P5140030
Shoulder Instability, Anterior or Muitiaxial
Shoulder instabilities can develop after acute dislocations, chronic subłuxaHon/ or long term overuse acthities which stretch the shoulder capsule (baseball pitchers, tertnis, javelin). In most cases the instability is the result o/ ań acute injury to the anterior region of the shoulder capsule.
Kinesio Tape is not designed to mechanically stop a motion or movement of a body tissue. It does not have the tensile strength to stop the humerał head from dislocating, it can provide a proprioceptive stimulus thmugh the skin that will cause the bodies tissues to adjust.
The Kinesio taping techniąue will assist in redudng edema, pain and providc proprioceptive stimu-lus.
ar
I
i

Application of the lymphatic corrective technique to reduce edema resulting from inflammation durin* acute phase. Two lymphatic corręction strips will be applied. For review see lymphatic corrective tech-nique.
Posterion begin by placing the base of the Kinesio • fan strip near the middie one third of the spine of the scapula, direct the tai Is of the fan over the AC joint j and towards the anterior deltoid region.
Anterior: begin by placing the base of the Kinesio f
_K fan strip near the middie one third of the clavicle, -I
direct the taiis of the fan over the AC joint towards I the posterior deltoid region.
The two strips should form a crisscross pat tern. '
Depending upon the evaluation by the practitio- ' ner, a basie deltoid muscle taping technique may be applied. Th is may be found to benefit overall shoulder support shoulder instability.
The practitioner may also determine that addi- | tional muscles may require basie muscle applicatioti f to assist with shoulder pain or weakness.

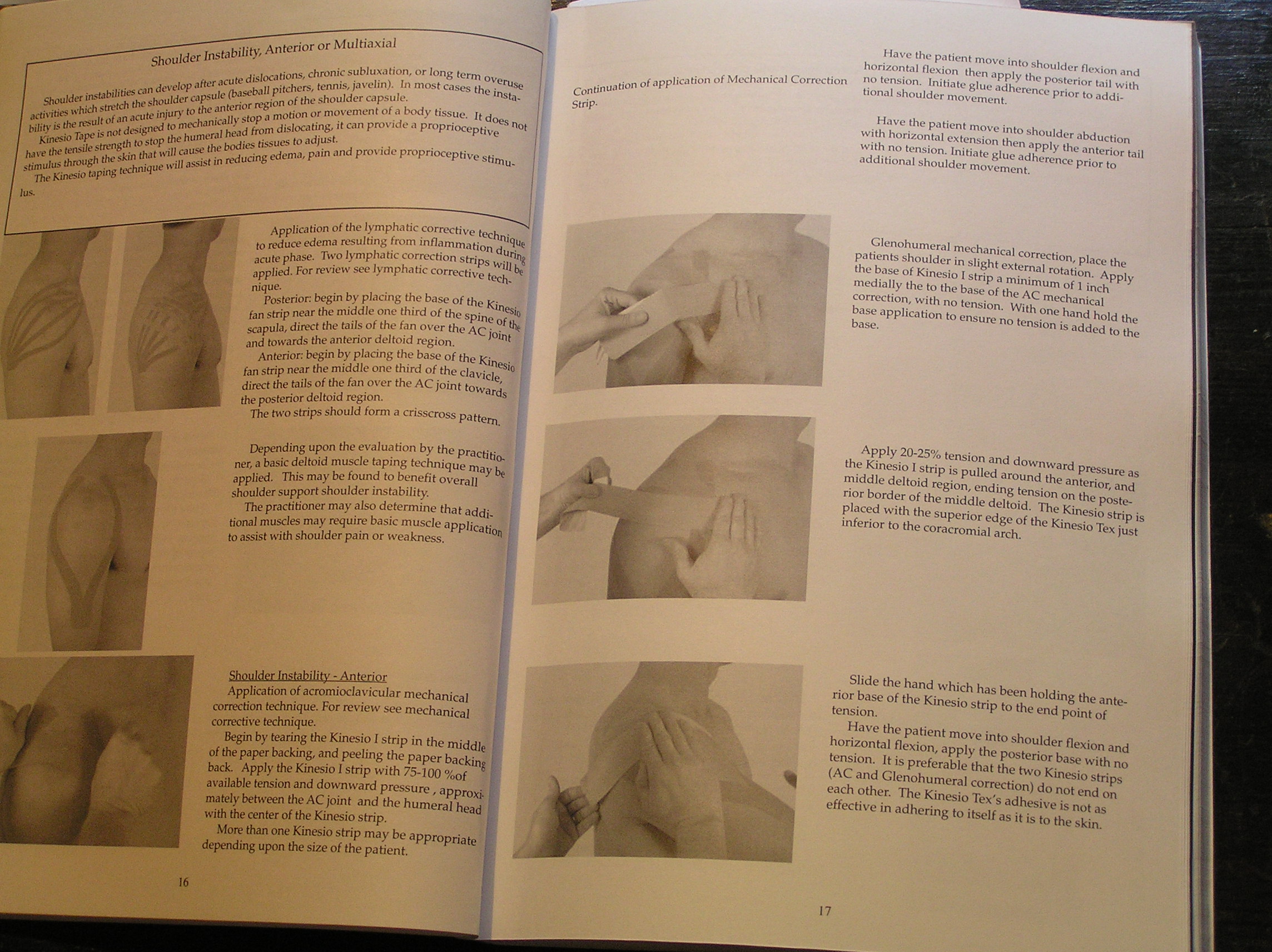
Shoulder Instability - Anterior Application of acromioclavicular mechanical corręction technique. For review see mechanical cotrective technique.
