C
ha
pt
er
291
42
Judy S. Blebea, MD
Bone Tumors
1. What radiographic features should be considered when evaluating a suspected bone
tumor?
When evaluating a suspected bone tumor, morphologic features, periosteal reaction, location in a bone (epiphysis,
metaphysis, diaphysis), distribution within the skeleton (axial vs. appendicular), presence of tumor matrix, and soft tissue
mass should be considered. Morphologic features to consider are the pattern of bone destruction and the size, shape,
margins, and zone of transition of the lesion. A lesion with a sharp border suggests a nonaggressive or benign lesion,
whereas a poorly defined margin, especially one associated with cortical destruction, favors malignancy. Periosteal
reaction reflects the rate of growth of the underlying lesion. Slow-growing lesions may produce a laminated periosteal
reaction with uniform, wavy layers. Malignant lesions that grow in spurts can produce an “onion-skin” pattern, whereas
aggressive lesions with rapid growth are associated with a “sunburst” or “hair-on-end” periosteal reaction. Codman
triangle is the uplifting of the periosteum in a triangular configuration and can be seen with benign and malignant
lesions.
2. How do cartilage tumor matrix and neoplastic bone matrix differ?
Cartilage matrix is typically ringlike, flocculent, or flecklike—in the shape of rings and arcs—whereas
neoplastic bone matrix is typically cloudlike, amorphous, or ivory-like. The detection of tumor matrix can be
helpful in recognizing the etiologic factor of the underlying lesion—that is, whether it is osseous or cartilaginous
in origin.
3. Which imaging study is most useful in arriving at an accurate differential diagnosis
for a bone tumor?
Plain radiography is the first step in detecting and diagnosing a bone tumor. Plain films should also be obtained
initially, even with suspected soft tissue tumors, to identify possible underlying bone involvement or the presence
of calcifications.
4. What is the role of magnetic resonance imaging (MRI) and computed tomography
(CT) in the evaluation of musculoskeletal tumors?
MRI is the most important diagnostic test for local staging and preoperative planning of primary bone and soft tissue
tumors. It is also useful for monitoring the response to chemotherapy or radiation therapy and detecting postoperative
tumor recurrence. CT may be helpful in the detection of tumor matrix and the location of the nidus in a suspected
osteoid osteoma. CT is also used for percutaneous image-guided biopsy of bone tumors.
5. What are some tumor features evaluated with MRI? Can MRI be used to distinguish
between benign and malignant tumors?
The tumor location, extent, and relationship to the neurovascular bundle and the presence of skip lesions and
joint involvement are important features that are assessed with MRI and help to determine the stage of the
tumor and to plan a surgical approach. Although MRI may help in the assessment of the aggressiveness of a
lesion and in the recognition of certain “pathognomonic” lesions, it cannot be used to distinguish reliably between
benign and malignant tumors, and is generally nonspecific in determining tumor cell type. Biopsy of the lesion is
often required.
Key Points: Plain Radiographic Features to Assess for Bone Tumors
1. Morphologic features and pattern of bone destruction, zone of transition
2. Periosteal reaction
3. Location in the bone and distribution in the skeleton
4. Presence of tumor matrix
5. Presence of a soft tissue mass
292
Bone Tumors
6. What is the role of intravenous gadolinium contrast enhancement in MRI of
musculoskeletal tumors?
There is some controversy about the need for intravenous contrast enhancement during pretherapy MRI for a patient
with a suspected musculoskeletal tumor. Contrast enhancement may be used to help distinguish tumor margins and
assess tumor vascularity. Its use may also help distinguish malignant viable tissue from inflammatory changes and
necrosis for preoperative biopsy planning. For a follow-up or post-therapy MRI evaluation, contrast enhancement can be
helpful to assess the patient’s response to chemotherapy, to determine the presence of a fluid collection postoperatively,
and to detect tumor recurrence.
7. What is the staging system adopted by the Musculoskeletal Tumor Society, and what
three features form the basis of this staging system?
