PERSONAL USE
ONLY
W W W
.
M
E D
S
C I
M
O N I T
.
C O M
Diagnostics and Medical Technology
© Med Sci Monit, 2004; 10(4): MT53-63
PMID: 15039654
MT53
MT
Prolonged intracranial pressure (ICP) monitoring
in non-traumatic pediatric neurosurgical diseases
Gianpiero Tamburrinibcdef, Concezio Di Roccoa, Francesco Velardia,
Pietro Santinia
Pediatric Neurosurgical Unit, Catholic University Medical School, Rome, Italy
Source of support: Department sources.
Summary
Background:
A limited number of studies have addressed the methods, indications and particular problems
that may occur when programming prolonged intracranial pressure (ICP) monitoring in
pediatric patients. Parenchymal fiberoptic transducers have been shown to give reliable ICP
readings; moreover, they present a relatively low rate of complications, are easily placed and,
as they are solid state, they are not subject to obstruction.
Material/Methods:
A recently developed fiberoptic ICP transducer (Codman
®
intraparenchymal sensor) was used
to continuously monitor intracranial pressure in seventy children with non-traumatic neuro-
surgical diseases. The admitting diagnoses were hydrocephalus or shunt-related problems in
33 cases, single-suture (5 cases) or complex (16 cases) craniosynostosis in 21 patients, and syl-
vian scissure arachnoid cyst (SAC) in 16 cases. A software (ICP monitoring release
®
) designed
in our department was used for ICP recording storage and analysis.
Results:
Raised ICP values were found in six of the seventeen patients with a suspected active hydro-
cephalus, 24% of children with non-syndromic craniosynostosis, 52.8% of syndromic cranio-
synostosis patients, 50% of the children with a Type II SAC and two of the three patients with
Type III SAC.
Conclusions:
Overall, prolonged ICP monitoring proved to be extremely useful in guiding surgical indica-
tions. The fiberoptic device used in our unit was shown to be reliable and associated with a
relatively low rate of complications. Finally, the software allowed easy review and analysis of
the obtained data.
key words:
intracranial pressure • monitoring • children • non-traumatic diseases
Full-text PDF:
http://www.MedSciMonit.com/pub/vol_10/no_4/4188.pdf
Word count:
4631
Tables:
3
Figures:
1
References:
31
Received: 2003.09.22
Accepted: 2003.12.03
Published: 2004.04.01
Author’s address:
Gianpiero Tamburrini, Pediatric Neurosurgical Unit, Catholic University Medical School, Largo ‘A. Gemelli’ ,8,
00168 Rome, Italy, e-mail: gtamburrini@hotmail.com
Authors’ Contribution:
A
Study Design
B
Data Collection
C
Statistical Analysis
D
Data Interpretation
E
Manuscript Preparation
F
Literature Search
G
Funds Collection
Electronic PDF security powered by ISL-science.com
This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited.

PERSONAL USE
ONLY
MT54
Med Sci Monit, 2004; 10(4): MT53-63
Diagnostics and Medical Technology
B
ACKGROUND
Intracranial pressure (ICP) monitoring is now a widely
accepted tool in the management of various neurosurgi-
cal diseases. The results and complications of monitoring
adult patients have been extensively reported; in con-
trast, a limited number of studies have been addressed to
the indications and particular problems that may occur
in pediatric patients. The main indications in children
have been head trauma, ventriculomegaly and shunt
complications (i.e. shunt malfunction, slit ventricles syn-
drome), craniosynostosis, intracranial tumors, and hem-
orrhage [1–11].
One problem is that there is no universally accepted
scale of normal and abnormal ICP values in children.
The lack of accurate measurements in normal babies
and modifications of the intracranial compliance during
the first year of life specifically contribute to this point
[5,9,12,13]. Most papers refer to Minns’ conclusions;
according to this author, who reviewed all studies
before 1990 in which ICP had been objectively mea-
sured, the upper limits of normal are: 3.5 mmHg in
neonates, 5.8 mmHg in infants, 6.4 mmHg in children,
and 15.3 mmHg in adolescents and adults [13].
However, some authors disagree with this assessment,
stating that all the children above one year of life with
closed sutures should be evaluated with adult parame-
ters (normal range: 0–15 mmHg) [8,9,11].
One of the other main difficulties encountered when
programming ICP measurement in children is the lack
of cooperation of younger patients, which influences the
reliability of the recordings. A number of devices and
techniques have been proposed which can be divided in
three major groups: 1) extracranial devices (anterior
fontanelle transducers, tympanic membrane displace-
ment sensors) [10,14], 2) superficial ICP monitoring
transducers (extradural subdural and subarachnoid
bolts) [5,6,12,15,16], and 3) deep devices (intraparenchy-
mal fiberoptic transducers and ventricular catheters)
[8,9,11]. Whatever the chosen monitoring apparatus,
continuous and prolonged ICP recording is needed in
most cases. Currently, paper waveforms have been
replaced by digital recorders which, however, if taken
alone, require periodic nurse control and value registra-
tion. In addition, most of them do not allow wave analy-
sis, which can be particularly useful in sleep recordings.
For this reason a number of software has been created to
store registrations on a personal computer’s (PC) hard
disk, with the possibility to analyze the data obtained ret-
rospectively [1–4, 17–22).
The present study had two objectives: the first was to
evaluate the reliability of a recently developed fiberoptic
ICP transducer (Codman
®
intraparenchymal sensor) in
a population of pediatric patients with different non-
traumatic neurosurgical diseases; the second was to
review our experience with a software (ICP Monitoring
Release
®
) that was designed in 1998 in our department
for this kind of transducer and the connected digital
analyzer system (Codman
®
ICP Express).
M
ATERIAL AND
M
ETHODS
All children with non-traumatic neurosurgical diseases
who underwent ICP monitoring in our Unit between
1998 and January 2003 were reviewed. Seventy patients
were selected and subdivided into three groups accord-
ing to admission diagnoses: the first group was com-
posed of 33 children admitted with a diagnosis of ven-
triculomegaly, hydrocephalus or shunt-related prob-
lems; the second was composed of 21 children affected
by single suture (5 cases) or complex (16 cases) cranio-
synostoses and the third of 16 children who were affect-
ed by arachnoid cysts (sylvian arachnoid cysts: 15 cases,
intraventricular arachnoid cysts: 1 case). The children
with sylvian arachnoid cysts (SAC) were further subdi-
vided into three groups based on CT scan and MRI
imaging, according to the morphological classification
propounded by Galassi et al. in 1980 [23]. Group I was
made up of four children with Type I cysts: i.e. small
semicircular arachnoid cysts confined to the anterior
part of the temporal fossa. Group II comprised eight
children with quadrangular, medium-sized temporal
cysts (Type II). Finally, group III consisted of three
children with Type III cysts: i.e. large, oval, fluid collec-
tions which occupied the temporal fossa entirely,
opened the Sylvian fissure and partially extended over
the cerebral convexity.
Prolonged intracranial pressure (ICP) recording (min:
12 h; max: 92 h; mean recording time: 47 h) was per-
formed in all cases. For this we utilized a system com-
posed of an extensible silicone microprocessor (Cod-
man
®
) connected to a Codman ICP Express
®
display
developed for ICP check. ICP Express
®
is programmed
to give an electrical signal which is proportional to the
ICP values. The collected information was uploaded by
cable to a personal computer (PC) provided with a digi-
tal/analog converter card. A software devised in our
department (ICP Monitoring Release
®
) was used to
store ICP recordings (256 values/sec) on the PC’s hard
disk. This program allows continuous tracking during
the recording or at a later time, with the possibility of
choosing the date, hour and minutes of the recording to
review. It also enables the automatic analysis of the col-
lected ICP values in bar or star graphics once a time
interval (1–24 h) is selected.
