
WHO definition and
diagnostic criteria for
diabetes mellitus
Jan Szewieczek
Jan Szewieczek
Katedra i Klinika
Katedra i Klinika
Chorób Wewnętrznych i Metabolicznych
Chorób Wewnętrznych i Metabolicznych
Śl.A.M. Katowice
Śl.A.M. Katowice

Definition (1)
The term diabetes mellitus describes a
The term diabetes mellitus describes a
metabolic disorder of multiple aetiology
metabolic disorder of multiple aetiology
characterized by chronic
characterized by chronic
hyperglycaemia with disturbances of
hyperglycaemia with disturbances of
carbohydrate, fat and protein
carbohydrate, fat and protein
metabolism resulting from defects in
metabolism resulting from defects in
insulin secretion, insulin action, or
insulin secretion, insulin action, or
both.
both.

Definition (2)
The effects of diabetes mellitus include
The effects of diabetes mellitus include
long-term damage, dysfunction and failure
long-term damage, dysfunction and failure
of various organs. Diabetes mellitus may
of various organs. Diabetes mellitus may
present with characteristic symptoms such
present with characteristic symptoms such
as thirst, polyuria, blurring of vision, and
as thirst, polyuria, blurring of vision, and
weight loss. In its most severe forms,
weight loss. In its most severe forms,
ketoacidosis or a non-ketotic
ketoacidosis or a non-ketotic
hyperosmolar state may develop and lead
hyperosmolar state may develop and lead
to stupor, coma and, in absence of
to stupor, coma and, in absence of
effective treatment, death.
effective treatment, death.

Definition (3)
Often symptoms are not severe, or may be absent,
Often symptoms are not severe, or may be absent,
and consequently hyperglycaemia sufficient to
and consequently hyperglycaemia sufficient to
cause pathological and functional changes may be
cause pathological and functional changes may be
present for a long time before the diagnosis is
present for a long time before the diagnosis is
made. The long-term effects of diabetes mellitus
made. The long-term effects of diabetes mellitus
include progressive development of the specific
include progressive development of the specific
complications of retinopathy with potential
complications of retinopathy with potential
blindness, nephropathy that may lead to renal
blindness, nephropathy that may lead to renal
failure, and/or neuropathy with risk of foot ulcers,
failure, and/or neuropathy with risk of foot ulcers,
amputation, Charcot joints, and features of
amputation, Charcot joints, and features of
autonomic dysfunction, including sexual
autonomic dysfunction, including sexual
dysfunction.
dysfunction.

Definition (4)
People with diabetes are at
People with diabetes are at
increased risk of cardiovascular,
increased risk of cardiovascular,
peripheral vascular and
peripheral vascular and
cerebrovascular disease.
cerebrovascular disease.
Diagnosis (1)
If a diagnosis of diabetes is made,
If a diagnosis of diabetes is made,
the clinician must feel confident
the clinician must feel confident
that the diagnosis is fully
that the diagnosis is fully
established since the
established since the
consequences for the individual
consequences for the individual
are considerable and lifelong.
are considerable and lifelong.

Diagnosis (2)
The requirements for diagnostic confirmation
The requirements for diagnostic confirmation
for a person presenting with severe symptoms
for a person presenting with severe symptoms
and gross hyperglycaemia differ from those
and gross hyperglycaemia differ from those
for the asymptomatic person with blood
for the asymptomatic person with blood
glucose values found to be just above the
glucose values found to be just above the
diagnostic cut-off value. Severe
diagnostic cut-off value. Severe
hyperglycaemia detected under conditions of
hyperglycaemia detected under conditions of
acute infective, traumatic, circulatory or other
acute infective, traumatic, circulatory or other
stress may be transitory and should not in
stress may be transitory and should not in
itself be regarded as diagnostic of diabetes.
itself be regarded as diagnostic of diabetes.

Diagnosis (3)
For the asymptomatic person, at least one
For the asymptomatic person, at least one
additional plasma/blood glucose test result
additional plasma/blood glucose test result
with a value in the diabetic range is
with a value in the diabetic range is
essential, either fasting, from a random
essential, either fasting, from a random
(casual) sample, or from the oral glucose
(casual) sample, or from the oral glucose
tolerance test (OGTT). If such samples fail to
tolerance test (OGTT). If such samples fail to
confirm the diagnosis of diabetes mellitus, it
confirm the diagnosis of diabetes mellitus, it
will usually be advisable to maintain
will usually be advisable to maintain
surveillance with periodic re-testing until the
surveillance with periodic re-testing until the
diagnostic situation becomes clear.
diagnostic situation becomes clear.

Diagnostic algorithm
(1)
1. Symptomatic
1. Symptomatic
or
or
glycosuria
glycosuria
or
or
incidental hyperglycaemia
incidental hyperglycaemia
Check
Check
random venous plasma
random venous plasma
glucose
glucose
If
If
>11.0 mmol/l ( >=200 mg/dl ) =
>11.0 mmol/l ( >=200 mg/dl ) =
"Diabetes"
"Diabetes"
If
If
>5.5 mmol/l ( >=100 mg/dl )
>5.5 mmol/l ( >=100 mg/dl )
then
then
proceed to next step (2.)
proceed to next step (2.)
Diagnostic algorithm
(2)
2. Random
2. Random
or
or
fasting screening glucose
fasting screening glucose
>5.5 mmol/l ( >=100 mg/dl )
>5.5 mmol/l ( >=100 mg/dl )
Check
Check
fasting venous plasma glucose
fasting venous plasma glucose
If
If
>=7.0 mmol/l ( >125 mg/dl ), repeat and
>=7.0 mmol/l ( >125 mg/dl ), repeat and
if confirmed = "Diabetes"
if confirmed = "Diabetes"
If
If
>6.0 mmol/l ( >=110 mg/dl ) do oral
>6.0 mmol/l ( >=110 mg/dl ) do oral
glucose tolerance test ( OGTT )
glucose tolerance test ( OGTT )
If
If
>5.0 mmol/l ( >90 mg/dl ), consider
>5.0 mmol/l ( >90 mg/dl ), consider
yearly reassessment of arterial risk factors
yearly reassessment of arterial risk factors

