C
ha
pt
er
60
418
Kerry Bron, MD, and
Avrum N. Pollock, MD
Pediatric Gastrointestinal radioloGy
1. What are the most common causes of small bowel obstruction in a child?
AAIIMM is a mnemonic that makes it easy to remember the causes:
•
A = Adhesions, usually postsurgical
•
A = Appendicitis
•
I = Intussusception
•
I = Incarcerated inguinal hernia
•
M = Malrotation with volvulus or bands
•
M = Miscellaneous, such as Meckel diverticulum or intestinal duplication
2. What is intussusception?
Intussusception is a condition in which a proximal portion of the bowel (intussusceptum) telescopes into the
adjacent distal bowel (intussuscipiens). When the inner loop and its mesentery become obstructed, a small bowel
obstruction occurs.
3. What causes intussusception?
In most cases, intussusception is idiopathic. In less than 5% of cases, the intussusception contains a lead point, such as
a polyp, Meckel diverticulum, or hypertrophic lymphatic tissue. Most intussusceptions are ileocolic.
4. Describe the clinical signs of intussusception.
The classic clinical triad of intussusception is intermittent colicky abdominal pain, current jelly stools, and a palpable
abdominal mass. Less than 50% of patients present with these symptoms, however. Children often cry and are very irritable
during bouts of abdominal pain, and then become drowsy and lethargic. Vomiting and fever may also occur. Intussusception
is most common in children 3 months to 4 years old, with a peak incidence at 3 to 9 months. It is more common in boys.
5. How is intussusception diagnosed radiologically?
The most accurate technique for the diagnosis of intussusception is ultrasound (US). The characteristic US appearance
is a mass that measures 3 to 5 cm, which is easily detectable. On the transverse scan, the mass has a “target”
appearance that contains echogenic fat. The
“pseudokidney” sign appears in the longitudinal
direction. A barium enema can also be used to
diagnose intussusception. Although the plain
film has been used in the past to diagnose
intussusception by detection of a soft tissue mass
in the right upper quadrant and lack of large bowel
gas, particularly in the right upper quadrant, studies
have shown poor interobserver agreement and
predictive value of only approximately 50%.
6. How is an intussusception treated?
An intussusception is treated by air enema with
fluoroscopic guidance or hydrostatic enema
using barium or water-soluble contrast agent
(
). The advantages of the air enema are
that it is quicker, less messy, easier to perform,
and delivers less radiation to the patient. The
only contraindications to enema reduction of
intussusception are pneumoperitoneum or peritonitis.
The air enema can generates pressure of 120 mm Hg
to reduce the intussusception.
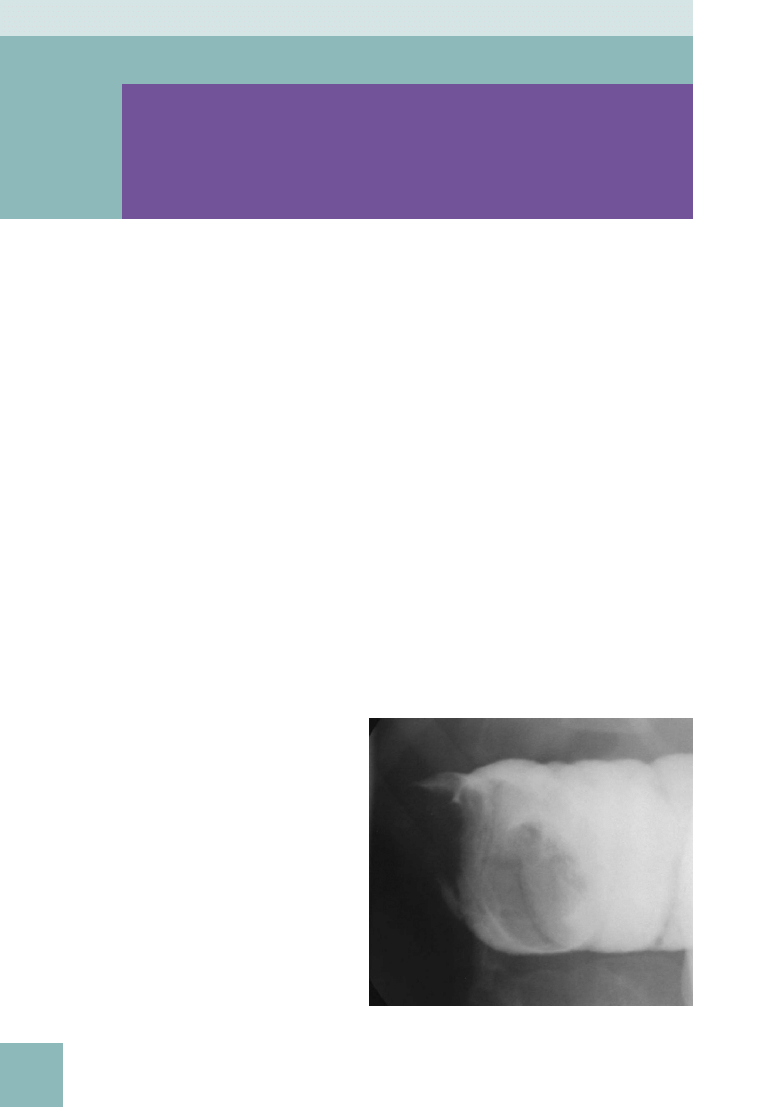
Figure 60-1.
