Diabetes Mellitus -
Management
Jan Szewieczek
Jan Szewieczek
Katedra i Klinika
Katedra i Klinika
Chorób Wewnętrznych i Metabolicznych
Chorób Wewnętrznych i Metabolicznych
Śl.A.M. Katowice
Śl.A.M. Katowice

Principals
Prevention of diabetes
Prevention of diabetes
Early recognition
Early recognition
Complex management
Complex management
Education
Education
Monitoring
Monitoring
Clinical
Clinical
Self-monitoring
Self-monitoring
Regular treatment
Regular treatment
Non-pharmacological (nutrition, body mass control,
Non-pharmacological (nutrition, body mass control,
physical activity)
physical activity)
Pharmacological (oral hipoglicaemic drugs, insulin)
Pharmacological (oral hipoglicaemic drugs, insulin)
Secondary prophylaxis
Secondary prophylaxis
Management in acute complications
Management in acute complications

Education (1)
A salient goal for diabetes care
A salient goal for diabetes care
is to enable each person with
is to enable each person with
diabetes to lead
diabetes to lead
the health-care team involved
the health-care team involved
in the management of their
in the management of their
diabetes
diabetes

Education (2)
It is the right of each person with diabetes
It is the right of each person with diabetes
to become empowered to derive the
to become empowered to derive the
maximum benefit from the health-care
maximum benefit from the health-care
system
system
It is the responsibility of the diabetes team
It is the responsibility of the diabetes team
to ensure that the person with diabetes
to ensure that the person with diabetes
can follow the life-style of their educated
can follow the life-style of their educated
choice, based on the three elements
choice, based on the three elements
of empowerment: knowledge, behavioural
of empowerment: knowledge, behavioural
skills, and self-responsibility
skills, and self-responsibility