Diagnostic algorithm
(3)
OGTT ( venous plasma glucose ) :
OGTT ( venous plasma glucose ) :
If
If
2-h >11.0 mmol/l ( >=200 mg/dl ) =
2-h >11.0 mmol/l ( >=200 mg/dl ) =
"Diabetes"
"Diabetes"
If
If
2-h <=11.0 mmol/l ( <200 mg/dl ) and
2-h <=11.0 mmol/l ( <200 mg/dl ) and
>=7.8 mmol/l ( >=140 mg/dl ) = "IGT"
>=7.8 mmol/l ( >=140 mg/dl ) = "IGT"
If
If
fasting >6.0 mmol/l ( >=110 mg/dl )
fasting >6.0 mmol/l ( >=110 mg/dl )
and 2-h <7.8 mmol/l ( <140 mg/dl ) =
and 2-h <7.8 mmol/l ( <140 mg/dl ) =
"IFG"
"IFG"

Diagnosis (4)
4. Diagnostic procedures should not
4. Diagnostic procedures should not
be performed :
be performed :
o
o
in the presence of
in the presence of
acute
acute
illness or after trauma or
illness or after trauma or
surgery
surgery
during short courses of
during short courses of
blood
blood
glucose raising drugs
glucose raising drugs

Diagnosis (5)
5. Diagnostic tests should be
5. Diagnostic tests should be
interpreted with reservation :
interpreted with reservation :
o
o
in people on long-term
in people on long-term
blood
blood
glucose raising drugs
glucose raising drugs
o
o
in people with reversible
in people with reversible
endocrine conditions
endocrine conditions
in
in
pregnant women
pregnant women
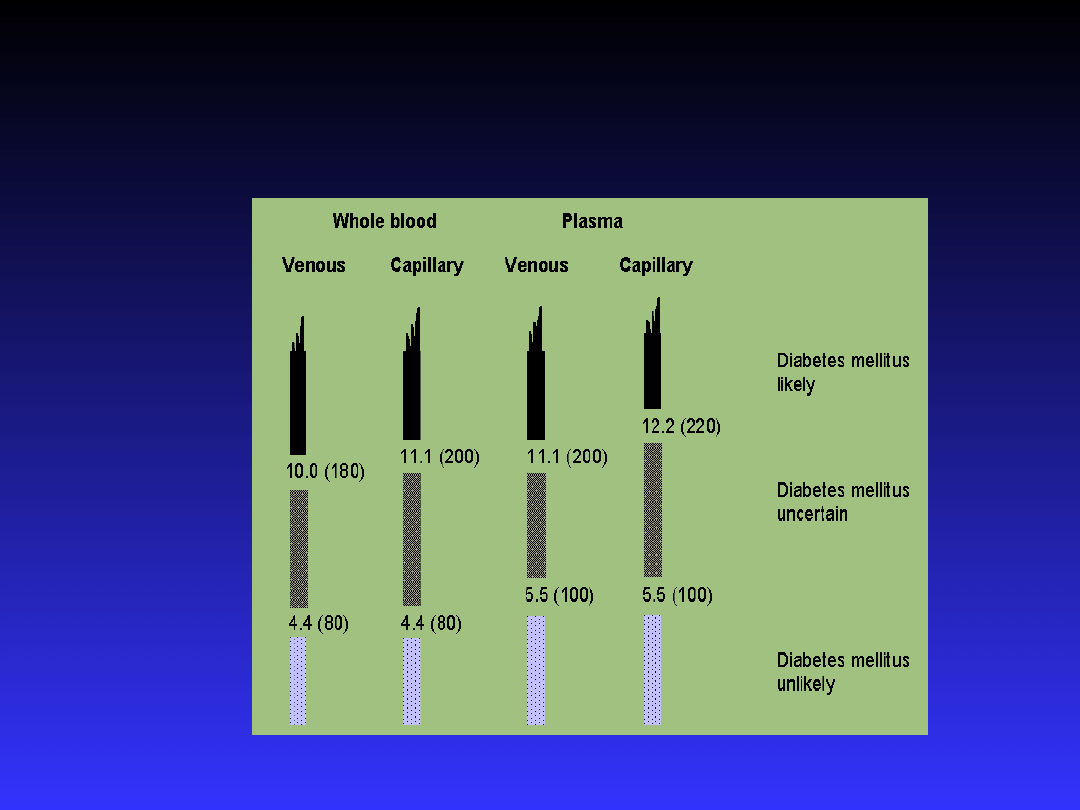
Laboratory equivalents

Terminology (1)
It is recommended that the terms
It is recommended that the terms
"insulin-dependent diabetes mellitus"
"insulin-dependent diabetes mellitus"
and "non-insulin-dependent diabetes
and "non-insulin-dependent diabetes
mellitus" and their acronyms "IDDM"
mellitus" and their acronyms "IDDM"
and "NIDDM" no longer be used.
and "NIDDM" no longer be used.
These terms have been confusing and
These terms have been confusing and
frequently resulted in patients being
frequently resulted in patients being
classified based on treatment rather
classified based on treatment rather
than on pathogenesis.
than on pathogenesis.

