Psychological Aspects of
Treatment of the Somatic
Patient
PART 2
The doctor – patient relationship and the
selected aspects of psychosomatic
diagnosis
Magdalena Lazarewicz, Dept. of Medical Psychology, Warsaw Medical University
magda.lazarewicz@gmail.com
Last week
The Doctor – Patient Relationship
Barriers of Interpersonal Communication
Models of Doctor - Patient relationship
Principles underlying development of good
doctor-patient relationship
Iatrogenic errors - introduction

Today…
Homework – summary
Communication - exercise
Iatrogenic errors - summary
Appropriate information
Selected aspects of psychosomatic
diagnosis
Communicatio
n
Delay at the polish airport…
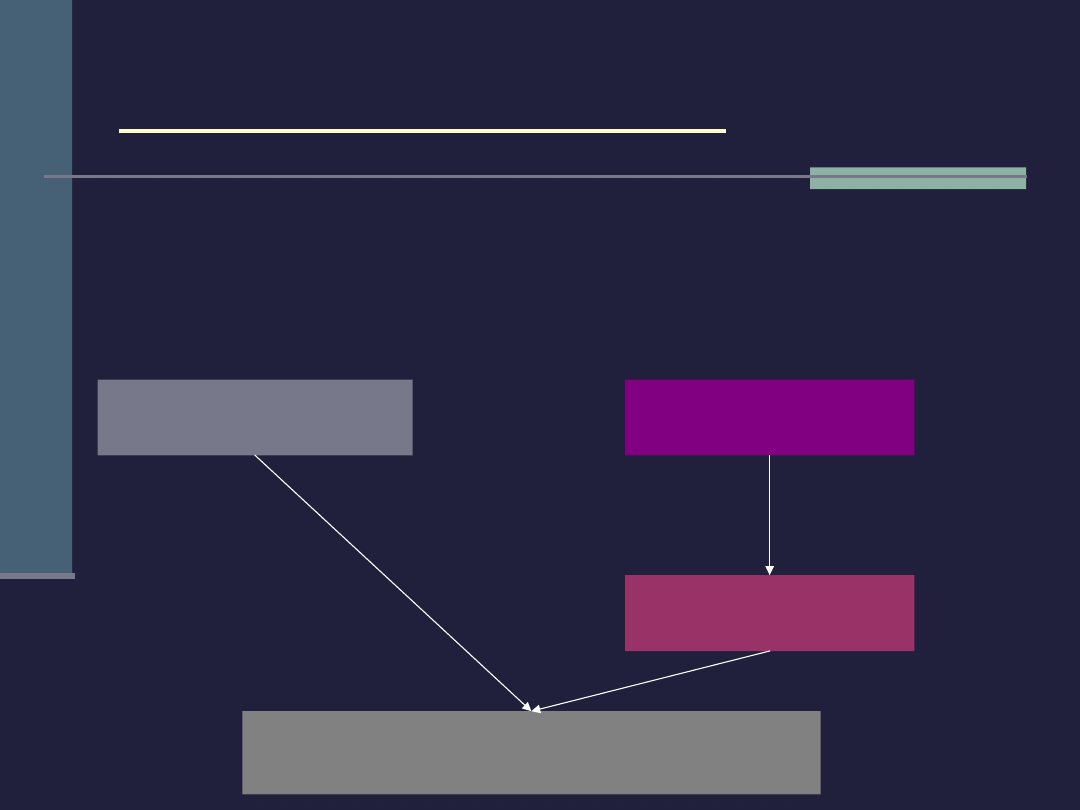
Iatrogenic errors 1
An error committed by the doctor or other member of the medical
staff which leads to deterioration of the patient’s state of health.
wrong direct physical
intervention
improper or
tactless behaviour
deterioration of the patient’s
health
psychological
effects
Direct
error
Indirect
error
Iatrogenic errors 2
during the medical
examination
during treatment
disturbed interpersonal
communication
Indirect iatrogenic
errors
Examining the patient
in the presence of
other patients (or
unnecessary medical
stuff)
Some uncontrolled
behaviours (nodding
seriously, gasping)
Useless additional
tests and „taking the
patient by surprise”
Unnecessary
prescription of an
excessive amount of
medication
Frequent issuing of
sick-leave
Unjustified
qualification of
patients for invalid
pension
Lack of any information,
more or less incomplete
information
Unintentionally raising the
patient’s fears in order to
encourage the patient to
comply more diligently with
the doctor’s orders
Highly professional „slang”
Going around one’s own
business when interviewing
the patient
Appropriate information as an
expression of proper doctor-patient
relations
The doctor as a main source of
information
What does „appropriate information”
mean?
Diagnosis and causes of the
disease
Predicted course of the illness
and the prognosis
Planned treatment
Practical instructions (workout,
diet etc)
Empirical studies – S. Miller
• Pulse rate
: prior to the information, after the information, after the
diagnostic procedure.
• Relationship between
compatibility/incompatibility of the information
with the patient’s need for information and emotional tension
Information
seekers
Information
avoiders
Detailed
information
concerning the
diagnostic
procedure
Detailed
information
concerning the
diagnostic
procedure
Minimal
information
concerning the
diagnostic
procedure
Minimal
information
concerning
the diagnostic
procedure
Patients (vaginal endoscopy)
A
B
C
D
Empirical studies – S. Miller
The number of details which the doctor conveys in
his/her information should be adjusted to the
patients individual expectations
Information
seekers