The Musculoskeletal Tumor Society has adopted the Enneking staging system. Grade, local extent, and presence of
metastases are the three features assessed with this system.
8. Which primary bone tumors tend
to involve the epiphysis most
commonly?
Chondroblastoma and giant cell tumors tend
to involve the epiphysis most commonly.
Chondroblastoma is a benign lesion that is typically
well defined and located in the epiphysis. Although
benign, chondroblastomas can be locally invasive
and metastasize to the lungs. A giant cell tumor
usually arises in the metaphyseal region and
extends to involve the epiphysis. Giant cell tumors
are eccentrically located lesions with a nonsclerotic
zone of transition that typically occurs after
closure of the growth plate (
). A clear cell
chondrosarcoma may also occur in the epiphyseal
region.
9. What is the difference between a
nonossifying fibroma and a fibrous
cortical defect?
Both entities are benign, usually asymptomatic,
well-defined cortical-based lesions with sclerotic
borders seen in the metaphysis or diametaphysis
of long bones, and are identical in their histology.
They differ only in size. Fibrous cortical defects are
smaller (<2 cm), whereas nonossifying fibromas
are larger (>2 cm); both are usually detected
incidentally on radiographs in children and often
subsequently heal with sclerosis.
10. What is the most common malignant tumor involving the skeleton?
Metastases are the most common malignant skeletal tumors.
11. What is the most common primary malignant bone tumor in adults?
Multiple myeloma represents approximately 1% of all malignant diseases and about 10% to 15% of hematologic
malignancies. The excessive proliferation of abnormal plasma cells can result in the formation of a single lesion
(plasmacytoma) or multiple lesions (multiple myeloma).
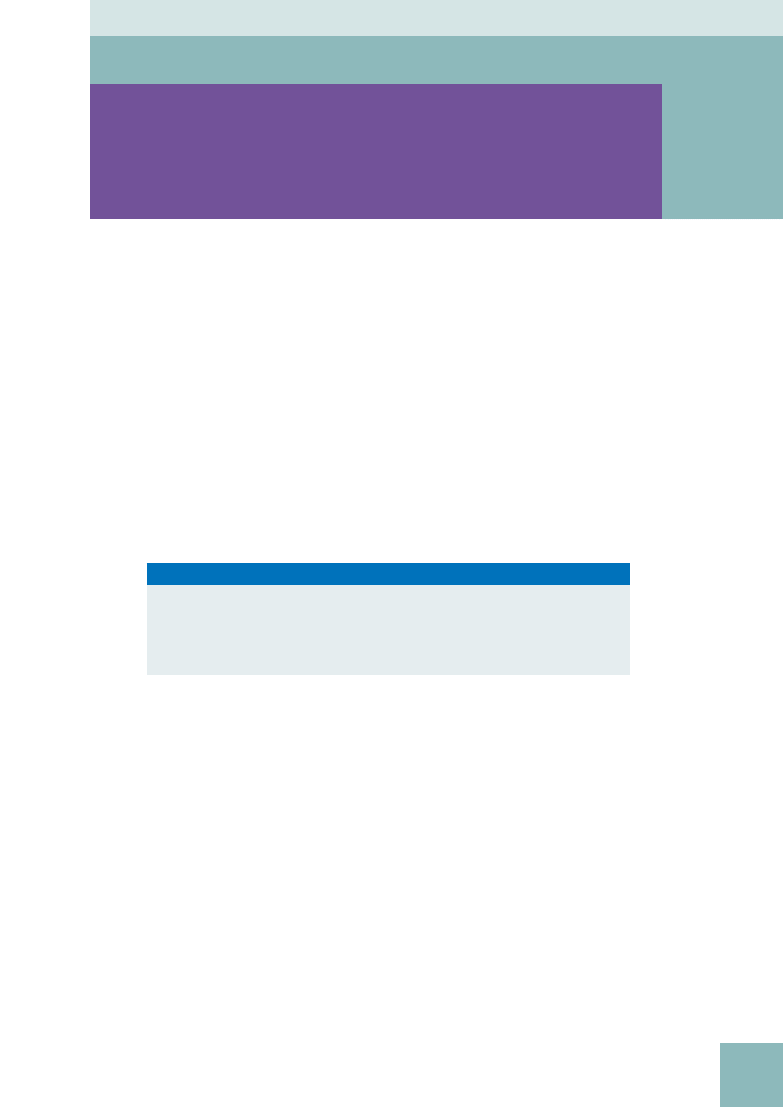
Figure 42-1.