The microprocessor was implanted intraparenchimally
in the posterior right frontal brain tissue in the children
of the first two groups (hydrocephalus, shunt-related
diseases, and craniosynostosis) and adjacent to the
major extension of the arachnoid cyst in the last group
(arachnoid cysts).
Nurses and parents were asked to register the child’s
activity during the recording period; artifacts due to
crying, feeding, or playing were noted and excluded
from the final assessment. For all the patients we evalu-
ated the tracks of the continuous recording and changes
in ICP during physiological sleep and those following
artificial maneuvers, such as jugular vein compression
and release. The presence or absence of plateau A-
waves was also accounted and was chosen as a decision
Electronic PDF security powered by ISL-science.com
This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited.
PERSONAL USE
ONLY
MT55
Med Sci Monit, 2004; 10(4): MT53-63
Gianpiero T et al – Prolonged intracranial pressure (ICP) monitoring…
MT
parameter in children with doubtful results of the ICP
recordings. Ten mmHg was chosen as the upper nor-
mal ICP limit in resting conditions in children under
one year of age and/or with opened sutures and 15
mmHg in patients with closed sutures. Bar graphs were
utilized in each case to illustrate the percentage distribu-
tion of the ICP values during the recording period, gen-
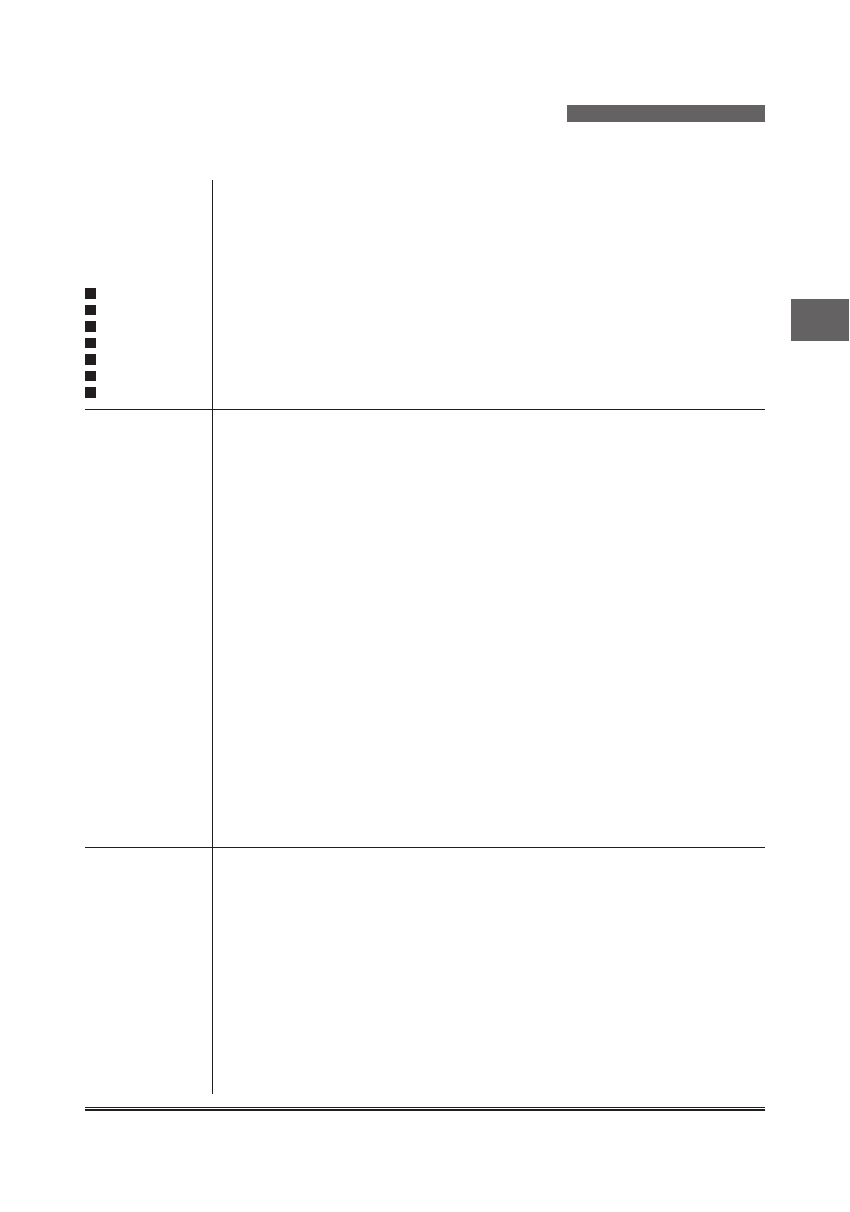
erally in steps of 2, 5 or 10 mmHg. A ‘star-like’ graphic
representation of the ICP pattern was also utilized to
compare visually ICP behavior immediately during the
day and night (Figure 1).
R
ESULTS
Hydrocephalus and shunt-related diseases
This group was composed of 33 children (M/F=22/11)
with ages at diagnosis varying between 3 months and 17
years (mean: 5.27 years). The indication to ICP moni-
toring was ventriculomegaly or suspected active hydro-
cephalus in 17 cases, suspected shunt malfunction in 10
patients, slit ventricles syndrome in 4 cases, and an inci-
dentally discovered shunt migration and a post-shunt
craniosynostosis with secondary Chiari I in the last two
cases. Symptoms at the time of admission to our unit
included macrocrania in 16 cases, symptoms of intracra-
nial hypertension (headache, vomiting, tense anterior
fontanelle) in 17 patients, seizures in four patients, and
a psychomotor retardation in one case. The patient with
the incidental discovery of shunt migration was asymp-
tomatic. Neuroradiologic examinations (CT and/or
MRI) did not allow definite conclusions in all cases.
The length of ICP monitoring varied between 12 and
92 hours (mean: 46.1 h). Six of the 17 patients with ven-
triculomegaly or suspected active hydrocephalus (four
children with congenital hydrocephalus and one each
with hydrocephalus in myelomeningocele and post-
hemorrhagic hydrocephalus) showed abnormal ICP val-
ues for 65 % or more of the recording time period.
Plateau A-waves were documented in three of these
cases. Normal ICP values (62% or more in the normal
range) were recorded in the remaining eleven patients
of this group (five patients with benign hydrocephalus;
three with congenital hydrocephalus, 2 with arrested
hydrocephalus, and 1 with post-hemorrhagic hydro-
cephalus), excluding the need to surgical treatment.
Four of the ten patients referred to us with a diagnosis
of shunt malfunction had normal ICP values (68–93.8%
of the recordings in the normal range), in spite of symp-
toms simulating intracranial hypertension (H/A, vomit-
ing) had been exhibited by three of them. Slight clinical
symptoms indicated ICP monitoring in the other six
patients of this group that showed pathological ICP val-
ues for 43.2% to 79.4% of the recording time. Plateau A-
waves were also found in 5/6 of these children. The
presence or absence of nocturnal A-waves was particu-
larly important in the evaluation of children with sus-
Figure 1. An example of the images offered by the software used in our Unit for ICP monitoring; (A) Trace of ICP recording; (B) Automatic bar graphic
of the ICP percentages distribution during the entire recording; (C) Automatic star graphic showing day and night distribution of ICP values.
Electronic PDF security powered by ISL-science.com
This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited.

