Systemic diseases of old age
Ophthalmic manifestations Part 2
ABDO has awarded this article
2 CET credits (GD).
The College of Optometrists has
awarded this article 2 CET credits.
There are 12 MCQs with
a pass mark of 60%.
29
|
November 28
|
2003 OT
GCA and AAION
Giant cell arteritis (GCA) is a disease of the
elderly. The annual incidence rate for the
disease is estimated to be between 15 to 30
cases per 100,000 in people aged over 50
years. However, the rate for ages between 60
and 69 years increases to 33 per 100,000, and
over the age of 80 is 844 cases per 100,000.
The female:male ratio is approximately 3:1 to
4:1.
The precise aetiology of cranial arteritis is
not clearly understood. The significantly
higher frequency found in Caucasians
compared to Afro-Caribbeans, the reports of
the disease in immediate relatives, and the
association with human leukocyte antigen
HLA-DR1, suggest that a genetic
predisposition may exist.
The main ocular finding of GCA is the
so-called arteritic anterior ischaemic optic
neuropathy (AAION). Arteritic is one of the
two main forms of anterior ischaemic optic
neuropathy. The second is the non-arteritic
anterior ischaemic optic neuropathy
Continuing Professional Development
(NAAION) which is not associated with GCA.
Patients with NAAION are generally healthy
or only have associated hypertension or
diabetes mellitus.
Ophthalmic manifestations
Anterior ischaemic optic neuropathy (AION),
in general, presents with rapid onset of
painless, unilateral visual loss manifests as
decreased visual acuity, visual field
impairment, or both.
In approximately 5% of cases, AION is
categorised as arteritic, associated with
temporal arteritis. Visual loss with AAION
tends to be more profound than with
NAAION. Seventy percent of patients have
visual acuity of 6/60 or worse, and levels of
finger counting to no light perception are
common. In some cases, the abrupt visual
loss is preceded by transient visual
disturbances, similar to that of carotid artery
disease.
Typically, AAION presents in older
patients (mean age: 70 years) as compared to
the non-arteritic form of the disease, which
occurs in relatively younger patients (mean
age: 60 years). A relative afferent pupillary
defect (RAPD) is invariably present with
monocular optic neuropathy. An altitudinal
field defect is the most common pattern of
visual field impairment, but generalised
depression, broad arcuate scotomas, and
centrocaecal scotomas are also seen. Visual
field defects in patients with AAION are more
severe than those in patients with NAAION.
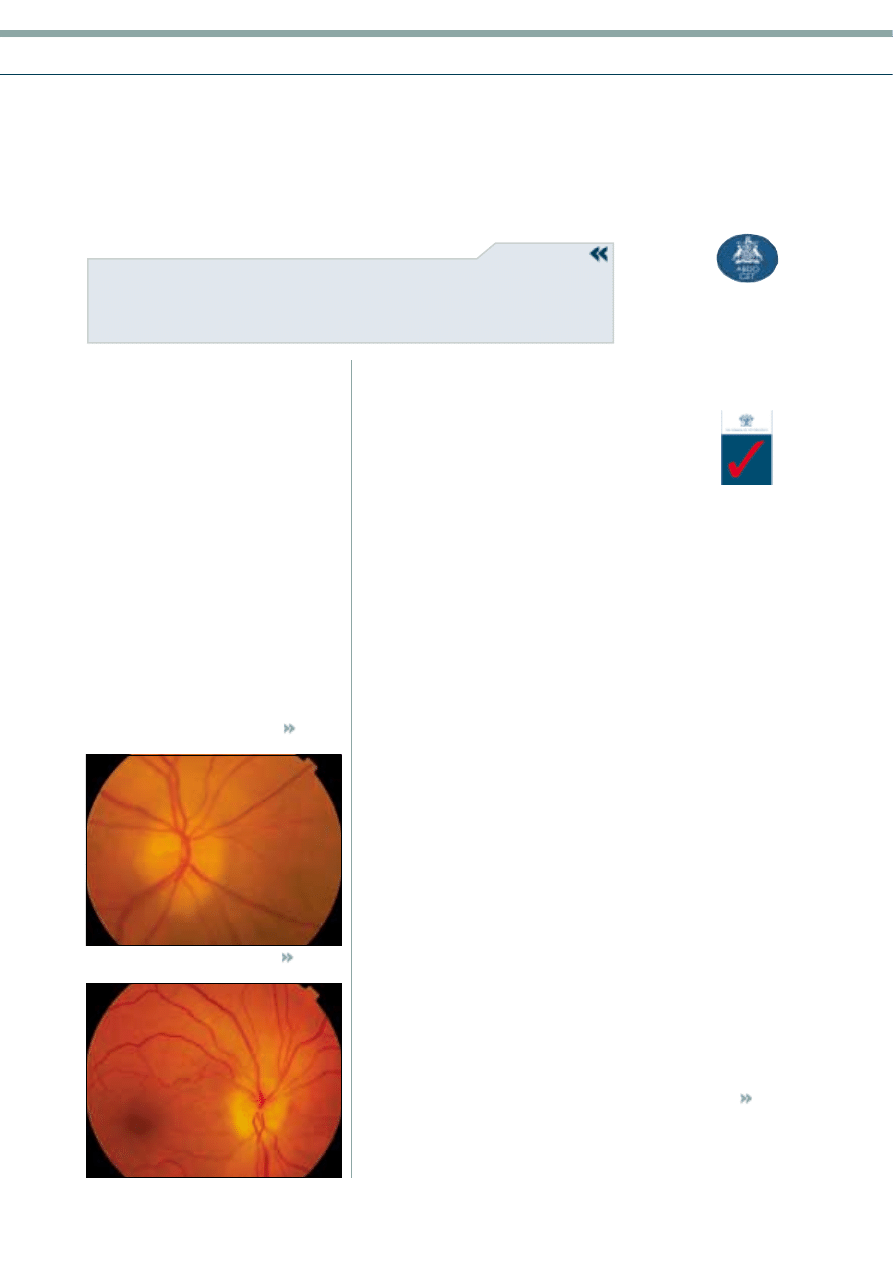
The optic disc is oedematous at onset,
characterised by a milk-pale oedema that
sometimes extends into the peripapillary
retina (Figure 1). Pallor is associated with
oedema of the optic disc more frequently in
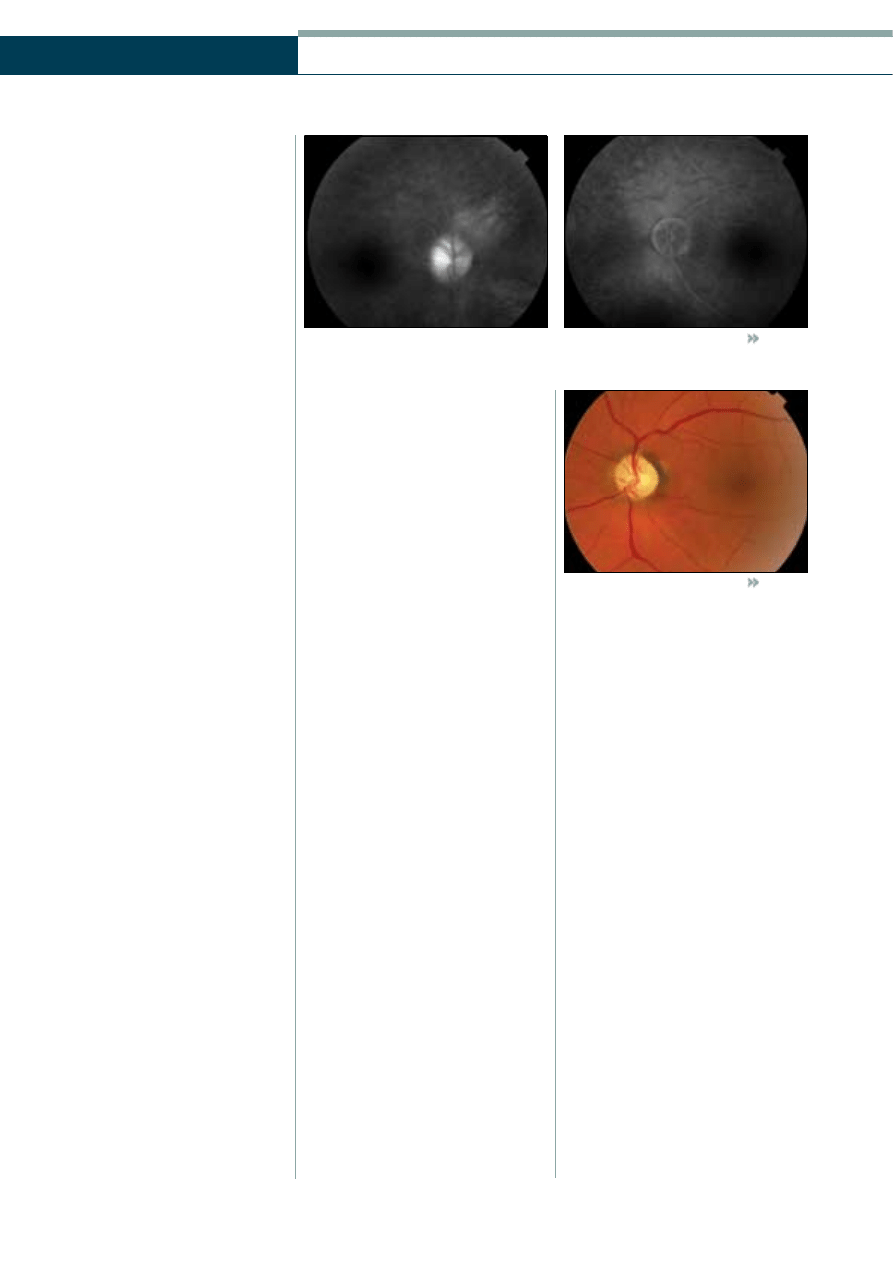
AAION than in the non-arteritic form. Focal
or diffuse surface telangiectasia is not unusual
