
Principles of Neurosurgery,
edited by Robert G. Grossman. Rosenberg © 1991'
Published by Raven Press, Ltd., New York.
CHAPTER 11
Trigeminal and Glossopharyngeal Neuralgia
and Hemifacial Spasm
Ronald I. Apfelbaum
Trigeminal and Glossopharyngeal Neuralgia, 223
Incidence, 223
Etiology and Pathology, 223
Symptoms, 224
Signs, 225
Diagnostic Tests, 225
Treatment, 226
Outcome, 231
Hemifacial Spasm, 231
Incidence, 231
Etiology and Pathology, 231
Symptoms, 232
Signs, 232
Diagnostic Tests, 232
Treatment, 233
Outcome, 233
References, 234
TRIGEMINAL AND
GLOSSOPHARYNGEAL NEURALGIA
Incidence
The true incidence of trigeminal neuralgia is not known,
but it has been estimated from some limited epidemio-
logic studies that approximately 5,000 to 10,000 new
cases occur annually in the United States (1). Women
are more commonly afflicted than men, by a margin of
approximately three to two. Glossopharyngeal neuralgia
is much less common, occurring only once for every 70
to 100 cases of trigeminal neuralgia (2).
Etiology and Pathology
Ancient medical writings describe variations in head
and face pain that probably included cases of trigeminal
neuralgia. The first full description of this condition by a
physician is attributed to John Locke in 1677. Nicholas
Andre is credited with recognition of trigeminal neural-
gia as a definite clinical entity in 1756; in 1773 John
Fothergill published a similar account, unaware of the
R. I. Apfelbaum: Division of Neurological Surgery, The Uni-
versity of Utah, School of Medicine, Salt Lake City, Utah
84132.
French physician's earlier contribution (3). From these
beginnings, gradually increasing recognition of trigemi-
nal neuralgia ensued. Because the condition presents as a
well-defined clinical entity and because patients afflicted
with this condition suffer so greatly, a great deal of atten-
tion has been focused on studying the problem and at-
tempting to treat it.
Glossopharyngeal neuralgia, on the other hand, is a
much less common problem and has been recognized
only fairly recently as a distinct clinical entity. Weisen-
berg in 1910 first reported this symptom complex in a
patient with a tumor in the cerebellopontine angle; a
report by Sicard and Robineau in 1920 followed. Harris
first used the term glossopharyngeal neuralgia in 1921.
White and Sweet called attention to the involvement of
some of the vagal fibers and suggested the term vagoglos-
sopharyngeal neuralgia in 1969 (2). Though technically
more precise, this term has not gained widespread use.
In attempting to explain the etiology and pathophysiol-
ogy of these conditions, various authors have hypothe-
sized about the possible roles of trauma, dental pathol-
ogy and suppuration, clinical and subclinical viral
infections, congenital and acquired skull base distor-
tions, demyelinating processes, neoplasms, vascular
compressive lesions, and intrinsic brainstem pathway
dysfunction. Many theories have been advanced and
have enjoyed brief popularity before falling by the way-
side. Thus, for example, when studies demonstrated a.
223

224 / CHAPTER 11
frequent occurrence of herpes virus within the gasserian
ganglion, the virus was advocated as the etiologic agent
of trigeminal neuralgia—until control studies demon-
strated an equally high incidence in asymptomatic indi-
viduals.
The one consistent observation, which holds true both
for patients with demyelinating disease and for those
without, is that there are segmental pathological changes
at the root entry zone of the nerve affecting the centrally
myelinated portion of the nerve (4-7). Central myelin
(derived from oligodendroglial cells) extends a few milli-
meters from the brainstem into the nerve before being
replaced by myelin formed by Schwann cells (8). In elec-
tron-microscopic studies there has been consistent de-
myelination in this area, as well as axonal disruption. In
patients suffering from multiple sclerosis who also have
trigeminal neuralgia, demyelinating plaques are invari-
ably located in this region (and may also be found in
other portions of the trigeminal pathway within the
brainstem).
Walter Dandy first observed the high incidence of vas-
cular channels impinging upon the root entry zone of the
nerve and suggested that this might be the cause of tri-
geminal neuralgia (9). It was not until Dr. Peter Jannetta
applied the operating microscope to the systematic study
of these problems that the truly high incidence of such
root entry zone compression was accurately appreciated
(over 97 percent) (10,11). Several postmortem studies
have confirmed the abnormally high incidence of vascu-
lar lesions in patients suffering from trigeminal neuralgia
as compared to control populations (12-14). This com-
pression appears to be the cause of the demyelination
and is accepted by most, but not all, specialists in this
field as the cause of the symptoms in most patients. The
major exception is in patients with multiple sclerosis,
who of course have intrinsic neural disease.
The anatomical derangement in the nerve apparently
alters the physiology in an as yet incompletely under-
stood manner. Gardner has hypothesized the develop-
ment of a "short circuit" in the nerve at the site of de-
myelination, resulting in touch sensation carried by the
larger afferent fibers actuating thinner pain fibers (15).
Loeser, Calvin, and Howe have suggested that antidro-
mic reflectance of a normal nerve impulse sets up a re-
verberating circuit, explaining how a light touch can trig-
ger a painful paroxysm (16,17).
Because of its rarity, similar pathological studies have
not been performed in patients with glossopharyngeal
neuralgia, but the conditions are otherwise analogous
and are thought to have the same physiological basis.
Symptoms
These conditions are characterized by a very consis-
tent clinical pattern among patients. Patients will experi-
ence brief repetitive paroxysmal spasms of unilateral
pain of extreme intensity, confined entirely to the terri-
tory of one or more divisions of the trigeminal or the
glossopharyngeal nerve. The pain is frequently described
as a "bolt of lightening" or an electric shock-like phe-
nomenon, and patients will often, in describing the pain,
make a characteristic gesture, flinging open a closed
hand to demonstrate the rapid onset and spread of the
pain.
The pain may occur spontaneously but is often trig-
gered by nonpainful tactile stimuli, usually, but not in-
variably, within the territory of the affected nerve. Thus,
in the case of trigeminal neuralgia, the pain may be acti-
vated by a breeze on the face, touching the face lightly,
chewing, talking, or eating. Common activities, such as
face washing, hair combing, and tooth brushing, become
difficult or impossible. The attack of pain is always uni-
lateral, with an approximately 60 to 40 right to left pre-
dominance. Some patients may be unfortunate enough
to suffer from this condition bilaterally (1 to 3 percent),
but the pain is neither simultaneous nor synchronous on
the two sides.
Most patients will not have any underlying back-
ground pain. But an occasional patient may complain of
a burning or drawing feeling after the sharp paroxysm
subsides, and some will note a prickling, burning or
throbbing sensation before the tic starts (18). In obtain-
ing a history, one must also be careful that repetitive
paroxysms occurring in long volleys are not mistaken for
one steady, long pain.
When the diagnosis is doubtful (usually because the
patient is a poor historian) one should inquire about the
patient's behavior during the pain attacks. Patients with
trigeminal neuralgia tend to remain as immobile as possi-
ble and to guard against any contact with the exposed
area. This is in contradistinction to other types of pain
such as cluster headache (Horton's cephalgia), in which
patients tend to pace or throw themselves about, often
crying out. These latter patients may often place hot or
cold compresses on the face or massage the affected area
in an attempt to diminish the pain.
Both trigeminal and glossopharyngeal neuralgia are
conditions that seem to occur with increasing frequency
with advancing age. Contrary to some descriptions, how-
ever, they are not exclusively diseases of elderly patients
and may occur as early as the teenage years in rare in-
stances. The peak age of onset is in midlife, during the
fifth to sixth decades.