Education (3)
The aims of education and
The aims of education and
training are to provide
training are to provide
information in an acceptable
information in an acceptable
form,
form,
in order that people with diabetes
in order that people with diabetes
develop the knowledge to self-
develop the knowledge to self-
manage their diabetes
manage their diabetes
and empower them to make
and empower them to make
informed choices in their life
informed choices in their life
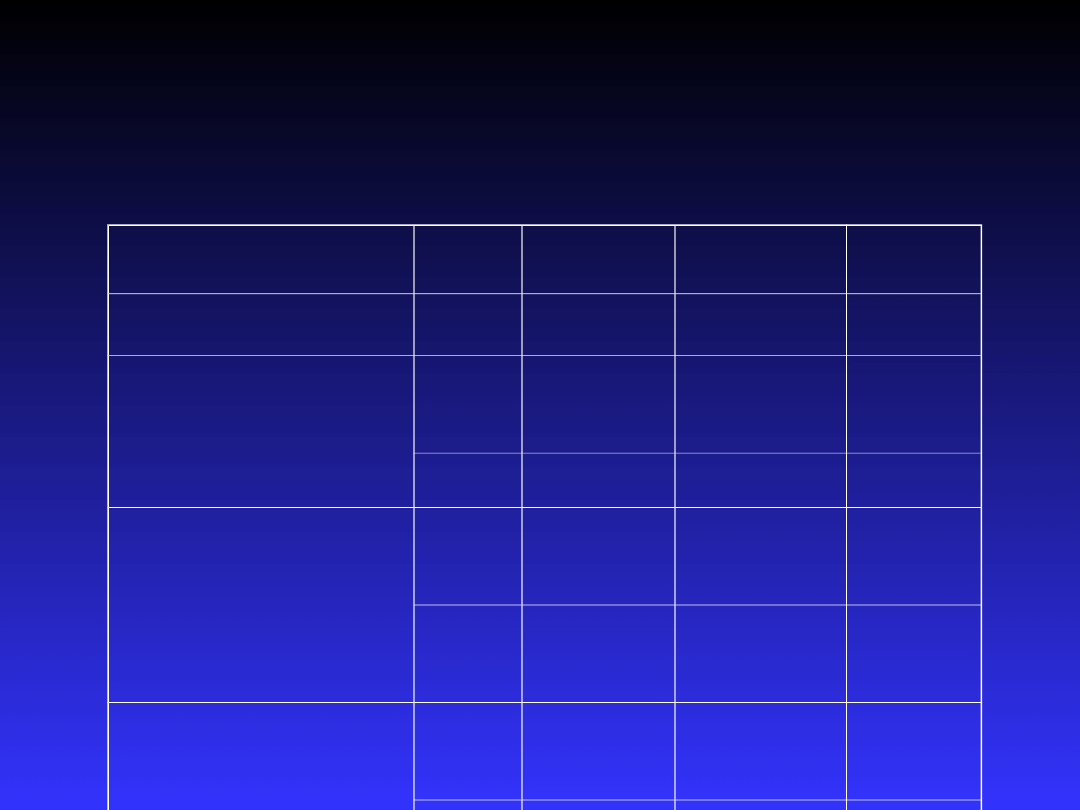
Schedule for clinical monitoring at
different types of visit (1)
Review topics
Review topics
Initial
Initial
review
review
/
/
referral
referral
Regular
Regular
review
review
Annual
Annual
review
review
Long-term and/or recent diabetes
Long-term and/or recent diabetes
history
history
Social history / lifestyle review
Social history / lifestyle review
Diabetes understanding / self-
Diabetes understanding / self-
management
management
Self-monitoring skills / results
Self-monitoring skills / results
Complications history and/or symptoms
Complications history and/or symptoms
Smoking
Smoking
If
If
problem
problem
Other medical history / systems review
Other medical history / systems review
Family history diabetes / arterial disease
Family history diabetes / arterial disease
Drug history / current drugs
Drug history / current drugs
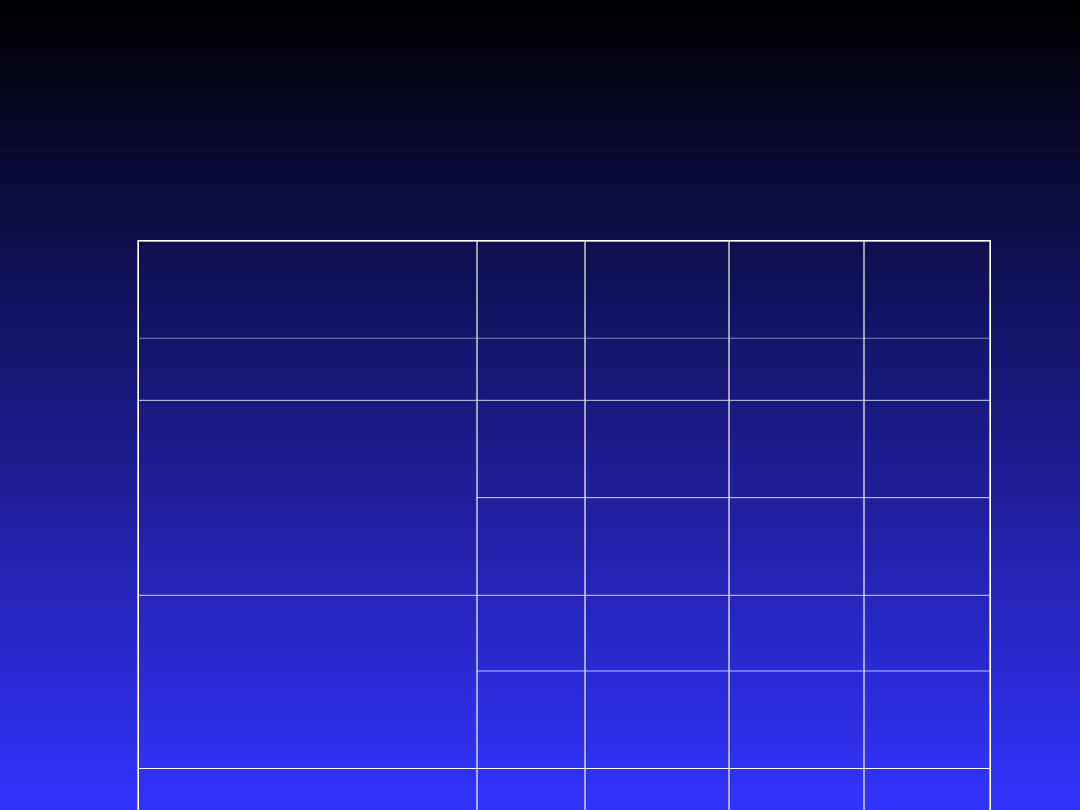
Schedule for clinical monitoring at
different types of visit (2)
Review topics
Review topics
Initial
Initial
review
review
/
/
referral
referral
Regular
Regular
review
review
Annual
Annual
review
review
Weight / body mass index
Weight / body mass index
General examination
General examination
Foot examination / injection sites
Foot examination / injection sites
If
If
problem
problem
Eye / vision examination
Eye / vision examination
If
If
problem
problem
Blood pressure
Blood pressure
If
If
problem
problem
Glycated haemoglobin
Glycated haemoglobin
Lipid profile*
Lipid profile*
If
If
problem
problem
Urine protein
Urine protein
Urine albumin excretion**
Urine albumin excretion**
If
If
problem
problem
Serum creatinine
Serum creatinine
If
If
problem
problem
Nutritional management
Nutritional management is an
Nutritional management is an
integral part of initial and
integral part of initial and
continuing education
continuing education
programmes
programmes

Healthy eating
Advise
Advise
carbohydrate intake should be higher, and fat intake
carbohydrate intake should be higher, and fat intake
lower than that of most Europeans, but not different from
lower than that of most Europeans, but not different from
recommendations for the population in general
recommendations for the population in general
The proposed contribution to energy intake should be :
The proposed contribution to energy intake should be :
Fat:
Fat:
saturated fat <10 %; replace excess saturated fat
saturated fat <10 %; replace excess saturated fat
with monounsaturates, or polyunsaturates ( up to 10 % ), or
with monounsaturates, or polyunsaturates ( up to 10 % ), or
carbohydrate
carbohydrate
Carbohydrate:
Carbohydrate:
around 50-55 %. Use foods containing
around 50-55 %. Use foods containing
soluble fibre in a carbohydrate rich diet. Simple sugars need
soluble fibre in a carbohydrate rich diet. Simple sugars need
not be rigorously excluded from the diet, but often need to
not be rigorously excluded from the diet, but often need to
be limited
be limited
Protein:
Protein:
around 15 %
around 15 %
Recommend
Recommend
fresh fruit and vegetables
fresh fruit and vegetables