and may be pronounced (Figure 2). In many
cases, flame-shaped haemorrhages and
cotton-wool spots are located adjacent to the
disc, while the peripapillary retinal arterioles
are frequently narrowed.
Choroidal ischaemia may be associated
with the optic neuropathy. It may produce
peripapillary pallor and oedema deep in the
retina, or it may occur with no optic disc
involvement. Central retinal artery occlusion
with a cherry-red spot may also occur.
The disc of the fellow eye in most cases is
of normal diameter, with a normal
About the author
Panagiotis Karadimas is a
Consultant Ophthalmic Surgeon in
the 1st Department of
Ophthalmology, Henry Dunant
Hospital, Athens, Greece.
T
he second part of this article, describing the most common
systemic disorders associated with ophthalmic manifestations
in the older population, covers giant cell arteritis, carotid artery
disease and ocular ischaemic syndrome, strokes and
paraneoplastic syndromes.
Panagiotis Karadimas MD
Module 5 Part 12 of
the ageing eye series
SPECIALISTS IN EYECARE
Sponsored by
a
Figure 1
Optic disc oedema in a patient with AAION
Figure 2
Oedematous disc with a surface telangiectasia
Continuing Professional Development
Panagiotis Karadimas MD
30
|
November 28
|
2003 OT
SPECIALISTS IN EYECARE
a
Sponsored by
physiological cup. This is in contrast to the
optic discs of patients with NAAION,
which are smaller and have a smaller
cup-to-disc ratio. So, a normal or large cup
in the fellow eye of a patient with AION
must raise the suspicion of the arteritic
form of the disease.
Fluorescein angiography demonstrates
delayed filling of the optic disc and
choroid. The degree of the delay of
choroidal filling has been depicted as a
characteristic of AAION, and has been
suggested as one useful criterion by which
to differentiate AAION from NAAION.
Delayed completion of choroidal
fluorescein filling, that averages 30 to 69
seconds, has been reported in AAION,
compared to a mean of five to 13 seconds
in NAAION. At the late phases of the
angiogram, the oedematous optic disc
demonstrates diffuse hyperfluorescence
(Figure 3).
Patients who have the arteritic form
usually note other symptoms of GCA. The
most common are headache, jaw
claudication, and temporal artery or scalp
tenderness. Malaise, anorexia, weight loss,
fever, proximal joint arthralgia, and
myalgia also are common. However, GCA
occasionally presents with visual loss in the
absence of overt systemic symptoms; this
type of the disease is called occult GCA.
Pathogenesis
AAION originates from vasculitis of the
short posterior ciliary arteries, which results
in optic nerve head infarction. Human
autopsy studies of acute AAION
demonstrate ischaemic necrosis of the
prelaminar, laminar and retrolaminar
portions of the optic nerve and infiltration
of the short posterior ciliary arteries by
chronic inflammatory cells. In some cases,
segments of these vessels have been
occluded by inflammatory thickening and
thrombus.