PERSONAL USE
ONLY
MT56
Med Sci Monit, 2004; 10(4): MT53-63
Diagnostics and Medical Technology
pected slit ventricles syndrome; indeed, although all of
them had normal ICP values for more than 50% of the
recordings, plateau A-waves were found in three cases,
indicating the need for a surgical treatment (Table 1).
Craniosynostosis
Twenty-one children (13 M/8 F) affected by simple (five
cases) or complex (sixteen cases) craniosynostosis under-
went ICP monitoring in our unit between 1998 and
January 2003. Mean age was 1.6 years (min: 3 months,
max: 5 years). Diagnoses at admission were Apert syn-
drome in five children, Crouzon syndrome in four
cases, Pfeiffer syndrome in three cases (two children
with Pfeiffer III and one child with Pfeiffer II syn-
drome), scaphocephaly in three cases, brachicephaly in
two cases, turricephaly in two children, and osteopetro-
sis in the last two cases. A clinical geneticist confirmed
the diagnosis in all cases.
Fourteen out of the sixteen children with complex cran-
iosynostosis (five with Apert syndrome, four with
Crouzon syndrome, two with Pfeiffer syndrome, two
with turricephaly, and one with osteopetrosis) presented
abnormal ICP values with evidence of nocturnal A-
waves in all cases (mean length of ICP monitoring: 43.5
h). A case-based surgical treatment was performed in
these patients: eleven children underwent an occipital
expansive cranioplasty as a first step, followed by a
bifronto-orbital advancement in four cases (two patients
with Crouzon syndrome, one with Pfeiffer II syndrome,
and one with Apert syndrome), or by a ventriculo-peri-
toneal shunt for an associated hydrocephalus in two
patients (one child with Pfeiffer III syndrome and the
second with Apert syndrome), or by a bifronto-orbital
advancement and subsequent ventriculoperitoneal
shunt in two cases (one child with Apert syndrome and
one with turricephaly). The last three children of this
subgroup (one with Crouzon syndrome, one with Apert
syndrome, and one with osteopetrosis), all showing rela-
tively lower ICP values (53.2%, 45.4%, 45.7% of the
recordings in the normal range), underwent exclusively
a bifronto-orbital advancement.
Post-operative ICP monitoring was effected in seven
patients (mean postoperative length of ICP monitoring:
42.1 h) and a significant reduction of ICP values, a re-
duction or disappearance of plateau A-waves was docu-
mented in all cases. Only two children affected by com-
plex craniosynostosis (one with Pfeiffer III syndrome
and one with osteopetrosis) who underwent preopera-
tive ICP monitoring had normal ICP values for the
majority of the recording time (86.5%–97.9% of the ICP
values within the normal range).
The five patients affected by single-suture craniosynos-
tosis (three children with scaphocephaly and two chil-
dren with brachicephaly) had all ICP values in the nor-
mal range (mean recording time: 39.6 h, 65.1–82.4% of
the recordings <15mmHg); plateau A-waves were
absent in all cases (Table 2).
Arachnoyd cysts
Of our sixteen children with arachnoid cysts, fifteen
were affected by sylvian fissure arachnoid cysts (SAC)
and one by a left lateral ventricle cyst. Eight patients
were symptomatic: three presented with a history of
recurrent headache (one had a Type I SAC and two had
a Type II SAC) and one with epileptic seizures (Type I
SAC). The other four children of this subgroup of
patients (one with a Type II SAC and three with Type
III SAC) showed signs of increased ICP (tense and
bulging anterior fontanelle in one case, headache and
vomiting in the remaining three cases). The diagnosis
was incidental in six of the remaining eight children
after a CT or MR imaging carried out because of head
injury in three cases (two with a Type I and the third
with a Type II SAC), macrocrania in one case (left ven-
tricular cyst), or to investigate the possible cause of
hypertonia (1 case: Type II SAC) or generalized dyston-
ic movements (1 case: Type II SAC). In two instances a
temporal cyst was recognized in utero at ‘routine’ echo-
graphic examination during pregnancy. Both of the
infants had a Type II SAC and did not show any appar-
ent sign of increased ICP at birth. Neurological exami-
nation at admission was negative in ten patients and
presumably unrelated to the presence of the arachnoid
cyst in three (psychomotor delay and increased muscle
tone due to perinatal hypoxia in two cases and bilateral
anacusia in one case). Bilateral papilledema was discov-
ered in one patient, while cranial asymmetry was the
only sign in the last two cases (Table 3).
The EEG examination was normal or characterized only
by unspecific abnormalities in 13 cases. In particular,
the only child who presented with seizures had bilateral,
unspecific EEG abnormalities. Three children, one har-
boring a Type I, the second a Type II, and the third a
Type III cyst, showed focal EEG anomalies on the tem-
poral region homolaterally to the lesion.
Mean length of ICP monitoring was 46.9 hours. ICP
recordings were in the normal range in the four chil-
dren with type I SAC, in spite of the fact that two of
them were symptomatic (one complaining of recurrent
headaches, the second of epileptic seizures). When the
ICP values were distributed in steps of 5 mmHg, they
remained below the limit of 15 mmHg for more than
80% of the recording time in all cases (83.9%, 87.9%,
89.6%, 92%, respectively). Four of the eight children
with a Type II SAC had repeated episodes of abnormal-
ly elevated ICP (55%, 57%, 76%, 84.4% of the record-
ings >15 mmHg), even though three of them had inci-
dental (1 case) or prenatal (2 cases) diagnosis. The
remaining four patients with Type II SAC had normal
ICP values for more than 80% of the recording time
period. Two of the three patients with Type III SAC
had almost constantly abnormal ICP values (92.9%,
98.7% >15 mmHg), while ICP values were in the nor-
mal range in the third patient of this subgroup, which
was apparently symptomatic at admission (headache,
vomiting). The patient with an intraventricular arach-
noid cyst had normal ICP values for more than 70% of
the recording time.
Electronic PDF security powered by ISL-science.com
This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited.
PERSONAL USE
ONLY
MT57
Med Sci Monit, 2004; 10(4): MT53-63
Gianpiero T et al – Prolonged intracranial pressure (ICP) monitoring…
MT
Patient
Sex
Age
Diagnosis*
*Sy/Si
CT/MRI
*TR
ICP <10
MmHg
ICP >10
MmHg
ICP <15
MmHg
ICP >15
MmHg
Plateau
A-waves
Complica-
tions
1 .A.A.
2. A.C.
3. A.F.
4. A.I.
5. A.M.
6. B.A.
7. B.R.
8. B.Re.
9. C.G.
10. C.M.
11. E.G.
12. G.V.
13. L.C.
14. L.A.
15. L.G.
16. L. Gi.
17. L.P.
18. M.A.
19. M.D.
20. M.V.
21. M.F.
22. M.J.
23. M.A.
24. P.F.
25. P.G.
26. P.V.
27. R.F.
28. S.N.
29. T.M
30. T.R.
31. T.F.
32. V.E.
33. V.N.
M
F
F
F
F
M
F
F
M
F
M
F
M
F
M
M
M
M
M
F
M
M
M
M
F
M
M
M
M
M
M
M
M
15 Y
11 M
6 M
3 Y
4 Y
7 Y
11 Y
11 M
4 Y
3 Y
13 M
4 Y
3 Y
3 M
11 Y
15 M
15 Y
9 M
4 M
17 Y
9 Y
4 Y
5 Y
2 Y
3 Y
14 Y
8 Y
4 Y
3 Y
4 Y
2 Y
11 Y
2 Y
**Sh. Malf.
(PE Hy)
**Hy/MMC
Pe Hy
Sh. Malf.