Nutritional management in
DM 1
Meal patterns
Meal patterns
Multiple injection regimens
Multiple injection regimens
:
:
Advise
Advise
snacks will help to attain better blood glucose control,
snacks will help to attain better blood glucose control,
but use self-monitoring to learn what is necessary and
but use self-monitoring to learn what is necessary and
desirable
desirable
Advise
Advise
on flexibility to adjust meal timing and content
on flexibility to adjust meal timing and content
( together with insulin doses ) without affecting blood glucose
( together with insulin doses ) without affecting blood glucose
control. But
control. But
warn
warn
about the temptations of extra total calories
about the temptations of extra total calories
Rapid-acting insulin analogue regimens
Rapid-acting insulin analogue regimens
:
:
Advise
Advise
snacks only if self-monitoring suggests a need; check
snacks only if self-monitoring suggests a need; check
particularly if a high insulin analogue dose is needed to
particularly if a high insulin analogue dose is needed to
correct hyperglycaemia present pre-prandially
correct hyperglycaemia present pre-prandially

PHYSICAL EXERCISE
Advise
Advise
that physical exercise :
that physical exercise :
can benefit insulin sensitivity, hypertension, and blood lipid control
can benefit insulin sensitivity, hypertension, and blood lipid control
should be taken at least every 2-3 days for optimum effect
should be taken at least every 2-3 days for optimum effect
may increase the risk of acute and delayed hypoglycaemia
may increase the risk of acute and delayed hypoglycaemia
Manage
Manage
physical exercise using :
physical exercise using :
self-monitoring to learn about the exercise response, and the effects
self-monitoring to learn about the exercise response, and the effects
of insulin and dietary changes on this
of insulin and dietary changes on this
a prospective reduction in insulin dose for regular exercise
a prospective reduction in insulin dose for regular exercise
additional carbohydrate as necessary
additional carbohydrate as necessary
warnings :
warnings :
o
o
about delayed hypoglycaemia, especially with more prolonged,
about delayed hypoglycaemia, especially with more prolonged,
severe, or unusual exercise, and a possible need for less insulin overnight
severe, or unusual exercise, and a possible need for less insulin overnight
and the next day
and the next day
O
O
that exercise during insulin deficiency will raise blood glucose and
that exercise during insulin deficiency will raise blood glucose and
ketone levels
ketone levels
O
O
that alcohol may exacerbate the risk of hypoglycaemia after exercise
that alcohol may exacerbate the risk of hypoglycaemia after exercise
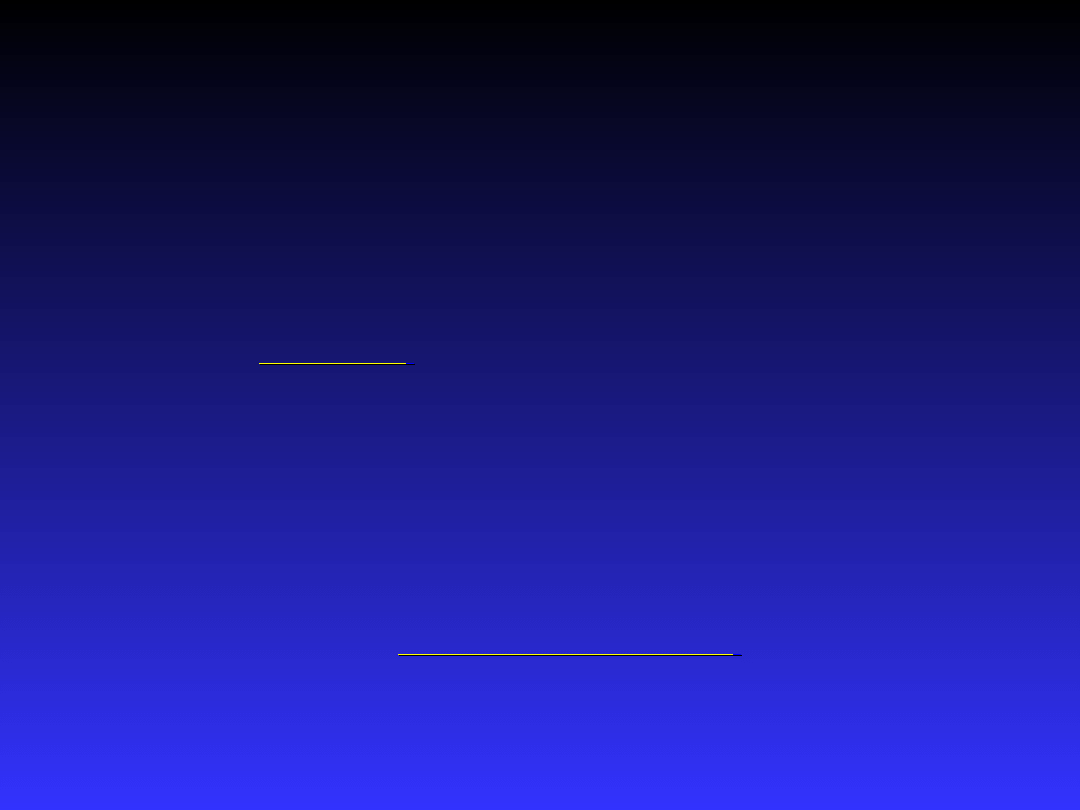
Glucose control assessment
levels in DM 1
Non-
Non-
diabetic
diabetic
Adequate
Adequate
Inadequa
Inadequa
te
te
HbA
HbA
1c
1c
%Hb
%Hb
<6.1
<6.1
6.2-7.5
6.2-7.5
>7.5
>7.5
Fasting / pre-
Fasting / pre-
prandial
prandial
mmol/
mmol/
l
l
4.0-
4.0-
5.0
5.0
5.1-6.5
5.1-6.5
>6.5
>6.5
mg/dl
mg/dl
70-90
70-90
91-120
91-120
>120
>120
Post-prandial
Post-prandial
(peak)
(peak)
mmol/
mmol/
l
l
4.0-
4.0-
7.5
7.5
7.6-9.0
7.6-9.0
>9.0
>9.0
mg/dl
mg/dl
70-
70-
135
135
136-
136-
160
160
>160
>160
Pre-bed
Pre-bed
mmol/
mmol/
l
l
4.0-
4.0-
5.0
5.0
6.0-7.5
6.0-7.5
>7.5
>7.5
mg/dl
mg/dl
70-90
70-90
110-
110-
135
135
>135
>135