Diagnosis
The most important early step in the
management of AION is to distinguish the
arteritic from the non-arteritic form. It is
critical and a true ophthalmic emergency to
diagnose the arteritic AION, because
prompt steroid therapy may restore some
degree of vision in the affected eye, prevent
a similar visual deficit in the other eye, and
potentially improve long-term systemic
morbidity and mortality.
Measurement of the erythrocyte
sedimentation rate (ESR) is considered the
most consistently helpful laboratory test in
the confirmation of diagnosis, and is the
standard first test ordered. Active GCA
usually is associated with an elevation of
ESR to 70-120mm/h, and this finding
suggests the arteritic form of the disease.
The following rule for calculating the
maximal normal ESR at a given age, is
usually used: in men (age in years)/2; in
women (age in years +10)/2. However, the
test has considerable limitations and
normal measurements are found in about
16% of biopsy-proved cases of GCA.
Conversely, abnormally high readings
usually occur with increasing age and with
other diseases, most commonly occult
malignancy, other inflammatory disease
and diabetes.
Levels of serum C-reactive protein may
be more specific and may aid in differential
diagnosis. Some authors have stated that
C-reactive protein is elevated along with
ESR in patients with GCA, but not in
control subjects with an elevated ESR
without GCA. This suggests that C-reactive
protein is extremely useful for both
diagnosis of the disease and monitoring of
the therapy. However, it should be noted
that not all authorities share this view.
In any case of AION in which a clinical
suspicion of arteritis exists based on age,
associated systemic symptoms, the severity
of visual loss and an elevated ESR, it is
recommended to confirm the diagnosis of
GCA by a superficial temporal artery
biopsy. Positive biopsy (characterised
histologically by intimal thickening,
internal limiting lamina fragmentation and
chronic inflammatory infiltration with
giant cells) provides support for long-term
systemic corticosteroid therapy. A negative
biopsy, however, does not exclude GCA.
There are two reasons for this. First,
because arterial involvement may be
discontinuous (the so-called ‘skip lesions’)
and, second because temporal artery
inflammation may be solely ipsilateral. So,
in a given temporal artery biopsy, the site
of inflammation may be missed producing
a false negative result. In the case of a
negative initial biopsy, consideration
should be given to contralateral biopsy in
cases with high clinical suspicion of GCA.
Course
The natural history of AAION is progressive
visual loss and finally the development of
optic atrophy (Figure 4). However, the
most important event is the involvement of
the second eye. Without treatment,
involvement of the fellow eye occurs in
54-95% of cases, typically within four
months. The major goal of therapy in
AAION is to prevent visual loss in the
fellow eye. Corticosteroid therapy reduces
the risk to 13%.
Treatment
In any patient with the suspicion of
AAION, systemic corticosteroid therapy at
high doses (e.g. oral prednisone at
80-100mg/day or intravenous
methylprednisolone at 250mg every six
hours) should be instituted immediately on
presumed diagnosis. Therapy should not be
delayed for results of ESR, other laboratory
investigations or biopsy. Symptomatic
response to steroids, excluding vision, may
be dramatic within 24 hours, with relief of
headache and malaise.
As already stressed, the main goal of
therapy in AAION is to prevent visual loss
in the second eye. Prognosis for visual
recovery in the affected eye as a result of
the treatment is generally considered poor.
However, some reports suggest that a
15-34% improvement rate may occur,
especially if intravenous instead of oral
therapy is utilised. On the other hand,
worsening of vision, in spite of therapy, has
also been reported in 9-17% of cases.
For the elderly patient, hospitalisation
may be justified to monitor the side effects
of large steroid doses on blood glucose,
serum potassium and blood pressure. Most
patients will experience side effects of
steroid medication. Indeed, severe events
like cardiac arrhythmia, anaphylaxis, and
even sudden death, have been reported.
Prolonged steroid therapy should be
adjusted according to the symptomatic
Figure 4
Optic atrophy following AAION
Figure 3
Fluorescein angiography demonstrating diffuse hyperfluoresecnce (hot disc) in a patient with
ischaemic optic neuropathy (A). Compare with the normal fellow eye (B)
A
B
gradual, over a period of weeks to months,
but it can occur abruptly. In the setting of
rapid visual loss, frequently a cherry-red
spot is seen in the fundus. Approximately
5% of patients have a previous history of
amaurosis fugax.
The severity of the visual loss is variable.
About one third of affected eyes present
with a visual acuity of 6/12 or better, one
third ranges from 6/15 to 6/120 while
in the remaining third, visual acuity is
counting fingers or worse. The absence
of light perception is uncommon at
presentation, but it may develop as sequela
of severe posterior segment ischaemia and
neovascular glaucoma.
An intermittent dull aching pain over
the eye or brow is reported by up to 40%
of patients. The pain is the result of either
ischaemia of the globe or elevated
intraocular pressure (IOP) caused by
neovascular glaucoma. The pain associated
with ocular ischaemic syndrome is
sometimes called ‘ocular angina’.
Anterior segment
Anterior segment findings in ocular
ischaemic syndrome are common.
Neovascularisation of the iris is the most
prominent feature and it is encountered in
approximately two thirds of eyes that have
ocular ischaemic syndrome at the time of
initial examination. In severe cases,
ectropion uvea may develop. Iris
neovascularisation in the eye of a
non-diabetic, with no evidence of venous
occlusive disease or other predisposing
cause, must arise the suspicion of ocular
ischaemic syndrome.
Neovascular glaucoma, defined as
neovascularisation of the iris and an IOP
greater than 22mmHg, is seen in only half
of the ocular ischaemic patients who
have neovascularisation of the iris.
Some patients, despite having
neovascularisation of the iris and complete
closure of the anterior chamber angle with
fibrovascular tissue, have IOPs in the
normal range. This phenomenon is
considered a result of impaired ciliary body
perfusion and decreased aqueous
production as a consequence of carotid
stenosis.
Anterior uveitis is present in 20% of eyes
that have ocular ischaemic syndrome and it
is generally mild. Flare is a more
prominent feature than the cellular
response, while keratic precipitates are seen
infrequently. In patients over 50 years of
age who have new onset anterior uveitis,
the possibility of ocular ischaemic
syndrome should be considered.
Cataracts may occur in the end stages of
ocular ischaemic syndrome, but these are
not usually a prominent feature at earlier
stages.