(**Co. Hy)
Sh. Malf.
(Co. Hy)
Sh. Malf.
(Pe Hy)
Co. Hy
Sh. Malf.
(Co. Hy)
Co. Hy
**Arr. Hy
**Be. Hy
**SVS
SVS
Co. Hy
Sh. Malf.
(Pe Hy)
Be. Hy
Sh. Malf.
(Pe Hy)
Co. Hy.
Sh. Malf.
(Co. Hy)
Sh. Malf.
(Co. Hy)
Sh. Malf.
(Co. Hy)
Be. Hy
SVS
**Sh. Migr.
Be. Hy
Post-shunt
**CRS and
Chiari I
SVS
Co. Hy
Co. Hy
Arr. Hy
Pe Hy
Co. Hy
Be. Hy
**H/A, Vo.
Ma.
**Se. Ps.
Ret., Ma.
H/A
H/A
H/A
H/A, Vo.
Ma.
Ma., H/A
Ma.
Ma.
H/A, Vo.
H/A, Vo.
**Taf, Vo.
H/A
Ma.
Se., H/A,
Vo.
Ma.
Ma.
H/A, Vo.
H/A
Ma.
H/A, Vo.
Asympto-
matic
Ma.
H/A
H/A
Ma.
Ma.
Ma., Vo.
Ma., Se.
Ma., Se.
Ma.
No VD
Tetra-VD
Extreme
Tetra-VD
Moderate
Tetra-VD
Moderate
Tri-VD
Moderate
Tetra-VD
Tetra-vd
Tri-VD
Tetra-VD
Tetra-VD
Moderate
Tetra-VD
SV
SV
Tetra-VD
Tri-VD
Moderate
Tetra-VD
No VD
Moderate
Tetra-VD
Tetra-VD
No VD
No VD
Moderate
Tri-VD
SV
Moderate
Tri-VD
Moderate
Tetra-VD
Chiari I
SV
Tetra-VD
Tetra-VD
Tri-VD
Tri-VD
Tri-VD
Moderate
Tetra-VD
42 h
39 h
36 h
42 h
24 h
36 h
46 h
40 h
48 h
48 h
62 h
74 h
92 h
38 h
87 h
27 h
36 h
36 h
48 h
36 h
70 h
72 h
48 h
50 h
12 h
24 h
46 h
60 h
36 h
62 h
46 h
24 h
36 h
–
20.6%
21.4%
–
–
–
–
56.8%
–
–
–
–
–
34.7%
–
92.5%
–
12.6%
87.5%
–
–
–
–
–
–
–
–
–
–
–
–
–
–
–
79.4%
78.6%
–
–
–
–
43.2%
–
–
–
–
–
65.3%
–
7.5%
–
87.4%
12.5%
–
–
–
–
–
–
–
–
–
–
–
–
–
–
93.8%
–
–
68.6%
20.6%
74.3%
98.1%
–
21.4%
81.5%
66.8%
96.4%
75.7%
–
29.5%
–
22.9%
–
–
47.5%
28.6%
69.1%
57.6%
89.0%
93.6%
72.7%
64.3%
73.5%
19.8%
63.6%
62.7%
96.9%
89.6%
6.2%
–
–
31.4%
79.4%
25.7%
1.9%
–
78.6%
18.5%
33.2%
3.6%
24.3%
–
70.5%
–
77.1%
–
–
52.5%
71.4%
30.9%
42.4%
11.0%
6.4%
27.3%
35.7%
26.5%
80.2%
36.4%
37.3%
3.1%
10.4%
No
No
Yes
No
No
No
No
Yes
Yes
No
No
Yes
No
Yes
Yes
No
Yes
Yes
No
Yes
Yes
No
Yes
No
No
Yes
Yes
No
Yes
No
No
No
No
No
No
CSF leak
No
No
No
No
CSF leak
No
No
No
No
No
CSF leak
No
No
No
No
CSF leak
No
No
No
No
No
No
Hemorrha-
ge + me-
chanical
malfunction
No
No
No
No
No
No
No
Table 1. Clinical features and ICP findings in patients affected by hydrocephalus or shunt- related problems.
* diagnosis – at admission; sy/si – symptoms/signs; tr – length of icp monitoring;
** h/a – headache; vo. – vomiting; hy – hydrocephalus; be. – benign; co. – congenital; arr. – arrested; pe – posthemorrhagic; mmc – mielomeningocele;
ext hy – external hydrocephalus; sh. migr.– shunt migration; sh. malf. – shunt malfunction; svs – slit ventricle sindrome; vd – ventricular dilatation; sv – slit ventricles ;
se – seizures; ps. ret. – psychomotor retardation; ma. – macrocrania; taf – tense anterior fontanel; crs – craniosynostosis
Electronic PDF security powered by ISL-science.com
This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited.
PERSONAL USE
ONLY
MT58
Med Sci Monit, 2004; 10(4): MT53-63
Diagnostics and Medical Technology
Patient
Sex
Age
Diagnosis* Tr/Preop*
Preop ICP
<10 MmHg
Preop ICP
>10 MmHg
Preop
plateau
A-waves
Type
of surgery
Postop
(TR) ICP
<10 MmHg
Postop
ICP
>10 MmHg
Postop
plateau
A-waves
Complica-
tions
1. C.G.
2. C.Ma.
3. C.M.
4. C.S.
5. D.S.
6. F.G.
7. F.A.
8. K.R.
9. L.P.
10. M.A.
11. M.V.
12. M.F.
13. N.D.
14. P.M.
15. P.F
16. P.Fr.
17. P.G.
18. S.F.
19. T. A.
20. T.F.
21. T.A
M
M
M
F
F
F
F
M
M
M
M
F
M
M
M
F
M
F
M
F
M
5 M
8 M
8 M
6 M
6 M
2 Y
3 Y
6 M
2 M
5 Y
11 M
8 M
5 M
2 Y
4 M
5 M
7 M
3 M
8 Y
3 M
4 M
Apert
Pfeiffer III
Scaphocephaly
Apert
Crouzon
Scaphocephaly
(moderate)
Turricephaly
Apert
Crouzon
Turricephaly
Scaphocephaly
Crouzon
Brachicephaly
Apert
Osteopetrosis
Pfeiffer II
Brachicephaly
Pfeiffer III
Osteopetrosis
Crouzon
Apert
39 h
48 h
48 h
30 h
40 h
49 h
48 h
30 h
48 h
63 h
45 h
65 h
36 h
45 h
36 h
67 h
24 h
36 h
44 h
50 h
48 h
45.9%
86.5%
82.4%
14.1%
17%
67.9%
(<15
MmHg)
3.4%
(<15
MmHg)
6.1%
67.3%
36.1%
(<15
MmHg)
65.1%
53.2%
68.5%
45.7%
(<15
MmHg)
97.9%
20.1%
73.7%
1.8%
45.4%
(<15
MmHg)
57.1%
5.0%
54.1%
13.5%
17.6%
85.9%
83.0%
32.1%
(>15
MmHg)
96.6%
(>15
MmHg)
93.9%
32.7%
63.9%
(>15
MmHg)
34.9%
46.8%
31.5%
54.3%
(>15
MmHg)
2.1%
79.9%
26.3%
98.2%
54.6%
(>15
MmHg)
42.9%
95.0%
Yes
No
No
Yes
Yes
No
Yes
Yes
Yes
Yes
No
Yes
Yes
Yes
No
Yes
No
Yes
Yes
Yes
Yes
**Occipital
EC **VPS
–
Biparietal
CP
1.Occipital
EC
2. Bifronto
A.
