The Effect of Duration of Stretching
of the Hamstring Muscle Group for
Increasing Range of Motion in
People Aged 65 Years or Older
APTA is a sponsor of the
Decade, an international,
multidisciplinary initiative
to improve health-related
quality of life for people with
musculoskeletal disorders.
Background and Purpose. Stretching protocols for elderly people (
ⱖ65
years of age) have not been studied to determine the effectiveness of
increasing range of motion (ROM). The purpose of this study was to
determine which of 3 durations of stretches would produce and
maintain the greatest gains in knee extension ROM with the femur
held at 90 degrees of hip flexion in a group of elderly individuals.
Subjects. Sixty-two subjects (mean age
⫽84.7 years, SD⫽5.6, range⫽
65–97) with tight hamstring muscles (defined as the inability to extend
the knee to less than 20° of knee flexion) participated. Subjects were
recruited from a retirement housing complex and were independent
in activities of daily living. Methods. Subjects were randomly assigned
to 1 of 4 groups and completed a physical activity questionnaire. The
subjects in group 1 (n
⫽13, mean age⫽85.1 years, SD⫽6.4, range⫽
70 –97), a control group, performed no stretching. The randomly
selected right or left limb of subjects in group 2 (n
⫽17, mean
age
⫽85.5 years, SD⫽4.5, range⫽80–93), group 3 (n⫽15, mean
age
⫽85.2 years, SD⫽6.5, range⫽65–92), and group 4 (n⫽17, mean
age
⫽83.2 years, SD⫽4.6, range⫽68–90) was stretched 5 times per
week for 6 weeks for 15, 30, and 60 seconds, respectively. Range of
motion was measured once a week for 10 weeks to determine the
treatment and residual effects. Data were analyzed using a growth
curve model. Results. A 60-second stretch produced a greater rate of
gains in ROM (60-second stretch
⫽2.4° per week, 30-second
stretch
⫽1.3° per week, 15-second stretch⫽0.6° per week), which
persisted longer than the gains in any other group (group 4 still had
5.4° more ROM 4 weeks after treatment than at pretest as compared
with 0.7° and 0.8° for groups 2 and 3, respectively). Discussion and
Conclusion. Longer hold times during stretching of the hamstring
muscles resulted in a greater rate of gains in ROM and a more
sustained increase in ROM in elderly subjects. These results may differ
from those of studies performed with younger populations because of
age-related physiologic changes. [Feland JB, Myrer JW, Schulthies SS,
et al. The effect of duration of stretching of the hamstring muscle
group for increasing range of motion in people aged 65 years or older.
Phys Ther. 2001;81:1100 –1117.]
Key Words: Age, Elderly, Flexibility, Hamstring muscles, Lower extremity.
1110
Physical Therapy . Volume 81 . Number 5 . May 2001
Research
Report
J Brent Feland
J William Myrer
Shane S Schulthies
Gill W Fellingham
Gary W Measom
䢇
ўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўў
ўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўў
ўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўў

N
umerous researchers have compared various
stretching techniques to determine which
technique is most effective for increasing
joint range of motion (ROM).
1–5
Stretching
is important because it is believed to provide many
physical benefits, including improved flexibility,
3,6,7
improved muscle or athletic performance,
8,9
improved
running economy (decreased energy expenditure at a
given speed),
10,11
injury prevention,
3,11
promotion of
healing, and possibly decreased delayed-onset muscle
soreness.
12,13
Although evidence to support these beliefs
is limited, stretching appears to us to be in widespread
use.
Researchers have looked at the effect of different vari-
ables associated with stretching, including force or inten-
sity,
14
position,
15
frequency and duration,
6,16,17
and
repetition.
18
In the majority of these studies, younger
people, usually between the ages of 18 and 39 years, were
the subjects. The results of these studies, therefore, may
not be applicable to all age groups, particularly elderly
people because of age-related physiological changes.
Physiologic changes that are said to occur with age
include muscle atrophy
19
; reduced capacity for healing,
diminished
capillary
blood
supply,
and
reduced
amounts of mesenchymal stem cells
20
; and loss of
strength and elasticity in soft-tissue matrices.
20
Increased
muscle and joint stiffness with increased amounts of
fibrous connective tissue
11,21
has also been reported.
It is our opinion, based on the review of the literature,
that connective tissue compliance appears to be a major
factor in musculoskeletal flexibility. Plastic rather than
elastic deformation, theoretically, can result in more
permanent lengthening of the tissues.
22
Plastic changes
to connective tissue are thought to be brought about by
slow, low-intensity, and long-duration stretches that do
not injure the muscle.
1,23
Some authors
6,17,24
have sug-
gested stretch durations of 15 to 30 seconds using either
proprioceptive neuromuscular facilitation (PNF) tech-
niques or other stretching methods, whereas Smith,
3
based on a review of the literature, suggested that the
stretch should be held for 15 to 20 seconds.
JB Feland, PT, PhD, is Assistant Professor, Department of Physical Education, College of Health and Human Performance, Brigham Young
University, RB 120A, Provo, UT 84602 (USA) (Brent_Feland@byu.edu). Address all correspondence to Dr Feland.
JW Myrer, PhD, is Associate Professor, Department of Physical Education, College of Health and Human Performance, Brigham Young University.
SS Schulthies, PT, PhD, ATC, is Associate Professor, Department of Physical Education, College of Health and Human Performance, Brigham
Young University.
GW Fellingham, PhD, is Associate Professor, Department of Statistics, Brigham Young University.
GW Measom, PhD, APRN, is Associate Professor, Department of Nursing, Brigham Young University.
Dr Feland, Dr Myrer, Dr Schulthies, and Dr Fellingham provided concept/research design. Dr Feland, Dr Myrer, and Dr Schulthies provided
writing. Dr Feland provided data collection, project management, fund procurement, and facilities/equipment. Dr Fellingham provided data
analysis. All authors provided consultation (including review of manuscript before submission. The authors thank Jason Adams, Jody Alley,
Rebecca Jo Langford, AnnMarie Linnett, Eric Lowe, and Adam Turley for their assistance in the data collection process.