Posterior segment
Numerous signs of the disease are present
at the posterior segment examination, as a
31
|
November 28
|
2003 OT
Continuing Professional Development
response and normalisation of the ESR. A
high oral dosage is often maintained for
approximately four to eight weeks, and
then it is tapered as long as the patient
remains free of symptoms and the ESR is
below 40mm/hr. Complications of
prolonged steroid usage are well known
and are not limited to gastric ulcers,
hyperglycaemia, osteoporosis and
recrudescence of tuberculosis.
Corticosteroids in this age group can
produce severe and rapid proximal
myopathy, myalgia and weakness, which
may be mistakenly diagnosed as persisting
or deteriorating symptomatology of GCA,
suggesting that the dosage should be
increased. In general, after the initial
presentation and initiation of therapy, the
risk of delayed visual loss should be
compared to the risks that prolonged use of
steroids represents to the general health. As
an alternative to corticosteroid therapy, other
immunosupressant agents may be used.
Ocular ischaemic syndrome
and carotid artery disease
Ocular ischaemic syndrome is an
ophthalmic condition with variable signs
and symptoms which result from chronic
ocular hypoperfusion, usually secondary to
severe carotid artery obstruction. Forty
percent of patients die within five years of
diagnosis of ocular ischaemic syndrome
which reflects the severity of the systemic
vascular disease.
Epidemiology and pathogenesis
Ocular ischaemic syndrome is a disease of
the elderly. Its mean age of presentation is
65 years and generally the condition does
not develop before 50 years of age. The
male:female ratio is 2:1, which reflects the
higher incidence of atherosclerotic
cardiovascular disease in men. No racial
predilection exists. Bilateral involvement
occurs in approximately 20% of cases. The
incidence of ocular ischaemic syndrome is
not known precisely, but it is estimated to
be seven to eight cases per million
population annually. Approximately 5% of
patients who have haemodynamically
significant carotid artery disease develop
ocular ischaemic syndrome.
The pathogenetic cause of the syndrome
is the chronic decreased arterial inflow.
However, the period and extent of the
impaired blood flow necessary to develop
this syndrome is not clear. Using a colour
Doppler imaging, reversal of ophthalmic
artery flow, decreased peak systolic flow
velocities of the central retinal artery, and
posterior ciliary artery hypoperfusion have
all been demonstrated.
Ophthalmic manifestations
Symptoms
Loss of vision is present in over 90% of
affected patients at the time of
presentation. The visual loss is usually
If you are GOC registered, you can
now answer the questions on-line
at
w
ww
ww
w..oottccppdd..ccoo..uukk
. Enter your
GOC number and surname to log
onto the system.
CPD online
Select
01-
for optometrist
or
D-
for dispensing optician
Select the examination you want
to enter from those available. It
is important that you choose the
right one and do not enter your
answers into any other available
examinations running at the same
time as you will not be able to go
back to try again. Any errors
made by participants cannot be
recalled.
Enter your answers, and an
optional email address if you want
email notification of your results.
Check your name is correct and
press the ‘send answers’ button.
The next screen will show your
percentage and any credits
gained. This will also be emailed
to you if you entered your email
address earlier. You do not have
to do anything else, apart from
logging out as these results will
be sent to the accreditation
bodies in due course.
SPECIALISTS IN EYECARE
a
Sponsored by
Note:
Netscape
Navigator
5
and
Internet
E
xplorer
5
or
more
recent
is
recommended.
Continuing Professional Development
32
|
November 28
|
2003 OT
SPECIALISTS IN EYECARE
a
Sponsored by
Panagiotis Karadimas MD
result of vascular system involvement.
In eyes with ocular ischaemic syndrome,
retinal arterial narrowing (associated with
areas of focal constriction) is present.
However, it may be difficult to distinguish
these changes from the narrowed vessels
commonly seen in the elderly.
Retinal veins are frequently dilated and
may additionally have significant beading,
similar to eyes that have preproliferative or
proliferative diabetic retinopathy. On the
other hand, retinal venous tortuosity is not
a prominent feature, in contrast to eyes
that have suffered central retinal venous
occlusion. This is a helpful feature in the
differential diagnosis of these two
conditions.
Retinal haemorrhages are seen in 80%
of eyes. In most cases, haemorrhages
have a dot and blot configuration and are
located in the fundus mid-periphery.
Microaneurysms may also be seen in the
same areas. Neovascularisation of the optic
disc occurs in over one third of patients,
while retinal neovascularisation is present
in 8% of affected eyes.
A cherry-red spot is seen in 12% of eyes
that display ocular ischaemic syndrome at
presentation. It is a result of high IOP from
neovascular glaucoma, which exceeds the
central retinal artery’s perfusion pressure.
Cotton-wool spots and spontaneous
pulsations of the retinal arteries are each
present in about 5% of the eyes. When not
present spontaneously, retinal arterial
pulsations can be elicited easily by
minimal pressure on the globe, because
of the severe diminution in ocular
perfusion pressure. In contrast, eyes with
non-ischaemic central retinal venous
occlusion require a normal amount of
digital pressure to induce retinal arterial
pulsations.
Diagnosis
Fluorescein angiography is very useful in
establishing the diagnosis of ocular
ischaemic syndrome. It demonstrates
delayed arm-to-choroid and arm-to-retina
circulation times. In addition,
demonstration of a well-demarcated
leading edge of fluorescein dye within a
retinal artery is very unusual for a normal
eye and suggests ocular hypoperfusion.
Patchy choroidal filling, lasting more than
five seconds is seen in about 60% of eyes
with ocular ischaemic syndrome.
Other findings on fluorescein
angiography include an increased
arteriovenous transit time (that exceeds 11
seconds in approximately 95% of affected
eyes), staining of the retinal vessels,
macular oedema, and retinal capillary non-
perfusion. Late staining of retinal vessels,
which is more prominent in arterioles than
in venules, is present in about 85% of
cases, probably as a consequence of
endothelial cell ischaemia.
Electroretinography often demonstrates
a decrease in both the a and b-waves in
eyes that are affected by ocular ischaemic
syndrome, corresponding to outer and
inner retinal ischaemia, respectively.
Colour Doppler imaging is an excellent
non-invasive method to assess the velocity
of blood flow in the retrobulbar
circulation. It demonstrates diminution of
blood flow velocities in the central retinal
artery, choroidal vessels, and ophthalmic
artery and reversal of blood flow in the
ophthalmic artery. Colour Doppler imaging
may be used for the simultaneous
assessment of the carotid arteries.
