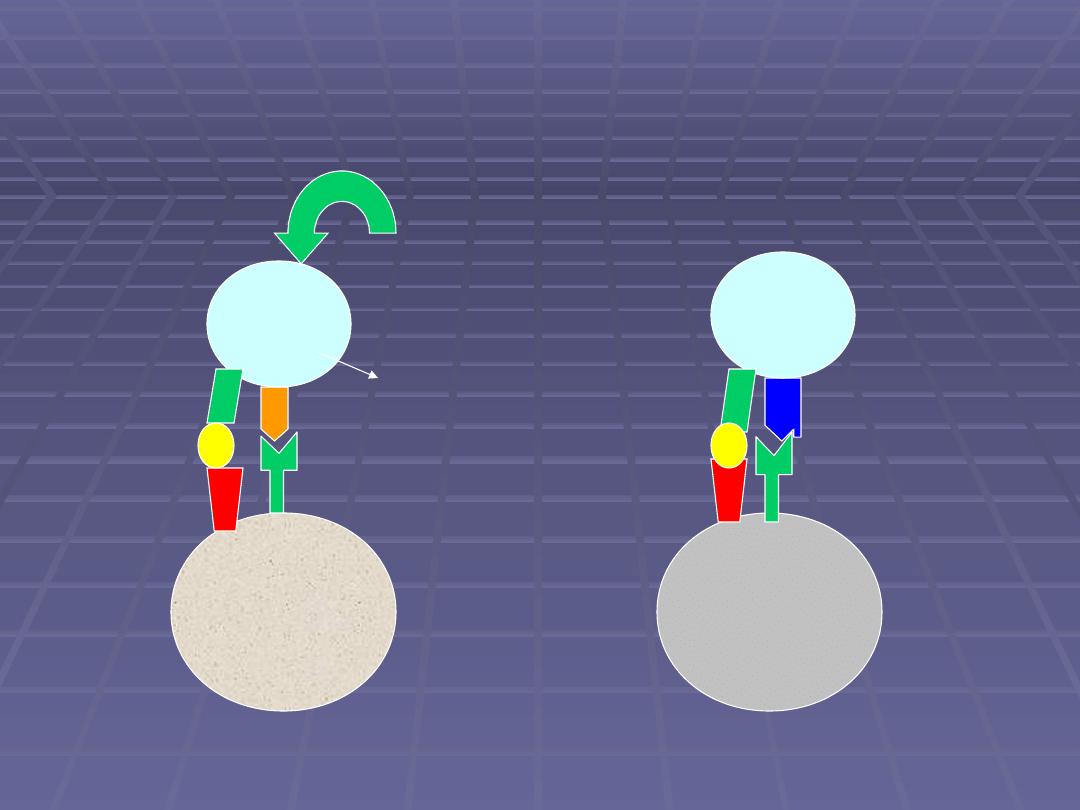
Autoantibody binded to important receptor
Autoantibody binded to important receptor
- Graves Basedov – TSHR tyreotropine receptor stimulation
- Graves Basedov – TSHR tyreotropine receptor stimulation
- miasthemia gravis – AChR blocking
- miasthemia gravis – AChR blocking
Immunological complex
Immunological complex
disorders
disorders
IgM antibodies bind to intracellular
IgM antibodies bind to intracellular
antigens released after cell death
antigens released after cell death
Activate complement
Activate complement
Eliminated by macrophages in liver
Eliminated by macrophages in liver
and spleen
and spleen
Pathological IgG antibodies
Pathological IgG antibodies
Thank
you
Document Outline
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Slide 45
- Slide 46
- Slide 47
- Slide 48
- Slide 49
- Slide 50
- Slide 51
- Slide 52
- Slide 53
- Slide 54
- Slide 55
- Slide 56
- Slide 57
- Slide 58
- Slide 59
- Slide 60
- Slide 61
- Slide 62
- Slide 63
- Slide 64
- Slide 65
- Slide 66
- Slide 67
- Slide 68
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
Wyszukiwarka
Podobne podstrony:
Basel II and Regulatory Framework for Islamic Banks
Basel II and Regulatory Framework for Islamic Banks
Physiological Arousal, Distress Tolerance, and Social Problem Solving Deficits Among Adolescent Self
inside out int rules and regulations
1999 USA Ju Jitsu Official Rules and Regulations
Sulphur handle setup and regulation sheet 6
alternator and regulator
tolerancja ok, Immunologia
Obwodowe mechanizmy tolerancji na autoantygen, studia, immunologia
VWL-REGULAMIN0607, Nauka, Immunologia, Semestr I
5 Rozwoj i regulacja ukladu immunologicznego
II Regulacja odpowiedzi immunologicznej
5Rozwój i regulacja układu immunologicznego, III ROK, immuno
regulamin ćwiczeń 2012, Stomatologia UMED Łódź, immunologia
Mechanizmy tolerancji centralnej na autoantygeny, studia, immunologia
więcej podobnych podstron