Terminology (2)
The terms Type 1 and Type 2
The terms Type 1 and Type 2
should be reintroduced. The
should be reintroduced. The
aetiological type named Type 1
aetiological type named Type 1
encompasses the majority of cases
encompasses the majority of cases
which are primarily due to
which are primarily due to
pancreatic
islet
beta-cell
pancreatic
islet
beta-cell
destruction and are prone to
destruction and are prone to
ketoacidosis.
ketoacidosis.

Terminology (3)
Type 1 includes those cases attributable to
Type 1 includes those cases attributable to
an autoimmune process, as well as those
an autoimmune process, as well as those
with beta-cell destruction and who are prone
with beta-cell destruction and who are prone
to ketoacidosis for which neither an aetiology
to ketoacidosis for which neither an aetiology
nor a pathogenesis is known (idiopathic). It
nor a pathogenesis is known (idiopathic). It
does not include those forms of beta-cell
does not include those forms of beta-cell
destruction or failure to which specific
destruction or failure to which specific
causes can be assigned (e.g. cystic fibrosis,
causes can be assigned (e.g. cystic fibrosis,
mitochondrial defects, etc.). Some subjects
mitochondrial defects, etc.). Some subjects
with this type can be identified at earlier
with this type can be identified at earlier
clinical stages than "diabetes mellitus".
clinical stages than "diabetes mellitus".

Terminology (4)
The type named Type 2 includes
The type named Type 2 includes
the common major form of
the common major form of
diabetes which results from
diabetes which results from
defect(s) in insulin secretion,
defect(s) in insulin secretion,
almost always with a major
almost always with a major
contribution from insulin
contribution from insulin
resistance.
resistance.
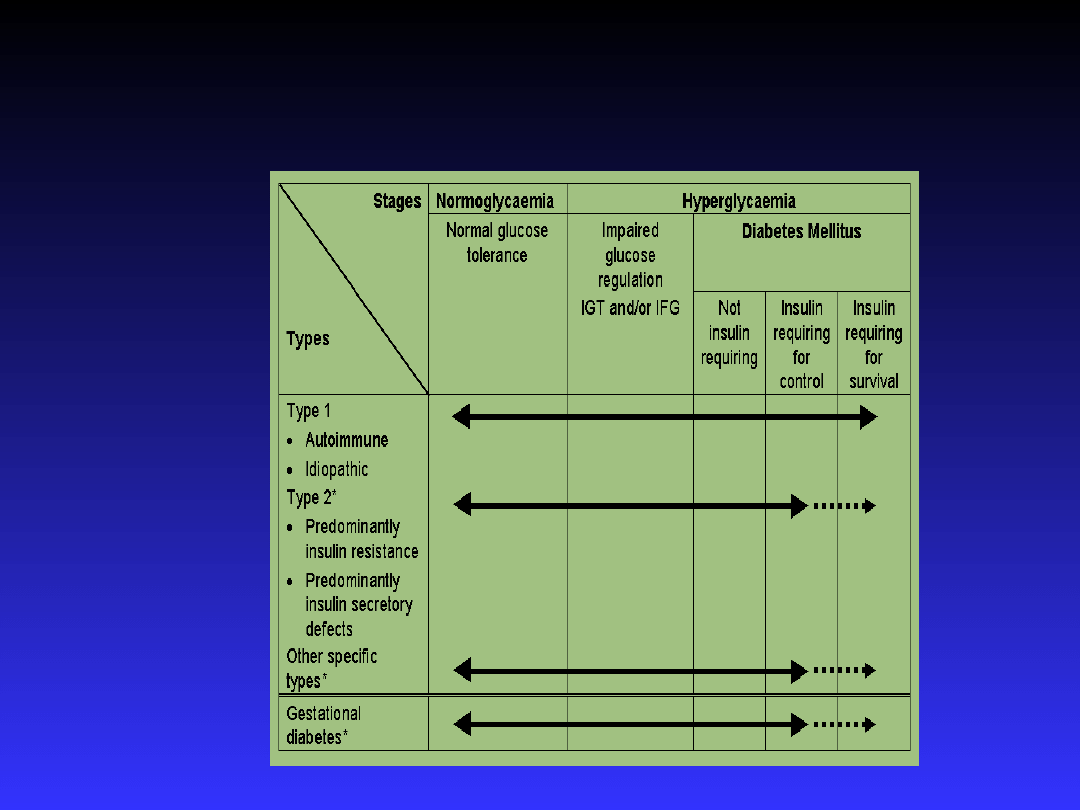
Aethiological types and stages

IGT and IFG
Impaired glucose regulation (IGT and
Impaired glucose regulation (IGT and
IFG) refers to a metabolic state
IFG) refers to a metabolic state
intermediate between normal glucose
intermediate between normal glucose
homeostasis and diabetes. It should be
homeostasis and diabetes. It should be
stated unequivocally, however, that
stated unequivocally, however, that
IFG and IGT are not interchangeable
IFG and IGT are not interchangeable
and represent different abnormalities
and represent different abnormalities
of glucose regulation, one in the
of glucose regulation, one in the
fasting state and one post-prandial.
fasting state and one post-prandial.