In the natural history of trigeminal neuralgia, remis-
sions are common and may last for extended periods of
time. With increased duration of the illness, however,
remissions tend to become shorter and periods of exacer-
bation longer.
Another useful characteristic in the differential diag-
nosis is the infrequent occurrence of nocturnal pain.
Many patients are able to find a comfortable position
TRIGEMINAL AND GLOSSOPHARYNGEAL NEURALGIA AND HEMIFACIAL SPASM / 225
and get adequate rest. This condition therefore is not a
chronic pain but rather an acute pain syndrome occur-
ring repetitively. Narcotic analgesics are impotent in this
situation, and thus it is extremely uncommon to find a
patient who is habituated or even a frequent user of nar-
cotics.
There is a well-established association between trigemi-
nal neuralgia and multiple sclerosis. In a large series of
patients with multiple sclerosis, 1 to 2 percent will be
found to have trigeminal neuralgia (19). Conversely, a
similar percentage of patients suffering from trigeminal
neuralgia will be found to have multiple sclerosis. As
previously mentioned, in these patients there is a demye-
linating plaque at the root entry zone of the trigeminal
nerve. The site of pathology, therefore, is in exactly the
same area as that found in trigeminal neuralgia pro-
duced by vascular compression, but in these patients the
disease is intrinsic within the nerve rather than due to an
extrinsic cause. The clinical symptoms are also identical.
The association of glossopharyngeal neuralgia and multi-
ple sclerosis has been documented only rarely.
The symptoms of glossopharyngeal neuralgia are gen-
erally similar to those of trigeminal neuralgia but have
some additional features. The pain resembles that of tri-
geminal neuralgia and occurs as brief paroxysms in the
throat or ear. A higher number of patients, however, ex-
perience a dull, aching, or burning feeling. As in trigemi-
nal neuralgia, the episodes of pain are usually triggered,
the common provocative maneuvers being swallowing,
chewing, coughing, or talking. Patients may experience
paroxysms of coughing with their attacks of pain. Syn-
cope has also been reported, but appears to be a very
uncommon associated symptom. It may be due to hyper-
sensitivity of the carotid sinus nerve, producing asystole.
Signs
The diagnosis of trigeminal neuralgia is made by his-
tory. On very close examination with careful attention
being directed to facial cutaneous sensibility, abnormali-
ties may be encountered in as many as 25 percent of
patients; these are minimal changes, which will not nor-
mally be detected on routing neurologic examination.
Of course, if the patient has had prior destructive sur-
gery, appropriate abnormalities may exist.
Tumors in the cerebellopontine angle, which may be a
cause of trigeminal or glossopharyngeal neuralgia, may
produce deficits in several of the lower cranial nerves,
cerebellar dysfunction, and papilledema. These signs
may be detected on a careful neurologic examination.
Diagnostic Tests
There is no specific test that will establish the diagnosis
of trigeminal neuralgia. The diagnosis rests entirely upon
a careful and adequate history. A magnetic resonance
imaging (MRI) scan should be performed, with particu-
lar attention paid to the affected nerve in the middle and
posterior fossa, on every patient who has this problem so
as to exclude an underlying neoplasm. Multiple sclerosis
will usually be readily detected on the MRI scan, but if
doubt exists other appropriate tests may include audi-
tory and visual evoked responses and spinal fluid analy-
sis to help establish the diagnosis.
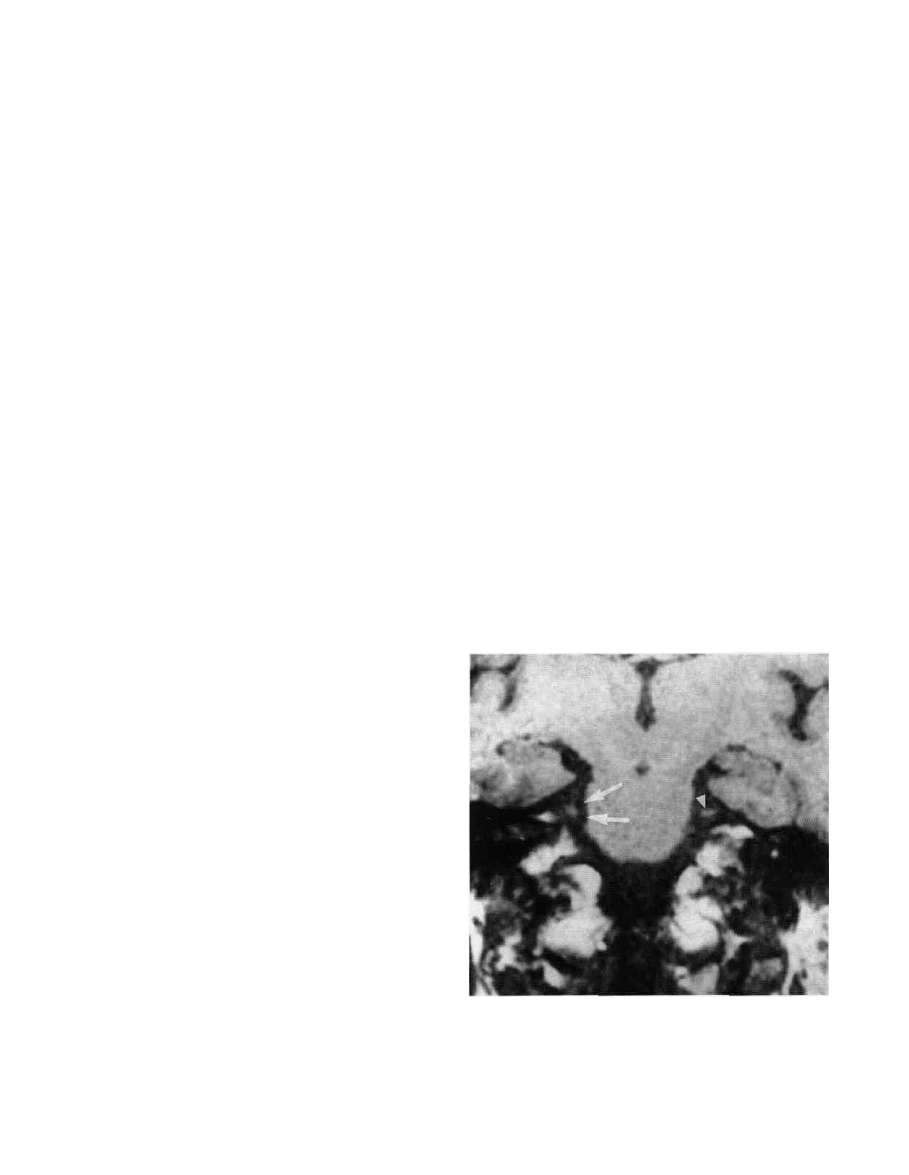
In addition to excluding neoplasms and ruling out
multiple sclerosis, MRI scanning in trigeminal neuralgia
has demonstrated the flow voids of vascular loops adja-
cent to the root entry zone of the affected nerve, with
distortion of the nerve. Abnormal uptake of gadolinium
in the compressed region also may be seen. These
changes in the preganglionic segment of the trigeminal
nerve are best viewed on coronal T,-weighted sequences
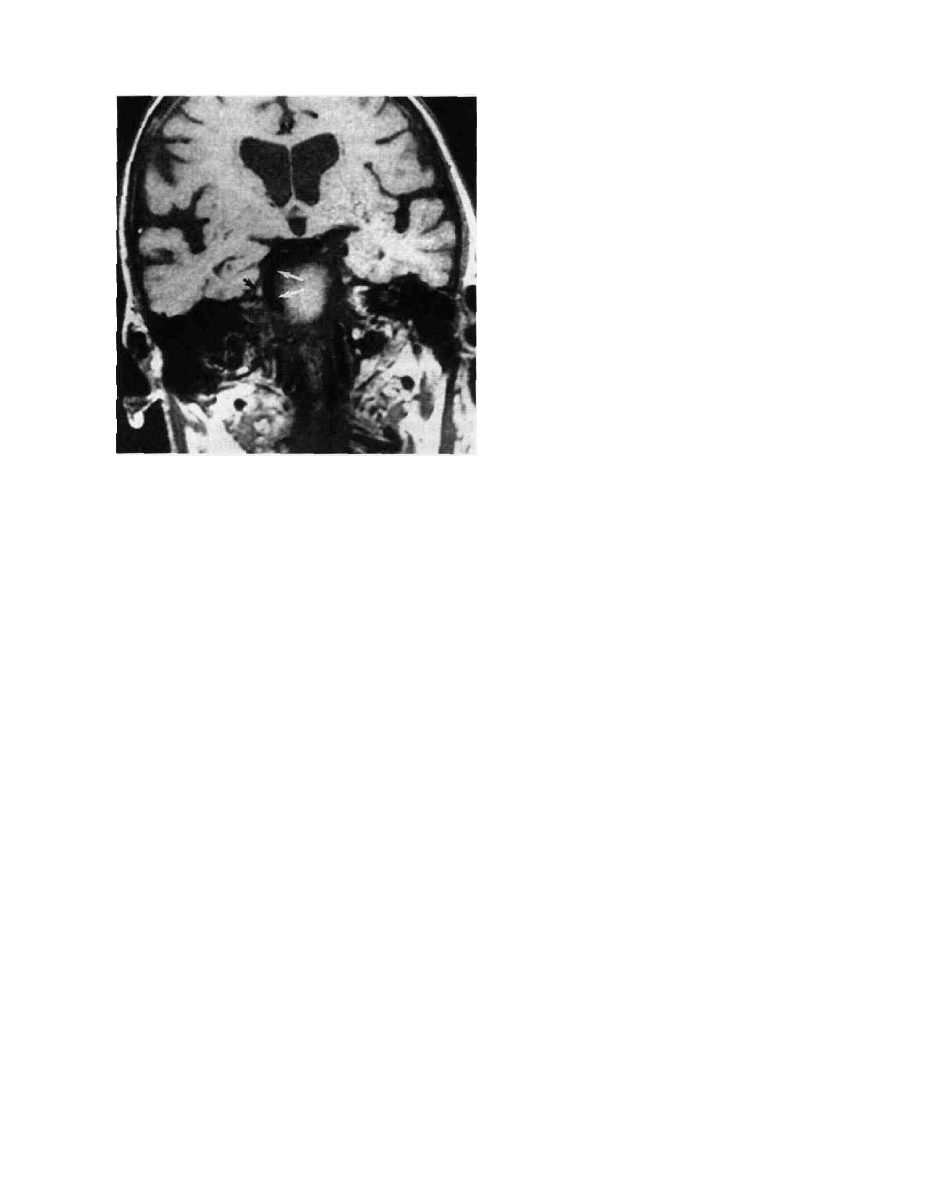
(Fig. 1) (20). Scanning also alerts the surgeon to the pres-
ence of dolichoectatic major vessels (Fig. 2), aneurysms,
and vascular malformations. All are infrequent causes of
vascular compression but ones that may require differ-
ent treatment or surgical strategics.
In glossopharyngeal neuralgia, in addition to the
above, a useful diagnostic test is the application of a topi-
cal solution of 10 percent cocaine to the oropharynx.