This study was approved by the Institutional Review Board at Brigham Young University.
This article was submitted December 10, 1999, and was accepted October 24, 2000.
Physical Therapy . Volume 81 . Number 5 . May 2001
Feland et al . 1111
ўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўўў
ў

For our study, a “long-duration” stretch was defined as a
stretch of greater than 30 seconds’ duration for one
repetition, and a “low-intensity” stretch was defined as a
stretch based on each subject’s perception of the onset
of discomfort in the back of the thigh. Low-intensity and
long-duration stretching approaches may optimize
increases in ROM among elderly people due to the
amount of connective tissue, increased stiffness, and
decreased elasticity that can occur with the aging process.
Although various researchers have investigated the
effects of exercise on ROM
13,25–27
and joint stiffness
28
in
elderly people, the optimal duration of a stretch of the
hamstring muscles to improve knee extension ROM has
not been determined.
Therefore, the purpose of our study was to compare the
effects of 6 weeks of repeated stretching of the hamstring
muscle group for 15, 30, or 60 seconds to determine
whether a longer stretch duration enhances ROM gains
among elderly people.
Method
Subjects
Subjects recruited for this study were independently
living in a retirement housing complex and were
informed of the purpose of the study and the need for
volunteers through a community meeting at the retire-
ment facility. Of the 78 subjects who volunteered for the
study, 62 subjects (mean age
⫽84.7 years, SD⫽5.6,
range
⫽65–97) qualified by not having any hip or knee
replacements or any history of pathology in the low back,
hips, or knees for the 3 months prior to the study.
Subjects voluntarily participated and signed an informed
consent form approved by Brigham Young University,
Provo, Utah.
To further qualify for the study, subjects had to demon-
strate “tight” hamstring muscles, defined as inability to
extend the knee to less than 20 degrees of knee flexion
with the femur held at 90 degrees of hip flexion while
the person was positioned supine. Subjects were also
screened to rule out knee joint flexion contractures by
checking knee extension ROM, as described by Norkin
and White,
29
while they were lying in a prone position. A
questionnaire was administered to all qualified subjects
in order to quantify physical activity levels. This physical
activity questionnaire has been shown to generate valid
and reliable classification scores for activity in a group of
elderly subjects who were similar, but not identical, to
ours.
30
Subjects were asked to maintain their level of
activity throughout the study. Sixty subjects (14 male,
46 female) completed the treatment portion of the study
(2 subjects did not complete the stretching phase of the
study because 1 subject voluntarily withdrew and the
other subject moved away). Fifty-six subjects (12 male, 44
female) continued through the 4-week recovery period
(out of the 4 subjects who dropped out during the
recovery period, 3 subjects developed other health prob-
lems and 1 subject moved to another residence).
Instrumentation
A double-arm (30.5-cm [12-in]) clear plastic goniometer
was used to measure knee extension ROM. Prior to data
collection, we performed a pilot study to establish intra-
tester reliability of measurements of knee extension
ROM. A test-retest design was used on 14 subjects of
similar age (
ⱖ65 years), with measurements taken 1
week apart by the research assistant who would perform