Plain film anteroposterior radiograph of the ankle shows
a geographic lesion that extends to the epiphyseal region in the distal
tibia. In this patient with closed growth plates, the most likely diagnosis
is giant cell tumor.
Key Points: Primary Bone Tumors in the Epiphyseal Region
1. Chondroblastoma
2. Giant cell tumor
3. Clear cell chondrosarcoma
Bone Tumors
293
musculoskeleTal radiology
12. If the diagnosis of multiple myeloma is suspected, what radiographic evaluation
should be performed?
A skeletal survey is usually obtained. Approximately 75% of patients with multiple myeloma have positive radiographic
findings with “punched-out” osteolytic lesions that have discrete margins and uniform size. Multiple compression
fractures can also be seen. MRI is very sensitive for detecting the presence of marrow lesions and may help in
determining tumor extent.
13. What are the most common primary neoplasms that metastasize to bone?
A few primary tumors account for most metastatic bone lesions. Cancers most likely to metastasize to bone
include prostate, breast, kidney, thyroid, and lung, and are remembered by the mnemonic PB (lead) KetTLe. Other
primary tumors that can metastasize to bone include colon, rectum, stomach, and bladder. The axial skeleton is
seeded more than the appendicular skeleton because of the presence of red bone marrow. It is rare to have bone
metastases below the elbow or knee. Lytic bone metastases must have destroyed 30% to 50% of the bone to
be seen on radiographs. Nuclear medicine bone scans are more sensitive than radiographs for the detection of
metastatic bone disease.
14. Which tumors can give rise to lytic, expansile, “blown-out” metastases of bone?
Bone metastases from renal cell carcinoma and thyroid cancer can show this pattern. Bone metastases from malignant
melanoma may be expansile as well.
15. What is the second most common primary bone tumor after multiple myeloma?
Osteosarcoma is the second most common primary bone tumor after multiple myeloma (
). About 75% of
osteosarcoma lesions occur around the knee and typically arise in the metaphyseal region. The peak incidence is in the
second and third decades, and there is a smaller second peak in patients older than 50 years; this later peak has more
pelvic and craniofacial involvement. Osteosarcoma can develop after radiation exposure, with an average latent period
of 11 years.
16. Which type of tumor can manifest with bone pain,
swelling, tenderness, fever, and increased sedimentation
rate, mimicking an infection?
Ewing sarcoma is a malignant round cell tumor with a predilection for the long
bones and pelvis. Plain films may show a permeative or moth-eaten pattern
of bone destruction with an onion-skin type of periosteal reaction and an
associated soft tissue mass.
17. Where do sarcomas most commonly metastasize?
Sarcomas tend to undergo hematogenous spread, with pulmonary metastases
being the most common.
18. What is the most common benign skeletal neoplasm?
Osteochondroma is the most common benign skeletal neoplasm (
This lesion accounts for 20% to 50% of benign bone tumors and 10% to 15%
of all bone tumors. Osteochondromas occur most commonly in the first 2
decades of life, arise from the metaphysis pointing away from the joint, and can
be either flattened (sessile) or stalklike. There is usually cessation of growth of
the osteochondroma after closure of the growth plate. Osteochondromas can
occur after radiation therapy in children and may present with pain because of
mechanical irritation or fracture.