Carotid non-invasive tests, such as
ultrasonography and duplex scanning, are
approximately 90% accurate in detecting a
carotid artery stenosis of 50% or greater
and can be used for screening in suspected
cases. Digital subtraction angiography and
magnetic resonance angiography may be
required as confirmatory examinations.
By these means, a carotid artery stenosis
greater than 90% is usually detected in eyes
with ocular ischaemic syndrome.
Systemic associations
The atherosclerosis that affects the carotid
artery sufficiently to cause ocular ischaemic
syndrome is generally widespread.
Of patients who have ocular ischaemic
syndrome, 50% show evidence of
ischaemic heart disease and 25% have a
history of previous cerebrovascular
accidents.
Additional risk factors for atherosclerosis
are commonly found in these patients,
such as systemic hypertension (which is
found in two thirds of patients who have
ocular ischaemic syndrome) and diabetes
mellitus (which is found in more than 50%
of these patients).
A five-year mortality rate in 40% of
patients who have ocular ischaemic
syndrome reflects the severity of their
systemic vascular disease. The main cause
of death in these patients is ischaemic heart
disease, and the second most common
cause is stroke.
Treatment, course and outcome
The natural course of eyes that have
full-blown ocular ischaemic syndrome is
poor. Surgical treatment of carotid stenosis
may help to maintain or improve vision in
eyes that have this syndrome. Stabilisation
or improvement of vision has been
reported in about 25% of eyes after surgical
treatment of carotid stenosis (carotid
endarterectomy). Occasionally, in the
sub-group of eyes with ciliary body
hypoperfusion, complete angle closure, and
normal IOP, carotid endarterectomy may
result in severe glaucoma immediately after
surgery.
Recent studies of the outcome of
patients after carotid endarterectomy also
need to be considered. In patients who
have had a recent retinal transient
ischaemic attack, a hemispheric transient
ischaemic attack, or a non-disabling stroke
and had carotid stenosis of 70-99%, the
North American Symptomatic Carotid
Endarterectomy Trial Collaborators found
that the two-year stroke rate was 9% in
patients who had endarterectomy as
compared with 26% in those managed
with antiplatelet therapy. However, the
immediate post-operative rate of severe
stroke or death was 2.1% in the patients
who underwent surgery versus 0.9% for the
antiplatelet group. It should be noted that
surgeons who participated in the trial were
selected carefully for low rates of
postsurgical complications. Thus, the
decision to undergo a carotid
endarterectomy is a difficult one.
In patients who have iris
neovascularisation, in which the anterior
chamber angle is open, panretinal
photocoagulation may induce regression of
the rubeosis. Unfortunately, the regression
is not as prominent as that seen in patients
who have rubeosis iridis after central retinal
vein occlusion. Elevated IOP from
neovascular glaucoma may require
cyclodestructive therapies, or filtering
procedures.
Strokes
The typical ischaemic stroke presents with
the abrupt onset of a focal neurologic
deficit. The most reliable indicator of
impending stroke is a transient ischaemic
attack (TIA). Vascular sites that may
produce TIAs and stroke are: carotid and
ophthalmic artery; middle cerebral artery;
posterior cerebral (terminal basilar) artery;
and basilar artery.
Carotid and ophthalmic artery
Carotid and ophthalmic artery TIAs most
commonly manifest as amaurosis fugax
caused by hypoperfusion of the retina. The
patient is at risk of permanent visual loss,
mainly as a result of occlusion of the
central retinal artery, which represents the
equivalent of an ‘ocular stroke’.
Severe chronic carotid artery stenosis
may lead to hypoperfusion of the optic
nerve and retina, causing the ocular
ischaemic syndrome.
Middle cerebral artery
The second major ocular sign of carotid
occlusive disease (in addition to amaurosis
fugax) is partial or complete contralateral
homonymous hemianopia, often the result
of hypoperfusion in the middle cerebral
artery (MCA). However, posterior cerebral
occlusion is by far the most common cause
of homonymous hemianopia. Cerebral
TIAs tend to be longer in duration than
ocular TIAs. Ischaemic reversible neurologic
deficits may also occur.
Ischaemia of the cortical and deep
cerebral branches of the left MCA may
produce isolated motor aphasia and often
contralateral hemiparesis and sensory loss.
When TIA of the MCA are on the right
(non-dominant side) transient motor or
sensory loss is produced on the left,
without aphasia.
The MCA stroke often fluctuates and
33
|
November 28
|
2003 OT
Continuing Professional Development
SPECIALISTS IN EYECARE
a
Sponsored by
progresses gradually. Anterior MCA branch
occlusion produces hemiparesis in the leg
and loss of sensation without hemianopia.
Posterior MCA branch occlusion produces
incomplete incongruous homonymous
hemianopia, without macular sparing. Left
MCA stroke produces aphasia, in contrast
to right-sided lesions that produce
contralateral hemispatial neglect and
supranuclear horizontal gaze paresis to the
side of the lesion.
Homonymous hemianopia is the major
neuro-ophthalmic sign of an MCA stroke
and it may be the only sign. It is the result
of damage to the optic radiation. The
prognosis in MCA stroke is poor and, until
recently, no known treatment existed.
However, specialised stroke centres now use
a urokinase anticoagulation protocol; if
treatment can be instituted within a few
hours, the prognosis is much better.
Posterior cerebral artery
Transient visual symptoms due to posterior
cerebral artery (PCA) hypoperfusion are
encountered less commonly and are less
dramatic to the patient than amaurosis
fugax of carotid origin. Isolated visual
migraine may present in a similar way and
must be differentiated from that of an
impending stroke.
Clinically, visual migraine is very
common, in contrast to occipital TIA,
though each can mimic the aura of classic
migraine. True vascular TIAs that involve
the occipital lobes are usually sudden in
onset with a complete or incomplete
homonymous hemianopia. These events
may be accompanied by basilar vertebral
symptoms, such as unsteadiness, dysarthria
(motor speech disorder), facial numbness
or weakness.
Isolated homonymous hemianopias are
usually due to vascular occlusion of the
PCA and, therefore, are the main features of
occipital stroke. Infarction of the PCA is the
result of an embolism in the vast majority
of cases; rarely is it caused by
atherosclerosis. Usually, PCA strokes occur
suddenly without preceding symptoms.