Diabetes type 1 (1)
Type 1 indicates the processes of beta-cell
Type 1 indicates the processes of beta-cell
destruction that may ultimately lead to
destruction that may ultimately lead to
diabetes mellitus in which "insulin is
diabetes mellitus in which "insulin is
required for survival" to prevent the
required for survival" to prevent the
development of ketoacidosis, coma and
development of ketoacidosis, coma and
death. An individual with a Type 1 process
death. An individual with a Type 1 process
may be metabolically normal before the
may be metabolically normal before the
disease is clinically manifest, but the
disease is clinically manifest, but the
process of beta-cell destruction can be
process of beta-cell destruction can be
detected.
detected.

Diabetes type 1 (2)
Type 1 is usually characterized by the
Type 1 is usually characterized by the
presence of anti-GAD, islet cell or
presence of anti-GAD, islet cell or
insulin antibodies which identify the
insulin antibodies which identify the
autoimmune processes that lead to
autoimmune processes that lead to
beta-cell destruction. In some subjects
beta-cell destruction. In some subjects
no evidence of an autoimmune disorder
no evidence of an autoimmune disorder
is demonstrable and these are classified
is demonstrable and these are classified
as "Type 1 idiopathic".
as "Type 1 idiopathic".

Diabetes type 1 (3)
The slowly progressive form
The slowly progressive form
generally occurs in adults and is
generally occurs in adults and is
sometimes referred to as latent
sometimes referred to as latent
autoimmune diabetes in adults
autoimmune diabetes in adults
(LADA).
(LADA).

Diabetes type 1 (4)
Individuals with this form of Type 1
Individuals with this form of Type 1
diabetes often become dependent
diabetes often become dependent
on insulin for survival eventually
on insulin for survival eventually
and are at risk for ketoacidosis. At
and are at risk for ketoacidosis. At
this stage of the disease, there is
this stage of the disease, there is
little or no insulin secretion as
little or no insulin secretion as
manifested by low or undetectable
manifested by low or undetectable
levels of plasma C-peptide
levels of plasma C-peptide

Diabetes type 1 (5)
Markers of immune destruction,
Markers of immune destruction,
including islet cell autoantibodies,
including islet cell autoantibodies,
and/or autoantibodies to insulin, and
and/or autoantibodies to insulin, and
autoantibodies to glutamic acid
autoantibodies to glutamic acid
decarboxylase (GAD) are present in
decarboxylase (GAD) are present in
85-90 % of individuals with Type 1
85-90 % of individuals with Type 1
diabetes mellitus when fasting
diabetes mellitus when fasting
diabetic hyperglycaemia is initially
diabetic hyperglycaemia is initially
detected.
detected.

Diabetes type 1 (6)
There
is
a
genetic
predisposition
to
There
is
a
genetic
predisposition
to
autoimmune destruction of beta cells, and it is
autoimmune destruction of beta cells, and it is
also related to environmental factors that are
also related to environmental factors that are
still poorly defined. Although patients are
still poorly defined. Although patients are
usually not obese when they present with this
usually not obese when they present with this
type of diabetes, the presence of obesity is not
type of diabetes, the presence of obesity is not
incompatible with the diagnosis. These
incompatible with the diagnosis. These
patients may also have other autoimmune
patients may also have other autoimmune
disorders such as Graves' disease, Hashimoto's
disorders such as Graves' disease, Hashimoto's
thyroiditis, and Addison's disease.
thyroiditis, and Addison's disease.

Diabetes type 2 (1)
Type 2 is the most common form of
Type 2 is the most common form of
diabetes and is characterized by
diabetes and is characterized by
disorders of insulin action and insulin
disorders of insulin action and insulin
secretion, either of which may be the
secretion, either of which may be the
predominant feature. Both are usually
predominant feature. Both are usually
present at the time that this form of
present at the time that this form of
diabetes is clinically manifest. By
diabetes is clinically manifest. By
definition, the specific reasons for the
definition, the specific reasons for the
development of these abnormalities
development of these abnormalities
are not yet known.
are not yet known.

Diabetes type 2 (2)
Diabetes mellitus of this type previously
Diabetes mellitus of this type previously
encompassed non-insulin-dependent
encompassed non-insulin-dependent
diabetes, or adult-onset diabetes. It is a
diabetes, or adult-onset diabetes. It is a
term used for individuals who have relative
term used for individuals who have relative
(rather than absolute) insulin deficiency.
(rather than absolute) insulin deficiency.
People with this type of diabetes frequently
People with this type of diabetes frequently
are resistant to the action of insulin. At
are resistant to the action of insulin. At
least initially, and often throughout their
least initially, and often throughout their
lifetime, these individuals do not need
lifetime, these individuals do not need
insulin treatment to survive.
insulin treatment to survive.

Diabetes type 2 (3)
This form of diabetes is frequently
This form of diabetes is frequently
undiagnosed for many years because
undiagnosed for many years because
the hyperglycaemia is often not
the hyperglycaemia is often not
severe enough to provoke noticeable
severe enough to provoke noticeable
symptoms of diabetes. Nevertheless,
symptoms of diabetes. Nevertheless,
such patients are at increased risk of
such patients are at increased risk of
developing macrovascular and
developing macrovascular and
microvascular complications
microvascular complications

Diabetes type 2 (4)
The majority of patients with this form of
The majority of patients with this form of
diabetes are obese, and obesity itself causes
diabetes are obese, and obesity itself causes
or aggravates insulin resistance. Many of
or aggravates insulin resistance. Many of
those who are not obese by traditional weight
those who are not obese by traditional weight
criteria may have an increased percentage of
criteria may have an increased percentage of
body fat distributed predominantly in the
body fat distributed predominantly in the
abdominal region. Ketoacidosis is infrequent
abdominal region. Ketoacidosis is infrequent
in this type of diabetes; when seen it usually
in this type of diabetes; when seen it usually
arises in association with the stress of
arises in association with the stress of
another illness such as infection
another illness such as infection

Diabetes type 2 (5)
The risk of developing Type 2
The risk of developing Type 2
diabetes increases with age,
diabetes increases with age,
obesity, and lack of physical
obesity, and lack of physical
activity. It occurs more frequently
activity. It occurs more frequently
in women with prior GDM and in
in women with prior GDM and in
individuals with hypertension or
individuals with hypertension or
dyslipidaemia.
dyslipidaemia.