1.Occipital
ec
2. Bifronto
A.
–
Occipital
EC
Occipital
EC
Occipital
EC
1. Occipital
EC
2. ** Bi-
fronto. A
3.VPS
Biparietal
CP
Bifronto. A
Bifronto. A
Bifronto. A
Bifronto. A
1. Occipi-
tal EC 2.
Bifronto. A
Bifronto. A
1. Occipital
EC 2. VPS
Bifronto. A
1. Occipital
EC 2. Bi-
fronto. A
1. Occipital
EC 2. VPS
3. Bifronto.
A
(46 h)
67.5%
–
–
(36 h)
69.3%
(68 h)
62.7%
–
(68h)
37.6%
(<15
MmHg)
(32 h)
50.2%
–
–
–
–
–
–
–
–
–
–
(46h)
73.3%
(<15
MmHg)
–
(46 h)
67.3%
32.5%
–
–
30.7%
37.3%
–
62.4%
>15
MmHg)
49.8%
–
–
–
–
–
–
–
–
–
–
26.7%
(>15
MmHg)
–
32.7%
Yes
(Reduced)
–
–
No
No
–
No
Yes
(reduced)
–
–
–
–
–
–
–
–
–
–
No
–
No
CSF leak
No
No
CSF leak
CSF leak
No
No
No
No
No
No
No
No
No
No
No
No
No
No
No
No
Table 2. Clinical features and ICP findings in patients affected by Craniosynostosis.
* diagnosis – at admission; tr – length of icp monitoring;
** ec – expansive cranioplasty; hy – hidrocephalus; vps – ventriculo-peritoneal shunt; bifronto. a – bifrontoorbital advancement; cp – cranioplasty
Electronic PDF security powered by ISL-science.com
This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited.
PERSONAL USE
ONLY
MT59
Med Sci Monit, 2004; 10(4): MT53-63
Gianpiero T et al – Prolonged intracranial pressure (ICP) monitoring…
MT
Complications
The overall complication rate was 17.1%, including 9 cases
of CSF leak (12.8%), which resolved with medication of
the surgical wound, two cases of mechanical failure (2.8%)
which required the reimplantation of the transducer, and
one case of hemorrhage (1.4%) surrounding the tip of the
fiberoptic device. The hemorrhage was documented on a
control CT performed because of a malfunction of the
ICP transducer (ICP values >100 mmHg, in an asympto-
matic child); no specific medical or surgical treatment was
required. No case of infection was recorded.
D
ISCUSSION
There is increasing experience in the use of continuous
ICP monitoring in pediatric neurosurgical diseases. The
major indication that can be found in the literature
involves children with severe craniocerebral trauma
[8,11,15,16,21,22]. Less information is available on
patients with non-traumatic conditions. However, dif-
ferent authors have stressed the importance of pro-
longed ICP recording in the diagnosis and preoperative
management of children with hydrocephalus, shunt-
related problems, and craniosynostosis [1–7,9,15]. Many
techniques have been proposed; extracranial as well as
epidural, subdural, and deep devices have been alterna-
tively used. Extracranial devices have the advantage of
being mini-invasive, not requiring a surgical procedure
to be implanted. A comparison with deep ICP measure-
ments (intraparenchymal and ventricular) has also
demonstrated their good reliability. They do, however,
present serious problems of fixation; indeed, exact
coplanimetry is needed. Furthermore, results are influ-
Patient
Sex
Age
Location
Symptoms that
lead to diagnosis
Clinical
symptoms
at admission
Neuroilogical
examination
at admission
EEG
(TR) ICP
<15
MmHg %
ICP >15
MmHg
Complica-
tions
1. B.S.
2. C.M.
3. S.G.M.
4.S. M.
5. A.R.
6. S. V.
7. D. F.
8. R. M.
9. N.S.
10. B. E.
11. S. E.
12. V.G.
13. B.M.
14. M.M.
15. M.S.
16. O.W.
M
M
M
M
M
F
M
M
M
M
M
M
M
M
M
M
8 Y
2 Y
3 Y
2 Y
12 Y
12 Y
1 Y
12 Y
11 Y
2 Y
15 Y
13 M
5 Y
15 Days
10 Y
4 Y
*L. Sylvian
(*type I)
R. Sylvian
(*type I)
L. Sylvian
(*type I)
*R. Sylvian
(*type I)
L. Sylvian
(*type ii)
L. sylvian
(*type II)
L. Sylvian
(*type II)
L. Sylvian
(*type II)
L. Sylvian
(*type II)
R. Sylvian
(*type II)
R. Sylvian
(*type II)
R. sylvian
(*type II)
L Sylvian
(*type III)
R. Sylvian
(*type III)
L Sylvian
(*type III)
Intraventricular
(*LLV)
Incidental
posttraumatic
Incidental
posttraumatic
Incidental
posttraumatic
Epilepsy
Headache
Psycomothor
delay due to
perinatal hypoxia
Increased bilateral
muscle tone
Functional dysto-
nic movement
of the neck and
the four arms
Headache,
vomiting
Incidental: prena-
tal ecographic
Incidental:
posttraumatic
Incidental: prena-
tal ecographic
Headache,
vomiting
Incidental:
prenatal
ecographic
Headache,
vomiting
Macrocrania
Asymptomatic
Asymptomatic
Headache
Epilepsy
Headache
Headache
Asymptomatic
Asymptomatic
Headache,
vomiting
Asymptomatic
Asymptomatic
Asymptomatic
Headache,
vomiting
Intracranial
hypertension
(tense a.f.)
Headache,
vomiting
Asymptomatic
Negative
Negative
Cranial
asymmetry
Psychomotor
delay
Negative
Psychomotor
delay; spastic
tetraparesis
Negative
Negative
Negative
Bilateral anacusia
(not related)
Negative
Negative
Bilateral
papilledema
Cranial
asymmetry
Negative
Negative
Focal
Aspecific
Aspecific
Aspecific
Aspecific
Aspecific
Aspecific
Aspecific
Aspecific
Aspecific
Focal
Aspecific
Aspecific
Aspecific
Focal
Negative
(46 h)
92%
(43 h)
83.9%
(40 h)
87.9%
(36 h)
89.6%
(46 h)
85%
(42 h)
85%
(51 h)
96.7%
(48 h)
81%
(46 h)
24%
(48 h)
45%
(60 h)
43%
(48 h)
15.6%
(65 h)
7.8%
(52 h) 1.3 %
(<10
MmHg)
(50 h)
99.1%
(30 h)
74.6%
8.0%
16.1%
12.1%
10.4%
15.0%
25.0%
3.3%
19.0%
76.30%
55.0%
57.0%
84.4%
92.2%
98.7%
(>10
mmhg)
0.9%
25.4%
No
No
No
No
No
No
CSF leak
No
No
No
No
mechani-
cal mal-
function
No
CSF leak
No
No
Table 3. Synopsis of clinical and ICP findings in children with arachnoid cysts.
* L – left; R – right; TYPE – according to Galassi classification; LLV – left lateral ventricle; ECM – endoscopic cyst marsupialization
Electronic PDF security powered by ISL-science.com
This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited.

PERSONAL USE
ONLY
MT60
Med Sci Monit, 2004; 10(4): MT53-63
Diagnostics and Medical Technology
enced by the external pressure applied and by the ten-
sion of the contact surface (for example, anterior
fontanelle and tympanic membrane) [10,13,14].