This will provide several hours of relief, during which the
majority of patients with this problem will be able to eat
and drink without experiencing pain. This time helps to
establish the diagnosis and also aids in predicting the
outcome of surgical treatment.
FIG. 1. Coronal T1-weighted MRI demonstrating two flow
voids (arrows) adjacent to and distorting the right pregan-
glionic segment of the trigeminal nerve. Note the normal ap-
pearing left preganglionic segment of trigeminal nerve (arrow
head) for comparison.
226 / CHAPTER 11
FIG 2 Coronal T1 -weighted MRI demonstrating a large, do-
lichoectatic basilar artery (winte arrows) compressing and
distorting the preganglionic segment of the left trigeminal
nerve (smaller black arrow).
Treatment
The goal of any treatment is to render the patient pain
free at a tolerable level of side effects. The treatment
must provide reliable and consistent pain control so that
not only is the pain relieved but also the fear of pain
recurrence, which can dominate a patient's life. Partial
control is not a satisfactory goal in this day and age.
Trigeminal Neuralgia: Medical
The management of trigeminal neuralgia (21,22) is
first and foremost medical, with surgical treatment re-
served for those patients who are refractory to medical
treatment or who develop toxicity. Two drugs, pheny-
toin (Dilantin®) and carbamazepine (Tegretol®), are the
mainstays of treatment (23). Many physicians prefer to
start with phenytoin because of its lower toxicity, al-
though it is effective only in about one-half of patients
and has a relatively high failure rate after a period of
time. After an appropriate loading dose, 300 to 400 mg a
day will usually be adequate if this drug is effective.
Serum phenytoin levels can be determined and dosage
adjusted to obtain a therapeutic level of 10 to 20 meg/ml.
We usually start with carbamazepine 100 mg twice a
day and increase it by 100 mg every other day until con-
trol is achieved or toxicity develops. Unlike phenytoin,
this drug has no absolute dosage range. Although some
atients may achieve control with as little as 200 mg a
day, many patients will require 1,600 mg or more. An
average dose might be 800 mg per day (200 mg q.i.d.).
This medication should be given with food or milk to
avoid gastric upset. Common subjective side effects in-
clude mental obtundation, sedation, interference with
higher cognitive functions, disequilibrium, and incoordi-
nation. These are usually dose related. Significant liver,
renal, and especially hematologic side effects also occur.
Patients should therefore have periodic blood tests, ini-
tially every two weeks and then at monthly intervals
while on the medication. The development of toxicity
may limit the use of this drug, but it is initially effective
in over 80 percent of the patients treated. Because carba-
mazepine is so effective, the patient's failure to respond
when an adequate dosage can be tolerated should alert
one to reassess the diagnosis.
Phenytoin may be added to carbamazepine and may
increase the effectiveness of the latter or allow good pain
control at a lower dose, reducing side effects. It, of
course, may be used alone in case of carbamazepine intol-
erance or toxicity. Liver function abnormalities, a cuta-
neous rash, disequilibrium, and sedation are some of the
more common side effects and may require discontinu-
ance of the drug.
Baclofen (Lioresal®) and chlorphenesin carbamate
(Maolate®) are second-order drugs that may help some
patients. In our experience they are most useful for pa-
tients who are well controlled on carbamazepine or
phenytoin but who have to stop using these medications
due to toxicity. They rarely provide significant pain con-
trol for any length of time in patients who do not re-
spond to phenytoin or carbamazepine.
Trigeminal Neuralgia: Surgical
Two types of surgical procedures, percutaneous partial
destruction of the trigeminal preganglionic rootlets and
the Jannetta microvascular decompression of the trigemi-
nal nerve via a posterior fossa craniectomy, are the
current operative procedures of choice for patients who
have become refractory or have developed toxicity to
medical therapy.
Percutaneous neurolysis may be accomplished in sev-
eral ways. These techniques have replaced peripheral
nerve sections or injections, and intracranial sections,
because a more controlled selective partial destruction of
the nerve can be produced. This achieves pain control
with some preservation of sensation and provides better
long-term results with less risk.