all measurements throughout the study. Reliability was
determined using an intraclass correlation coefficient
(ICC [3,1]). An ICC of .96 was considered appropriate
for continuing the study.
Experimental Procedure
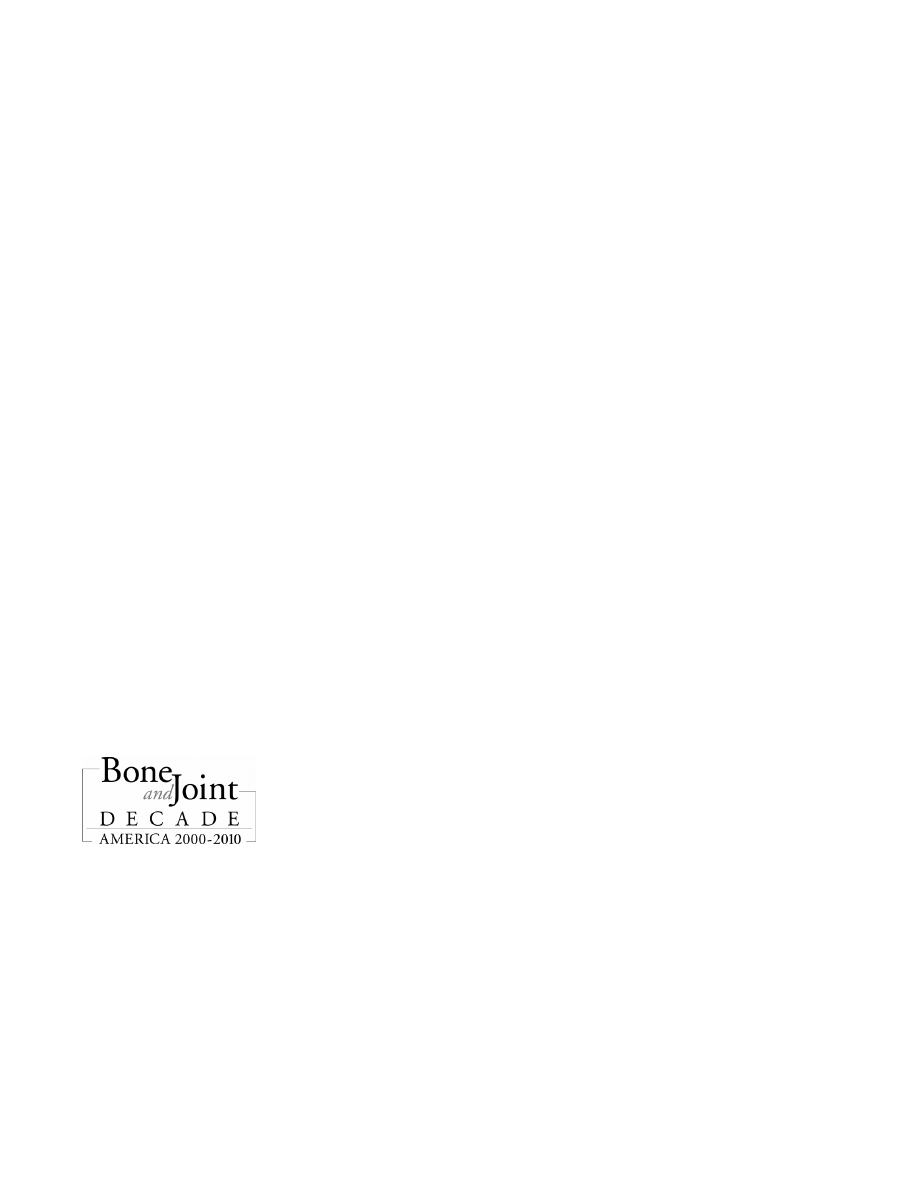
Measurement protocol. Choice of which lower extremity
to use for the stretching protocols was determined by the
toss of a coin for each subject; tails represented the left
lower extremity, and heads represented the right lower
extremity. Each subject was then measured for knee
extension ROM on both lower extremities. Measure-
ment of knee extension ROM was made with the subject
lying supine with the opposite lower extremity extended
and the lower extremity being measured positioned at
90 degrees of hip flexion. The greater trochanter and
the lateral epicondyle of the femur and lateral malleolus
were palpated and served as landmarks during measure-
ment, as outlined by Norkin and White.
29
We attempted
to maintain hip flexion at 90 degrees while the research
assistant moved the tibia into the terminal position of
knee extension, which was defined as the point at which
the subject reported feeling discomfort. The goniomet-
ric value was then recorded. The measurement recorded
was the angle between the leg position and full knee
extension (considered to be 0°) (Fig. 1). Because knee
joint contractures were ruled out, the measurement of
knee extension ROM was considered to be an indirect
measure of hamstring muscle flexibility, with hamstring
muscle tightness being the purported cause of a lack of
knee extension ROM.
All subjects were measured on the same day and at the
same time each week, before they had stretching for that
day. Measurements were taken on the stretched lower
extremity once a week for 6 weeks during the treatment
period and for 4 weeks posttreatment (recovery) to
determine the residual effect of the stretching. The
research assistant who performed the measurements was
unaware of group assignment.
1112 . Feland et al
Physical Therapy . Volume 81 . Number 5 . May 2001
Group assignment. After the initial measurements, the
subjects were randomly assigned to 1 of 4 groups.
Subjects assigned to group 1 (3 men, 10 women; mean
age
⫽85.1 years, SD⫽6.4, range⫽70–97) served as the
control and received no stretching. Group 2 (3 men, 14
women; mean age
⫽85.5 years, SD⫽4.5, range⫽80–93)
received a passive static stretch that was sustained for 15
seconds. Group 3 (4 men, 11 women; mean age
⫽85.2
years, SD
⫽6.5, range⫽65–92) received a passive static
stretch that was sustained for 30 seconds. Group 4
(5 men, 12 women; mean age
⫽83.2 years, SD⫽4.6,
range
⫽68–90) received a passive static stretch that was
sustained for 60 seconds.
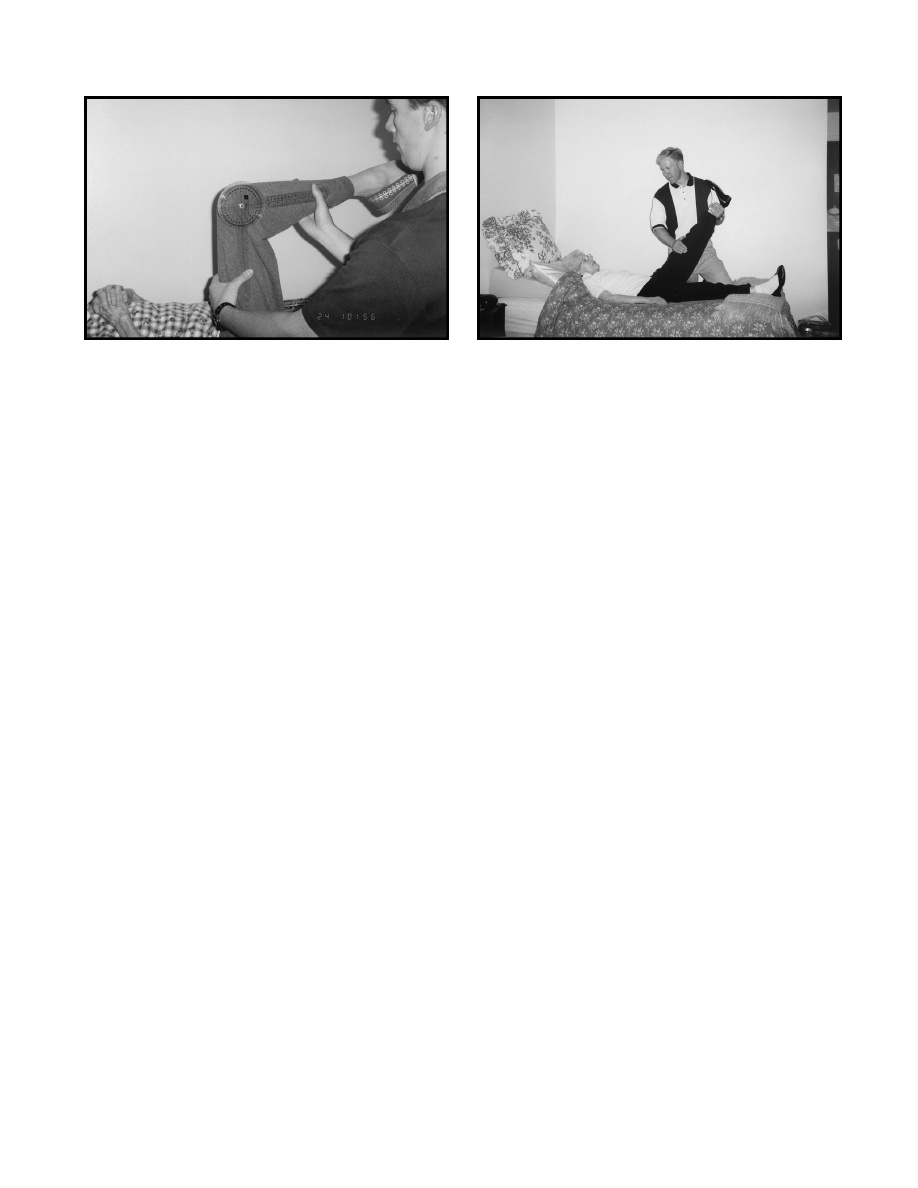
Stretching procedure. Stretching of the hamstring mus-
cles was performed by the primary researcher and 5
other research assistants (seniors in sports medicine and
exercise science). A straight-leg-raising technique was
used for this stretch because we believe that it is com-
monly used in the clinical setting for elderly people. All
subjects were supine lying as flat as possible. Due to
age-related changes in the upper thoracic and cervical
spine, we used a pillow to help maintain a comfortable
position for subjects who complained of neck pain when
trying to lie flat. Subjects who required a pillow (ie, for
both stretching and measurement) always used a pillow.
Based on the primary researcher’s observations, each
subject’s knee was maintained in extension with the
ankle at 90 degrees without medial (internal) or lateral