Epidural screws avoid opening of the dura, theoretically
lessening the risk of surgical complications. However,
they have not proven to be reliable because of signal
dampening and recording artifacts [13]. In this respect,
modern subdural and subarachnoid bolts give more
predictable results, although some authors have report-
ed disparate recordings (compared with ventricular
catheters) at pressures greater than 20 mmHg
[11,13,15]. Historically, the most accurate ICP record-
ings are obtained from the ventricles; however, ven-
triculostomy is related to a higher though limited risk of
complications compared with the other techniques
(seizures, hematoma, catheter obstruction and CSF
infections) [11,13].
Intraparenchymal fiberoptic devices were introduced at
the beginning of 1990s in order to reduce these risks
and obtain results comparable to ventricular ICP mea-
surements. After more than ten years of practice, the
advantages and disadvantages of the technique have
become clearer. The advantages are that transducers
give reliable ICP readings, can be easily placed, and
they are solid state, not subject to obstruction. Further-
more, they allow direct measurement of brain tissue
pressure in patients with small, compressed, or dislocat-
ed ventricles in which placement of a ventricular
catheter would be difficult. The main disadvantages are
a relatively high rate of mechanical failures and the
inability to recalibrate devices in situ [11–13,15,16].
Concerning mechanical failures, most authors report an
incidence of 2–7%. In a series of 98 children, Jensen et
al. referred to a rate as high as 13%. However, these
authors probably overstated this kind of complication;
indeed, in twelve patients there was only a suspicion of
‘drifting’ of the system, and only in one case (1%) was
there a real malfunction of the fiberoptic device [12].
Other complications that have been described using
parenchymal fiberoptic devices are hemorrhages sur-
rounding the tip of the transducer (0.5–1.5%), CSF
leaks (1.9–3%), and infections (0.3–7%) [11–13,15,16].
In our experience, nine children presented a CSF leak
(12.8%), a rate higher than in previous reports. Six
patients were under one year of age: it is possible that
the presence of more slack subcutaneous tissues in
infants may have favored the occurrence of this compli-
cation in our series. Mechanical failure (2.8%) and hem-
orrhage (1.4%) rates were in line with literature data.
No infection was observed.
Another important point to consider when performing
prolonged monitoring of the ICP is how to store and
analyze the results. In the past this kind of assessment
was carried out on paper tracings. Since the early 1980s,
a number of software systems have been proposed for
PC storage of the obtained data. Single pulse analysis of
the ICP waves, pulse-amplitude, and mean pressure
diagrams have been the main parameters included in
the evaluation programs [18–20]. For intensive care use,
the analysis of intracranial pressure has also been inte-
grated within the cerebrovascular parameters (cerebral
perfusion pressure, transcranial Doppler blood flow
velocity, and jugular bulb oxygen saturation) with the
objective of multimodal studies [10]. Eide et al. recently
proposed a software which allows not only the evalua-
tion of mean ICP and pulse waves, but also the relation-
ship between mean ICP and the number of ICP eleva-
tions within 10–24-hour periods [1–4]. The software
used in our unit (ICP monitoring release
®
), apart from
on-line and off-line evaluation of pulse waves, allows the
analysis of the mean ICP percentage distribution for
any chosen time period as well as for the whole record-
ing. Bar and star graphics can be automatically
obtained, enabling a general view. Furthermore, a cur-
sor can be moved over the desired part of the record-
ing; in this way not only the number and duration of
ICP elevations can be calculated, but artifacts can be
excluded from the final evaluation.
Hydrocephalus and shunt-related problems
Clinical symptoms and radiological data ensure the diag-
nosis of active hydrocephalus or shunt dysfunction
(mechanical obstruction, SVS) in most cases. However,
there is a significant minority of patients in whom the
clinical and radiological pictures are not so clear.
Symptoms, which may include headache and vomiting,
may not be related to the shunt or to the presence of
hydrocephalus. Viral infections or migraine may indeed
present with a picture suggesting an increase in intracra-
nial pressure, and children with chronic or episodic low
ICP after shunting may present with symptoms which
simulate a mechanical obstruction of the shunt. As the
long-term risks of a shunt implantation or revision may
be far from benign, it is important to make the right
diagnosis. Fouyas et al. continuously monitored intra-
parenchymal intracranial pressure in 18 patients with
ventriculomegaly and 23 patients with presumed shunt
malfunction. In 9 of the 18 children with ventricu-
lomegaly, the ICP was within normal limits and the
insertion of a shunt could be avoided; in 13 of the 23
children assessed for shunt malfunction, the change in
the ICP profile indicated a siphoning or over-drainage
process [9]. Massager studied intracranial pressure in 20
asymptomatic infants with increased head growth rates:
only eight of these children showed pathological ICP
recordings and needed surgical treatment [10].
Our experience confirms previous reports. Only six of
the seventeen patients with suspected active hydro-
cephalus showed abnormal ICP values and needed sur-
gical treatment. Four of the ten patients referred to us
with a diagnosis of shunt malfunction had normal ICP
values in spite of symptoms simulating intracranial
hypertension (H/A, vomiting) present in three of them.
The usefulness of ICP monitoring has also been demon-
strated in children with suspected slit ventricles syn-
drome (SVS). Using a parenchymal fiberoptic transduc-
er, Rekate was able to identify five separate groups of
patients among those initially referred for a SVS. He
concluded that there are several different syndromes
associated with headaches and small ventricles in shunt-
ed children, and that ICP monitoring can help to select
Electronic PDF security powered by ISL-science.com
This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited.

PERSONAL USE
ONLY
MT61
Med Sci Monit, 2004; 10(4): MT53-63
Gianpiero T et al – Prolonged intracranial pressure (ICP) monitoring…
MT
the proper management procedure [7]. The presence
or absence of plateau A-waves, in our experience was a
particularly important parameter for the evaluation of
these patients. Indeed, although all of them had normal
ICP values for more than 50% of the recordings,
plateau A-waves were found in three cases, indicating a
periodic pathological increase in the ICP and the need
for surgical treatment.
Craniosynostosis
Different factors may contribute to an elevation of the
ICP in children with craniosynostosis. Apart from the
restricted skull volume, herniation of the hindbrain,
intracranial venous congestion, hydrocephalus, and
upper airways obstruction are well-documented associa-
tions particularly with the syndromic forms, and all can
be responsible of this process. Clinical and radiological
features often give little information. For this reason,
ICP monitoring can be a particularly important diag-
nostic tool. Indeed, the separation of children with an
increase in ICP from those with an exclusively cosmetic
problem is an important parameter in the definition of
the surgical indication and may help to establish the
times of single- or multiple-staged operative treatment.
A limited number of studies can be found on this issue;
moreover, differing techniques of patient selection and
the measurement and interpretation of ICP values do
not allow meaningful comparisons between them.
Thompson et al. measured ICP in a consecutive series
of 136 patients. Eighty-three of them were affected by
non-syndromic craniosynostosis and fifty-three by syn-
dromic craniosynostosis. A Camino fiberoptic subdural
device was selected for continuous ICP monitoring
(mean time of ICP monitoring: 21 h). There was a sig-
nificant difference in the prevalence of raised ICP
between the non-syndromic and syndromic groups. In
non-syndromic craniosynostosis, raised ICP was present
in 24% of the cases, compared with 52.8% in the syn-
dromic group. Among the non-syndromic children,
cases of single-suture synostosis showed a significantly
lower prevalence of raised ICP (12.9%) than cases where
more than one suture was fused (brachicephaly, multi-
ple sutures) (57.1%). Of the syndromic craniosynostoses,
Crouzon (65%) and Pfeiffer (60%) syndrome were the
most commonly associated with increased ICP. Apart
from mean ICP, plateau sleep waves were recorded; a
significant difference was found in the presence of these
waves between non-syndromic (28.2%) and syndromic
(62.2%) patients. Postoperative assessment of the ICP
was performed in 15 patients; five of them (two with
Apert syndrome, two with cloverleaf craniosynostosis,
and one with Crouzon syndrome) had persistent post-
operative elevated ICP, confirming that increased ICP
may have a multifactorial pathogenesis in children with
syndromic craniosynostosis [5,6].