Diabetes type 3 (1)
Other Specific Types are currently less
Other Specific Types are currently less
common causes of diabetes mellitus,
common causes of diabetes mellitus,
but are those in which the underlying
but are those in which the underlying
defect or disease process can be
defect or disease process can be
identified in a relatively specific
identified in a relatively specific
manner. They include, for example,
manner. They include, for example,
fibrocalculous pancreatopathy, a form
fibrocalculous pancreatopathy, a form
of diabetes which was formerly
of diabetes which was formerly
classified as one type of malnutrition-
classified as one type of malnutrition-
related diabetes mellitus.
related diabetes mellitus.

Diabetes type 3 A (1)
Several forms of the diabetic state may be
Several forms of the diabetic state may be
associated with monogenic defects in
associated with monogenic defects in
-
-
cell function, frequently characterized by
cell function, frequently characterized by
onset of mild hyperglycaemia at an early
onset of mild hyperglycaemia at an early
age (generally before age 25 years). They
age (generally before age 25 years). They
are usually inherited in an autosomal
are usually inherited in an autosomal
dominant pattern. Patients with these
dominant pattern. Patients with these
forms of diabetes, formerly referred to as
forms of diabetes, formerly referred to as
maturity-onset diabetes of the young
maturity-onset diabetes of the young
(MODY), have impaired insulin secretion
(MODY), have impaired insulin secretion
with minimal or no defect in insulin action.
with minimal or no defect in insulin action.

Diabetes type 3 A (2)
Abnormalities at three genetic loci
Abnormalities at three genetic loci
on different chromosomes have
on different chromosomes have
now been characterized. The most
now been characterized. The most
common form is associated with
common form is associated with
mutations on chromosome 12 in a
mutations on chromosome 12 in a
hepatic nuclear transcription
hepatic nuclear transcription
factor referred to as HNF1alpha.
factor referred to as HNF1alpha.

Diabetes type 3 A (3)
A second form is associated with mutations
A second form is associated with mutations
in the glucokinase gene on chromosome
in the glucokinase gene on chromosome
7p. Glucokinase converts glucose to
7p. Glucokinase converts glucose to
glucose-6-phosphate, the metabolism of
glucose-6-phosphate, the metabolism of
which in turn stimulates insulin secretion
which in turn stimulates insulin secretion
by the beta cell. Thus, glucokinase serves
by the beta cell. Thus, glucokinase serves
as the "glucose sensor" for the beta cell.
as the "glucose sensor" for the beta cell.
Because of defects in the glucokinase gene,
Because of defects in the glucokinase gene,
increased levels of glucose are necessary
increased levels of glucose are necessary
to elicit normal levels of insulin secretion.
to elicit normal levels of insulin secretion.

Diabetes type 3 A (4)
A third form is associated with a mutation in
A third form is associated with a mutation in
the HNF4alpha gene on chromosome 20q.
the HNF4alpha gene on chromosome 20q.
HNF4alpha is a transcription factor which is
HNF4alpha is a transcription factor which is
involved in the regulation of the expression
involved in the regulation of the expression
of HNF1alpha. A fourth variant has recently
of HNF1alpha. A fourth variant has recently
been ascribed to mutations in another
been ascribed to mutations in another
transcription factor gene, IPF-1, which in its
transcription factor gene, IPF-1, which in its
homozygous form leads to total pancreatic
homozygous form leads to total pancreatic
agenesis. Specific genetic defects in other
agenesis. Specific genetic defects in other
individuals who have a similar clinical
individuals who have a similar clinical
presentation are currently being defined.
presentation are currently being defined.

Diabetes type 3 A (5)
Point mutations in mitochondrial DNA have
Point mutations in mitochondrial DNA have
been found to be associated with diabetes
been found to be associated with diabetes
mellitus and deafness. The most common
mellitus and deafness. The most common
mutation occurs at position 3243 in the tRNA
mutation occurs at position 3243 in the tRNA
leucine gene, leading to an A to G
leucine gene, leading to an A to G
substitution. An identical lesion occurs in the
substitution. An identical lesion occurs in the
MELAS syndr
MELAS syndr
.
.
(Mitochondrial myopathy,
(Mitochondrial myopathy,
Encephalopathy, Lactic Acidosis, and Stroke-
Encephalopathy, Lactic Acidosis, and Stroke-
like syndrome); however, diabetes is not part
like syndrome); however, diabetes is not part
of this syndr
of this syndr
.,
.,
suggesting for unknown reasons
suggesting for unknown reasons
different phenotypic expressions of this
different phenotypic expressions of this
genetic lesion.
genetic lesion.