Insulin, injections, and
associated education
(1)
Advise
Advise
:
:
the use of unmodified ( soluble, regular ) human
the use of unmodified ( soluble, regular ) human
insulin before each meal, and human NPH insulin in
insulin before each meal, and human NPH insulin in
combination unless :
combination unless :
o
o
multiple injection therapy is not wanted by the person
multiple injection therapy is not wanted by the person
with diabetes
with diabetes
o
o
flexibility of life-style is not important
flexibility of life-style is not important
o
o
insulin secretory capacity is high ( honeymoon period )
insulin secretory capacity is high ( honeymoon period )
o
o
insulin analogue therapy is indicated ( see below )
insulin analogue therapy is indicated ( see below )
the use of pen systems for insulin delivery
the use of pen systems for insulin delivery
the use of the abdominal wall for meal-time injections, and
the use of the abdominal wall for meal-time injections, and
the thigh for extended-acting insulin; advise also rotation of
the thigh for extended-acting insulin; advise also rotation of
sites within these areas
sites within these areas
Insulin, injections, and
associated education
(2)
Enable
Enable
the person with diabetes to :
the person with diabetes to :
handle the injection device proficiently and confidently,
handle the injection device proficiently and confidently,
including re-suspension of NPH crystals, insulin storage, and disposal
including re-suspension of NPH crystals, insulin storage, and disposal
self-monitor
self-monitor
accurately and easily at appropriate times
accurately and easily at appropriate times
place insulin consistently into deep subcutaneous tissue,
place insulin consistently into deep subcutaneous tissue,
usually by means of a lifted skin flap with the injection device at a
usually by means of a lifted skin flap with the injection device at a
45° angle
45° angle
prevent, recognize and manage hypoglycaemia
prevent, recognize and manage hypoglycaemia
understand the absorption characteristics of the two insulin
understand the absorption characteristics of the two insulin
preparations used, and changes of insulin requirement with meal
preparations used, and changes of insulin requirement with meal
size and physical activity, thus allowing them to learn insulin dose
size and physical activity, thus allowing them to learn insulin dose
self-adjustment
self-adjustment
access the
access the
diabetes professional team
diabetes professional team
freely for advice
freely for advice
manage sickness and travel successfully
manage sickness and travel successfully

Insulin, injections, and
associated education
(3)
Expect
Expect
:
:
overnight basal requirements to
overnight basal requirements to
require up to 50 % of total dose
require up to 50 % of total dose
unmodified insulin to last for 6-8
unmodified insulin to last for 6-8
hours, and therefore sometimes to
hours, and therefore sometimes to
overlap into the next meal or into the
overlap into the next meal or into the
night; reduce doses accordingly
night; reduce doses accordingly
high pre-breakfast insulin
high pre-breakfast insulin
requirements, due to insulin deficiency at
requirements, due to insulin deficiency at
the end of the night
the end of the night

Rapid-acting insulin
analogue regimens
Make
Make
the following changes when using rapid-acting
the following changes when using rapid-acting
analogues compared to unmodified human insulin:
analogues compared to unmodified human insulin:
monitor the effect of a short-acting analogue post-
monitor the effect of a short-acting analogue post-
prandially ( at 1-2 h ), and always less than 4 h after injection
prandially ( at 1-2 h ), and always less than 4 h after injection
expect to use lower pre-meal insulin doses than with
expect to use lower pre-meal insulin doses than with
human insulin
human insulin
use combined NPH + analogue injection before meals,
use combined NPH + analogue injection before meals,
if the between-meal interval is to be greater than 5 h
if the between-meal interval is to be greater than 5 h
use a higher late-evening NPH dose ( unless the aim is
use a higher late-evening NPH dose ( unless the aim is
specifically to deal with a problem of night-time
specifically to deal with a problem of night-time
hypoglycaemia )
hypoglycaemia )
use late-evening NPH no longer than 4 h after the evening
use late-evening NPH no longer than 4 h after the evening
analogue injection
analogue injection