Information
avoiders
Detailed
information
concerning the
diagnostic
procedure
Detailed
information
concerning the
diagnostic
procedure
Minimal
information
concerning the
diagnostic
procedure
Minimal
information
concerning
the diagnostic
procedure
Patients (vaginal endoscopy)
A
B
C
D
Less tension
Less tension
Oral Information –
reccomendations for improving
complience*
*compliance – „the extent to which the patient’s
behaviour
(in terms of taking medication, following diets or
other lifestyle changes)
coincides with medical or health
advice”
(Haynes et al., 1979)
Primacy Effect – patients have a tendency to
remember the first thing they are told
Stress the importance of compliance
Simplify the information
Use repetition
Be specific
Follow-up the consultation with additional
interviews
Objective and range of
psychosomatic interview
To extend the information concerning the patient
Description of the psychosocial determinants of the disease
and its consequences and also the psychosocial aspects of
the treatment process
The meaning which the particular patient ascribes to his/her
disease
type of disease
moment of onset
the need hierarchy
Attitude Towards Illness
attitudes of the nearest environment towards patient
Psychosomatic diagnosis layout
General information: age, sex, occupation
Medical diagnosis
Observational data
appearance
Indices of emotional tension
Patient’s behaviour during examination
Psychological risk factors and factors affecting the course of
illness
Attitude Towards Illness
Cognitive components
Motivational components
Emotional components
Basic problems
Assessment of relationship with the patient
Indications for doctor in charge, the patient, the patient’s
family and psychologist (if necessary) resulting from the
psychosomatic diagnosis
The psychosomatic
interview
AIM: to collect information* on the
interviewee, from the interviewee and
from other people who know the
interviewee.
* information on the various spheres of the patient’s life and
functioning which are important for the diagnosis
The interviewer has to …
develop sufficient motivation in the
interviewee so that he/she will be encouraged
to share significant information
weaken motivation which is counter-productive
to communication
Fear of the interviewer’s moral evaluation and
criticism
Fear that the information will be used to harm the
interviewee
Fear of bringing to daylight certain facts from the
interviewee’s life
Fear that the interviewer will „look him/her through”
The psychosomatic
interview
Observation
Verbal contact
Observational data
Objective – a thorough description of
the observed facts (no premature
interpretations)
It is a source of hypothesis which may
modify the course of the interview
It allows the interviewer to monitor the
emotional state of the interviewee
In is a source of diagnostic information