Diabetes type 3 A (6)
Genetic abnormalities that result in the inability
Genetic abnormalities that result in the inability
to convert proinsulin to insulin have been
to convert proinsulin to insulin have been
identified in a few families. Such traits are
identified in a few families. Such traits are
usually inherited in an autosomal dominant
usually inherited in an autosomal dominant
pattern and the resultant carbohydrate
pattern and the resultant carbohydrate
intolerance is mild. Similarly, mutant insulin
intolerance is mild. Similarly, mutant insulin
molecules with impaired receptor binding
molecules with impaired receptor binding
have been identified in a few families. These
have been identified in a few families. These
are also associated with autosomal
are also associated with autosomal
inheritance and either normal or only mildly
inheritance and either normal or only mildly
impaired carbohydrate metabolism.
impaired carbohydrate metabolism.

Diabetes type 3 A (7)
Type 3 A.
Type 3 A.
Genetic defects of beta-cell function
Genetic defects of beta-cell function
Chromosome 20, HNF4alpha (MODY1)
Chromosome 20, HNF4alpha (MODY1)
Chromosome 7, glucokinase (MODY2)
Chromosome 7, glucokinase (MODY2)
Chromosome 12, HNF1alpha (MODY3)
Chromosome 12, HNF1alpha (MODY3)
Chromosome 13, IPF-1 (MODY4)
Chromosome 13, IPF-1 (MODY4)
Mitochondrial DNA 3243 mutation
Mitochondrial DNA 3243 mutation
Others
Others

Diabetes type 3 B (1)
There are some unusual causes of diabetes
There are some unusual causes of diabetes
which result from genetically determined
which result from genetically determined
abnormalities of insulin action. The metabolic
abnormalities of insulin action. The metabolic
abnormalities associated with mutations of the
abnormalities associated with mutations of the
insulin receptor may range from
insulin receptor may range from
hyperinsulinaemia and modest
hyperinsulinaemia and modest
hyperglycaemia to symptomatic diabetes.
hyperglycaemia to symptomatic diabetes.
Some individuals with these mutations have
Some individuals with these mutations have
acanthosis nigricans. Women may have
acanthosis nigricans. Women may have
virilization and have enlarged, cystic ovaries.
virilization and have enlarged, cystic ovaries.
In the past, this syndrome was termed Type A
In the past, this syndrome was termed Type A
insulin resistance.
insulin resistance.

Diabetes type 3 B (2)
Leprechaunism and Rabson-Mendenhall
Leprechaunism and Rabson-Mendenhall
syndrome are two paediatric syndromes
syndrome are two paediatric syndromes
that have mutations in the insulin
that have mutations in the insulin
receptor gene with subsequent alterations
receptor gene with subsequent alterations
in insulin receptor function and extreme
in insulin receptor function and extreme
insulin resistance. The former has
insulin resistance. The former has
characteristic facial features while the
characteristic facial features while the
latter is associated with abnormalities of
latter is associated with abnormalities of
teeth and nails and pineal gland
teeth and nails and pineal gland
hyperplasia.
hyperplasia.

Diabetes type 3 B (3)
Type 3 B.
Type 3 B.
Genetic defects in insulin action
Genetic defects in insulin action
Type A insulin resistance
Type A insulin resistance
Leprechaunism
Leprechaunism
Rabson-Mendenhall syndrome
Rabson-Mendenhall syndrome
Lipoatrophic diabetes
Lipoatrophic diabetes
Others
Others

Diabetes type 3 C (1)
Any process that diffusely injures the pancreas can cause
Any process that diffusely injures the pancreas can cause
diabetes. Acquired processes include pancreatitis, trauma,
diabetes. Acquired processes include pancreatitis, trauma,
infection, pancreatic carcinoma, and pancreatectomy. With
infection, pancreatic carcinoma, and pancreatectomy. With
the exception of cancer, damage to the pancreas must be
the exception of cancer, damage to the pancreas must be
extensive for diabetes to occur. However,
extensive for diabetes to occur. However,
adenocarcinomas
adenocarcinomas
that involve only a small portion of the pancreas have been
that involve only a small portion of the pancreas have been
associated with diabetes. This implies a mechanism other
associated with diabetes. This implies a mechanism other
than simple reduction in
than simple reduction in
-cell mass. If extensive enough,
-cell mass. If extensive enough,
cystic fibrosis and haemochromatosis will also damage beta
cystic fibrosis and haemochromatosis will also damage beta
cells and impair insulin secretion. Fibrocalculous
cells and impair insulin secretion. Fibrocalculous
pancreatopathy may be accompanied by abdominal pain
pancreatopathy may be accompanied by abdominal pain
radiating to the back and pancreatic calcification on X-ray
radiating to the back and pancreatic calcification on X-ray
and ductal dilatation. Pancreatic fibrosis and calcified stones
and ductal dilatation. Pancreatic fibrosis and calcified stones
in the exocrine ducts are found at autopsy.
in the exocrine ducts are found at autopsy.

Diabetes type 3 C (2)
Type 3 C.
Type 3 C.
Diseases of the exocrine pancreas
Diseases of the exocrine pancreas
Fibrocalculous pancreatopathy
Fibrocalculous pancreatopathy
Pancreatitis
Pancreatitis
Trauma / pancreatectomy
Trauma / pancreatectomy
Neoplasia
Neoplasia
Cystic fibrosis
Cystic fibrosis
Haemochromatosis
Haemochromatosis
Others
Others

Diabetes type 3 D (1)
Several hormones (e.g. growth hormone, cortisol,
Several hormones (e.g. growth hormone, cortisol,
glucagon, epinephrine) antagonize insulin action.
glucagon, epinephrine) antagonize insulin action.
Diseases associated with excess secretion of these
Diseases associated with excess secretion of these
hormones can cause diabetes (e.g. Acromegaly,
hormones can cause diabetes (e.g. Acromegaly,
Cushing's Syndrome, Glucagonoma and Phaeo
Cushing's Syndrome, Glucagonoma and Phaeo
-
-
chromocytoma).
chromocytoma).
Somatostatinoma, and aldostero
Somatostatinoma, and aldostero
-
-
noma-induced hypokalaemia, can cause diabetes,
noma-induced hypokalaemia, can cause diabetes,
at least in part by inhibiting insulin secretion.
at least in part by inhibiting insulin secretion.
Hyperglycaemia generally resolves following
Hyperglycaemia generally resolves following
successful removal of the tumour
successful removal of the tumour
and
and
when the
when the
hormone excess is removed.
hormone excess is removed.