Fourteen of the sixteen children with complex cran-
iosynostosis (87.5%) in our series presented abnormal
ICP values with the evidence of nocturnal plateau waves
in all cases. In particular, pathological ICP recordings
were documented in all the patients with Apert and
Crouzon syndrome, in both the children with cloverleaf
craniosynostosis, in two of the three children with
Pfeiffer syndrome, and in one of the two patients with
osteopetrosis. Post-operative ICP monitoring was effect-
ed in seven of these patients (four of the five children
with Apert syndrome and one each with a Crouzon syn-
drome, a cloverleaf craniosynostosis and osteopetrosis)
and documented a reduction of ICP values in all cases.
However, in no case was there a return of ICP to nor-
mal; nevertheless, plateau sleep waves disappeared in
only four of these children, while they were only
reduced in the remaining three cases. This finding con-
firms previous reports. Upper airways obstruction,
which is an almost constant association in syndromic
craniosynostosis, contributes to the persistence of patho-
logical ICP parameters in this kind of patient. This may
be particularly true for plateau waves which are related
with REM sleep. The restricted number of children with
non-syndromic craniosynostosis of our series does not
allow definite conclusions; however, it should be noticed
that, including the two children with brachicephaly, in
no case could we find a pathological increase in ICP.
Arachnoid cysts
The relatively frequent detection of arachnoid cysts in
apparently otherwise asymptomatic patients has empha-
sized the current lack of reliable surgical indicators in a
significant proportion of cases [24–31]. Consequently, a
conservative approach in patients, followed by means of
seriated neuroimaging and neuropsychological exami-
nations, has been advocated by several authors [26,30].
In 1980 Galassi and co-workers proposed a classification
based on the cysts size and the effectiveness of their
anatomofunctional communication with the normal sub-
arachnoid spaces, evaluated by means of metrizamide-
enhanced CT cysternography. This classification identi-
fies three main types. Type I cysts usually are biconvex
or semicircular, small in size, and confined to the anteri-
or part of the temporal fossa. These cysts exert only a
negligible mass effect because of free and rapid commu-
nication with the basal cisterns. Type II cysts tend to be
roughly triangular or quadrangular in shape and medi-
um-sized. They often have a moderate mass effect,
mostly within the anterior and middle portions of the
temporal fossa. Type II cysts fill with water-soluble con-
trast medium relatively late on CT cisternography.
Finally, Type III cysts are large, roundish or oval
lesions that occupy the middle cranial fossa entirely,
obviously compressing the adjacent nervous and vascu-
lar structures, eventually causing deformation of the
homolateral cerebral ventricle and controlateral midline
shift. These cysts may appear to be not permeable to the
contrast medium, or filled only very late because of
absent or functionally inadequate communication with
the normal subarachnoid spaces [23].
The results we obtained by prolonged ICP recording in
the series here examined appear to confirm the useful-
ness of Galassi’s classification, as the recorded ICP val-
ues tended to be within the normal range in Type I
lesions and consistently above the limit in two of the
three children with Type III cysts. Unfortunately, the
Electronic PDF security powered by ISL-science.com
This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited.
PERSONAL USE
ONLY
MT62
Med Sci Monit, 2004; 10(4): MT53-63
Diagnostics and Medical Technology
examination proved less discriminating in Type II cysts,
where normal and abnormally elevated ICP values
could be observed with similar incidence. With the limit
of the relatively small number of patients, prolonged
recording of ICP appears to be particularly important
in ruling out the need to relieve the pressure exerted by
the lesion in patients with Type I cysts, even in cases
presenting with unspecific clinical manifestations, such
as transient headache or seizure disorders. Similarly,
this is confirmed by the results of this study. The detec-
tion of one patient with a Type III cyst and normal ICP
recordings confirms that an increase in ICP is not
always at the base of a severe distortion or compression
of neurological structures revealed by neuroimaging
studies.
In cases of Type II temporal arachnoid cysts, prolonged
ICP recording may be particularly useful for the surgi-
cal indication, as it may allow to differentiate those
patients who may benefit from the surgical excision of
the cystic lesion or diversion of its content, because of
evidence of increased intracranial pressure, from those
cases where a wait-and-see policy could be adopted, in
which the pressure of the cyst does not appear to impair
CSF dynamics.
Future developments of the present study may come
from a comparison between ICP findings and cerebral
perfusion examinations results. In 2001, in fact, Sgouros
and Chapman demonstrated a reduction in cerebral
blood flow not associated with signs or symptoms of
increased ICP in three children with Sylvian arachnoid
cysts who were investigated by means of SPECT scans.
In all cases, surgical excision of the cyst resulted in nor-
malization of cerebral blood flow following a partial re-
expansion of the temporal lobe [31].
C
ONCLUSIONS
The present study confirms that prolonged ICP moni-
toring is an important diagnostic tool in non-traumatic
pediatric neurosurgical diseases. In our experience, it
enabled a more correct surgical indication in children
with hydrocephalus and arachnoid cysts. In children
with craniosynostosis it was useful in defining the func-
tional role of the disease and to establish the times of
the operative treatment.
R
EFERENCES
:
1. Eide PK: Quantitative analysis of continuous intracranial pressure
recordings in symptomatic patients with extracranial shunts.
J Neurol Neurosurg Psychiatry, 2003; 74(2): 231-37
2. Eide PK, Helseth E, Due-Tonnessen B, Lundar T. Assessment
of continuous intracranial pressure recordings in childhood cran-
iosynostosis. Pediatr Neurosurg, 2002; 37(6): 310-20
3. Eide PK, Due-Tonnessen B, Helseth E, Lundar T. Differences
in quantitative characteristics of intracranial pressure in hydro-
cephalic children treated surgically or conservatively. Pediatr
Neurosurg, 2002; 36(6): 304-13
4. Eide PK, Helseth E, Due-Tonnessen B, Lundar T: Changes
in intracranial pressure after calvarial expansion surgery in chil-
dren with slit ventricle syndrome. Pediatr Neurosurg, 2001; 35(4):
195-204
5. Thompson DNP, Harkness W, Jones B et al: Subdural intracranial
pressure monitoring in craniosynostosis: its role in surgical man-
agement. Child’s Nerv Syst, 1995; 11: 269-75
6. Thompson DNP, Malcolm GP, Jones BM et al: Intracranial pres-
sure in single suture craniosynostosis. Pediatr Neurosurg, 1995; 22:
235-40
7. Rekate HL. Classification of Slit-Ventricle-Syndromes using intracra-
nial pressure monitoring. Pediatr Neurosurg, 1993; 19: 15-20
8. Pople IK, Muhlbauer MS, Sanford RA, Kirk E: Results and compli-
cations of intracranial pressure monitoring in 303 children. Pediatr
Neurosurg, 1995; 23: 64-67
9. Fouyas IP, Casey ATH, Thompson D et al: Use of intracranial pres-
sure monitoring in the management of childhood hydrocephalus
and shunt-related problems. Neurosurgery, 1996; 38(4): 726-32
10. Massager N, Wayenberg JL, Raftopoulos C et al: Anterior
fontanelle pressure monitoring for the evaluation of asymptomatic
infants with increased head growth rate. Child’s Nerv Syst, 1996;
12: 38-42
11. Gambardella G, Zaccone C, Cardia E, Tomasello F. Intracranial
pressure monitoring in children: comparison of external ventricu-
lar device with the fiberoptic system. Child’s Nerv Syst, 1993; 9:
470-73
12. Jensen RL, Hahn YS, Ciro E: Risk factors of intracranial pressure
monitoring in children with fiberoptic devices: a critical review.