(external) rotation of the lower extremity, and the
extremity was raised until the subject reported discom-
fort (Fig. 2). The subject was asked to relax the lower
extremity in an effort to prevent contracting muscles
from affecting the stretch and to allow for a slow stretch.
No warm-up was allowed prior to stretching.
Subjects in groups 2 through 4 received 4 stretches for
their designated time period, with a 10-second rest
between stretches. During the 10-second rest, each sub-
ject was asked to move the lower extremity back and
forth from knee to chest to lower-extremity extension in
order to prevent what has been called “thixotropic
stiffening.”
31,32
Subjects in groups 2 through 4 had stretching 5 days per
week for 6 weeks. All subjects whose lower extremity was
stretched were retested for knee extension ROM every
week. A ROM measurement was also made at the end of
the 6-week treatment on the uninvolved lower extremity
to determine whether a stretching program indirectly
affected contralateral flexibility.
All research assistants were trained in administering the
stretching protocol by practicing on a similar-aged vol-
unteer who was not participating in the study due to time
constraints. Instructions included the use of the same
verbal cues to minimize variation in administration. All
stretching sessions were documented to record whether
the subjects received stretching, and assistants were
randomly assigned each day to subjects in order to
reduce the risk of interaction between treatment and
assistant.
If a subject missed a scheduled session, he or she made
up the session on another day during the same week; this
occurred a total of 16 times throughout the stretching
period of 6 weeks (once for 10 subjects and twice for 3
subjects). Prior to treatment, the researchers decided
that if any subject missed more than 4 days without
stretching, the subject would be eliminated from the
study. No subject missed more than 2 “stretch days”
throughout the 6-week treatment program.
Data Analysis
Because we were primarily interested in changes occur-
ring over time, it seemed reasonable to analyze the data
using linear growth curves. The slope of a line represents
a rate of change, and different slopes in different
treatment conditions (treatment and recovery) would
Figure 1.
Measurement of knee extension range of motion using a goniometer.
Figure 2.
Stretching of subject’s hamstring muscles using straight-leg-raising
method.
Physical Therapy . Volume 81 . Number 5 . May 2001
Feland et al . 1113
ўўўўўўўўўўўўўўўўўўўўўўўўўўў
ў
indicate different rates of impact of the various treat-
ments. To implement such an analysis, the SAS (version
6.12) MIXED Procedure
33
was used to analyze the data
from treatment and recovery period times. With multi-
ple measures per subject, it is important to appropriately
account for the within-subject covari-
ance structure. An autoregressive lag 1
(AR[1]) structure was found to most
closely fit the data, not unusual when
measurements are taken at equally
spaced time points. The problems
with the more traditional repeated-
measures analysis of variance in this
setting have been well documented.
34
The SAS General Linear Models Proce-
dure was used for analysis of contralat-
eral lower-extremity values and for
comparison of pretest and 4-week post-
test values for all groups. A post hoc
Student-Newman-Keuls test was used to
compare the pretest values with the
4-week posttest values to determine
whether a difference existed between
groups when both the treatment and
recovery periods were included.