Diabetes type 3 D (2)
Type 3 D.
Type 3 D.
Endocrinopathies
Endocrinopathies
Cushing's syndrome
Cushing's syndrome
Acromegaly
Acromegaly
Phaeochromocytoma
Phaeochromocytoma
Glucagonoma
Glucagonoma
Hyperthyroidism
Hyperthyroidism
Somatostatinoma
Somatostatinoma
Others
Others
Diabetes type 3 E (1)
Many drugs can impair insulin secretion.
Many drugs can impair insulin secretion.
These drugs may not, by themselves,
These drugs may not, by themselves,
cause diabetes but they may precipitate
cause diabetes but they may precipitate
diabetes in persons with insulin
diabetes in persons with insulin
resistance. Certain
resistance. Certain
rare
rare
toxins such as
toxins such as
Vacor (a rat poison) and pentamidine can
Vacor (a rat poison) and pentamidine can
permanently destroy pancreatic beta cells.
permanently destroy pancreatic beta cells.
There are also many drugs and hormones
There are also many drugs and hormones
which can impair insulin action. Examples
which can impair insulin action. Examples
include nicotinic acid and glucocorticoids.
include nicotinic acid and glucocorticoids.

Diabetes type 3 E (2)
Type 3 E.
Type 3 E.
Drug- or chemical-induced
Drug- or chemical-induced
Nicotinic acid
Nicotinic acid
Glucocorticoids
Glucocorticoids
Thyroid hormone
Thyroid hormone
Alpha-adrenergic agonists
Alpha-adrenergic agonists
Beta-adrenergic agonists
Beta-adrenergic agonists
Thiazides
Thiazides
Dilantin
Dilantin
Pentamidine
Pentamidine
Vacor
Vacor
Interferon-alpha therapy
Interferon-alpha therapy
Others
Others

Diabetes type 3 F (1)
Type 3 F.
Type 3 F.
Infections
Infections
Congenital rubella
Congenital rubella
Cytomegalovirus
Cytomegalovirus
Others
Others

Diabetes type 3 G (1)
Diabetes may be associated with several immunological
Diabetes may be associated with several immunological
diseases different from the Type 1 diabetes. Postprandial
diseases different from the Type 1 diabetes. Postprandial
hyperglycaemia of a severity sufficient to fulfil the criteria for
hyperglycaemia of a severity sufficient to fulfil the criteria for
diabetes
diabetes
is present
is present
in rare individuals who spontaneously
in rare individuals who spontaneously
develop insulin autoantibodies
develop insulin autoantibodies
.
.
However, these individuals
However, these individuals
generally present with symptoms of hypoglycaemia rather than
generally present with symptoms of hypoglycaemia rather than
hyperglycaemia. The "stiff man syndrome" is an autoimmune
hyperglycaemia. The "stiff man syndrome" is an autoimmune
disorder of the central nervous system, characterized by
disorder of the central nervous system, characterized by
stiffness of the axial muscles with painful spasms. Affected
stiffness of the axial muscles with painful spasms. Affected
people usually have high titres of the GAD autoantibodies and
people usually have high titres of the GAD autoantibodies and
approximately one-half will develop diabetes. Patients receiving
approximately one-half will develop diabetes. Patients receiving
interferon alpha have been reported to develop diabetes
interferon alpha have been reported to develop diabetes
associated with islet cell autoantibodies and, in certain
associated with islet cell autoantibodies and, in certain
instances, severe insulin deficiency.
instances, severe insulin deficiency.

Diabetes type 3 G (2)
Anti-insulin receptor antibodies can cause diabetes
Anti-insulin receptor antibodies can cause diabetes
by binding to the insulin receptor thereby reducing
by binding to the insulin receptor thereby reducing
the binding of insulin to target tissues. However,
the binding of insulin to target tissues. However,
these antibodies also can act as an insulin agonist
these antibodies also can act as an insulin agonist
after binding to the receptor and can thereby cause
after binding to the receptor and can thereby cause
hypoglycaemia.
hypoglycaemia.
Anti-insulin receptor antibodies are occasionally
Anti-insulin receptor antibodies are occasionally
found in patients with systemic lupus
found in patients with systemic lupus
erythematosus and other autoimmune diseases. As
erythematosus and other autoimmune diseases. As
in other states of extreme insulin resistance,
in other states of extreme insulin resistance,
patients with anti-insulin receptor antibodies often
patients with anti-insulin receptor antibodies often
have acanthosis nigricans. In the past, this
have acanthosis nigricans. In the past, this
syndrome was termed Type B insulin resistance.
syndrome was termed Type B insulin resistance.
Diabetes type 3 G (3)
Type 3 G.
Type 3 G.
Uncommon forms of immune-
Uncommon forms of immune-
mediated diabetes
mediated diabetes
Insulin autoimmune syndrome
Insulin autoimmune syndrome
(antibodies to insulin)
(antibodies to insulin)
Anti-insulin receptor antibodies
Anti-insulin receptor antibodies
"Stiff Man" syndrome
"Stiff Man" syndrome
Others
Others

