C
ha
pt
er
39
275
Neil Roach, MD
OsteOpOrOsis
1. What is osteoporosis? How does it differ from osteomalacia and osteopenia?
•
Osteoporosis is characterized by low bone mass and microarchitectural deterioration of bone tissue, leading to increased
bone fragility and an increased risk of fracture. The bone has normal mineralization and histologic characteristics.
•
Osteomalacia is characterized by incomplete mineralization of normal osteoid tissue. Osteomalacia in a growing child
is also known as rickets.
•
Osteopenia is a descriptive term for decreased calcification or density of bone. Osteopenia if not due to a particular
cause, pathophysiology, or disease.
2. What are potential causes for generalized osteoporosis?
Arthritis may be either primary or secondary. Any patient who presents with osteoporosis should be evaluated
for secondary causes before being diagnosed with primary osteoporosis. Causes of primary osteoporosis include
involutional osteoporosis, juvenile osteoporosis, and idiopathic osteoporosis (premenopausal women or middle-aged
men). Secondary osteoporosis has a wide differential diagnosis, including:
•
Endocrine diseases (e.g., hypogonadism, ovarian agenesis, hyperadrenocorticism, hyperthyroidism,
hyperparathyroidism, diabetes mellitus, and acromegaly)
•
Gastrointestinal diseases (e.g., subtotal gastrectomy, malabsorption syndromes, chronic obstructive jaundice, primary
biliary cirrhosis, severe malnutrition, and anorexia nervosa)
•
Bone marrow disorders (e.g., multiple myeloma, systemic mastocytosis, and disseminated carcinoma)
•
Connective tissue diseases (e.g., osteogenesis imperfecta, homocystinuria, Ehlers-Danlos syndrome, and Marfan syndrome)
•
Miscellaneous causes (e.g., immobilization, chronic obstructive pulmonary disease, chronic alcoholism, long-term
heparin therapy, and rheumatoid arthritis)
3. What are some causes for regional or localized osteoporosis?
A focal area of bone loss can be highly localized (also known as a lytic lesion). Metastasis, multiple myeloma, and
osteomyelitis are the most common causes of lytic lesions. Larger areas of bone loss, usually without violation of
cortical bone, may be caused by a stroke or immobility of an extremity. Another cause for regional osteoporosis is reflex
sympathetic dystrophy syndrome, or Sudeck atrophy. Reflex sympathetic dystrophy is a multifactorial disorder. The
underlying cause is typically trauma, followed by regional or localized osteoporosis.
4. In what demographic groups is generalized osteoporosis most prevalent?
Bone loss starts to occur in men and women around 35 years old. Women have a greater rate of bone loss. Whites and
Asians are more likely to develop osteoporosis than blacks. A white or Asian woman has the greatest risk of developing
osteoporosis.
5. Are conventional radiographs sensitive enough to diagnose osteoporosis?
No. A large percentage (30% to 40%) of bone must be lost to appreciate a change on radiographic examination. There is
also marked intrareader and inter-reader variability for this diagnosis on radiographs.
6. What radiographic features are useful in diagnosing osteoporosis?
Decreased bone density, prominence of vertebral body end plates, and cortical thinning can be seen with osteoporosis,
but are subjective. Accentuation of trabecular stress lines from resorption of secondary trabecula is another radiographic
sign of osteoporosis; this is best appreciated around the femoral neck.
7. Is computed tomography (CT) more sensitive than conventional radiographs for
evaluating bone mineral density (BMD)?
Yes. Quantitative CT can be performed using software that is added to a standard CT scanner to measure
BMD. Other methods of assessment based on relative absorption of x-rays using a less expensive scanner are
preferred.
276
OsteOpOrOsis
8. What are other quantitative methods of measuring BMD?
Single-photon absorptiometry and dual-photon absorptiometry were the early techniques for measuring BMD. Both
used radioactive sources to produce photons. These units have essentially been replaced with dual x-ray absorptiometry
(DXA) units. DXA uses the same principles as dual-photon absorptiometry except that the radionuclide source is
replaced with an x-ray tube. Two distinct energy x-ray beams are used (usually 70 kVp and 140 kVp). DXA is the
examination of choice for the diagnosis and follow-up of osteoporosis.