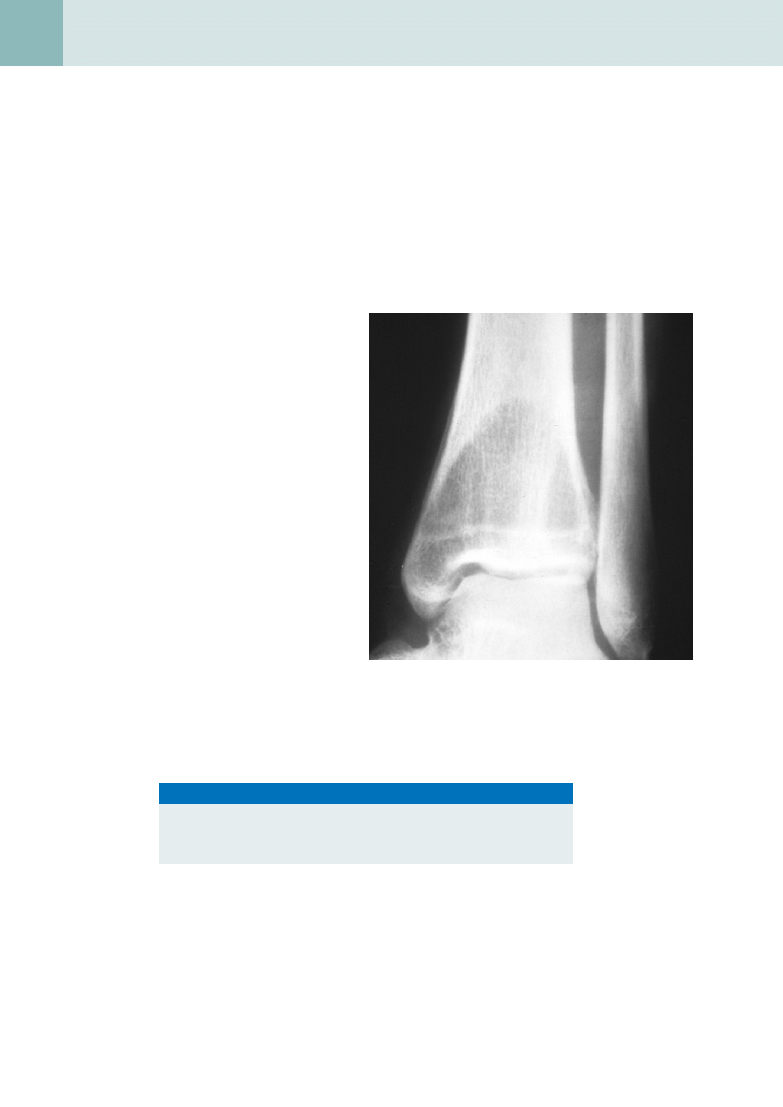
Figure 42-2.
Plain film radiograph shows exuberant bone formation in
this osteosarcoma.
Figure 42-3.
A sessile bony
protuberance is noted arising from the
femur on this plain film radiograph;
this represents an osteochondroma.
Osteochondromas are the most common
benign skeletal neoplasm.
294
Bone Tumors
19. Which clinical and radiographic
features suggest malignant
degeneration of an
osteochondroma?
Features suggesting malignant degeneration
include pain, growth after closure of the growth
plate, bony destruction, thickened cartilage
cap, and soft tissue mass. The risk of malignant
transformation of a solitary osteochondroma is
approximately 1%, whereas the risk of hereditary
multiple osteochondromatosis is much higher
and may be 25% to 30%. A sessile lesion is
more likely to degenerate, usually undergoing
malignant transformation to a chondrosarcoma
(
).
20. What is the most common benign
bone tumor of the hand? Where
else may these lesions occur, and
what are the features of malignant
transformation?