Diabetes type 3 H (1)
Many genetic syndromes are accompanied by
Many genetic syndromes are accompanied by
an increased incidence of diabetes mellitus.
an increased incidence of diabetes mellitus.
These include the chromosomal abnormalities
These include the chromosomal abnormalities
of Down's syndrome, Klinefelter's syndrome
of Down's syndrome, Klinefelter's syndrome
and Turner's syndrome. Wolfram's syndrome
and Turner's syndrome. Wolfram's syndrome
is an autosomal recessive disorder
is an autosomal recessive disorder
characterized by insulin-deficient diabetes
characterized by insulin-deficient diabetes
and the absence of beta cells at autopsy.
and the absence of beta cells at autopsy.
Additional manifestations include diabetes
Additional manifestations include diabetes
insipidus, hypogonadism, optic atrophy, and
insipidus, hypogonadism, optic atrophy, and
neural deafness.
neural deafness.

Diabetes type 3 H (2)
Type 3 H.
Type 3 H.
Other Genetic Syndromes Sometimes Associated with
Other Genetic Syndromes Sometimes Associated with
Diabetes
Diabetes
Down's syndrome
Down's syndrome
Friedreich's ataxia
Friedreich's ataxia
Huntington's chorea
Huntington's chorea
Klinefelter's syndrome
Klinefelter's syndrome
Lawrence-Moon-Biedel syndrome
Lawrence-Moon-Biedel syndrome
Myotonic dystrophy
Myotonic dystrophy
Porphyria
Porphyria
Prader-Willi syndrome
Prader-Willi syndrome
Turner's syndrome
Turner's syndrome
Wolfram's syndrome
Wolfram's syndrome

Gestational Diabetes
(1)
Gestational diabetes is carbohydrate
Gestational diabetes is carbohydrate
intolerance resulting in hyperglycaemia of
intolerance resulting in hyperglycaemia of
variable severity with onset or first
variable severity with onset or first
recognition during pregnancy. It does not
recognition during pregnancy. It does not
exclude the possibility that the glucose
exclude the possibility that the glucose
intolerance may antedate pregnancy but
intolerance may antedate pregnancy but
has been previously unrecognized. The
has been previously unrecognized. The
definition applies irrespective of whether
definition applies irrespective of whether
or not insulin is used for treatment or the
or not insulin is used for treatment or the
condition persists after pregnancy.
condition persists after pregnancy.

Gestational Diabetes
(2)
Women who become pregnant and
Women who become pregnant and
who are known to have diabetes
who are known to have diabetes
mellitus which antedates pregnancy
mellitus which antedates pregnancy
do not have gestational diabetes but
do not have gestational diabetes but
have "diabetes mellitus and
have "diabetes mellitus and
pregnancy" and should be treated
pregnancy" and should be treated
accordingly before, during, and
accordingly before, during, and
after the pregnancy.
after the pregnancy.

Gestational Diabetes
(3)
Individuals at high risk for gestational
Individuals at high risk for gestational
diabetes include older women, those with
diabetes include older women, those with
previous history of glucose intolerance,
previous history of glucose intolerance,
those with a history of large for gestational
those with a history of large for gestational
age babies, women from certain high-risk
age babies, women from certain high-risk
ethnic groups, and any pregnant woman
ethnic groups, and any pregnant woman
who has elevated fasting, or casual, blood
who has elevated fasting, or casual, blood
glucose levels. Formal systematic testing
glucose levels. Formal systematic testing
for gestational diabetes is usually done
for gestational diabetes is usually done
between 24 and 28 weeks of gestation.
between 24 and 28 weeks of gestation.

Gestational Diabetes
(4)
To determine if gestational diabetes is present
To determine if gestational diabetes is present
in pregnant women, a standard OGTT
in pregnant women, a standard OGTT
should be performed after overnight fasting
should be performed after overnight fasting
(8-14 hours) by giving 75 g anhydrous
(8-14 hours) by giving 75 g anhydrous
glucose in 250-300 ml water. Plasma
glucose in 250-300 ml water. Plasma
glucose is measured fasting and after 2
glucose is measured fasting and after 2
hours. Pregnant women who meet WHO
hours. Pregnant women who meet WHO
criteria for diabetes mellitus or IGT are
criteria for diabetes mellitus or IGT are
classified as having Gestational Diabetes
classified as having Gestational Diabetes
Mellitus (GDM). After the pregnancy ends,
Mellitus (GDM). After the pregnancy ends,
the woman should be re-classified
the woman should be re-classified
Document Outline
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Slide 45
- Slide 46
- Slide 47
- Slide 48
- Slide 49
- Slide 50
- Slide 51
- Slide 52
- Slide 53
- Slide 54
- Slide 55
- Slide 56
- Slide 57
- Slide 58
Wyszukiwarka
Podobne podstrony:
DM ang Dgn black
DM ang Trtm
DM NewThreats ang id 137396 Nieznany
Hydrocephalus(ang)
DP i DM
DM
Wstrzasy ang ppt
Glikoliza prezentacja (ang)
08 BIOCHEMIA mechanizmy adaptac mikroor ANG 2id 7389 ppt
dgn NM
3Kocioł ang
Dgn Ukł Krąż
ns EiT 1 2st ang 2008
2010 ang
osteoarthritis ang ppt
j ang ark pdst
Kody TV do pilota DM 800HD
więcej podobnych podstron