Spot radiograph from a contrast enema examination
shows intussusception, with the lead point outlined by the barium.
419
7. How can one tell that an intussusception has been successfully reduced?
If a successful air reduction has been performed, fluid with air bubbles should be seen passing through the ileocecal
valve into the terminal ileum. If a successful reduction with contrast agent has been performed, contrast agent must
reflux into multiple loops of small bowel. If reflux into the small bowel is not seen, the intussusception may not have
been completely reduced, and a distal lead point may have been overlooked.
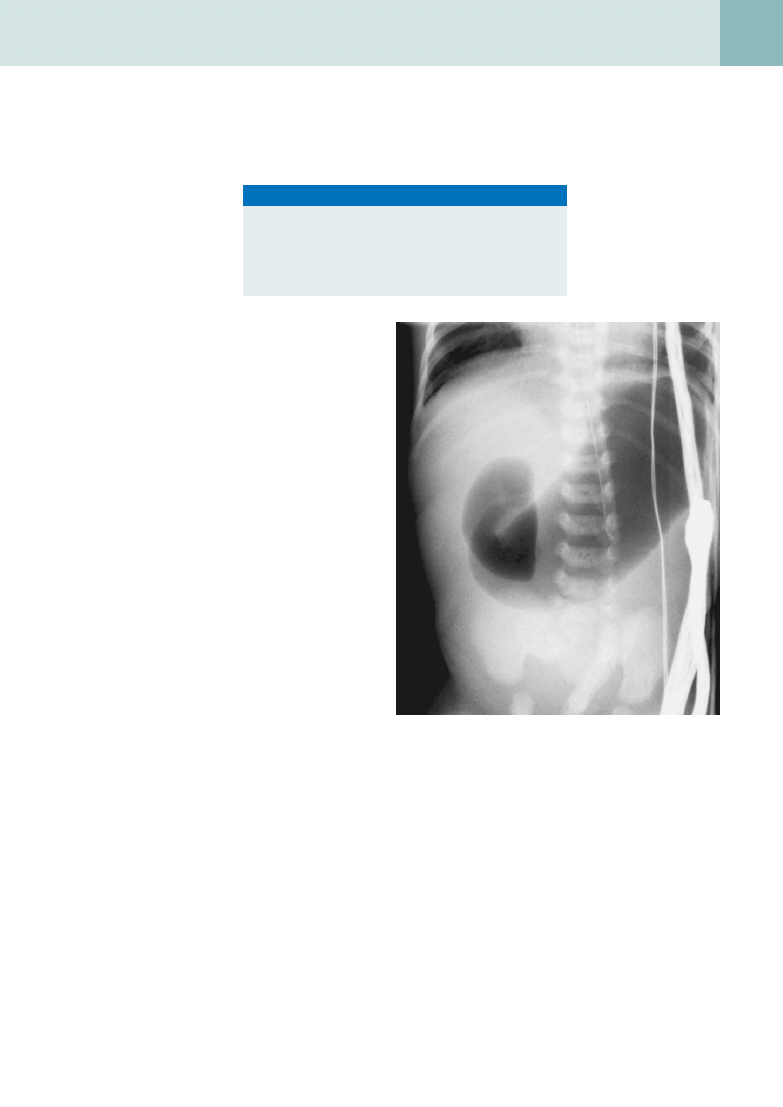
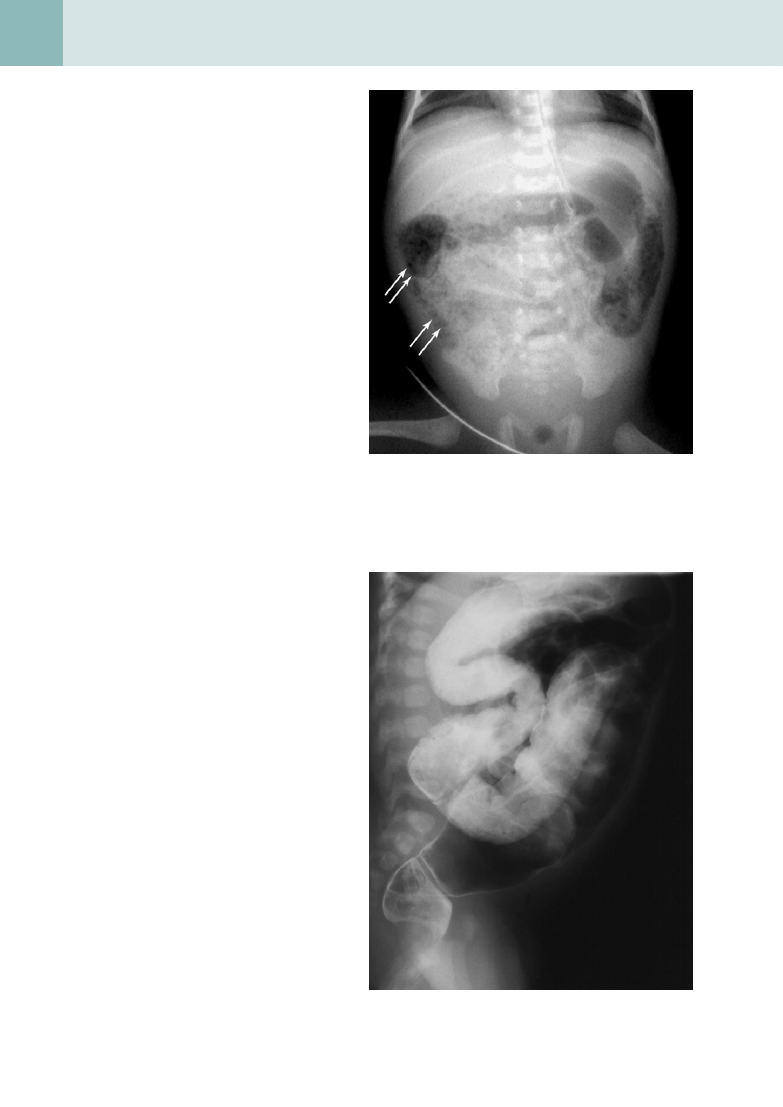
8. Describe the “double bubble” sign,
and name the conditions in which it
is found.
The “double bubble” sign is found on plain
radiographs and represents an air-filled or fluid-
filled distended stomach and duodenal bulb (
). It is seen in malrotation, duodenal atresia,
and jejunal atresia.
9. What is malrotation of the
intestines?
Malrotation of the intestines is a misnomer because
it is really nonrotation or incomplete rotation of
the bowel. To understand malrotation, one must
first consider normal embryologic rotation of the
intestines. During normal embryologic development
in the first trimester, the midgut leaves the
abdominal cavity, travels into the umbilical cord, and
returns to the abdominal cavity. As the intestines
return, the proximal and distal parts of the midgut
rotate around the superior mesenteric artery axis
270 degrees in a counterclockwise direction. The
ligament of Treitz (duodenojejunal junction) lands in
the left upper quadrant, and the cecum comes to
rest in the right lower quadrant. In malrotation, this
intestinal rotation and fixation occur abnormally. If
normal rotation does not occur, the cecum is not
anchored in the right lower quadrant and may be
midline or in the upper abdomen. The small bowel is
not anchored in the left upper quadrant and may lie
entirely in the right abdomen.
10. What are Ladd bands?
Ladd bands are dense peritoneal bands that develop as an attempt to fix the bowel to the abdominal wall in malrotation.
They may extend from the malpositioned cecum across the duodenum to the posterolateral abdomen and porta hepatis
in either incomplete rotation or nonrotation and can cause extrinsic duodenal obstruction.