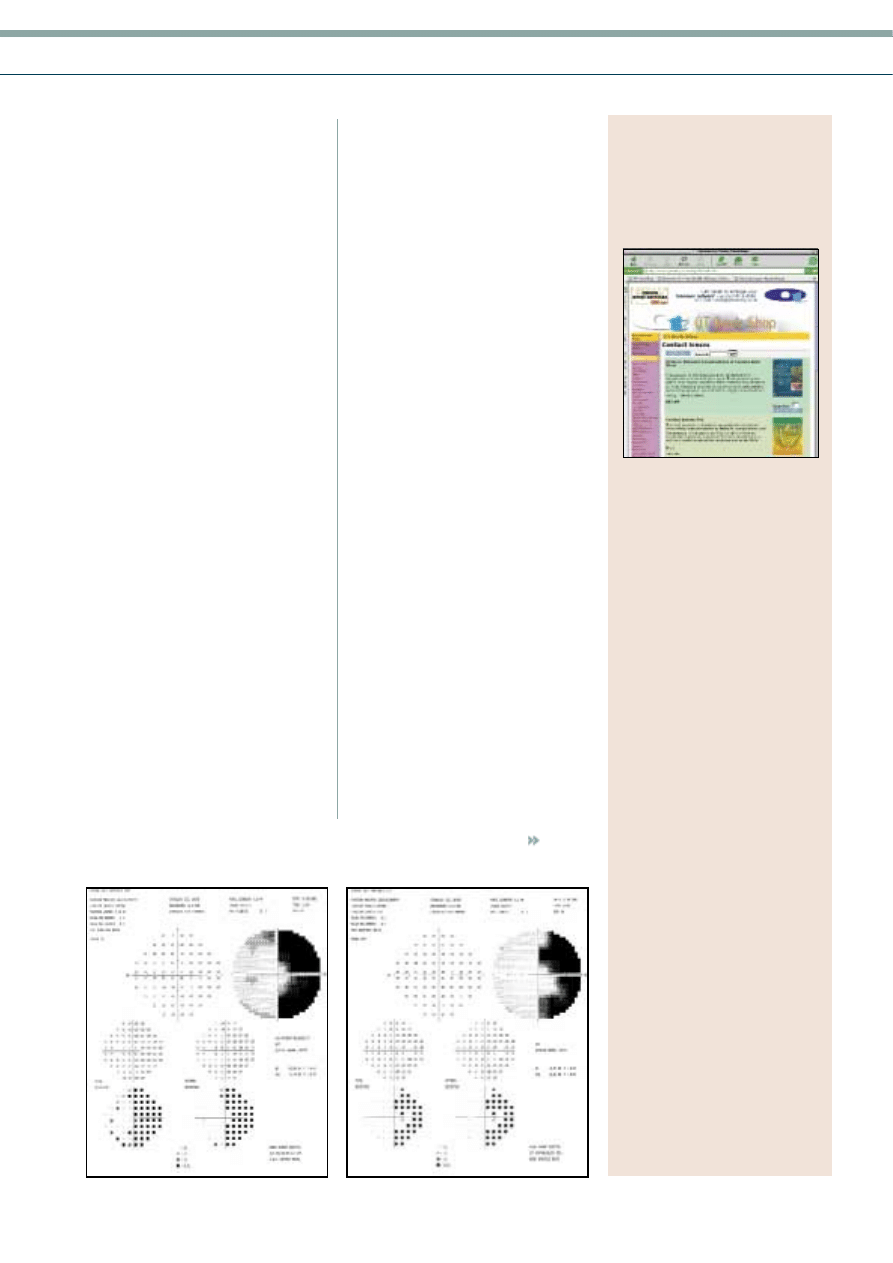
Calcarine cortex infarction results in
complete or incomplete hemianopia and
usually spares the macular field (Figure 5).
It is usually congruous. A complete
homonymous hemianopia usually spares
the macula and visual acuity is normal.
Patients often complain of ill-defined
‘blurred vision’ and are usually unaware of
the specific defect.
In clinical practice, testing optokinetic
nystagmus may help to localise the defect
in homonymous hemianopia due to stroke,
in the temporoparietal or occipital areas.
When stripes or other stimuli are moved in
the direction of a lesion that involves the
deep parietal lobe, the responses are
dampened, whereas in isolated occipital
(calcarine) lesions the responses are equal.
Improvement of the field defect within
weeks or months is the rule, particularly
when the defect has sloping margins or it is
not absolute to various size-test objects.
Neurologic symptoms and signs of
temporoparietal origin separate those cases
due to optic radiation damage from
isolated homonymous hemianopia of
occipital origin. The presence of
hemianopia should always lead to inquiry
for other neurologic deficits.
Vertebro-basilar arterial system
Reduction in vertebro-basilar blood flow
produces neurologic and visual
disturbances, as a result of damage to the
midbrain, pons, medulla, cerebellum and
occipital lobes. These disturbances may be
transient or persistent, with a varying
degree of sequela. Both oculomotor
disturbances and visual symptoms may
help in diagnosis.
In the vertebro-basilar territory, TIAs are
much more varied than they are in the
carotid system. Vertigo is the most common
neurologic symptom. Other symptoms
The
OT Bookshop
is now
on the web
200 books
available to
buy online
Categorised under
• Binocular vision
• CD ROMS
• CPD
• Colour blindness
• Contact lenses
• Dictionaries
• Legal
• Low vision
• Ocular conditions
• Ocular disease
• Ophthalmology
• Optometry, optics,
ophthalmics
• Orthoptics, vision therapy
• Paediatric vision
• Practice management
• Primary care
• Surgical
• Therapeutics
• Visual fields
www.optometry.co.uk
(click OT Book Shop,
then browse the categories)
Payment methods
• Credit card by secure
server
• Credit card by fax
• Credit card by phone
• UK cheque by post
Figure 5
Homonymous hemianopia, sparing the macula, recorded
with static perimetry in a patient with occipital lesion
LE
RE

34
|
November 28
|
2003 OT
Continuing Professional Development
SPECIALISTS IN EYECARE
a
Sponsored by
Panagiotis Karadimas MD
include dysarthria, transient weakness,
drop attacks and occipital headaches. The
most common visual symptom is a
characteristic, brief, binocular ‘grey out’ of
vision, which lasts a few seconds (rarely, up
to five minutes). Transient diplopia is a
rare symptom from ischaemia of the ocular
motor nerves, nuclei, supranuclear and
internuclear pathways. Typically, this
symptom lasts five to 10 minutes. Episodic
oscillopsia or ‘jumping vision’ may occur
during attacks of vertigo or dizziness.