An enchondroma is the most common benign
bone tumor of the hand. Small, peripheral
enchondromas of the hand are usually well-
defined lytic lesions that are typically benign,
but may be detected as a result of pathologic
fracture. Solitary enchondromas can also occur
in the long bones and are usually oval in shape
with central calcifications (
). Features
suggestive of malignant degeneration include
an enlarging painful lesion with progressive
destruction of the chondroid matrix and an
expansile soft tissue mass.
21. Which primary bone tumor has the
characteristic history of pain at
night that is relieved by aspirin?
Osteoid osteoma is a primary bone tumor that
has a characteristic history of pain at night that
is relieved by aspirin. The classic radiographic
appearance of this lesion is a round or oval
lucent lesion, which represents the nidus,
that typically measures less than 1 cm and is
surrounded by a zone of bone sclerosis with
cortical thickening.
22. What is fibrous dysplasia?
Fibrous dysplasia is a developmental anomaly of
bone that usually manifests as a solitary lesion
with focal bone expansion, cortical thinning or
thickening, and a “ground-glass” appearance.
Patients with these lesions may be asymptomatic
or present with pathologic fracture. Polyostotic
fibrous dysplasia with associated endocrine
dysfunction that is usually manifested as
precocious female sexual development is known
as McCune-Albright syndrome.
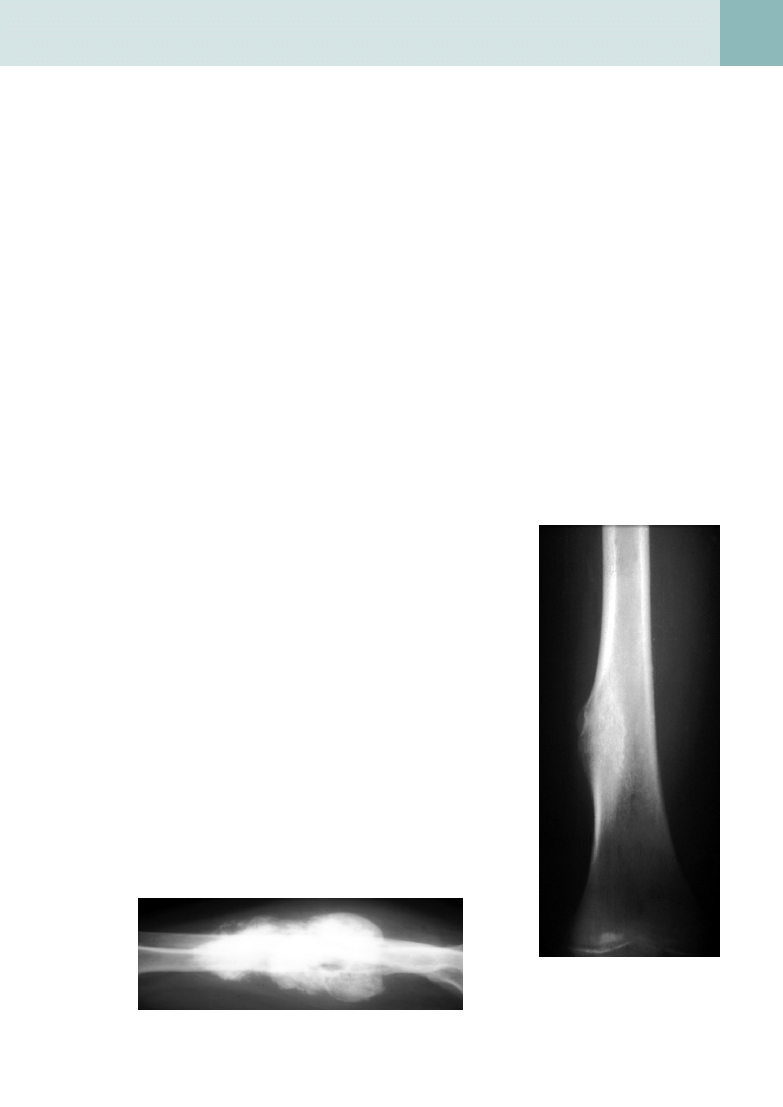
Figure 42-4.