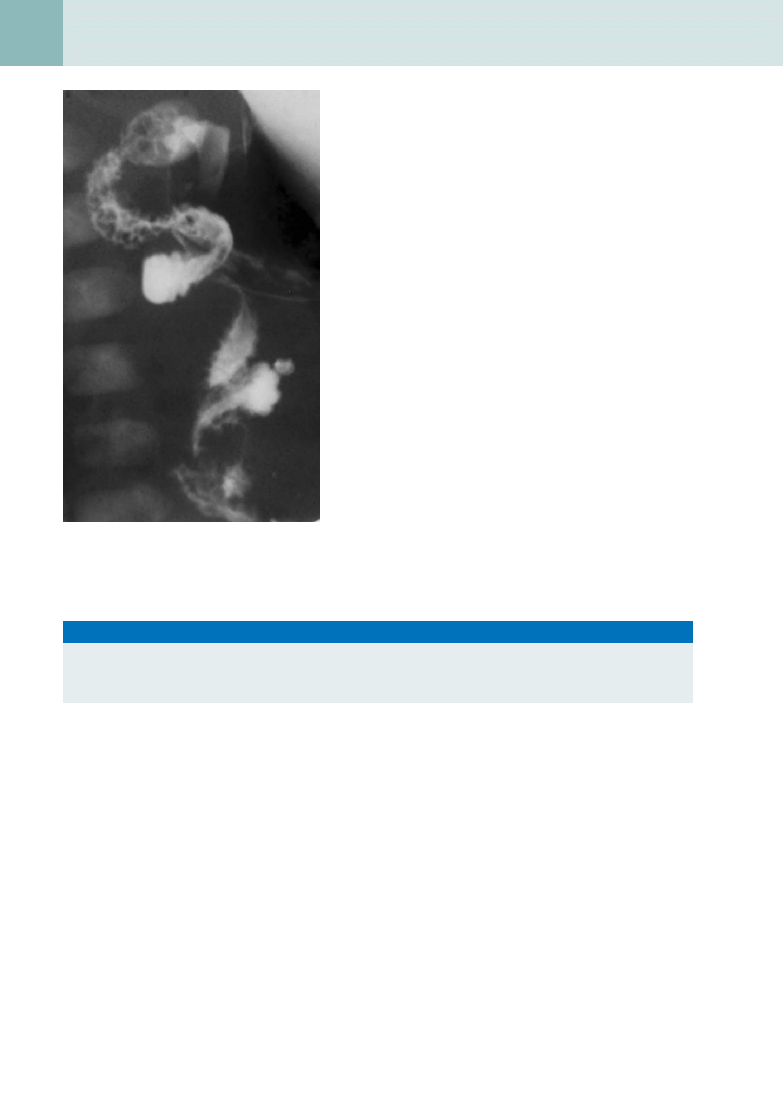
11. How does a midgut volvulus occur, and why is this an emergency?
Lack of attachment of the midgut to the posterior abdominal wall allows the midgut to twist on a shortened root
mesentery, which results from lack of complete rotation (
). This twisting is called a volvulus, and it causes
small bowel obstruction with concomitant obstruction to the lymphatic and venous supply of the bowel and eventually
to the arterial supply, which leads to ischemia and necrosis. If it is not repaired within several hours, all of the intestine
supplied by the superior mesenteric artery undergoes infarction.
12. Does a patient with malrotation always present with clinical symptoms.
Not all patients with malrotation are symptomatic because not all develop a midgut volvulus or extrinsic duodenal
obstruction from Ladd bands.
Figure 60-2.
Plain film of the abdomen in a child with duodenal
atresia, showing a dilated stomach and duodenal bulb—the “double
bubble” sign.
Key Points: Intussusception
1. Common cause of small bowel obstruction in children
2. Idiopathic in children, in contrast to in adults
3. Usually ileocolic
4. Diagnosed by US
5. Treated with air enema or contrast barium enema
pediatric radiology
420
pediatric gastrointestinal radiology
13. What is the clinical presentation of
malrotation?
Patients with incomplete rotation who have intestinal
obstruction usually present within the first week or first
month of life (75% of patients). They present with an acute
onset of bilious vomiting, which is a surgical emergency.
Some patients present later in childhood with intermittent
mechanical obstruction, which manifests as cyclic
vomiting. Malrotation in the remaining patients is often
found incidentally when the patients are studied for other
complaints.
14. Which study is the gold standard for
diagnosing malrotation?
The upper gastrointestinal (GI) examination is the gold standard
for diagnosing malrotation. To confirm normal rotation of the
bowel, the ligament of Treitz, which attaches the third and
fourth parts of the duodenum, must be visualized to the left of
midline. If there is malrotation, the ligament of Treitz may be
located to the right of midline or in the midline. Often, there is
inversion of the superior mesenteric artery and vein, which can
be visualized on computed tomography (CT).
15. List other anomalies that are associated with
malrotation.
•
Duodenal atresia or stenosis
•
Meckel diverticulum
•
Omphalocele
•
Gastroschisis
•
Polysplenia/asplenia syndromes
•
Situs ambiguus
•
Bochdalek hernia
•
Renal anomalies
16. Describe the clinical presentation of pyloric stenosis.
Hypertrophic pyloric stenosis, which is the most common GI surgical disease of infancy in the United States, manifests
most commonly during the second to sixth weeks of life, with a peak incidence at 3 weeks of age and rare presentation
after age 3 months. The major symptom is progressive nonbilious vomiting, which starts as simple regurgitation and
progresses to projectile vomiting. This progressive vomiting leads to dehydration and hypochloremic metabolic alkalosis
and weight loss. The condition is more common in boys. A palpable “olive” representing the thickened pylorus muscle is
present in the right upper quadrant approximately 80% of the time if the infant can be examined in a calm manner with
decreased stomach distention.