Percutaneous radiofrequency thermal lesioning of the
trigeminal nerve was introduced by Sweet and Wepsic in
1974 (24) as a refinement of earlier gross electrocoagula-
tion techniques of the gasserian ganglion pioneered by
Kirschner in 1931. Radiofrequency lesioning requires
only a brief hospitalization.
TRIGEMINAL AND GLOSSOPHARYNGEAL NEURALGIA AND HEMIFACIAL SPASM / 227
The procedure can be performed in the x-ray depart-
ment or in an operating theater. Neuroleptic analgesia is
utilized. The patient is sedated with droperidol 150 mg
per kg IM, and fentanyl 50 mg is given intravenously
initially. Supplemental increments of 25 mg of fentanyl
are given as needed, titrating the patient's perception of
pain against the patient's mental state to avoid obtunda-
tion. Fentanyl is a short-acting agent that facilitates good
control of the patient's discomfort, while allowing the
patient to cooperate during the procedure. Such coopera-
tion is essential for proper and safe performance of this
procedure. Some surgeons supplement the above by in-
ducing brief deeper anesthesia with methohexital (Brevi-
tal®) during the more painful moments of the procedure.
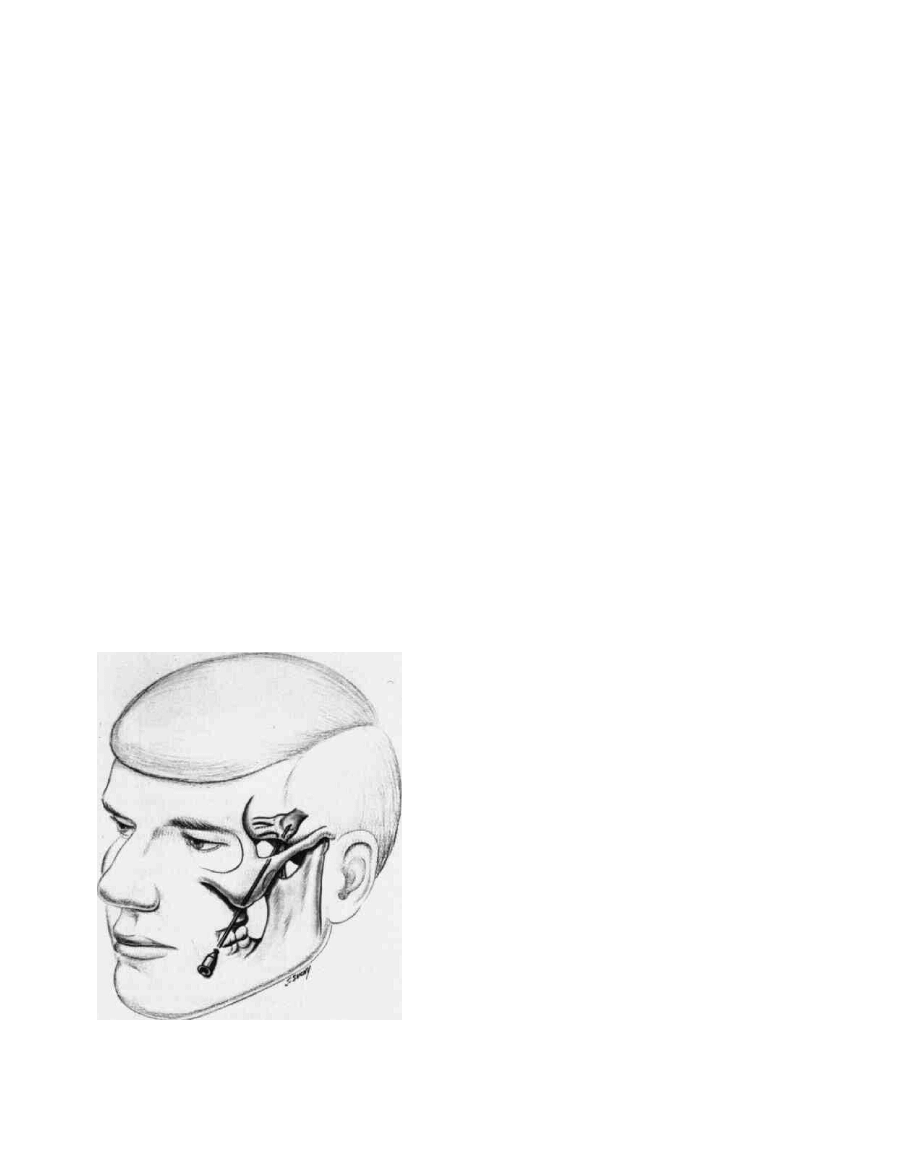
A needle electrode is inserted in the cheek approxi-
mately 2 cm lateral to the corner of the mouth and
through the foramen ovale under radiographic control,
utilizing the Hartel technique (Fig. 3) (25). Once the nee-
dle is in place, the stylet is withdrawn and an electrode is
inserted through the needle. Stimulation is then used to
localize the appropriate divisions of the trigeminal
nerve, adjusting the electrode's position as necessary.
Proper localization is achieved when the patient per-
ceives a nonpainful vibratory or paresthetic sensation in
the appropriate division at a threshold of under 0.4 volts
(50 Hz, 2.5 msec continuous pulse train). The radiofre-
quency current is then placed on the electrode, which
raises the temperature of the electrode tip, producing
some thermocoagulation of the preganglionic trigeminal
nerve fibers. After each incremental lesion, the patient is
FIG. 3. Placement of the needle through the lateral cheek
and into the gasserian ganglion for percutaneous radiofre-
quency lesioning. (From reference 51, with permission.)
tested and the procedure is terminated when moderate
or greater hypalgesia in the affected area is achieved.
Using carefully applied, small, graded increments of
heating, one can usually remove pain perception while
preserving some useful touch in the treated area, since
the thin unmyelinated pain fibers are more sensitive to
thermal destruction than the larger myelinated touch
fibers. At times the lesion will spread to adjacent divi-
sions of the nerve, producing a larger area of numbness
than desired.
This procedure can be well tolerated even by elderly or
medically debilitated patients. Patients must be aware
that this procedure will permanently alter facial sensa-
tion, producing significant numbness in 90 percent of
our patients, and that it may produce corneal anesthesia
if the first division is affected or the lesion spreads to
involve that division. Most patients are willing to accept
this small risk (18 percent experience decreased or ab-
sent corneal sensation; 2 percent corneal ulceration or
keratitis)* and can tolerate the numbness fairly well. An
occasional patient, however, will be greatly bothered by
the numbness. If there is any doubt as to a patient's abil-
ity to tolerate numbness, nerve blocks can be performed
to remove sensation temporarily so as to allow the pa-
tient to experience this numbness prior to deciding
whether or not to accept the procedure. I have found it
helpful to describe the altered facial sensation to the pa-
tient as similar to the feeling when a dental anesthetic
has partially worn off. The patient must be aware, how-
ever, that, unlike a dental anesthetic, this sensation will
be a permanent one and cannot be reversed.
More troublesome is the occurrence of dysesthetic
sensations (20 percent), which usually are fairly mild and
well tolerated but in a small percentage (4 percent) can
be quite severe and troublesome. These latter patients,
who suffer from analgesia or anesthesia dolorosa, are
bothered by constant and severe burning, itching, or
crawling sensations, which they may find as intolerable
as their initial trigeminal neuralgia pain. Unfortunately,
these sensations are refractory to treatment, although
some patients will respond to a combination of Trila-
fon 4 mg and amitriptyline hydrochloride (Elavil®) 25
mg q.i.d.