Vascular risk in people
with Type 1 diabetes
Manage arterial risk
Manage arterial risk
aggressively in people with
aggressively in people with
Type 1 diabetes
Type 1 diabetes
if any other risk factor is
if any other risk factor is
abnormal including family
abnormal including family
history of arterial disease
history of arterial disease
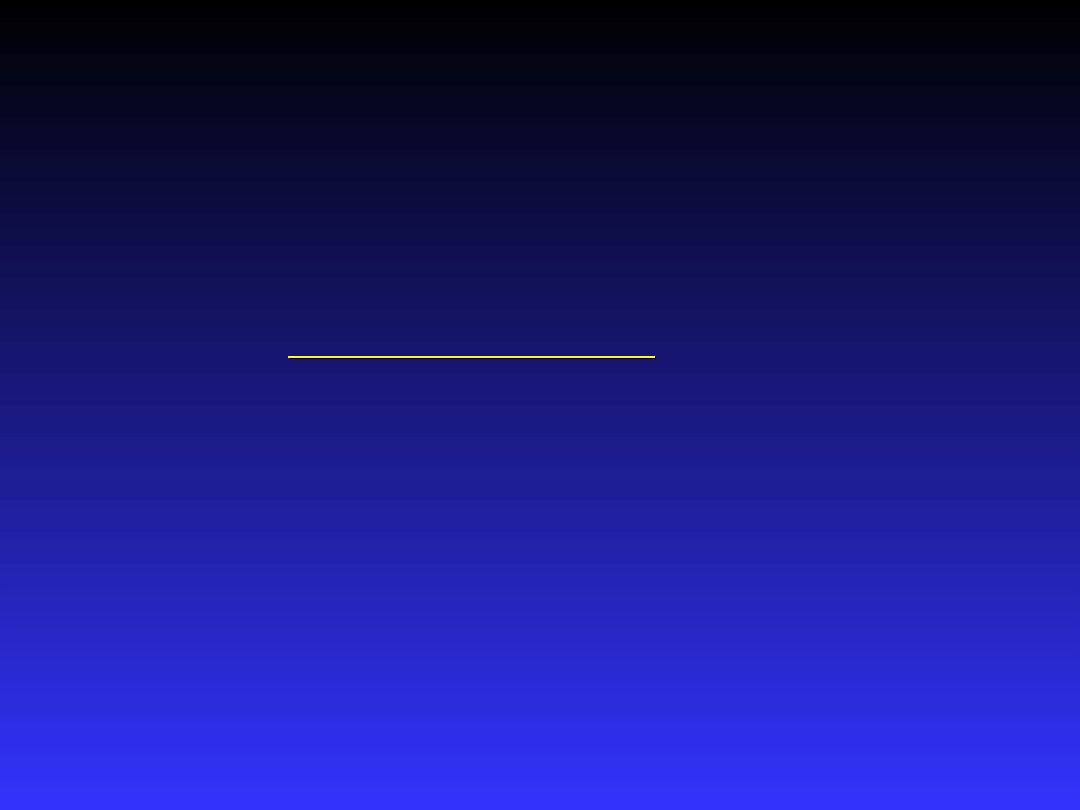
Blood glucose control
assessment levels, DM 2
Low risk
Low risk
Arterial
Arterial
risk
risk
Microva
Microva
scular
scular
risk
risk
HbA
HbA
1c
1c
%Hb
%Hb
<=6.5
<=6.5
>6.5
>6.5
>7.5
>7.5
Venous plasma
Venous plasma
Fasting / pre-
Fasting / pre-
prandial
prandial
mmol/
mmol/
l
l
<=6.0
<=6.0
>6.0
>6.0
>=7.
>=7.
0
0
mg/dl
mg/dl
<110
<110
>=11
>=11
0
0
>125
>125
Self-monitored
Self-monitored
Fasting / pre-
Fasting / pre-
prandial
prandial
mmol/
mmol/
l
l
<=5.5
<=5.5
>5.5
>5.5
>6.0
>6.0
mg/dl
mg/dl
<100
<100
>=10
>=10
0
0
>=1
>=1
10
10
Self-monitored
Self-monitored
Post-prandial
Post-prandial
(peak)
(peak)
mmol/
mmol/
l
l
<7.5
<7.5
>=7.
>=7.
5
5
>9.0
>9.0
mg/dl
mg/dl
<135
<135
>=13
>=13
5
5
>160
>160

Using oral glucose-lowering
drugs (1)
Begin
Begin
oral agent therapy when :
oral agent therapy when :
o
o
an adequate trial of life-style intervention /
an adequate trial of life-style intervention /
education has been given
education has been given
o
o
either
either
( usually ) :
( usually ) :
HbA
HbA
1c
1c
>6.5 %, fasting venous plasma
>6.5 %, fasting venous plasma
glucose >6.0 mmol/l ( >=110 mg/dl )
glucose >6.0 mmol/l ( >=110 mg/dl )
o
o
or
or
( occasionally ) if thin and no other
( occasionally ) if thin and no other
arterial risk factor :
arterial risk factor :
HbA
HbA
1c
1c
>7.5 %, fasting venous plasma glucose
>7.5 %, fasting venous plasma glucose
>=7.0 mmol/l ( >125 mg/dl )
>=7.0 mmol/l ( >125 mg/dl )

Using oral glucose-lowering
drugs (2)
Use
Use
:
:
o
o
metformin
metformin
o
o
insulin secretagogues
insulin secretagogues
(sulphonylureas and repaglinide)
(sulphonylureas and repaglinide)
o
o
alpha-glucosidase inhibitors
alpha-glucosidase inhibitors
o
o
thiazolidinediones and related
thiazolidinediones and related
PPARgamma-agonists
PPARgamma-agonists

Metformin
strong evidence base in the overweight,
strong evidence base in the overweight,
lowers LDL cholesterol, but gastro-
lowers LDL cholesterol, but gastro-
intestinal side effects in some patients;
intestinal side effects in some patients;
dose titration may help tolerance
dose titration may help tolerance
contraindicated ( risk of lactic acidosis )
contraindicated ( risk of lactic acidosis )
if renal impairment, overt liver
if renal impairment, overt liver
disease,
disease,
or severe cardiac failure; monitor
or severe cardiac failure; monitor
renal function at least yearly
renal function at least yearly