Axial T2-weighted MR image permits the evaluation of
the extent of this biopsy-proven chondrosarcoma. This image is helpful
for staging and preoperative planning.
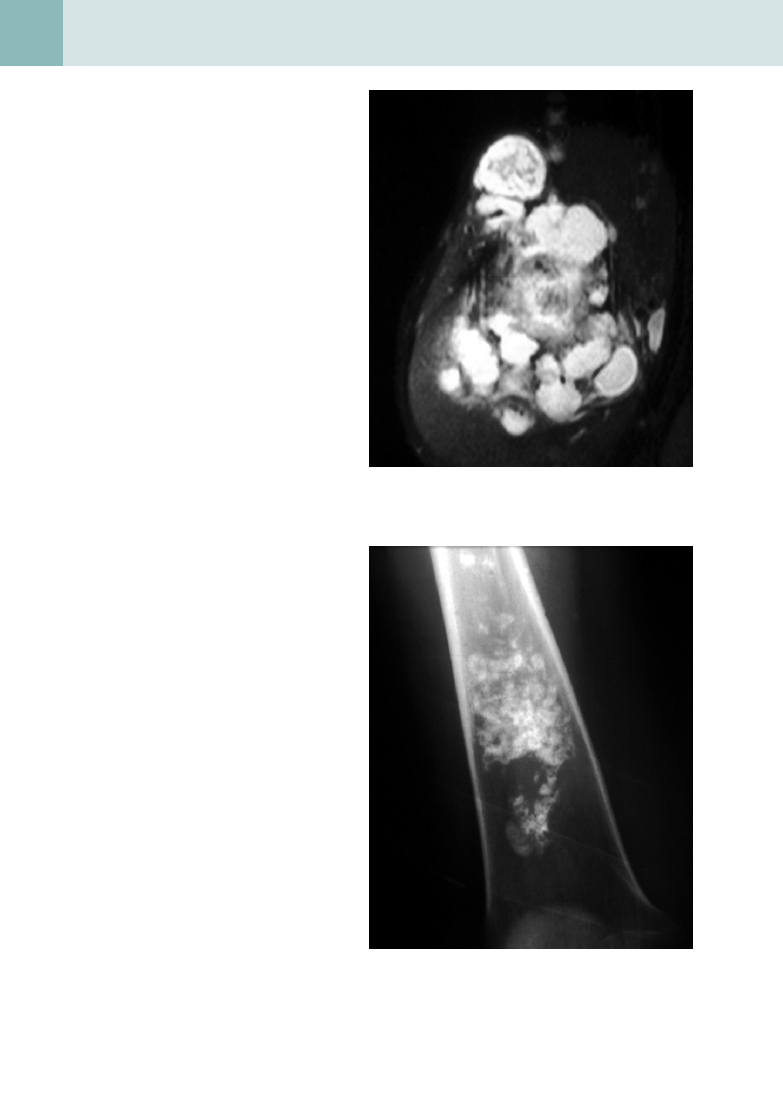
Figure 42-5.
Anteroposterior view of the femur shows the presence of
cartilage matrix, which is typically ringlike, flocculent, or flecklike, in this
patient with an enchondroma.
Bone Tumors
295
musculoskeleTal radiology
23. Which of the following has an increased incidence of skeletal malignancy: high-dose
radiation therapy, bone infarction, Paget disease, or chronic osteomyelitis?
All of these entities have an increased incidence of skeletal malignancy; osteosarcoma and fibrosarcoma are the most
common forms of malignant degeneration.
24. What is a bone island?
A bone island, or enostosis, is a benign lesion that appears radiographically as an oval or round sclerotic focus that may
have radiating bone spicules from the center of the lesion. Bone islands are typically asymptomatic, are incidentally
discovered, and usually do not show increased radiotracer uptake on a nuclear medicine bone scan.