The cause of vertebro-basilar TIA is
speculative. Congenital vascular anomalies
and haematological disorders are possible
causes. However, in most patients,
atheromatous disease is the main problem.
Stroke usually occurs without previous
TIAs in vertebro-basilar disease.
Hypertension and atherosclerosis are the
most common causes, in addition to
emboli from the heart or distal large
arteries. Combined brainstem symptoms
and signs include vestibular nystagmus,
miotic pupils, VI nerve and conjugate gaze,
and internuclear and facial palsies.
Terminal PCA ischaemia may occur alone
or together with a homonymous
hemianopia. Lesions in the vertebro-basilar
territory can produce bilateral deficits,
whereas carotid lesions produce unilateral
deficits.
Brainstem signs most often arise from
the lesions in the dorsal midbrain. These
are typically characterised by abnormal
vertical gaze, upgaze and/or downgaze
paresis with lid retraction, or as an isolated
upgaze paresis. Pupillary signs and
internuclear ophthalmoplegia may also be
present.
Periaqueductal midbrain infarctions are
usually accompanied by see-saw nystagmus
(pendular nystagmus, in which one eye
elevates and intorts while the other
depresses and extorts) and convergence-
retraction nystagmus (jerk nystagmus,
stimulated by attempted upward gaze, in
which the fast phase brings the two eyes
towards each other in a convergence
movement while the globe retracts into the
orbit). Strokes that involve these structures
can be identified using magnetic resonance
imaging (MRI).
Pontine strokes produce primarily
horizontal disorders of eye movement. Such
strokes are usually associated with dizziness,
facial nerve palsy, contralateral hemiparesis,
hemisensory symptoms and cerebellar signs.
Isolated VI nerve palsy without neurologic
signs has also been shown, using MRI, to be
due to a fascicular lesion. Unilateral
internuclear ophthalmoplegia may be due
to infarction of the medial longitudinal
fasciculus in the pons.
Paraneoplastic syndromes
Paraneoplastic syndromes result from the
immunologic effects of cancer located
remotely from the affected organ. Although
not exclusively a disease of the old age,
older adults are more commonly affected,
due to the increased frequency of
malignancies associated with visual
paraneoplastic syndromes in this age
group.
The two most common paraneoplastic
syndromes affecting the eye are cancer-
associated retinopathy and melanoma-
associated retinopathy.
Cancer-associated retinopathy
The cancer-associated retinopathy (CAR) is
a visual paraneoplastic disorder in which
autoantibodies against tumour antigen
cross-react with retinal proteins, resulting in
rod and cone dysfunction. Small cell
carcinoma of the lung is the systemic
malignancy most often associated with the
CAR syndrome. Gynaecologic, breast,
endocrine and a host of other
malignancies, may be also associated with
CAR. All of these malignancies induce the
expression of a 23-kD protein, which
triggers an autoimmune attack on the
retina. Patients present with severe,
progressive, bilateral loss of vision over
months. It is important to note that visual
symptoms may precede diagnosis of the
underlying malignancy and, as a result,
suspicion of this syndrome should prompt
investigation for a tumour if one has not
been detected.
Ophthalmic manifestations
Visual loss resulting from CAR may be
acute or subacute and it is often associated
with perception of flickering lights. Clinical
manifestations are the result of cone and
rod dysfunction. Cone dysfunction presents
with photosensitivity, colour vision
abnormalities, central scotomas and
decreased visual acuity. Rod dysfunction is
characterised by nyctalopia (night
blindness), prolonged dark adaptation and
peripheral or ring scotomas.
Although the fundus can appear normal
in the early stages of CAR syndrome,
progressive ocular findings include
narrowed retinal arteries, mottling of the
retinal pigment epithelial layer and optic
nerve pallor. Pathological involvement of
the retina may be patchy, and this accounts
for the analogous patchy loss of visual
field.
Visual field loss may manifest as either
peripheral constriction, mid-peripheral ring
scotomas that often cross the vertical
meridian, or central defects. The
electroretinogram shows reduced
amplitudes of both the cone and rod
responses, or even no detectable response.
Diagnosis of this condition is usually
helped by the findings of an abnormal
electroretinogram in conjunction with
normal fundi, absence of family history of
retinal disease, and a clinical course
compatible with this disorder.
Pathogenesis
CAR is considered a result of an
immunologic cross-reaction against a
retinal antigen, which is also expressed
from the malignant tumour. The CAR
retinal antigen was identified in 1992, and
is termed the 23-kD photoreceptor
component recoverin, a calcium-binding
protein which regulates phosphorylation of
the visual pigment rhodopsin during visual
transduction. The human recoverin gene
has been mapped to chromosome 17 in a
region containing other cancer-related loci.
Although the 23-kD recoverin protein is
the most common retinal antigen linked to
the CAR syndrome, it is only one of 15
antigens expressed by rods, cones and
ganglion cells of the retina, which are
thought to act as potential autoantigens in
CAR syndrome. The next most common
retinal autoantigen responsible for this
syndrome is a 40-kD protein, followed by
45 and 60-kD proteins, the sequences and
functions of which remain unknown.
Studies in cells exposed in vitro to the
anti-recoverin antibody have shown that
cell death occurs by apoptosis.
The 23-kD recoverin antigen is most
commonly associated with the CAR
syndrome. However, other patients have
been described with visual symptoms and
retinal changes similar to those seen in
CAR syndrome, with autoantibodies against
recoverin, but who, after three to five years
of evaluation, do not demonstrate any
evidence of malignancy. The term
‘recoverin-associated retinopathy’ has been
used to describe the condition of these
otherwise healthy patients.
Treatment
Many therapeutic interventions, including
treatment of the underlying malignancy,
steroid therapy, plasmapheresis and
administration of intravenous
immunoglobulin, have been used in the
management of patients with CAR, and
certain cases have demonsrated a good
response. In general, however, the visual
prognosis is considered poor.
Melanoma-associated retinopathy
Melanoma-associated retinopathy (MAR)
syndrome is another visual paraneoplastic
syndrome in which antibodies directed
against tumour antigen cross-react with
retinal cells. In contrast to CAR syndrome,
in which the identity of the retinal antigens
has been revealed by
immunohistochemical studies, no specific
retinal antigen has yet been identified as
aetiological in the MAR syndrome.