Surg Neurol, 1997; 47: 16-22
13. Minns RA: Intracranial pressure monitoring. Archives Dis Child,
1984; 59: 486-88
14. Reid A, Marchbanks RJ, Bateman DE et al: Mean intracranial pres-
sure monitoring by a non-invasive audiological technique: a pilot
study. J Neurol Neurosurg Psych, 1989; 52: 610-12
15. Munch E, Weigel R, Schmiedek P, Schurer L: The Camino
intracranial pressure device in clinical practice: reliability, handling
characteristics and complications. Acta Neurochir (Wien), 1998;
140(11): 1113-20
16. Morgalla MH, Cuno M, Mettenleiter H et al: ICP monitoring wih
a re-usable transducer: experimental and clinical evaluation of the
Gaeltec ICT/b pressure probe. Acta Neurochir (Wien), 1997; 139:
569-73
17. Penson RP, Allen R. Intracranial pressure monitoring by time
domain analysis. J R Soc Health, 1998; 118(5): 289-94
18. Morgalla MH, Stuum F, Hesse G: A computer-based method for
continuous single pulse analysis of intracranial pressure waves.
J Neurol Sci, 1999; 168(2): 90-95
19. Lemarie JJ, Boire JY, Chazal J, Irthum B: A computer software
for frequential analysis of slow intracranial pressure waves. Comput
Methods Programs Biomed, 1994; 42(1): 1-14
20. Gaab MR, Ungersbock K, Hufenbeck B: Evaluation of ICP by com-
puterized bedside monitoring. Neurol Res, 1986; 8(1): 44-52
21. Allen R: Time series methods in the monitoring of intracranial
pressure. Part 2: comparative study and initial assessment. J Bio-
med Engl, 1983; 5(2): 103-9
22. Steinmeier R, Hoffman RP, Bauhuf C et al: Continuous cerebral
autoregulation monitoring by cross-correlation analysis. J Neuro-
trauma 2002; 19(10): 1127-38
23. Galassi E, Tognetti F, Gaist G et al: CT scan and metrizamide CT
cisternography in arachnoid cysts of the middle cranial fossa: classi-
fication and pathophysiological aspects. Surg Neurol, 1982; 17(5):
363-69
24. Arai H, Sato K, WachiA et al: Arachnoid cyst of the middle cranial
fossa: experience with 77 patients who were treated with cystoperi-
toneal shunting. Neurosurgery, 1996; 39(6): 1108-12
25. Artico M, Cervani L, Salvati M et al: Supratentorial arachnoid cysts:
clinical and therapeutic remarks on 46 cases. Acta Neurochir, 1995;
132: 75-78
26. Daneyemez M, Gezen F, Akboru M et al: Presentation and manage-
ment of supratentorial and infratentorial arachnoid cysts. Review
of 25 cases. J Neurosurg Sci, 1999; 43(2): 115-23
27. Di Rocco C: Arachnoid cysts. In Youmans JR ed. Neurological
Surgery. Fourth Edition. Vol. 2, Part VI, Chapter 39, Philadelphia:
WB Saunders, 1996: 967-94
28. Fewel ME, Levy ML, McComb JG: Surgical treatment of 95 chil-
dren with 102 intracranial arachnoid cysts. Pediatr Neurosurg,
1996; 25: 165-73
Electronic PDF security powered by ISL-science.com
This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited.

PERSONAL USE
ONLY
MT63
Med Sci Monit, 2004; 10(4): MT53-63
Gianpiero T et al – Prolonged intracranial pressure (ICP) monitoring…
MT
29. Sommer IEC, Smit LME: Congenital supratentorial arachnoidal
and giant cysts in children: a clinical study with arguments for
a conservative approach. Childs Nerv Syst, 1997; 13(1): 8-12
30. Wester K: Documented growth of a temporal arachnoid cyst.
J Neurol Neurosurg Psychiatry, 2000; 69: 699-700
31. Sgouros S, Chapman S: Congenital middle fossa arachnoid cysts
may cause global brain ischemia: a study with 99 Tc-hexamethyl
propylene amineoxime Single Photon Emission Computerized
Tomography scans. Pediatr Neurosurg, 2001; 35: 188-194
Electronic PDF security powered by ISL-science.com
This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited.
PERSONAL USE
ONLY
Index
Copernicus
integrates
www.
IndexCopernicus
.com
Index Copernicus
Global Scientific Information Systems
for Scientists by Scientists
Index
Copernicus
integrates
IC Virtual Research Groups [VRG]
Web-based complete research
environment which enables researchers
to work on one project from distant
locations. VRG provides:
customizable and individually
self-tailored electronic research
protocols and data capture tools,
statistical analysis and report
creation tools,
profiled information on literature,
publications, grants and patents
related to the research project,
administration tools.
IC Scientists
Effective search tool for
collaborators worldwide.
Provides easy global
networking for scientists.
C.V.'s and dossiers on selected
scientists available. Increase
your professional visibility.
IC Patents
Provides information on patent
registration process, patent offices
and other legal issues. Provides
links to companies that may want
to license or purchase a patent.
IC Lab & Clinical Trial Register
Provides list of on-going laboratory
or clinical trials, including
research summaries and calls for
co-investigators.
IC Grant Awareness
Need grant assistance?
Step-by-step information on
how to apply for a grant. Provides
a list of grant institutions and
their requirements.
IC Journal Master List
Scientific literature database,
including abstracts, full text,
and journal ranking.
Instructions for authors
available from selected journals.
IC Conferences
Effective search tool for
worldwide medical conferences
and local meetings.
Index
Copernicus
integrates
EVALUATION & BENCHMARKING
PROFILED INFORMATION
NETWORKING & COOPERATION
VIRTUAL RESEARCH GROUPS
GRANTS
PATENTS
CLINICAL TRIALS
JOBS
STRATEGIC & FINANCIAL DECISIONS
EVALUATION & BENCHMARKING
PROFILED INFORMATION
NETWORKING & COOPERATION
VIRTUAL RESEARCH GROUPS
GRANTS
PATENTS
CLINICAL TRIALS
JOBS
STRATEGIC & FINANCIAL DECISIONS
Electronic PDF security powered by ISL-science.com
This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited. This copy is for personal use only - distribution prohibited.
Wyszukiwarka
Podobne podstrony:
raised intracranial pressure
Blood Pressure in Intracerebral Hemorrhage
tire pressure monitor reset
Monitoring ZM Pierzchala
Monitory
w 3 monitorowanie podróży
Pressure%20Cem[1]
Proces wdrazania i monitoringu strategii rozwoju
5 Terapia monitorowana
BHP przy obsludze monitorow ekranowych
Monitoring zrwnowaonej turystyki
monitoring gleb
Monitorowanie pacjentów w OIT
7 [ Biofizyczne metody monitorowania ciąży ]
monitoring wod
W2 , inform locyjne,PLANOWANIE i monitorowanie
monitoring
więcej podobnych podstron