Results
A comparison of intercepts and slopes
among all groups for the treatment
period is shown in Table 1. Plots of
response functions for all 4 groups in
both treatment and recovery conditions are shown in
Figure 3. The intercepts are model-adjusted estimates of
initial ROM means for each group. There was no differ-
ence in the starting intercept (pretest) among group 1
(41°), group 2 (45°), and group 3 (46°), but there was a
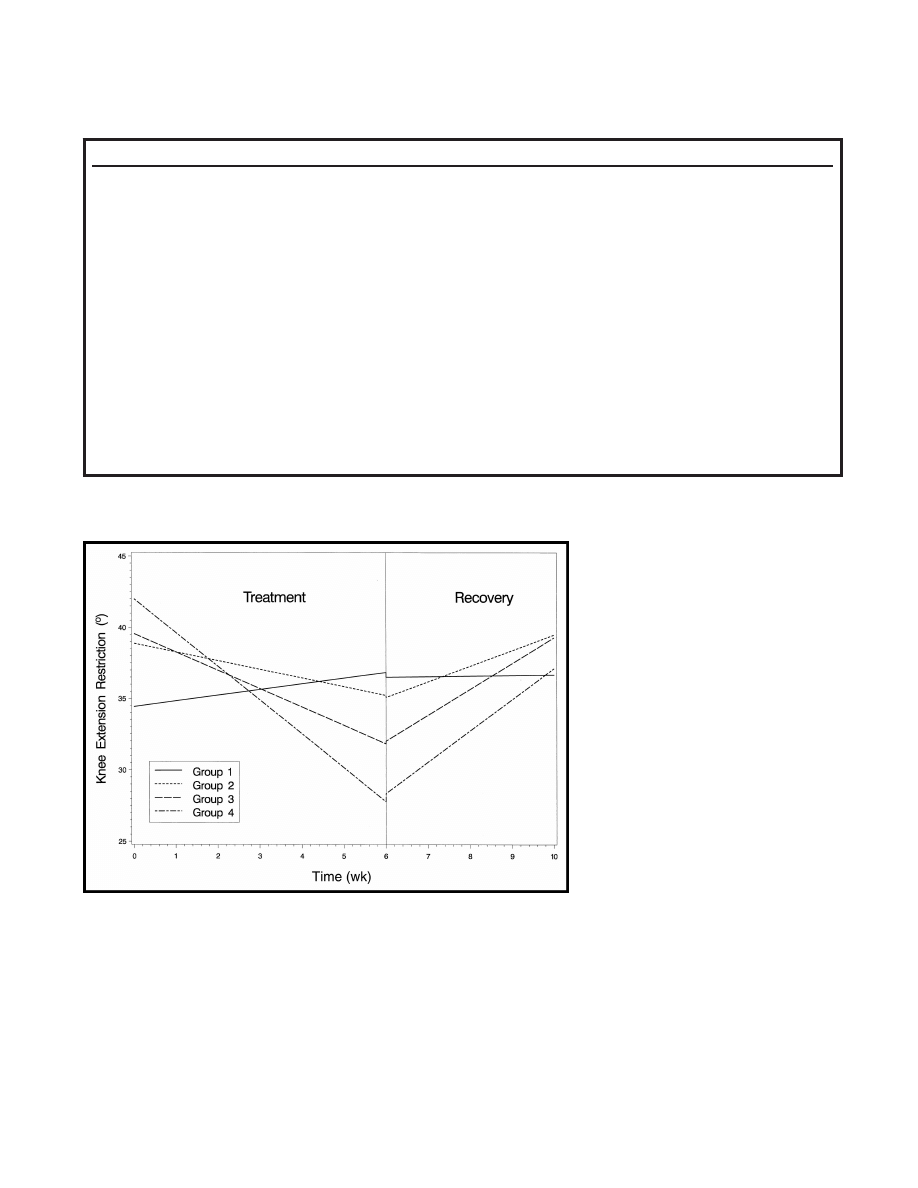
Figure 3.
Fitted line graph of intercepts and slopes for the 6-week treatment (stretching) and 4-week
recovery period. Note: the lines do not match-up at the 6-week point because they are fitted-plot
lines that represent 2 different periods of time for each group. Group 1 was a control (no
stretching) group, group 2 had 15-second stretches, group 3 had 30-second stretches, and
group 4 had 60-second stretches.
Table 1.
Intercepts and Slopes for 6-Week Stretching Period
Treatment
Value
Standard Error
Comparison
a
Intercept
Control (no stretch)
40.98710
2.95079
m (
t
⫽2.72, df⫽21)
Intercept
15-s stretch
45.43737
2.72627
Intercept
30-s stretch
46.11647
3.03633
Intercept
60-s stretch
48.55765
2.80192
j
(
t
⫽2.72, df⫽21)
Slope
Control (no stretch)
0.40292
0.32234
x
(control vs 15-s stretch;
t
⫽⫺2.41, df⫽390)
(control vs 30-s stretch;
t
⫽⫺3.85, df⫽390)
(control vs 60-s stretch;
t
⫽⫺6.58, df⫽390)
Slope
15-s stretch
⫺0.61078
0.27082
a
(
t
⫽⫺2.26, df⫽390)
j
(
t
⫽⫺2.41, df⫽390)
m (
t
⫽4.59, df⫽390)
Slope
30-s stretch
⫺1.28831
0.29843
a
(
t
⫽⫺4.32, df⫽390)
j
(
t
⫽⫺3.85, df⫽390)
m (
t
⫽2.68, df⫽390)
Slope
60-s stretch
⫺2.36798
0.27082
a
(
t
⫽⫺8.74, df⫽390)
x
(60-s stretch vs control;
t
⫽⫺6.58; df⫽390)
(60-s stretch vs 15-s stretch;
t
⫽4.59, df⫽390)
(60-s stretch vs 30-s stretch;
t
⫽2.68, df⫽390)
a
a
⫽significantly different from 0 (P⬍.05), j⫽significantly different from control (P⬍.05), m⫽significantly different from 60-second treatment (P⬍.05),
x
⫽significantly different from all other groups (P⬍.05).
1114 . Feland et al
Physical Therapy . Volume 81 . Number 5 . May 2001
difference between groups 1 and 4 (49°). We attributed
this difference to random error.
The slopes represent the rate of change in knee exten-
sion ROM during the 6-week stretching period. A com-
parison of the slopes (Tab. 1 and Fig. 3) for all 4 groups
revealed that after treatment, the ROM measurements
obtained for the treatment groups were different from
ROM measurement obtained for the control group. The
slope for group 1 was not different from 0, which
indicates there was no change in ROM over the treat-
ment period for that group. All 3 treatment groups had
slopes different from 0, indicating changes in ROM.