Some authors with greater experience have advocated
making less dense lesions to produce mild to moderate
rather than dense analgesia. This procedure, they claim,
is equally effective in relieving the pain but significantly
decreases the risks of corneal anesthesia and dysesthetic
sequelae (31).
Other unwanted side effects that have been reported
include the rare occurrence of intracranial infections and
* The percentages expressed here represent my personal experience
with 134 patients treated over 10 years by this technique. On analysis,
these percentages agree with many large published series (26-30).
228 / CHAPTER 11
abscesses, and injury to the third, fourth, and sixth cra-
nial nerves. Punctures of the carotid artery and cavern-
ous sinus usually are benign, but on occasion carotid
cavernous fistula and/or cerebral vascular accidents
have been reported. These latter complications, how-
ever, are all exceedingly rare.
Patients may resume full activity and diet immedi-
ately after recovery from the anesthetic and are usually
discharged the following day. There are no restrictions of
their activities after this procedure.
Percutaneous chemoneurolysis with glycerol was intro-
duced in 1981 by Hakanson (32). In this approach, pure
anhydrous glycerol (99.5 percent) is instilled into the tri-
geminal cistern under fluoroscopic control. It is not clear
whether the effect of the glycerol is due to chemical or
hyperosmotic damage to the trigeminal nerve pregan-
glionic rootlets. In any case, the effect is to produce ex-
cellent pain relief with usually only minimal sensory loss
at times none. Some patients, however, will get
significant sensory loss (4 percent), even anesthesia,
though the latter usually occurs only with sequential de-
structive procedures. In 158 patients treated with this
technique over seven years, we have only rarely observed
corneal anesthesia (4 percent) and have never seen kera-
titis develop as a sequela to the procedure. Dysesthetic
sensations are also very infrequent (3 percent) and
usually quite mild. Anesthesia dolorosa has not been re-
ported from this procedure (33).
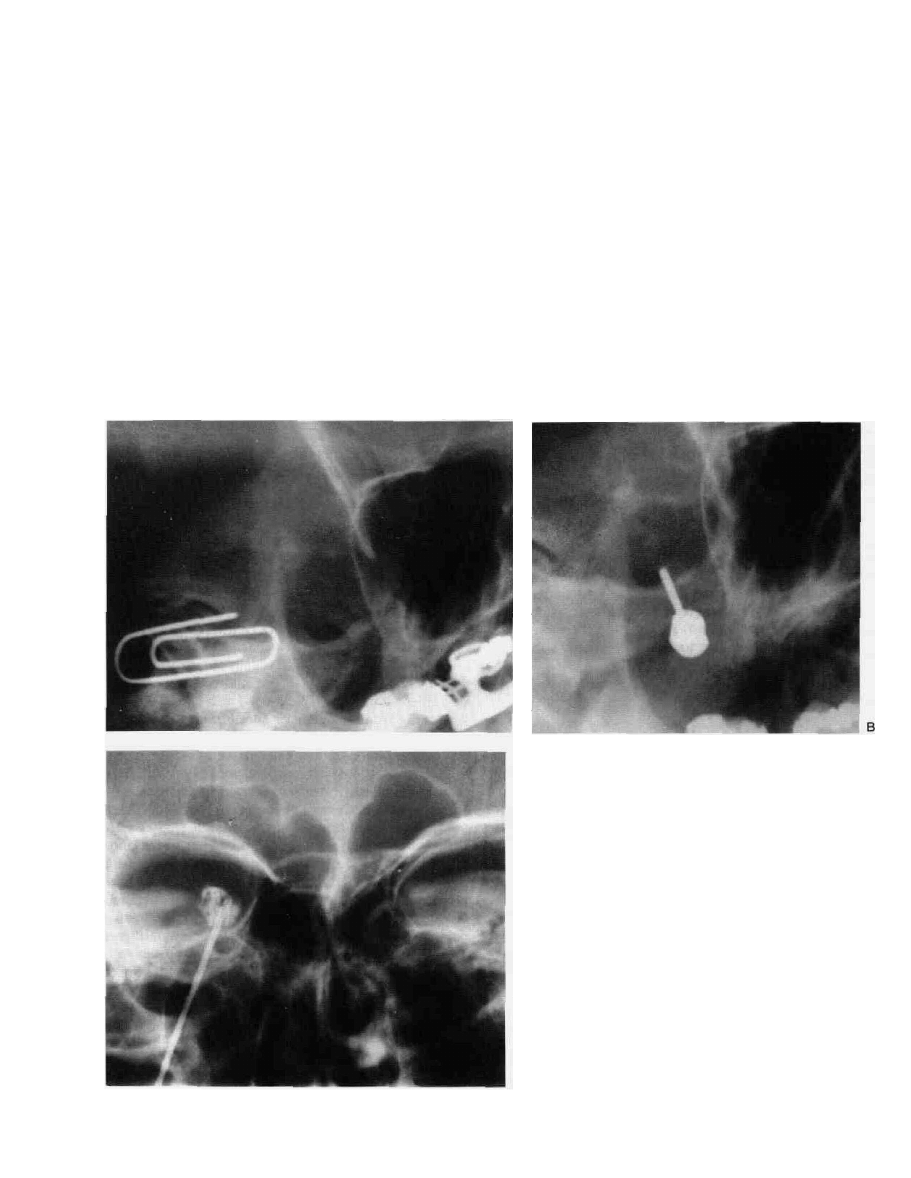
We perform the procedure in the x-ray suite, using the
same technique for puncturing the foramen ovale under
direct fluoroscopic guidance that we use for radiofre-
quency lesioning (25). The entry site, approximately 2 to
3 cm from the corner of the mouth, is selected fluoro-
scopically (Fig. 4A) by placing the patient with his neck
FIG. 4. Fiuoroscopic images during glycerol chemo-
neurolysis for trigeminal neuralgia. (A) Initial scout view
showing paper clip on skin at entrance site and end-on
view of foramen ovale. (B) Needle has now been in-
serted into the medial end of the foramen ovale, under
direct fluoroscopic imaging. (C) Trigeminal cisterno-
gram, AP projection with patient in upright position.
Preganglionic rootlets are visible as linear filling defects
within the cistern.
TRIGEMINAL AND GLOSSOPHARYNGEAL NEURALGIA AND HEMIFACIAL SPASM / 229
hyperextended and head rotated to the contralateral side
about 15 to 20 degrees. This allows visualization directly
along the needle pathway, with the foramen ovale seen
projecting over the petrous ridge.
Needle puncture and advancement through the fora-
men ovale is accomplished with the patient briefly anes-
thetized using 40 to 60 mg of methohexital. It is impor-
tant that the foramen ovale be punctured at its medial
end to properly engage the trigeminal cistern. This can
be reliably accomplished using the fluoroscopic tech-
nique described above and placing the needle through
the foramen as its progress is being monitored (Fig. 4B).
Once the needle is in place and a free flow of cerebro-
spinal fluid (CSF) is obtained, the patient is allowed to
awaken. A cisternogram is then performed by connect-
ing a J ml syringe and extension tubing filled with io-
hexol (Omnipaque®, Winthrop Pharmaceuticals, New
York) (350 mg% concentration) to the needle, tilting the
x-ray table to the vertical position, and slowly injecting
the contrast agent while fluoroscoping in the anteroposte-
rior (AP) projection. If the needle is properly placed, the
contrast will fill the small cup-shaped trigeminal cistern
(Fig. 4C), then overflow into the posterior fossa. The
cisternogram confirms the correct placement and also
allows quantification of the size of the trigeminal cistern.