17. If the “olive” cannot be palpated, how can pyloric stenosis be diagnosed with
radiologic studies?
The evaluation can begin with a supine or prone plain film of the abdomen, which can exclude other diagnoses
that could be causing similar obstructive symptoms. The plain film would also reveal a markedly dilated stomach,
soft tissue mass projecting into the gastric antrum, and paucity of gas in the distal bowel. The suspicion of pyloric
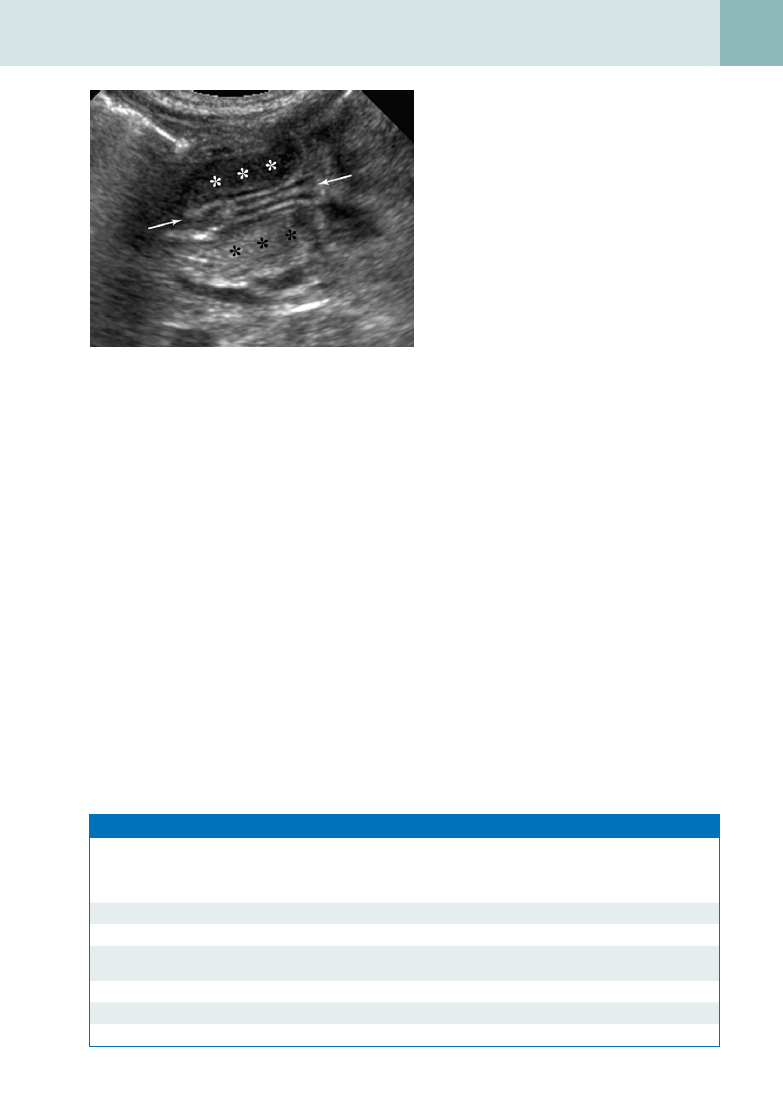
stenosis can be confirmed with either US or fluoroscopy. US is the imaging test of choice because it directly
visualizes the hypertrophied pylorus muscle without radiation (
), whereas an upper GI series infers the
presence of pyloric stenosis indirectly. With US, the pylorus muscle is seen as a hypoechoic structure greater than 4
mm thick surrounding an echogenic compressed pyloric channel. Although less sensitive, the pyloric channel length
is another measurement used to make the diagnosis. A length greater than 17 mm is considered diagnostic for
pyloric stenosis.
Figure 60-3.
Spot radiograph from an upper GI
examination showing the “corkscrew” finding of a midgut
volvulus.
Key Points: Malrotation of the Intestines
1. Malrotation causes small bowel obstruction through a midgut volvulus and Ladd bands.
2. Malrotation causes altered GI anatomy, with the ligament of Treitz not situated in the left upper quadrant and the
cecum not in the right lower quadrant.
pediatric gastrointestinal radiology
421
pediatric radiology
18. What is Meckel diverticulum?
Meckel diverticulum is the most common
anomaly of the GI tract. It is a persistence of the
omphalomesenteric duct at its junction with the
ileum. It can be remembered by the rules of 2:
It occurs in 2% of the population, 2% develop
complications, complications usually occur before
2 years of age, and it is located within 2 feet of the
ileocecal valve. The most common complication
of Meckel diverticulum is painless GI bleeding,
which occurs secondary to irritation or ulceration
from production of hydrochloric acid by the gastric
mucosa that lines it.