Sulphonylureas
good evidence base, provided patient has
good evidence base, provided patient has
useful islet B-cell function
useful islet B-cell function
hypoglycaemia a significant problem
hypoglycaemia a significant problem
:
:
glibenclamide > glipizide =
glibenclamide > glipizide =
chlorpropamide > gliclazide > tolbutamide
chlorpropamide > gliclazide > tolbutamide
(some other agents lack data);
(some other agents lack data);
avoid glibenclamide / chlorpropamide
avoid glibenclamide / chlorpropamide
particularly if renal impairment or in the
particularly if renal impairment or in the
thin insulin-sensitive patient ( especially if
thin insulin-sensitive patient ( especially if
elderly )
elderly )

Repaglinide
new rapid-acting insulin
new rapid-acting insulin
secretagogue; possible advantage
secretagogue; possible advantage
in hypoglycaemia avoidance and
in hypoglycaemia avoidance and
control of post-prandial glucose
control of post-prandial glucose
excursions
excursions

Alpha-glucosidase
inhibitors
effective control of post-prandial
effective control of post-prandial
hyperglycaemia, but poorly
hyperglycaemia, but poorly
tolerated by many patients; dose
tolerated by many patients; dose
titration may help tolerance
titration may help tolerance

PPARgamma-agonists
new agents, offering effective glucose-
new agents, offering effective glucose-
lowering particularly in combination
lowering particularly in combination
with insulin and insulin secretagogues
with insulin and insulin secretagogues
contraindicated
contraindicated
if any history of liver
if any history of liver
disease, and require organized
disease, and require organized
monitoring of
monitoring of
liver function tests until hepatic
liver function tests until hepatic
safety assured
safety assured

Maintaining good blood glucose
control with oral glucose-lowering
drugs
Expect :
Expect :
continuous deterioration of
continuous deterioration of
glucose control with time
glucose control with time
a need to increase therapy and
a need to increase therapy and
add new agents with time
add new agents with time
insulin therapy to be needed in
insulin therapy to be needed in
many patients after a variable
many patients after a variable
number of years
number of years

Insulin therapy in Type 2
diabetes (1)
Begin
Begin
when HbA1c has deteriorated to >7.5 %
when HbA1c has deteriorated to >7.5 %
after maximum attention to dietary control
after maximum attention to dietary control
and oral glucose-lowering therapy ( unless
and oral glucose-lowering therapy ( unless
poor life-expectancy and asymptomatic )
poor life-expectancy and asymptomatic )
o
o
Arrange dietary review when starting
Arrange dietary review when starting
insulin therapy
insulin therapy
o
o
Review ( or start ) self-monitoring of
Review ( or start ) self-monitoring of
blood glucose before starting insulin
blood glucose before starting insulin
Continue therapy with metformin / insulin
Continue therapy with metformin / insulin
secretagogues / PPARgamma-agonists
secretagogues / PPARgamma-agonists

Insulin therapy in Type 2
diabetes (2)
Use
Use
:
:
o
o
NPH insulin at night with oral glucose-
NPH insulin at night with oral glucose-
lowering drugs in people with good
lowering drugs in people with good
insulin secretory reserve
insulin secretory reserve
o
o
pre-mixed insulin twice daily in the
pre-mixed insulin twice daily in the
majority of people
majority of people
twice daily NPH insulin in people with high
twice daily NPH insulin in people with high
pre-breakfast blood glucose
pre-breakfast blood glucose
concentrations relative
concentrations relative
to their HbA
to their HbA
1c
1c
Adjust therapy
o
o
frequently at first, using self-monitored results,
frequently at first, using self-monitored results,
until insulin dose is adequate to
until insulin dose is adequate to
reach
reach
blood glucose targets,
blood glucose targets,
or hypoglycaemia
or hypoglycaemia
becomes a risk
becomes a risk
o
o
Consider more intensive insulin regimens
Consider more intensive insulin regimens
in the more active patient if control remains
in the more active patient if control remains
sub-optimal
sub-optimal
if control remains sub-optimal due to
if control remains sub-optimal due to
hypoglycaemia ( but not if due to insulin
hypoglycaemia ( but not if due to insulin
insensitivity )
insensitivity )
to assist achievement of more flexible life-styles
to assist achievement of more flexible life-styles

Diabetes control (1)
Good diabetes control means:
Good diabetes control means:
Good control of glycemia
Good control of glycemia
Good control of hypertension (if exists)
Good control of hypertension (if exists)
Good control of other concomitant
Good control of other concomitant
metabolic disorders (lipid profile,
metabolic disorders (lipid profile,
hyperuricemia)
hyperuricemia)

Diabetes control (2)
Good control of glycemia means:
Good control of glycemia means:
Maintenance of normoglycemia or near-
Maintenance of normoglycemia or near-
normoglycemia
normoglycemia
Low incidence of episodes of
Low incidence of episodes of
hyperglycemia
hyperglycemia
Low incidence of episodes of
Low incidence of episodes of
hypoglycemia
hypoglycemia

Diabetes control (3)
The more intensive pharmacological
The more intensive pharmacological
treatment, the lower values of
treatment, the lower values of
HbA
HbA
1c
1c
, and the more pronounced
, and the more pronounced
risk of hypoglycemia
risk of hypoglycemia

Diabetes control (4)
The more intensive pharmacological
The more intensive pharmacological
treatment, the more important
treatment, the more important
self-control
self-control