Comparison of slopes for the 3 treatment groups showed
that the slope for group 4 was greater than the slopes for
groups 2 and 3 and that the slopes for groups 2 and 3
were not different from each other (
␣⫽.05). Therefore,
group 4 had greater improvements in ROM compared
with groups 1 through 3. Groups 2 and 3 had greater
improvements in ROM than group 1 (no stretching).
Activity level was related to knee extension ROM. For
each unit increase in activity score, there was a 1.04-
degree increase in ROM. However, there was no associ-
ation of activity index with treatment slope, meaning
that a higher activity score indicated that the subject had
increased ROM that stayed higher throughout the treat-
ment and recovery phases of the study.
The longer the stretch duration, the steeper the slope
(the greater the rate of change in ROM) (Fig. 3) for
both the treatment and recovery periods. After the
6-week stretching protocol, model estimates of ROM
were highest for group 1 and lowest for group 4 (Tab. 2).
Slopes for the recovery period were positive, indicating a
regression toward pretest values. The slope for group 1
was again not different from 0.
Comparison of the treatment groups’ slopes with the
control group’s slope (during the recovery period)
revealed that the slopes for groups 3 and 4 were different
from the slope for group 1 (Tab. 2), but the slope for
group 2 was not different from the slope for group 1
(
␣⫽.05). A comparison of recovery slopes revealed that
the only difference between recovery slopes existed
between groups 2 and 4 (Tab. 2). Analysis of the pretest
and posttest measurements of the contralateral lower
extremity using the SAS General Linear Models Proce-
dure did not show a difference in ROM in any group
(P
⫽.2851).
To determine whether treatment effects incurred during
the treatment period were still evident at 4 weeks post-
treatment, an analysis of 4-week posttreatment scores
minus pretreatment scores was undertaken. An analysis
of variance on this change score showed differences
among treatment groups (P
⬍.0001). A post hoc Student-
Newman-Keuls test revealed that only group 4 still main-
tained incurred ROM. Group 4 still had 5.4 degrees
greater ROM than at pretest.
Discussion
The results indicated that a 60-second stretch was more
effective in increasing knee extension ROM than a 15- or
30-second stretch within this elderly group. These results
differ from those of Bandy and Irion,
17
who reported
that a 30-second stretch was as effective as a 60-second
static stretch of the hamstring muscles. More recently,
Bandy et al
16
reported that there was no difference
between stretching once or repeating the stretch 3 times
Table 2.
Intercepts and Slopes During 4-Week Recovery Period
Treatment
Value
Standard Error
Comparison
a
Intercept
Control (no stretch)
43.78760
3.25640
m (
t
⫽⫺2.71, df⫽21)
Intercept
15-s stretch
42.37451
3.02019
m (
t
⫽2.46, df⫽21)
Intercept
30-s stretch
39.30303
3.36433
Intercept
60-s stretch
35.63790
3.10655
j
(
t
⫽⫺2.71, df⫽21)
k
(
t
⫽2.46, df⫽21)
Slope
Control (no stretch)
0.40253
0.43348
l
(
t
⫽2.98, df⫽259)
m (
t
⫽3.80, df⫽259)
Slope
15-s stretch
1.10402
0.38803
a
(
t
⫽2.85, df⫽259)
m (
t
⫽⫺2.04; df⫽259)
Slope
30-s stretch
1.81556
0.40873
a
(
t
⫽4.44, df⫽259)
j
(
t
⫽2.98, df⫽259)
Slope
60-s stretch
2.19122
0.36419
a
(
t
⫽6.02, df⫽259)
j
(
t
⫽3.80, df⫽259)
k
(
t
⫽⫺2.04; df⫽259)
a
a
⫽significantly different from 0 (P⬍.05), j⫽significantly different from control (P⬍.05), k⫽significantly different from 15-second treatment (P⬍.05),
l
⫽significantly different from 30-second treatment (P⬍.05), m⫽significantly different from 60-second treatment (P⬍.05).
Physical Therapy . Volume 81 . Number 5 . May 2001
Feland et al . 1115
ўўўўўўўўўўўўўўўўўўўўўўўўўўў
ў

using either a 30- or 60-second static stretch. In both
studies by Bandy and colleagues, treatments were given
for 6 weeks, as in our study, and the researchers acknowl-
edged that the results should be applied only to a similar
age group (mean age
⫽26 years).
Understanding that a longer-duration stretch will
improve ROM in elderly people is particularly impor-
tant, in our opinion, because joint mobility declines with
increasing age.
35
Research has shown a decline in both
active and passive ROM of lower-limb joints from 70 to
92 years of age, with a more pronounced decline during
the ninth decade.
35
In our study, all stretches were repeated 4 times with a
10-second rest between stretches. We used repeated
stretches because Taylor et al
18
suggested that maximal
muscle-tendon unit elongation occurs after approxi-
mately 4 stretches, and additional stretches (ie, up to 10
stretches) resulted in little further improvement. We
believe that this cyclic stretching technique may be even
more beneficial for elderly people due to the physiolog-
ical changes of increased muscle stiffness and collagen
deposition that occur with aging.
We used a passive straight-leg-raise method of stretching
because we believe that this method promotes relaxation
of the hamstring muscles, and the static method was
chosen over a PNF-based approach because it has been
reported to be more comfortable
36
and, in our opinion,
is simple to perform. Older muscles are more susceptible
to contraction-induced injury, especially when the muscle
is lengthened during the contraction,
19
and have a dimin-
ished ability to recover from acute or repetitive musculo-
skeletal trauma.
11,20
This reduced capacity for healing,
combined with a higher predisposition for injury, is why we
believed that the static stretching technique may be more
suitable than PNF techniques for elderly people.