Ophthalmic manifestations
Patients with MAR syndrome most often
present with an established diagnosis of
cutaneous melanoma, and develop vision
problems years later, usually associated
with non-ocular metastasis. In a recent
review of the published cases, the average
age at presentation was 57.5 years (range
30–78 years) and the male: female ratio
was 4.7:1.
The presenting visual symptoms include
the sudden onset of shimmering, flickering
Continuing Professional Development
SPECIALISTS IN EYECARE
a
Sponsored by
35
|
November 28
|
2003 OT
1. How many cases of AION are
categorised as arteritic, associated
with temporal arteritis?
a. 5%
b. 10%
c.
25%
d. 50%
2. What is the main goal
of treatment in AAION?
a. To normalise laboratory findings
b. To restore vision
c.
To prevent further deterioration of
vision
d. To prevent involvement
of the fellow eye
3. When should treatment be instituted
in a patient with a suspicion of
AAION?
a. Immediately, on presumed diagnosis
b. After laboratory investigation is
completed
c.
After results of biopsy are available
d. After a general physical examination is
completed
4. Most of the patients with AAION
present with a visual acuity of:
a. 6/60 or worse
b. 6/60 to 6/24
c.
6/24 to 6/12
d. 6/12 or better
5. What is the five-year mortality rate in
patients who have ocular ischaemic
syndrome?
a. 5%
b. 10%
c.
20%
d. 40%
6. Which is the most prominent anterior
segment feature of ocular ischaemic
syndrome?
a. Ectropion uvea
b. Anterior uveitis
c.
Neovascularisation of the iris
d. Corneal oedema
7. Which one of the following is NOT a
posterior segment sign of ocular
ischaemic syndrome?
a. Dilation of retinal veins
b. Tortuosity of retinal veins
c.
Retinal haemorrhages
d. Neovascularisation of the optic disc
8. Which one of the following is NOT a
finding of ocular ischaemic syndrome
in fluorescein angiography?
a. Increased arteriovenous transit time
b. Patchy choroidal filling
c.
Leakage from choroidal
neovascular membrane
d. Late staining of retinal vessels
9. A patient presenting with amaurosis
fugax is at risk of visual loss,
mainly from:
a. advanced glaucoma
b. central retinal artery occlusion
c.
endophthalmitis
d. choroidal neovascular membrane
10. Which is the major neuro-ophthalmic
sign of middle cerebral artery
stroke?
a. Bitemporal hemianopia
b. Homonymous hemianopia
c.
Ipsilateral monocular visual loss
d. Contralateral monocular visual loss
11. Which tumour is most commonly
associated with CAR?
a. Small cell carcinoma of the lung
b. Endocrine cancers
c.
Breast cancer
d. Cutaneous melanoma
12. Which one of the following will
clearly differentiate between a
diagnosis of CAR and MAR?
a. Symptoms
b. Fundus appearance
c.
Visual fields
d. Electroretinogram
MCQs
An answer return form is included in this
issue. It should be completed and
returned to:
CPD initiatives (c4397j), OT,
Victoria House, 178-180 Fleet Road,
Fleet, Hampshire, GU51 4DA
by January 14, 2004.
Under no circumstances will forms
received after this date be marked
– the answers to the module will have
appeared in our January 16 issue and
scores sent electronically to the
accrediting bodies.
Systemic diseases of old age: Ophthalmic manifestations Part 2
Please note there is only
ONE correct answer
Module 5 Part 12
of the ageing eye series
or pulsating photopsias, night blindness,
mildly progressive visual loss and mild
peripheral field constriction.
In the early stages of the disorder, the
fundus may appear normal. With
progression, clinical features similar to
those in the CAR syndrome may occur.
Moreover, this syndrome may be associated
with acute anterior or posterior uveitis as
well as with patchy choroidal
depigmentation.
Visual fields usually show generalised
constriction. Central or paracentral
scotomas or depressions and arcuate visual
field defects, may also be seen.
The electroretinogram reveals a
characteristic pattern of a markedly
decreased b-wave, indicating compromised
bipolar cell function, in the presence of a
normal dark-adapted a-wave
(electronegative electroretinogram),
indicating normal photoreceptor cell
function. Similar electroretinographic
findings are seen in congenital stationary
night blindness.
Pathogenesis
In addition to electrophysiological
findings, histopathological observations
implicate the bipolar cells as the primary
site of paraneoplastic damage in MAR
syndrome. A marked reduction in the
density of bipolar neurons in the inner
nuclear layer, in the presence of normal
photoreceptor cells in the outer nuclear
layer, were demonstrated in the eyes of a
59-year old man who died of metastatic
cutaneous melanoma with visual loss
secondary to MAR.
Treatment
The therapeutic strategies that have been
employed to treat MAR are similar to those
used in CAR. Oral, subtenon’s or
intravenous corticosteroids,
plasmapheresis, intravenous
immunoglobulin, azathioprine, gabapentin
and x-irradiation of metastases or
cytoreductive surgery, have all been used.
Although, occasionally, combinations of
these agents have shown some benefit,
treatment of the visual loss associated with
MAR is considered largely ineffective.
Conclusion
Giant cell arteritis, carotid artery disease,
strokes and non-ocular cancer may all
result in ophthalmic manifestations in the
older population. Early diagnosis and
prompt treatment of ophthalmic and
general conditions may favourably alter the
course of these diseases.
Acknowledgement
The figures in both parts of this article were
provided by courtesy of the Medical Retina
Unit, 1st Department of Ophthalmology,
Henry Dunant Hospital, Athens.
References
For a full set of references, email nicky@optometry.co.uk.
Wyszukiwarka
Podobne podstrony:
Neuropatia n II 2
NEUROPSYCHOLOGIA W II Neuroanatomia zarys ogólny
NEUROPSYCHOLOGIA W II Neuroanatomia zarys ogólny
gent neuropatie n II
Neuropatia n II 2
Neuropeptydy kości, Weterynaria UP lublin, II rok, Materiały, Fizjologia
neuropatie cukrzycowe, Pielęgniarstwo licencjat cm umk, II rok, Patofizjologia
Prel II 7 szyny stałe i ruchome
Produkty przeciwwskazane w chorobach jelit II
9 Sieci komputerowe II
W wiatecznym nastroju II
W01(Patomorfologia) II Lek
Mała chirurgia II Sem IV MOD
Analiza czynnikowa II
więcej podobnych podstron