If not in the cistern (for example. CSF can be obtained in
the subarachnoid space beneath the temporal lobe), the
needle must be repositioned.
After satisfactory placement and cisternogram, the pa-
tient is again placed recumbent to allow the contrast
agent to flow out of the cistern; this is confirmed fluoro-
scopically. The patient then is placed back on a stretcher
in a full upright sitting position, and a quantity of glyc-
erol equal to the volume of the cistern is instilled slowly.
This may produce trigeminal pain, so it is best to pre-
medicate with analgesics, such as fentanyl, first. The pa-
tient is then transported back to his or her room but kept
sitting up at all times for about two hours to keep the
glycerol in the trigeminal cistern.
Most patients are pain free within a few hours and
may be discharged the following morning. Some will
continue to have tic pain for 7 to 10 days, though usually
it is distinctly less. Ten percent will require a second
procedure to get full relief. Once relieved. 75 percent
were still pain free after three years. For those with recur-
rence, the procedure can be readily repeated and has
been tolerated well so that there usually is no reluctance
on the patient's part to accept a repetition (unlike radio-
frequency lesioning).
Percutaneous compression of the gasserian ganglion
with a balloon catheter was introduced by Mullan in
1983 as technique to traumatize the trigeminal ganglion
and preganglionic rootlets mechanically using a percuta-
neously inserted balloon-tipped catheter (34). The cath-
eter is placed through the foramen ovale, using a similar
approach to the above two techniques, and then inflated
to compress the neural structures. The technique is
based on the earlier observation of Taarnhoj that me-
chanical trauma could relieve the pain of trigeminal neu-
ralgia, often for a significant period of time (35).
While long-term follow-up is not yet available, the ini-
tial results of this procedure appear to be comparable to
glycerol chemoneurolysis, with significantly less anesthe-
sia, dysesthesia, and corneal anesthesia than following
radiofrequency lesioning.
The Jannetta microvascular decompressive procedure,
in contradistinction to percutaneous neurolysis, in-
volves a formal operative procedure under general anes-
thesia. As such, it will always carry with it a higher risk. It
offers, however, the significant benefit of treating what
appears to be the probable cause of this problem and
achieving relief without neural destruction. Patients who
undergo this procedure, therefore, must accept a slightly
higher risk of serious complications but may be "cured"
of their problem without sacrificing neural function. We
usually reserve this procedure for the younger patient
(under 65) who is in good health and who is willing to
accept the somewhat higher risk to achieve these goals.
The procedure involves a limited suboccipital retro-
mastoid craniectomy performed under general endotra-
cheal anesthesia (35). I and many other surgeons have
preferentially used a sitting position for this operation;
however, equally satisfactory results can be achieved uti-
lizing a lateral, recumbent, or prone position. Access to
the trigeminal nerve is achieved by placing the craniec-
tomy just below the transverse sinus and just medial to
the sigmoid sinus. Opening the dura close to these ve- ,
nous sinuses allows exposure of the cerebellopontine an-
gle along the superior lateral margin of the cerebellum,
which is retracted gently. Prior microsurgical experience
and the use of the operating microscope are mandatory
for safe and accurate dissection. The petrosal vein is
usually coagulated and divided to gain access to the re-
gion of the trigeminal nerve, and the arachnoid around
the nerve is opened widely to inspect this area fully.
Elongated arterial loops impinging upon and cross-
compressing the root entry zone of the trigeminal nerve
are the most common findings in patients undergoing
this operation (Fig. 5A). In our personal series of over
300 cases, these were encountered 79 percent of the time
(36,37). Occasionally, venous channels impinging upon
the nerve in a similar manner were found (15 percent)
and, on rare occasions, tumors in the cerebellopontine
angle, such as meningiomas, acoustic neurinomas, or
cholesteatomas, were seen (3 percent). No pathology was
found in 3 percent of these patients. When tumors are
encountered, they are removed. Veins can be coagulated
and divided to decompress the root entry zone of the
nerve. Arterial channels are dissected completely free of
the root entry zone and secured with a small plastic
sponge prosthesis, usually Ivalon® (Unipoint Industries,
High Point, North Carolina) or a shredded teflon sponge
230 CHAPTER 11
B
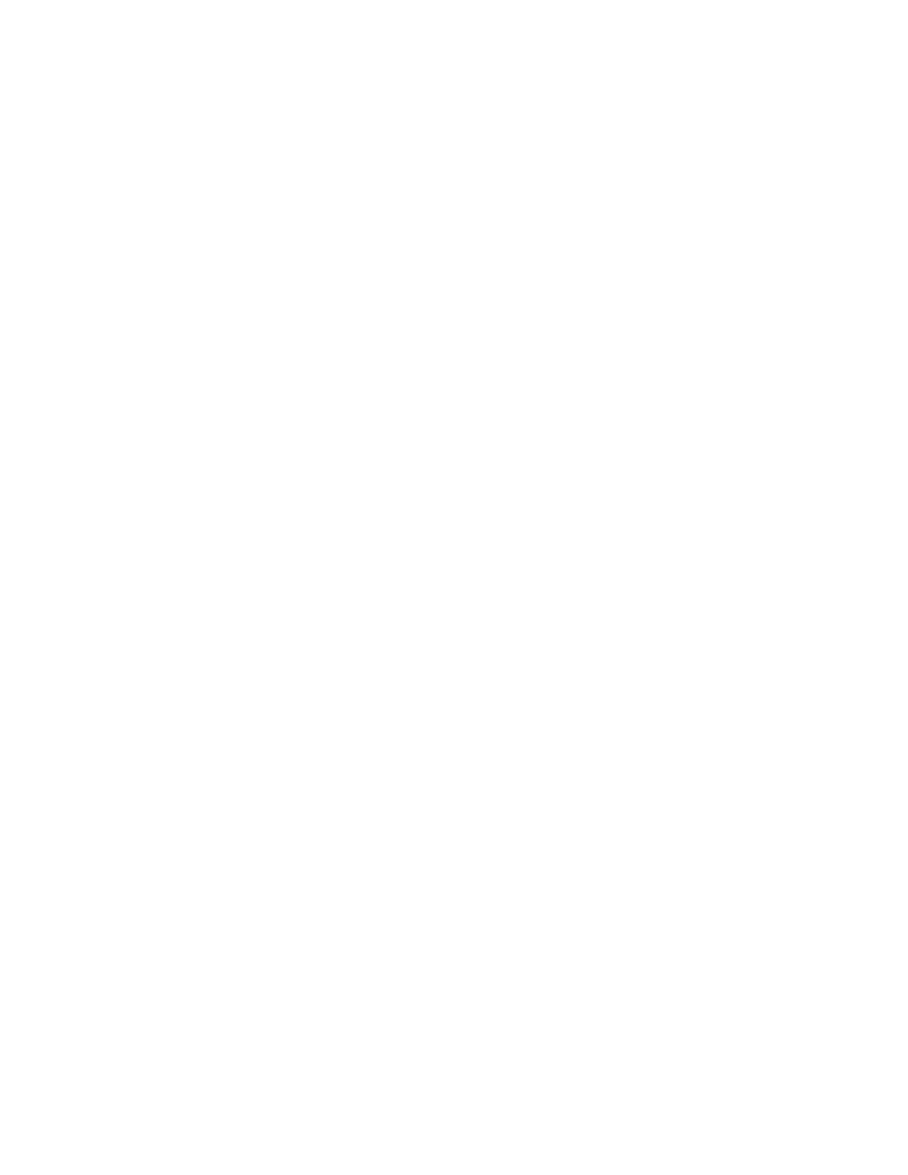
FIG. 5. (A) View through the operating microscope of the left trigeminal nerve, compressed by an
elongated superior cerebellar artery (SCA) as it traverses the brainstem. The artery is caught in the axilla
between the nerve and brainstem. (B) View after elevation of the arterial loop and placement of the
plastic prosthesis to prevent the reapposition of artery and nerve. (From reference 36, with permission.)