19. How is Meckel diverticulum
diagnosed?
Meckel diverticulum is detected by a nuclear
medicine scan with technetium (Tc)-99m
pertechnetate. The tracer accumulates within the
diverticulum, usually appearing at or approximately
at the same time as activity in the stomach, with
gradually increasing intensity, which verifies the
presence of ectopic gastric mucosa.
20. What are the most common causes of GI bleeding in children?
The differential diagnosis depends on the age of the patient (
21. What causes necrotizing enterocolitis (NEC)?
NEC is a multifactorial condition that has traditionally been thought to be caused by hypoxia, infection, and enteral
feeding. The pathology of NEC resembles that of ischemic necrosis. It may be that the main pathologic trigger in NEC
is injury to the intestinal mucosa, which can be caused by different factors in different patients.
22. Who develops NEC?
Approximately 80% of patients who develop NEC are premature infants. Older infants who develop NEC usually have
severe underlying medical problems, such as Hirschsprung disease or congenital heart disease. Patients with this
condition present with abdominal distention, vomiting, increased gastric residuals, blood in the stool, lethargy, apnea,
and temperature instability.
23. What findings of NEC can be seen on plain x-ray film, and what is the role of the
radiologist?
The radiographic findings of NEC are nonspecific when the condition is first suspected. Films are obtained serially; the
role of the radiologist is to try to diagnose the condition before bowel perforation occurs. In early NEC, the most commonly
detected abnormality is diffuse gaseous distention of the intestine. A more useful sign of early NEC is loss of the normal
symmetric bowel gas pattern, with a resulting disorganized or asymmetric pattern. In more advanced NEC, the finding
Figure 60-4.
US examination of the pylorus shows hypertrophic
pyloric stenosis. The thickened walls of the pylorus (asterisks) surround
the central lumen (arrows).
Table 60-1. Common Causes of Gastrointestinal Bleeding in Children
NEWBORN AND
NEONATE (<1 MO)
YOUNG INFANT
(1-3 MO)
OLDER INFANT
(3 MO–1 YR)
CHILD (1-10 YR)
Swallowed maternal blood
Esophagitis
Esophagitis
Esophagitis
Anal fissure
Intussusception
Anal fissure
Esophageal varices
Necrotizing enterocolitis
Anal fissure
Colon polyp
Colon polyp
Hemorrhagic disease of the
newborn
Gangrenous bowel
Intussusception
Anal fissure
Allergic or infectious colitis
Meckel diverticulum
Gangrenous bowel
Foreign body
Foreign body
Crohn disease
Ulcerative colitis
422
pediatric gastrointestinal radiology
of pneumatosis intestinalis (intramural gas) is
pathognomonic for the condition (
). Gas in
the portal venous system is another pathognomonic
finding in NEC, which occurs in 10% to 30% of
cases. Infants at risk for imminent perforation
often have portal venous gas. They may have the
persistent loop sign, which is a dilated loop of
intestine that remains unchanged over 24 to 36
hours. Another grave sign is a shift from a pattern
of generalized dilation to asymmetric bowel dilation.
Ascites is another sign of impending perforation.
When pneumoperitoneum develops, this is a definite
sign that the bowel has perforated, and the infant
must have surgery.
24. What are other causes of
pneumoperitoneum in infants and
children?
The most common causes are surgery and
instrumentation. Pneumoperitoneum can be
found after laparotomy, after paracentesis, or
after resuscitation. Also, distal bowel obstruction
from conditions such as Hirschsprung disease
or meconium ileus and dissection of air from
pneumomediastinum, a ruptured ulcer, or Meckel
diverticulum can cause pneumoperitoneum.
25. What is Hirschsprung disease?
Hirschsprung disease is a condition of distal
aganglionic bowel that results from the lack
of Auerbach (intermuscular) and Meissner
(submucosal) plexuses. Functional obstruction
of the distal bowel results. Hirschsprung disease
usually manifests in the first 48 hours of life with
the failure to pass meconium, or it may manifest
with abdominal distention, bilious vomiting, or
diarrhea. More than 80% of patients present in the
first 6 weeks of life.
26. What are the plain x-ray film
findings of Hirschsprung disease?
The most typical plain film finding of Hirschsprung
disease is a dilated colon proximal to the distal and
smaller aganglionic segment. Radiographs may also
show high-grade distal bowel obstruction. Radiologic
diagnosis of Hirschsprung disease requires a
). Spot radiographs are
obtained in the lateral and oblique projections, and
the examination is stopped after a transition zone
has been identified. The barium enema can show
the transition zone, which is situated between a
narrowed aganglionic segment and the distended
proximal bowel. The x-ray transition zone may be
visualized more distally than the histologic transition
zone secondary to stool dilating the proximal part of
the aganglionic segment.