Using blood lipid lowering
drugs
o
o
a statin
a statin
if
if
: LDL cholesterol >=3.0 mmol/l ( >=115 mg/dl )
: LDL cholesterol >=3.0 mmol/l ( >=115 mg/dl )
( >4.0 mmol/l ( >155 mg/dl ) if low risk including thin elderly )
( >4.0 mmol/l ( >155 mg/dl ) if low risk including thin elderly )
o
o
a fibrate
a fibrate
if
if
: triglyceride >2.2 mmol/l ( >200 mg/dl )
: triglyceride >2.2 mmol/l ( >200 mg/dl )
and
and
LDL cholesterol <3.0 mmol/l ( <115 mg/dl )
LDL cholesterol <3.0 mmol/l ( <115 mg/dl )
o
o
a fibrate first
a fibrate first
if triglyceride markedly elevated ( >6.8
if triglyceride markedly elevated ( >6.8
mmol/l (>600 mg/dl ) );
mmol/l (>600 mg/dl ) );
check thyroid, renal, and liver function ( and apoE genotype if
check thyroid, renal, and liver function ( and apoE genotype if
available );
available );
consider combination therapy with a statin if LDL cholesterol
consider combination therapy with a statin if LDL cholesterol
remains elevated
remains elevated
combination therapy
combination therapy
beginning with statin for high LDL
beginning with statin for high LDL
cholesterol and triglyceride
cholesterol and triglyceride

Using anti-hypertensive
drugs (1)
Monitor
Monitor
:
:
o
o
dietary quality and quantity
dietary quality and quantity
( including alcohol ), physical
( including alcohol ), physical
exercise level, body weight
exercise level, body weight
sitting blood pressure ( after 5 min
sitting blood pressure ( after 5 min
rest, 1st and 5th phase )
rest, 1st and 5th phase )
Using anti-hypertensive
drugs (2)
Use
Use
:
:
o
o
single agent therapy at rising
single agent therapy at rising
doses until target achieved ( or
doses until target achieved ( or
intolerance )
intolerance )
o
o
multiple therapy if targets not
multiple therapy if targets not
reached on maximum doses of single
reached on maximum doses of single
agents
agents
once daily drug administration regimens
once daily drug administration regimens

ACE-inhibitors
good evidence base in diabetes,
good evidence base in diabetes,
advancing renal disease, cardiac
advancing renal disease, cardiac
failure
failure
monitor renal function / K+ ( risk of
monitor renal function / K+ ( risk of
renal artery stenosis with arterial
renal artery stenosis with arterial
disease )
disease )

Beta-adrenergic
blockers
good evidence base in diabetes and
good evidence base in diabetes and
useful where angina or previous
useful where angina or previous
myocardial infarction
myocardial infarction
avoid combination with thiazides
avoid combination with thiazides
( metabolic deterioration ), and if
( metabolic deterioration ), and if
peripheral
peripheral
vascular disease. Ask about
vascular disease. Ask about
tiredness and impotence
tiredness and impotence

Calcium channel
antagonists
some evidence base in diabetes and
some evidence base in diabetes and
in advancing renal disease
in advancing renal disease
use only long-acting
use only long-acting
preparations
preparations
fluid retention a problem with some
fluid retention a problem with some
agents (avoid if history of foot
agents (avoid if history of foot
ulceration)
ulceration)
Thiazides
some evidence base in diabetes
some evidence base in diabetes
use low doses only and avoid
use low doses only and avoid
combination with beta-adrenergic
combination with beta-adrenergic
blockers ( metabolic
blockers ( metabolic
deterioration ). Ask about
deterioration ). Ask about
impotence
impotence

Loop diuretics
useful synergistic action with ACE-
useful synergistic action with ACE-
inhibitors
inhibitors

Alpha-adrenergic
blockers
effective blood pressure lowering
effective blood pressure lowering
and metabolically beneficial
and metabolically beneficial
use only long-acting drugs
use only long-acting drugs
( postural hypotension )
( postural hypotension )

Angiotensin II receptor
blockers
no special advantages
no special advantages

Choice of agents -
summary
Multiple therapy is often required; add loop
Multiple therapy is often required; add loop
diuretic to ACE-inhibitor, and avoid thiazides with
diuretic to ACE-inhibitor, and avoid thiazides with
beta-adrenergic blocker; otherwise most
beta-adrenergic blocker; otherwise most
combinations neutral
combinations neutral
Many older and less expensive agents are as
Many older and less expensive agents are as
effective as newer agents
effective as newer agents
If abnormal albumin excretion, particularly if
If abnormal albumin excretion, particularly if
progressive, begin with ACE-inhibitor, or calcium
progressive, begin with ACE-inhibitor, or calcium
channel
channel
antagonist if ACE-inhibitor not tolerated
antagonist if ACE-inhibitor not tolerated
If ischaemic heart disease, consider beta-
If ischaemic heart disease, consider beta-
adrenergic blocker first </UL< DL>
adrenergic blocker first </UL< DL>

Planning the treatment (1)
Each patient needs individual plan of
Each patient needs individual plan of
non-pharmacological and
non-pharmacological and
pharmacological treatment, the should
pharmacological treatment, the should
be modified according to current
be modified according to current
situation
situation

Planning the treatment (2)
Specific targets of treatment, given in
Specific targets of treatment, given in
standards, but also some patient’s
standards, but also some patient’s
conditions should be taken into account:
conditions should be taken into account:
Patient’s level of education
Patient’s level of education
Compliance in aspects of self-control, and the
Compliance in aspects of self-control, and the
treatment :
treatment :
Acceptation for the particular targets and kind of the
Acceptation for the particular targets and kind of the
treatment
treatment
Mental, physical, and financial ability to realize the
Mental, physical, and financial ability to realize the
necessary control, and treatment or a sufficient support
necessary control, and treatment or a sufficient support
from his/her family other persons or medical / social
from his/her family other persons or medical / social
institutions
institutions