(Fig. 5B). The goal is to redirect the arterial pulsation
away from the root entry zone. Our operative findings
fully support those of Jannetta, and our results and fol-
low-up closely agree with those he has reported (38,39).
After satisfactory decompression, the dura is closed in
a watertight fashion and the wound is closed in layers.
We routinely place our patients on steroids preopera-
tively and for 24 hours postoperatively. Most patients
tolerate this procedure well and are able to begin oral
intake and get out of bed on the first postoperative day. If
the patients are operated on in the sitting position, they
usually have a moderate postoperative headache, which
can be controlled with oral analgesics. The majority of
patients can be discharged five to seven days postopera-
tively and usually take another week or two of additional
convalescence at home. During this period, they are en-
couraged to increase their activities gradually.
As with any operation, this procedure is not without
risk and fatal complications have ensued (1 percent).
Cerebellar hematomas or hemorrhagic infarction (1.6
percent) and supratentorial strokes (1 percent) have oc-
curred and at times have been responsible for fatalities,
despite vigorous appropriate treatment. Other signifi-
cant complications have included transient fourth-nerve
palsies (4 percent), transient facial nerve palsies (1.6 per-
cent), and unilateral hearing loss (2 percent; 1 percent
severe).
In trigeminal neuralgia associated with multiple sclero-
sis, if medical treatment is unsuccessful, relief can be
effected only by a destructive procedure. Percutaneous
lesioning is therefore the procedure of choice. If this is
unsuccessful for technical reasons, section of the nerve in
the posterior fossa will produce a similar benefit and, if
performed immediately adjacent to the brainstem, pro-
duces a lower incidence of dysesthesia and of numbness
than more peripheral destruction of the nerve.
There is a somewhat higher incidence of bilateral tri-
geminal neuralgia in patients afflicted with multiple scle-
rosis than occurs otherwise. In a small percentage of pa-
tients, trigeminal neuralgia may be the initial presenting
symptom of multiple sclerosis. This may explain the oc-
casional negative posterior fossa exploration, especially
in the younger patients.
Glossopharyngeal Neuralgia
The medical principles of treatment as outlined for
trigeminal neuralgia apply equally to this condition. If
these are unsuccessful, the Jannetta micro vascular de-
compression appears to be the definitive procedure of
choice, offering, as with trigeminal neuralgia, the oppor-
tunity for the relief of pain without sacrificing neural
function (38,39).
Radiofrequency lesioning at the jugular foramen has
been attempted, but this only produces a lesion distal to
the ganglion. Thus, recurrences in a few months can be
expected, as with peripheral nerve sectioning.
An alternative procedure involves sectioning of the
glossopharyngeal nerve and the upper several fascicles of
the vagus nerve in the posterior fossa (2). This procedure,
employed since its introduction by Love in 1948, is pref-
erable in more elderly patients, rather than exposing
them to increased operating time and the risks of manip-
ulating their intracranial vessels.
Potential complications and postoperative care are as
described above for trigeminal neuralgia. After section-
ing of the nerve, dysphagia may occur, as well as unpleas-
ant pharyngeal sensations.

TRIGEMINAL AND GLOSSOPHARYNGEAL NEURALGIA AND HEMIFACIAL SPASM / 231
Outcome
Success in relieving the pain of trigeminal neuralgia
has been achieved in about 95 percent of the patients
treated with either of these two types of procedures. Re-
currences following percutaneous radiofrequency le-
sioning have varied significantly in different series, but
average approximately 35 percent within four years.
There is an increasing incidence of recurrences with the
passage of time after surgery. Recurrences may occur in
the treated area but are more common in adjacent un-
treated regions. If necessary, the procedure can be re-
peated and many surgeons have preferred to produce
minimal lesions, minimizing numbness and decreasing
the risk of corneal anesthesia and dysesthetic sequelae,
while accepting a higher recurrence rate and repeating
the procedure as often as necessary (27).
With the Jannetta microvascular decompression, re-
currences, when they occur, tend to occur early, usually
within the first year to 18 months, with only a rare recur-
rence being reported after that. Severe refractory recur-
rences have occurred in 13 percent of our patients. An
additional 19 percent of our patients have had some
pain, which was well controlled with medication, usually
at very low dosages. Many of these patients (about one-
half) subsequently have been able to discontinue the
medication. All were refractory to medical treatment pre-
operatively, and most have reported that they feel the
procedure was of significant benefit to them, even if they
have required additional medication. Thus the overall
success rate for excellent (painfree) and good (controlled
pain) results is 87 percent.
Both of these procedures, therefore, offer great poten-
tial for the relief of this severe, incapacitating pain. Pa-
tient satisfaction with either has been gratifying, though
patients undergoing microvascular decompression are
significantly happier, since they do not have any sensory
loss, with its annoyance serving as a constant reminder
of their problem. The lack of dysesthesia and fewer recur-
rences also contribute to this increased satisfaction.
The choice of procedure must ultimately be made by
the patient, after he or she has achieved a thorough un-
derstanding of the potential risks and benefits of each.
The physician's recommendation also must be based on
a careful analysis of the patient's general health. For the
patient under age 65, in good general health, we usually
recommend the Jannetta microvascular decompression.
Glycerol chemoneurolysis is our preferred technique for
those patients who do not meet the above criteria, who
have multiple sclerosis, who do not wish to accept the
risks of microvascular decompression, or who have a re-
current tic after a prior surgical procedure.
The results in glossopharyngeal neuralgia are similar,
in a smaller number of reported cases treated with the
Jannetta procedure, and also with sectioning of the
nerve. The frequency of recurrence after microvascular
decompression approximates that seen in trigeminal neu-
ralgia and is less with nerve sectioning if the upper vagal
rootlets are included.
HEMIFACIAL SPASM
Incidence
Hemifacial spasm is a relatively rare condition. There
are no published epidemiologic studies, so its true inci-
dence is not known. From personal experience I would
estimate this condition to be approximately 25 percent
as common as trigeminal neuralgia. This may not be a
true figure, however, because many individuals may en-
dure rather than seek treatment for this condition, which
is neither life threatening nor painful. Also great regional
variation in incidence occurs, with an especially high fre-
quency of occurrence noted in Oriental (especially Japa-
nese) patients.
Etiology and Pathology
Hemifacial spasm appears to be the direct motor ana-
logue of trigeminal neuralgia. That is, both are disorders
of paroxysmal hyperactivity occurring in a cranial nerve.
Hemifacial spasm involves the facial nerve and as such
manifests pure motor hyperactivity, in comparison with
trigeminal neuralgia, which occurs in a primarily sen-
sory nerve and causes paroxysms of pain.
Significant historical observations have noted that, if
the nerve is sectioned at the stylomastoid foramen and
anastomosed to itself, the spasms return with reinnerva-
tion. If, however, an anastomosis to another cranial
nerve is performed, the spasms do not return. Thus the
site of pathology must be proximal to the stylomastoid
foramen. It has also been observed that a supratentorial
stroke producing a hemiplegia does not relieve the spasm
even in an otherwise plegic face (40). Therefore, the
pathological process must be confined to the lower mo-
tor neuron.