27. Is Hirschsprung disease diagnosed
definitively by imaging?
To make a definitive diagnosis of Hirschsprung
disease, a rectal biopsy specimen must be obtained
that shows lack of ganglion cells.
Figure 60-5.
Plain film radiograph of the abdomen in a patient
with NEC. The mottled pattern of air in the bowel wall (arrows) is
typical of NEC.
Figure 60-6.
Lateral spot radiograph from a barium enema
examination in a patient with Hirschsprung disease shows transition
zone (from dilated to nondilated bowel) in the distal colon.
pediatric gastrointestinal radiology
423
pediatric radiology
28. Name the types of tracheoesophageal
fistulas (TEF). How common is each
type?
•
The most common type of TEF is esophageal
atresia with distal esophageal communication
with the tracheobronchial tree (
). This
accounts for more than 80% of cases.
•
The next most common type is esophageal atresia
without a TEF, which accounts for almost 10% of
cases.
•
H-type fistulas occur between an otherwise
intact trachea and esophagus and account for
approximately 5% of cases.
•
Esophageal atresias occurring with proximal and
distal communication with the trachea are found
in less than 2%
of cases, and esophageal atresia with proximal
communication is rare.
TEF is associated with VACTERL syndromes
(in which affected patients manifest at least
three of the following: vertebral anomalies, anal
atresia/imperforate anus, cardiac anomalies,
tracheoesophageal fistula, renal anomalies, and limb
anomalies).
29. What are the plain film findings in
TEF?
In a patient with esophageal atresia (and no fistula
or a proximal fistula), plain film may reveal a gasless
abdomen. A nasogastric tube may be seen coiled in the proximal esophagus. Patients with esophageal atresia with a distal
TEF or H-type fistula may present with a distended abdomen. Aspiration is a risk for all patients with esophageal atresia.
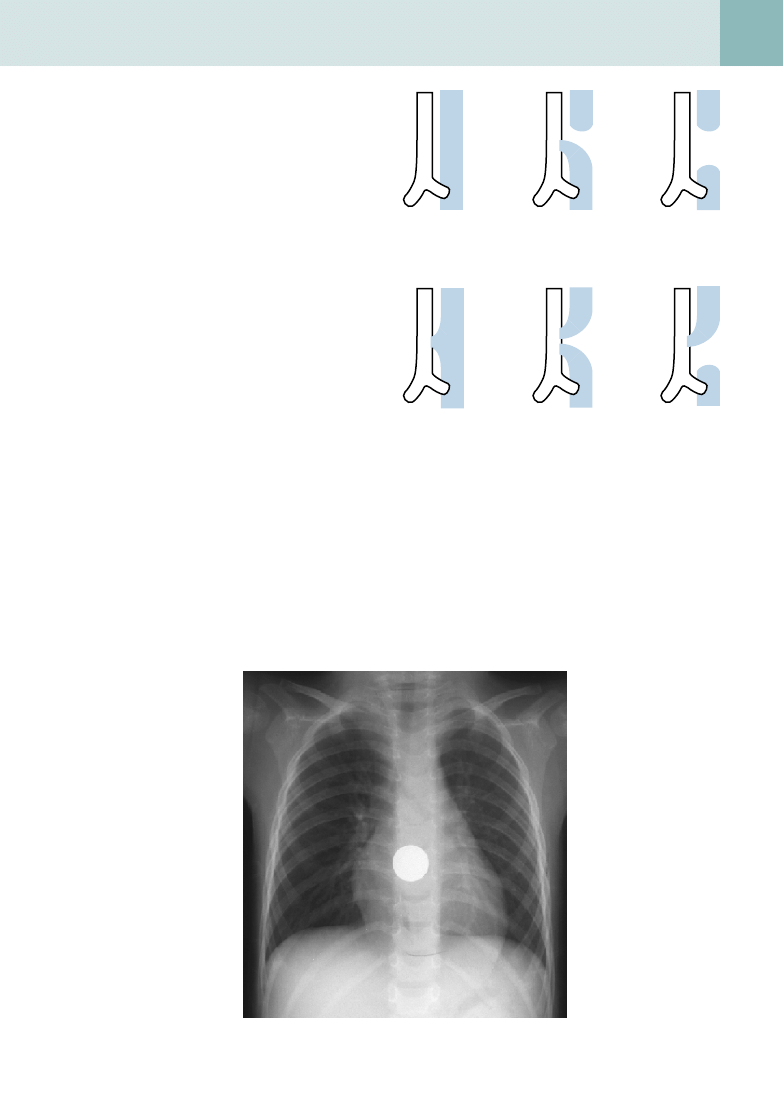
30. How can a plain film help to differentiate a coin in the esophagus from a coin in the
trachea?