0.2
20 25 30 35 40 45 50
Age
C
D
A
B
55 60 65
80 85
70 75
Total
0.4
BMD
0.6
0.8
1.0
1.2
1.4
1.6
0.2
20
L1
L2
L3
L4
25 30 35 40 45 50
Age
55 60 65
80 85
70 75
Total
0.4
BMD
0.6
0.8
1.0
1.2
1.4
1.6
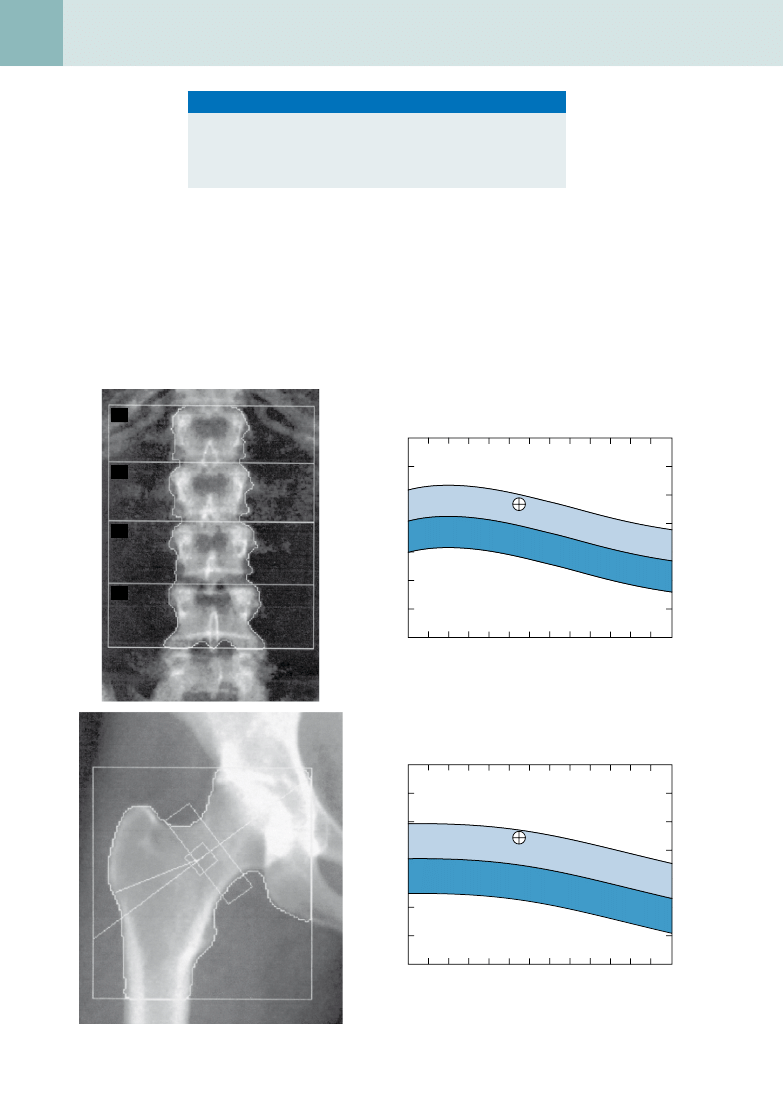
Figure 39-1.
A and B, Normal lumbar spine DXA scan in a 47-year-old woman. C and D, Normal right hip DXA scan in the same patient.
Key Points: Osteoporosis
1. Osteoporosis is the most common skeletal disorder worldwide.
2. Osteoporosis can start at any age.
3. Osteoporosis progresses silently over a long period.
4. Osteoporosis is preventable with therapy.
OsteOpOrOsis
277
mUsCULOsKeLetAL rADiOLOGY
9. What are the units of measurement of BMD?
BMD is measured in grams divided by area: g/cm
2
. Technically, it is not a density (weight/volume) being measured, but a
weight divided by area.
10. What sites of the skeleton are routinely assessed on a DXA scan?
The lumbar spine, from L1 or L2 to L4, and the proximal femur (regions of interest are the femoral neck, trochanteric
region, and Ward triangle) are routinely assessed on a DXA scan. Ward triangle is a site at the proximal femur where
bone mineral loss is thought to occur first (
).
11. How can large osteophytes and sclerotic changes in a patient with lumbar
degenerative disease affect bone densitometry assessment?
On an anteroposterior evaluation of the lumbar spine, the osteophytes and other degenerative changes in the vertebrae
and posterior elements can cause pseudoelevation of the BMD. This pseudoelevation can result in the BMD of an
osteoporotic patient appearing falsely normal. This is one reason that BMD measurements are routinely obtained in two
separate locations.