Planning the treatment (3)
In young patients the maintenance of
In young patients the maintenance of
near-normoglycemia is the most
near-normoglycemia is the most
important target of treatment
important target of treatment
In elderly – avoidance of hypoglycemic
In elderly – avoidance of hypoglycemic
episodes is more important
episodes is more important

Hypoglycemia
Symptoms of developing hypoglycemia can
Symptoms of developing hypoglycemia can
be atypical (inadequate) or difficult to
be atypical (inadequate) or difficult to
notice especially:
notice especially:
In elderly
In elderly
When
When
-adrenergic blockers
-adrenergic blockers
are used
are used
During and after prolonged intensive physical
During and after prolonged intensive physical
exercise
exercise
During mental stress
During mental stress
In acute ilness
In acute ilness
During the sleep
During the sleep

Acute decompensation of diabetes
(1)
Terms of ‘hyperglycemic hyperosmolar
Terms of ‘hyperglycemic hyperosmolar
nonketotic coma’ and ‘hyperglycemic
nonketotic coma’ and ‘hyperglycemic
hyperosmolar nonketotic state’ shoul be
hyperosmolar nonketotic state’ shoul be
replased with the term ‘hyperglycemic
replased with the term ‘hyperglycemic
hyperosmolar state’ (HHS)
hyperosmolar state’ (HHS)
The term ‘ketotic coma’ shoul be replased
The term ‘ketotic coma’ shoul be replased
with the term ‘diabetic ketoacidosis’ (DKA)
with the term ‘diabetic ketoacidosis’ (DKA)
Both are reffered as ‘hyperglycemic crises’
Both are reffered as ‘hyperglycemic crises’

Acute decompensation of diabetes
(2)
Clinical manifestations of ‘
hyperglycemic
hyperglycemic
crises’:
crises’:
Circulatory (dehydration,hypovolemia,
Circulatory (dehydration,hypovolemia,
hyperosmolarity,shock)
hyperosmolarity,shock)
Impared renal function
Impared renal function
Abdominal
Abdominal
(Pseudoperitonotis)
(Pseudoperitonotis)
Acute decompensation of diabetes
(3)
Management:
Management:
Fluids i.v
Fluids i.v
. (start with 1,0 l of 0,9% NaCl, 15-20
. (start with 1,0 l of 0,9% NaCl, 15-20
ml/kg/h, determine hydration status, evaluate
ml/kg/h, determine hydration status, evaluate
corrected serum Na
corrected serum Na
+
+
, continue 0,9% NaCl 4-14
, continue 0,9% NaCl 4-14
ml/kg/h if serum Na
ml/kg/h if serum Na
+
+
is normal or low; 0,45% NaCl
is normal or low; 0,45% NaCl
if serum Na
if serum Na
+
+
is high); change to 5% dextrose with
is high); change to 5% dextrose with
0,45% NaCl with adequate insulin (0,05-0,1 U/kg/h
0,45% NaCl with adequate insulin (0,05-0,1 U/kg/h
i.v.or 5-10 U. every 2h to keep the serum glucose
i.v.or 5-10 U. every 2h to keep the serum glucose
between 150-200 mg/dl until metabolic control is
between 150-200 mg/dl until metabolic control is
reached)
reached)
Insulin
Insulin
(Start with Regular 0,15 U/kg as i.v. bolus,
(Start with Regular 0,15 U/kg as i.v. bolus,
then 0,1 u/kg/h i.v.insulin infusion utill glycemia
then 0,1 u/kg/h i.v.insulin infusion utill glycemia
reaches 250 mg/dl)
reaches 250 mg/dl)

Acute decompensation of diabetes
(4)
Potassium: check serum K
Potassium: check serum K
+
+
every 2h
every 2h
If serum K
If serum K
+
+
is
is
5,5 mmol/l (mEq/l) do not
5,5 mmol/l (mEq/l) do not
give K
give K
+
+
When serum K
When serum K
+
+
falls below 5,5 mmol/l give
falls below 5,5 mmol/l give
20-30 mEq K
20-30 mEq K
+
+
(2/3 KCl and 1/3 KPO
(2/3 KCl and 1/3 KPO
4
4
) per
) per
each liter of fluid
each liter of fluid
If K
If K
+
+
< 3,3 mmol/l give 40 mEq K
< 3,3 mmol/l give 40 mEq K
+
+
(2/3 KCl
(2/3 KCl
and 1/3 KPO
and 1/3 KPO
4
4
) per 1h
) per 1h
Keep serum K
Keep serum K
+
+
at 4-5 mmol/l
at 4-5 mmol/l
Bicarbonate
Bicarbonate
if pH
if pH
7,0
7,0
Document Outline
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Slide 45
- Slide 46
- Slide 47
- Slide 48
- Slide 49
- Slide 50
- Slide 51
- Slide 52
Wyszukiwarka
Podobne podstrony:
DM ang Dgn black
DM ang Dgn
DM NewThreats ang id 137396 Nieznany
Hydrocephalus(ang)
DP i DM
DM
Wstrzasy ang ppt
Glikoliza prezentacja (ang)
08 BIOCHEMIA mechanizmy adaptac mikroor ANG 2id 7389 ppt
3Kocioł ang
ns EiT 1 2st ang 2008
2010 ang
osteoarthritis ang ppt
j ang ark pdst
Kody TV do pilota DM 800HD
Matlab Programming (ang)
2010 próbny ang transkrypcja
więcej podobnych podstron