Begin by tearing the Kinesio I strip in the middie 1 of the paper backing, and peeling the paper backing n back. Apply the Kinesio 1 strip with 75-100 %of available tension and downward pressure, approxJ K mately between the AC joint and the humerał head m with the center of the Kinesio strip.
Morę than one Kinesio strip may be appropriate ■ m depending upon the size of the patient.
Con^u Strip
.lication of Mechanical Corręction
Have the patient move into shoulder flcxion and horizontal flexion Ihen apply the posterior taił with no tension. Initiate glue adherence prior to addi-tional shoulder movement.
Have the patient move into shoulder abduction with horizontal extension then apply the anterior taił with no tension. Initiate glue adherence prior to shoulder movement.
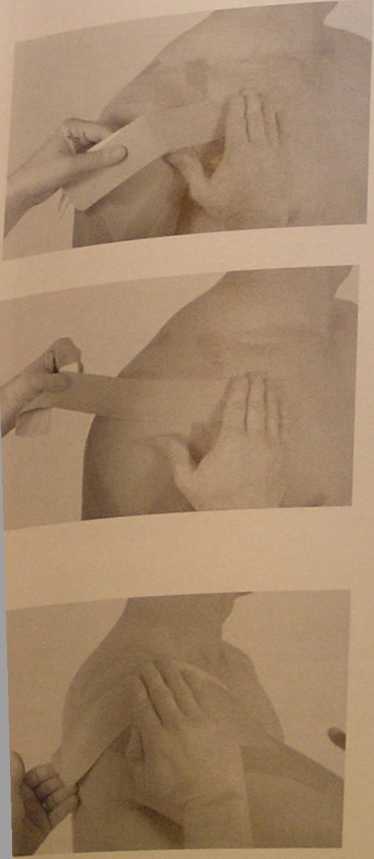
Glenohumeral mechanical corręction, place the patients shoulder in slight extemal rotation. Apply the base of Kinesio I strip a minimum of 1 inch medially the to the base of the AC mechanical corręction, with no tension. With one hand hołd the base application to ensure no tension is added to the base.
Apply 20-25% tension and downward pressure as the Kinesio I strip is pulled around the anterior, and middie deltoid region, ending tension on the posterior border of the middie deltoid. The Kinesio strip is placed with the superior edge of the Kinesio Tex just inferior to the coracromial arch.
Slide the hand which has been holding the anterior base of the Kinesio strip to the end point of tension.
Have the patient move into shoulder flexion and horizontal flexion, apply the posterior base with no tension. It is preferable that the two Kinesio strips (AC and Glenohumeral corręction) do not end on each other. The Kinesio Tex's adhesive is not as effeetiye in adhering to itself as it is to the skin.
17
Wyszukiwarka
Podobne podstrony:
pg093 Evenrg crcn itesgrtShoulder drapes Shouldtr drapes can ba an miegral porj ol a dtess or they c
iI crystal, or magnetic—can be employed. Stereo or mono tape recordings can be madę using the monito
About Views Views are customized prcsentations of data in one or morc tablcs or other views. You can
Using Data Recovery Advisor The recovery proccss bcgins when you cither suspect or discover a failur
Slip Stitch Patterns Whether the are worked in 4 the same or difTerent colors, you can aeate
particles of acidic or basie character, IR spectroscopy (also after pyridine adsorption) and NMR spe
DSC01982 Traumatic reticuloperitonitis (TRP) signs of chronic stagc S to 7 days after acute stage, n
img452 (6) Unit Language focus Vocabulary Professional practice 10 Business or pleasure? Modal ver
P5140031 Completed example of possible Kinesio Taping Technique for shoulder instability -
P5140098 theThe sccond strip should be posterior medial aspect of the CnłfC<?d from anterior
Download Manuał de Seguridad e Higiene Industrial PDF eBooks Free food, or should I say fats food, T
p24 (20) Servicing Circuit Breaker and Ignition Timer Circuit breaker points that are bumed or pitte
pg062 St *34M &0C<* The term strapless means that the bodoe is not supoorted by shouldcr sc
więcej podobnych podstron