On a plain chest film, a coin in the esophagus is visualized as a round object en face (a full circle can be seen)
(
). A coin in the trachea lies sagittally and appears end-on in a posteroanterior film.
A
B
C
D
E
F
Figure 60-7.
Different types of TEF.
A, Normal relationship of
esophagus anterior to trachea—no atresia or fistula.
B, Esophageal
atresia with distal TEF—most common (>80%).
C, Esophageal atresia
with no TEF (approximately 10%).
D, H-type fistula with no esophageal
atresia (approximately 5%).
E, Esophageal atresia with proximal and
distal fistulas (<2%).
F, Esophageal atresia with a proximal fistula (1%).
Figure 60-8.
Posteroanterior plain film of the chest shows a coin in the esophagus.

424
pediatric gastrointestinal radiology
B
iBliography
[1] C. Buonomo, The radiology of necrotizing enterocolitis, Radiol. Clin. North Am. 37 (1999) 1187–1197.
[2] A. Daneman, D. Alton, Intussusception: issues and controversies related to diagnosis and reduction, Radiol. Clin. North Am. 34 (1996)
743–755.
[3] K. Hayden, Ultrasonography of the acute pediatric abdomen, Radiol. Clin. North Am. 34 (1996) 791–806.
[4] M. Hernanz-Schulman, Imaging of neonatal gastrointestinal obstruction, Radiol. Clin. North Am. 37 (1999) 1163–1185.
[5] D.R. Kirks, Practical Pediatric Imaging: Diagnostic Imaging of Infants and Children, third ed., Lippincott-Raven, Philadelphia, 1997.
[6] W. McAlister, K. Kronemer, Emergency gastrointestinal radiology of the newborn, Radiol. Clin. North Am. 34 (1996) 819–844.
[7] D. Merten, Practical approaches to pediatric gastrointestinal radiology, Radiol. Clin. North Am. 31 (1993) 1395–1407.
Document Outline
- Pediatric Gastrointestinal Radiology
- What are the most common causes of small bowel obstruction in a child?
- What is intussusception?
- What causes intussusception?
- Describe the clinical signs of intussusception
- How is intussusception diagnosed radiologically?
- How is an intussusception treated?
- How can one tell that an intussusception has been successfully reduced?
- Describe the “double bubble” sign, and name the conditions in which it is found
- . What is malrotation of the intestines?
- . What are Ladd bands?
- How does a midgut volvulus occur, and why is this an emergency?
- Does a patient with malrotation always present with clinical symptoms
- What is the clinical presentation of malrotation?
- Which study is the gold standard for diagnosing malrotation?
- List other anomalies that are associated with malrotation
- Describe the clinical presentation of pyloric stenosis
- If the “olive” cannot be palpated, how can pyloric stenosis be diagnosed with radiologic studies?
- What is Meckel diverticulum?
- How is Meckel diverticulum diagnosed?
- What are the most common causes of GI bleeding in children?
- What causes necrotizing enterocolitis (NEC)?
- Who develops NEC?
- What findings of NEC can be seen on plain x-ray film, and what is the role of the radiologist?
- What are other causes of pneumoperitoneum in infants and children?
- What is Hirschsprung disease?
- What are the plain x-ray film findings of Hirschsprung disease?
- Is Hirschsprung disease diagnosed definitively by imaging?
- Name the types of tracheoesophageal fistulas (TEF). How common is each type?
- What are the plain film findings in TEF?
- How can a plain film help to differentiate a coin in the esophagus from a coin in the trachea?
- Bibliography
Wyszukiwarka
Podobne podstrony:
C20090551288 B9780323067942000420 main
C20090551288 B9780323067942000055 main
C20090551288 B9780323067942000407 main
C20090551288 B9780323067942000225 main
C20090551288 B9780323067942000432 main
C20090551288 B9780323067942000547 main
C20090551288 B9780323067942000298 main
C20090551288 B978032306794200047X main
C20090551288 B9780323067942000250 main
C20090551288 B9780323067942000638 main
C20090551288 B9780323067942000316 main
C20090551288 B9780323067942000286 main
C20090551288 B9780323067942000560 main
C20090551288 B9780323067942000341 main
C20090551288 B9780323067942000390 main
C20090551288 B9780323067942000766 main
C20090551288 B9780323067942000754 main
C20090551288 B9780323067942000122 main
C20090551288 B9780323067942000626 main
więcej podobnych podstron