The 60-second duration may have been more beneficial
than the 15- or 30-second durations in overcoming the
increased muscle stiffness and collagen deposition that
also accompany the aging process. We showed that the
more physically active a person was, the more ROM he
or she had initially and throughout all treatments. Even
though we did not measure the effect of ROM on
function, we believe this observation is important
because it suggests the importance of physical activity in
maintaining a level of flexibility.
We also attempted to determine whether stretching one
lower extremity resulted in any changes of the contralat-
eral (nonstretched) lower extremity. No differences in
ROM were found in the contralateral extremity in any
treatment group. Stretching one lower extremity did not
result in knee extension ROM improvements of the
opposite (nonstretched) lower extremity. Weekly mea-
surements of ROM were taken in hopes of seeing a trend
(when the greatest improvements occurred). We were
unable to show a pattern of when the majority of ROM
changes occurred. This finding may have been due to
our small sample size and the large standard deviation in
each group.
Our post hoc comparison showed that there was a differ-
ence between the initial measurements and the measure-
ments taken after 4 weeks without stretching in group 4,
but there was no difference within the other 3 groups.
Thus, groups 2 and 3 returned to their pretreatment
ROM measurement values after just 4 weeks of not
stretching, but group 4 still had more ROM than when
the study began. This finding may have been due to the
fact that the 60-second treatment resulted in greater
changes in ROM due to its greater rate of change and
the subjects in this group, therefore, had farther to
regress in order to return to pretest values. The slope for
the 60-second stretch was steeper for both the treatment
and recovery periods (Fig. 3). Thus, even though the
subjects in group 4 exhibited quicker improvements in
ROM, they also lost ROM during the 4-week recovery
period at a faster rate than the other groups. This
finding emphasizes the importance of continuing a
stretching regimen in order to maintain ROM gains.
Although it appears that longer-duration stretching
enhances ROM increases in elderly people, many ques-
tions remain unanswered with regard to stretching pro-
tocols in this population. Groups 2 through 4 stretched
for a daily total stretch time of 1 minute, 2 minutes, and
4 minutes, respectively. Further investigation is needed
to determine whether the improvement made by the
group that received the 60-second stretch was due to the
longer duration of stretching or due to the overall time
for stretching. Whether or not a single 60-second stretch
is as effective as repeated stretching in elderly people
also warrants further investigation. Future studies should
also compare 60-second stretches with longer periods of
stretching (ie, up to 2 minutes or longer) to determine
whether prolonged stretches further improve ROM or
enhance the residual effect.
Limitations of the Study
We examined the effects of repeated stretches of 15, 30,
and 60 seconds’ duration in the hamstring muscle group
on knee extension ROM in a group of elderly subjects.
Our subjects were predominantly Caucasian, and the
results may not be representative of other races. In
addition, the subjects were living in a retirement facility,
but they were independent in their activities of daily
living and thus may not be representative of people with
other characteristics. As 95% of our subjects were
between the ages of 75 and 95 years, further studies are
1116 . Feland et al
Physical Therapy . Volume 81 . Number 5 . May 2001

needed to determine whether the results of this study
can be generalized to middle-aged adults or to a younger
elderly population (65–75 years of age).
Conclusion
We demonstrated that 60-second stretching, repeated 4
times, once per day, 5 times per week for 6 weeks, can
yield a greater rate of improvement in knee extension
ROM than similar regimens of 15- or 30-second stretches
in elderly people. However, the groups that received 15-
and 30-second stretches had improvements in ROM
when compared with the group that had no stretching.
In order for ROM gains to be maintained, stretching
must be continued. The more active a person is, the
better his or her ROM will be prior to and after
treatment, regardless of treatment method. Stretching
one lower extremity will not necessarily improve the
ROM of the opposite lower extremity.
References
1
Hortoba´gyi T, Faludi J, Tihanyi J, Merkely B. Effects of intense
“stretching”-flexibility training on the mechanical profile of the knee
extensors and on the range of motion of the hip joint. Int J Sports Med.
1985;6:317–321.
2
Sady SP, Wortman M, Blanke D. Flexibility training: ballistic, static or
proprioceptive neuromuscular facilitation? Arch Phys Med Rehabil. 1982;
63:261–263.
3
Smith CA. The warm-up procedure: to stretch or not to stretch. A
brief review. J Orthop Sports Phys Ther. 1994;19:12–17.
4
Wallin D, Ekblom B, Grahn R, Nordenborg T. Improvement of
muscle flexibility: a comparison between two techniques. Am J Sports
Med. 1985;13:263–268.
5
Williford HN, Smith JF. A comparison of proprioceptive neuromus-
cular facilitation and static stretching techniques. Am Corr Ther J.
1985;39:30 –33.
6
Borms J, VanRoy P, Santens JP, Haentjens A. Optimal duration of
static stretching exercises for improvement of coxo-femoral flexibility.
J Sports Sci. 1987;5:39 – 47.
7
Halbertsma JPK, Van Bolhuis AI, Go¨eken LNH. Sport stretching:
effect on passive muscle stiffness of short hamstrings. Arch Phys Med
Rehabil. 1996;77:688 – 692.
8
Wilson GJ, Elliot BC, Wood BA. Stretch shorten cycle performance
enhancement through flexibility training. Med Sci Sports Exerc. 1992;24:
116 –123.
9
Worrell TW, Smith TL, Winegardner JW. Effect of hamstring stretch-
ing on hamstring muscle performance. J Orthop Sports Phys Ther.
1994;20:154 –159.
10
Godges JJ, MacRae H, Longdon C, et al. The effects of two
stretching procedures on hip range of motion and gait economy.
J Orthop Sports Phys Ther. 1989;10:350 –357.
11
Spence AP. Biology of Human Aging. Englewood Cliffs, NJ: Prentice-
Hall; 1989.
12
Buroker KC, Schwane JA. Does postexercise static stretching allevi-
ate delayed muscle soreness? The Physician and Sportsmedicine. 1989;17:
65– 83.