What shell we pay attention
to?
Appearance:
Height, weight, build, skin, nails
General hygiene, dress, hair-style, make-up
Emotional tension:
Tears, shiny eyes, paling and reddening of the face,
quickened breathing, sweating, trembling of the hands and
feet, shaky fingers
Excessive self-composure, rigidity (lack of spontaneity,
gesticulation, facial expression, shifting of the body position)
General mood:
Facial expression, gesticulation, eye expression
Adequacy of emotional behaviour to situation
Formal characteristics of speech:
Speech intensity, dynamics, tone, articulation, logic,
adequacy of response to questions, level of abstraction,
speech fluency etc
Halo-effect
The importance of the first impression
source of hypothesis
source of negative feelings or prejudice
source of positive feelings
„The only way to avoid one’s errors is to
analyze and correct one’s behaviour.”
(Wallen)

Developing a REAL
relationship
Have an „open” attitude: whatever is going on
between us in interaction is important and
intimate, no matter what is being discussed.
Develop in the interviewee a feeling that he/she is
accepted
Concentrate all your attention on the interviewee
Help the interviewee to express those contents
which are important for the diagnosis
Create a calm and unhurried atmosphere
Listen kindly with empathy
Do not express surprise
First minutes…
Try not to be late…
Concentrate fully and only at the
patient
Take care of the patients comfort
Organize the environment
Pay attention to the physical
distance
Introduce yourself…
The Art of asking questions
The first question: general, open, refer
to the interviewee’s general life
situation or the presenting problem
What brings you here?
What can I do for you?
What is your problem?
Why are you here? (in the hospital)
Could you tell me a bit more about …

The Art of asking questions
Narrowing down the questions (general to
specific)
Progression (relatively benign to personal)
Embedded Questions (hidden among
others)
Leading questions (indirect)
Postponed questions (change of context,
better moment)
Projective questions („some people…”,
description of interpersonal situation)
Language…
The language must be matched to:
interviewee’s intelectual level
verbal skills
personal experience
Avoid the proffesional language and
shortenings
How to maintain the rapport?
Verbal signals:
„Yes”, „I understand”, „Yhym”
„Could you tell me more about this?”
Paraphrasing
Silence
Nonverbal signals:
Body posture
Tilt of the head
Facial expression
Gestures
Eye expression
Smiling
Synchronisation
When the interview comes to
a close…
Check whether all problems have been discussed and leave
some time for their discussion
When time is up – communicate it directly instead of
constantly checking the time or „suggesting” that you have
to go (e.g.. By gathering the notes impatiently)
Try to summarize the interview
Finish the conversation stressing your interest in the
interviewee and in what has been said
You can ask the patient to evaluate the conversation
Say good-bye, get up and thank the interviewee for coming.
Psychosomatic diagnosis is
based on:
Information collected in an interview +
observational data + case history
What the patient said and what he
didn’t want to talk about (!)
It’s better to formulate questions than
premature statements.

Indications
For the doctor in charge, family, patient
and psychologist
General or/and specific
Realistic and constructive
Literature
This week reading:
Basic textbook, pages 81-92.
For the next week:
Prepare for your case role-playing
search the Internet for necessary information; imagine
what kind of person you will role-play; think of the first
question; think of your goals; try to imagine your patients
needs and problems etc.
Document Outline
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
Wyszukiwarka
Podobne podstrony:
The doctor and his patient
Juvenile Psychopaths The Super Predator of Crime
PSYCHOLOGIA the best, TiR UAM II ROK, Psychologia
Medical Psychology 4 effects of disease, IC, ATI
at the doctor's dialogues
Rok temu moje życie legło w gruzach, Psychomanipulacja, !!! THE SECRET, THE OPUS, THE COMPASS, SEKR
The Doctor Wont See You Now
28 At the doctor
Sarbin Narrative psychology, the storied nature of human conduct str vii, ix, 3 63, 117 125
at the doctor´s exercises
Supportive Psychotherapy for Borderline Patients
Lust s What The Doctor Ordered
B K , Wright The Doctors Secret
ANTIBIOTIC USE IN THE AVIANEXOTIC PATIENT
At the doctor s busuu
The Diamondback Ranch 1 The Doctor Wears A Stetson
You are at the doctor s surgery
NSSI in Young Adolescent Girls Moderators of the Distress Function Relationship
więcej podobnych podstron