0.2
20 25 30 35 40 45 50
Age
C
D
A
B
55 60 65
80 85
70 75
Total
0.4
BMD
0.6
0.8
1.0
1.2
1.4
1.6
0.4
20
L1
L2
L3
L4
25 30 35 40 45 50
Age
55 60 65
80 85
70 75
Total
BMD
0.6
0.8
1.0
1.2
1.4
1.6
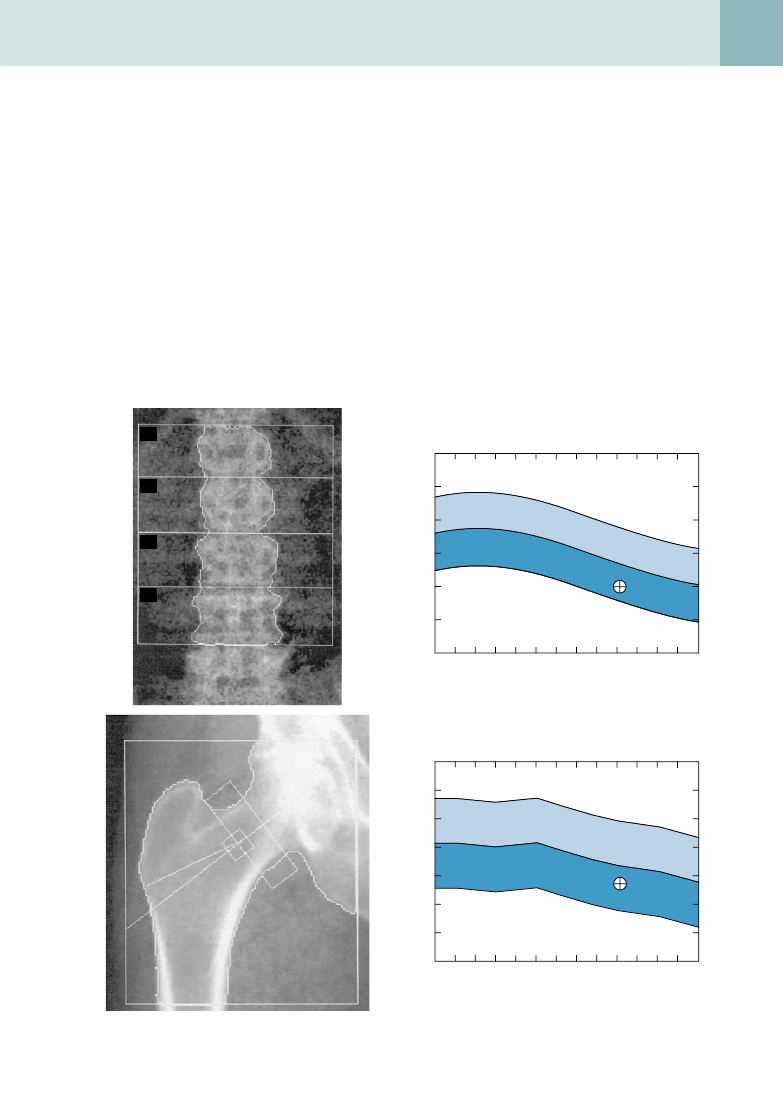
Figure 39-2.
A and B, Osteoporosis in a 65-year-old woman. The t score is −2.9. C and D, Osteopenia of the right hip with a t score of
−1.8 in the same patient.

278
OsteOpOrOsis
12. What are the World Health Organization criteria for the diagnoses of normal BMD,
osteopenia, and osteoporosis?
•
Normal is a BMD within 1 SD of the young adult reference mean.
•
Osteopenia is a BMD 1 to 2.5 SD below the young adult reference mean.
•
Osteoporosis is a BMD more than 2.5 SD below the young adult reference mean.
13. What are t and z scores?
•
The t score is the number of standard deviations above or below the young adult mean. The young adult mean is the
expected normal value for the patient compared with others of the same sex and ethnicity in a reference population
the manufacturer builds into the DXA software. It is approximately what the patient should have had at his or her peak
bone density at about age 20.
•
The z score is the number of standard deviations of the patient’s bone density above or below the values expected
for the patient’s age. By comparing the patient’s BMD with the expected BMD for his or her age, the z score can help
classify the type of osteoporosis. Primary osteoporosis is age-related osteoporosis in which no secondary causes are
found.
B
iBliography
[1] National Osteoporosis Foundation, Physicians Resource Manual on Osteoporosis: A Decision-making Guide, second ed., National
Osteoporosis Foundation, Washington, DC, 1991.
[2] World Health Organization, Assessment of fracture risk and its application to screening for postmenopausal osteoporosis: report of a WHO
study group, WHO Technical Report Series 843 (1994) 1–129.
Document Outline
- Osteoporosis
- What is osteoporosis? How does it differ from osteomalacia and osteopenia?
- What are potential causes for generalized osteoporosis?
- What are some causes for regional or localized osteoporosis?
- In what demographic groups is generalized osteoporosis most prevalent?
- Are conventional radiographs sensitive enough to diagnose osteoporosis?
- What radiographic features are useful in diagnosing osteoporosis?
- Is computed tomography (CT) more sensitive than conventional radiographs for evaluating bone mineral density (BMD)?
- What are other quantitative methods of measuring BMD?
- What are the units of measurement of BMD?
- What sites of the skeleton are routinely assessed on a DXA scan?
- How can large osteophytes and sclerotic changes in a patient with lumbar degenerative disease affect bone densitometry assessment?
- What are the World Health Organization criteria for the diagnoses of normal BMD, osteopenia, and osteoporosis?
- What are t and z scores?
- Bibliography
Wyszukiwarka
Podobne podstrony:
C20090551288 B9780323067942000420 main
C20090551288 B9780323067942000055 main
C20090551288 B9780323067942000407 main
C20090551288 B9780323067942000225 main
C20090551288 B9780323067942000432 main
C20090551288 B9780323067942000547 main
C20090551288 B9780323067942000298 main
C20090551288 B9780323067942000602 main
C20090551288 B978032306794200047X main
C20090551288 B9780323067942000250 main
C20090551288 B9780323067942000638 main
C20090551288 B9780323067942000316 main
C20090551288 B9780323067942000286 main
C20090551288 B9780323067942000560 main
C20090551288 B9780323067942000341 main
C20090551288 B9780323067942000766 main
C20090551288 B9780323067942000754 main
C20090551288 B9780323067942000122 main
C20090551288 B9780323067942000626 main
więcej podobnych podstron