13
DeVries HA. Physiological effects of an exercise training regimen
upon men aged 52 to 88. J Gerontol A Biol Sci Med Sci. 1970;25:325–336.
14
Walter J, Figoni SF, Andres FF, Brown E. Training intensity and
duration in flexibility. Clinical Kinesiology. 1996;50:40 – 45.
15
Sullivan MK, Dejulia JJ, Worrell TW. Effect of pelvic position and
stretching method on hamstring muscle flexibility. Med Sci Sports Exerc.
1992;24:1383–1389.
16
Bandy WD, Irion JM, Briggler M. The effect of time and frequency
of static stretching on flexibility of the hamstring muscles. Phys Ther.
1997;77:1090 –1096.
17
Bandy WD, Irion JM. The effect of time on static stretch on the
flexibility of the hamstring muscles. Phys Ther. 1994;74:845– 850.
18
Taylor DC, Dalton JD, Seaber AV, Garrett WE. Viscoelastic proper-
ties of muscle-tendon units: the biomechanical effects of stretching.
Am J Sports Med. 1990;18:300 –309.
19
Brooks SV, Faulkner JA. Skeletal muscle weakness in old age:
underlying mechanisms. Med Sci Sports Exerc. 1994;26:432– 439.
20
Buckwalter JA, Woo SL, Goldberg VM, et al. Soft tissue aging and
musculoskeletal function. J Bone Joint Surg Am. 1993;75:1533–1548.
21
Timiras PS, ed. The Physiological Basis for Aging and Geriatrics. 2nd ed.
Boca Raton, Fla: CRC Press; 1994.
22
Enoka RM. Neuromechanical Basis of Kinesiology. 2nd ed. Champaign,
Ill: Human Kinetics; 1994.
23
Sapega AA, Quedenfeld TC, Moyer RA, Butler RA. Biophysical
factors in range-of-motion exercise. The Physician and Sportsmedicine.
1981;9:57– 65.
24
Kisner C. Therapeutic Exercise: Foundations and Techniques. 2nd ed.
Philadelphia, Pa: FA Davis Co; 1990.
25
Raab DM, Agre JC, Mcadam M, Smith EL. Light resistance and
stretching exercise in elderly women: effect upon flexibility. Arch Phys
Med Rehabil. 1988;62:268 –272.
26
Girouard CK, Hurley BF. Does strength training inhibit gains in
range of motion from flexibility training in older adults? Med Sci Sports
Exerc. 1995;27:1444 –1449.
27
Mills EM. The effect of low-intensity aerobic exercise on muscle
strength, flexibility, and balance among sedentary elderly persons.
Nurs Res. 1994;43:207–211.
28
Chapman EA, DeVries HA, Swezey R. Joint stiffness: effects of
exercise on young and old men. J Gerontol A Biol Sci Med Sci. 1972;27:
218 –221.
29
Norkin CC, White DJ. Measurement of Joint Motion: A Guide to
Goniometry. 2nd ed. Philadelphia, Pa: FA Davis Co; 1995.
30
Voorrips LE., Ravelli ACJ, Dongelmans PCA, et al. A physical activity
questionnaire for the elderly. Med Sci Sports Exerc. 1991;23:974 –979.
31
Hagbarth KE, Ha¨gglund JV, Nordin M, Wallin EU. Thixotropic
behaviour of human finger flexor muscles with accompanying changes
in spindle and reflex responses to stretch. J Physiol. 1985;368:323–342.
32
Lakie M, Robson LG. Thixotropic changes in human muscle
stiffness and the effects of fatigue. QJ Exp Physiol. 1988;73:487–500.
33 SAS/STAT Software: Changes and Enhancements Through Release 6.12.
Cary, NC: SAS Institute Inc; 1999.
34
Keselman HJ, Huberty CJ, Lix LM, et al. Statistical practices of
educational researchers: an analysis of their ANOVA, MANOVA, and
ANCOVA analyses. Review of Educational Research. 1998;68:350 –386.
35
James B, Parker AW. Active and passive mobility of lower limb joints
in elderly men and women. Am J Phys Med Rehabil. 1989;68:162–167.
36
Moore MA, Hutton RS. Electromyographic investigation of muscle
stretching techniques. Med Sci Sports Exerc. 1980;12:322–329.
Physical Therapy . Volume 81 . Number 5 . May 2001
Feland et al . 1117
ўўўўўўўўўўўўўўўўўўўўўўўўўўў
ў
Wyszukiwarka
Podobne podstrony:
76 1075 1088 The Effect of a Nitride Layer on the Texturability of Steels for Plastic Moulds
Curseu, Schruijer The Effects of Framing on Inter group Negotiation
A systematic review and meta analysis of the effect of an ankle foot orthosis on gait biomechanics a
Glińska, Sława i inni The effect of EDTA and EDDS on lead uptake and localization in hydroponically
Understanding the effect of violent video games on violent crime S Cunningham , B Engelstätter, M R
The Effect of Childhood Sexual Abuse on Psychosexual Functioning During Adullthood
On the Effectiveness of Applying English Poetry to Extensive Reading Teaching Fanmei Kong
The Effects of Psychotherapy An Evaluation H J Eysenck (1957)
The effect of temperature on the nucleation of corrosion pit
The Effect of DNS Delays on Worm Propagation in an IPv6 Internet
The effect of sol
the effect of interorganizational trust on make or cooperate decisions deisentangling opportunism de
The effect of Nd
Ebsco Cabbil The Effects of Social Context and Expressive Writing on Pain Related Catastrophizing
How to assess the effectiveness of your anti virus
The effects of Chinese calligraphy handwriting and relaxation training on carcinoma patients
NSA Reducing the Effectiveness of Pass the Hash
Microwave drying characteristics of potato and the effect of different microwave powers on the dried
Jack Anderson The effects of embeddeddness on enterpreneurial proccess
więcej podobnych podstron