25. What is the most common location for a skeletal hemangioma?
The most common site of involvement is the spine, particularly the thoracic segment. Most vertebral hemangiomas are
small and asymptomatic, with a coarse, vertical trabecular pattern or corduroy appearance in the vertebral body on plain
films or CT.
B
ibliography
[1] A. Greenspan, Differential Diagnosis of Tumors and Tumor-like Lesions of Bones and Joints, Lippincott Williams & Wilkins, Philadelphia,
1998.
[2] T. Rand, P. Ritschl, S. Trattnig, et al., Imaging of Bone and Soft Tissue Tumors, Springer Verlag, New York, 2001.
[3] D. Resnick, Diagnosis of Bone and Joint Disorders, fourth ed., Saunders, Philadelphia, 2002.
Key Points: Imaging of Bone Tumors
1. Order a plain film first.
2. Use MRI for staging and preoperative planning.
3. Use CT for image-guided biopsy and detection of the nidus of an osteoid
osteoma or pulmonary metastases.
4. Use MRI for follow-up to detect response to therapy or tumor recurrence.
Document Outline
- Bone Tumors
- What radiographic features should be considered when evaluating a suspected bone tumor?
- How do cartilage tumor matrix and neoplastic bone matrix differ?
- Which imaging study is most useful in arriving at an accurate differential diagnosis for a bone tumor?
- What is the role of magnetic resonance imaging (MRI) and computed tomography (CT) in the evaluation of musculoskeletal tumors?
- What are some tumor features evaluated with MRI? Can MRI be used to distinguish between benign and malignant tumors?
- What is the role of intravenous gadolinium contrast enhancement in MRI of musculoskeletal tumors?
- What is the staging system adopted by the Musculoskeletal Tumor Society, and what three features form the basis of this staging system?
- Which primary bone tumors tend to involve the epiphysis most commonly?
- What is the difference between a nonossifying fibroma and a fibrous cortical defect?
- What is the most common malignant tumor involving the skeleton?
- What is the most common primary malignant bone tumor in adults?
- If the diagnosis of multiple myeloma is suspected, what radiographic evaluation should be performed?
- What are the most common primary neoplasms that metastasize to bone?
- Which tumors can give rise to lytic, expansile, “blown-out” metastases of bone?
- What is the second most common primary bone tumor after multiple myeloma?
- Which type of tumor can manifest with bone pain, swelling, tenderness, fever, and increased sedimentation rate, mimicking an infection?
- Where do sarcomas most commonly metastasize?
- What is the most common benign skeletal neoplasm?
- Which clinical and radiographic features suggest malignant degeneration of an osteochondroma?
- What is the most common benign bone tumor of the hand? Where else may these lesions occur, and what are the features of malignanttransformation?
- Which primary bone tumor has the characteristic history of pain at night that is relieved by aspirin?
- What is fibrous dysplasia?
- Which of the following has an increased incidence of skeletal malignancy: high-dose radiation therapy, bone infarction, Paget disease, or chronic osteomyelitis?
- What is a bone island?
- What is the most common location for a skeletal hemangioma?
- Bibliography
Wyszukiwarka
Podobne podstrony:
C20090551288 B9780323067942000055 main
C20090551288 B9780323067942000407 main
C20090551288 B9780323067942000225 main
C20090551288 B9780323067942000432 main
C20090551288 B9780323067942000547 main
C20090551288 B9780323067942000298 main
C20090551288 B9780323067942000602 main
C20090551288 B978032306794200047X main
C20090551288 B9780323067942000250 main
C20090551288 B9780323067942000638 main
C20090551288 B9780323067942000316 main
C20090551288 B9780323067942000286 main
C20090551288 B9780323067942000560 main
C20090551288 B9780323067942000341 main
C20090551288 B9780323067942000390 main
C20090551288 B9780323067942000766 main
C20090551288 B9780323067942000754 main
C20090551288 B9780323067942000122 main
C20090551288 B9780323067942000626 main
więcej podobnych podstron