Isolated case reports dating back to an autopsy study
by Schultze in 1875 (41) have demonstrated vascular
lesions compressing the facial nerve in the posterior
fossa. Campbell and Keedy published two cases in 1947
in which a "cirsoid aneurysm" (nowadays known as ver-
tebral basilar dolichoectasia) was found compressing the
facial nerve (42). Other isolated case reports support
these observations. Tumors compressing the facial nerve
in the posterior fossa and causing hemifacial spasm were
noted by Dandy (43,44) and Gushing (45). In 1961
Gardner and Sava presented their experience with 19
patients (46). In 14 of these they found mass lesions. In
the majority of cases, the problem appeared to stem from
either normal or abnormal blood vessels. Gardner and

CHAPTER 11
Sava also suggested that hemifacial spasm was a revers-
ible pathophysiological state.
It was not until the systematic application of the oper-
ating microscope by Peter Jannetta, commencing in
1967, that a large series of observations was made in
patients with hemifacial spasm. Jannetta not only firmly
established that root exit zone compression of the facial
nerve is present in virtually every patient afflicted with
this problem but also devised a nondestructive tech-
nique for moving the blood vessel (which is the common
cause) away from the nerve and securing it with a small
sponge prosthesis to decompress the nerve effectively.
Jannetta's observations have been substantiated by sev-
eral other surgeons (36,47), firmly establishing the etiol-
ogy of hemifacial spasm.
The exact physiological effect that this root exit zone
compression produces is not fully understood. Hunt in
1909 detailed the role of sensory afferent fibers in the
facial nerve. Gardner suggested a reverberating circuit
produced by afferent-efferent transaxonal "short-circuit-
ing" (46).
Symptoms
Hemifacial spasm usually begins with small, uncon-
trollable twitching movements occurring in a unilateral
orbicularis oculi muscle, with a slow and insidious pro-
gressive spreading of the spasms down the face. The hy-
peractivity is limited entirely to muscles supplied by the
seventh cranial nerve. The twitching is involuntary and
patients are unable to stop it.
The condition tends to worsen gradually with the pas-
sage of time, often slowly over months to years until
gross disfiguration of the face occurs. Far from being
only a cosmetic problem, hemifacial spasm creates signif-
icant functional disability because of the limitations on
vision imposed by the constant blinking and twitching.
This can impair many normal daily activities such as
reading and driving. With increased severity, the pla-
tysma muscle in the anterior neck and the corrugator
muscles of the forehead may ultimately become in-
volved. Jannetta and associates have also described an
atypical form of this problem, which starts in the mid-
face and advances up to the forehead (48).
Hemifacial spasm is slightly more common in men
and more common on the left side of the face. It has not
been described in children. Like many neurologic prob-
lems it will be aggravated by psychological stress as well
as fatigue and has therefore been erroneously thought to
have an emotional basis. Voluntary movement may ag-
gravate the spasms. Spasms often stop during sleep but
may persist in about 10 percent of patients. Bilaterality
has been described (6 percent), but, when this occurs, the
spasms are neither synchronous nor symmetrical.
Hemifacial spasm has been reported in association
with trigeminal neuralgia. Gushing apparently was the
first to describe this under the term "tic convulsif" (49).
Most commonly, mass lesions in the posterior fossa, re-
sulting in compression of both the fifth and seventh
nerves, have been associated with this combination. Sep-
arate independent lesions, however, may also occur.
Signs
The clinical appearance of patients suffering from this
problem is quite characteristic. Intermittent, uncontrol-
lable, brief, repetitive, and painless spasms of the facial
musculature, most prominent in the midface, are noted.
Occasionally the "tonus" phenomenon occurs, in which
sustained forceful contractures, usually of the midface
musculature, last for several seconds or even longer.
Physical examination will usually reveal abnormalities
of the cranial nerves. Mild facial paresis (between
spasms) may be noted, as well as mild decreased hearing
in the ipsilateral ear, in long-standing cases. Deficits in
cranial nerves V, VII, or IX or cerebellar or brainstem
findings suggest a mass lesion in the cerebellopontine
angle.
Diagnostic Tests
The diagnosis of hemifacial spasm can be made by the
clinical appearance in association with the history as
given above. There is remarkable consistency among pa-
tients in clinical presentation. On electrical testing, the
EMG in hemifacial spasm is quite characteristic, demon-
strating rhythmically occurring bursts of 5 to 20 dis-
charges per second, along with individual discharges and
longer lasting bursts (50). The rate of discharge of the
latter may be as high as 150 to 250 per second, with
almost complete synchronization of the discharges occur-
ring within the entire area of the affected facial muscles.
These electrical findings are not seen in other conditions
and will therefore differentiate hemifacial spasm from
other types of abnormal facial motor activity.
The differential diagnosis of hemifacial spasm in-
cludes blepharospasm, which is a bilateral forced con-
tracture of the muscles about the eyes and is distin-
guished from hemifacial spasm by its bilaterality and its
confinement entirely to the periorbital musculature. Fol-
lowing Bell's palsy, at times, synkinetic movements of
the face may mimic hemifacial spasm. This history of
antecedent Bell's palsy with the development of such
movements as the nerve regenerates usually will distin-
guish these, but electrical testing may be helpful. An-
other condition, facial myokymia, results in writhing
worm-like movements of the facial musculature. This is
seen with intrinsic brainstem disease and, again, can be
differentiated electrically if the clinical situation is not
clear-cut.
TRIGEMINAL AND GLOSSOPHARYNGEAL NEURALGIA AND HEMIFACIAL SPASM / 233
As in trigeminal neuralgia, a MR scan may disclose a
vascular loop but mainly is done to rule out a mass le-
sion.
Treatment
There is no effective medical treatment for hemifacial
spasm. This condition has been described as "socially,
psychologically and economically disabling" (48). There-
fore, surgery is of much more than cosmetic significance.
A number of procedures involving methods of destroy-
ing or injuring the facial nerve have been attempted but
result in incomplete relief of the problem and facial palsy
to some extent.
Some success has been achieved with partial denerva-
tion of the facial muscles by injecting botulinum toxin
into the most active regions. With small incremental in-
jections, denervation can be limited and the spasms re-
duced. Denervation of course does not fully resolve the
problem and may require repetitive treatments, but it
can be considered as an alternative, especially in elderly
or infirm patients.
The definitive treatment of this problem is the Jan-
netta microvascular decompressive operation, which in-
volves a limited retromastoid posterior fossa craniec-
tomy and microsurgical exploration of the root exit zone
of the facial nerve. Lesions impressing upon the nerve at
this area have been found in close to 100 percent of pa-
tients in several large series explored by this technique
(Fig. 6). Most commonly these are arterial channels, ei-
ther normal vessels (usually the posterior inferior cere-
bellar artery, the anterior inferior cerebellar artery, or the
vertebral artery) or dilated or ectatic vessels (previously
called cirsoid aneurysms), but on occasion venous chan-
nels, arteriovenous malformations, aneurysms, and
small tumors have been encountered. These latter of-
fending causes are surgically removed. Arterial channels
are dissected free of the nerve and secured with a small
plastic sponge prosthesis to prevent their reappostion.
The operative technique is similar to that employed in
the Jannetta operation for trigeminal neuralgia, except
that the exposure is from lateral inferior, beneath the
cerebellum (36,48).
Outcome
The Jannetta procedure has resulted in excellent relief
of hemifacial spasm in the vast majority of patients so
treated. Jannetta in 1980 reported excellent results in
213 of 229 patients (12 patients required a second proce-
dure) (39). An additional 11 patients (5 percent) had less
than 25 percent of their preoperative level of spasms but
were not completely relieved. The procedure failed in
five patients (2 percent).
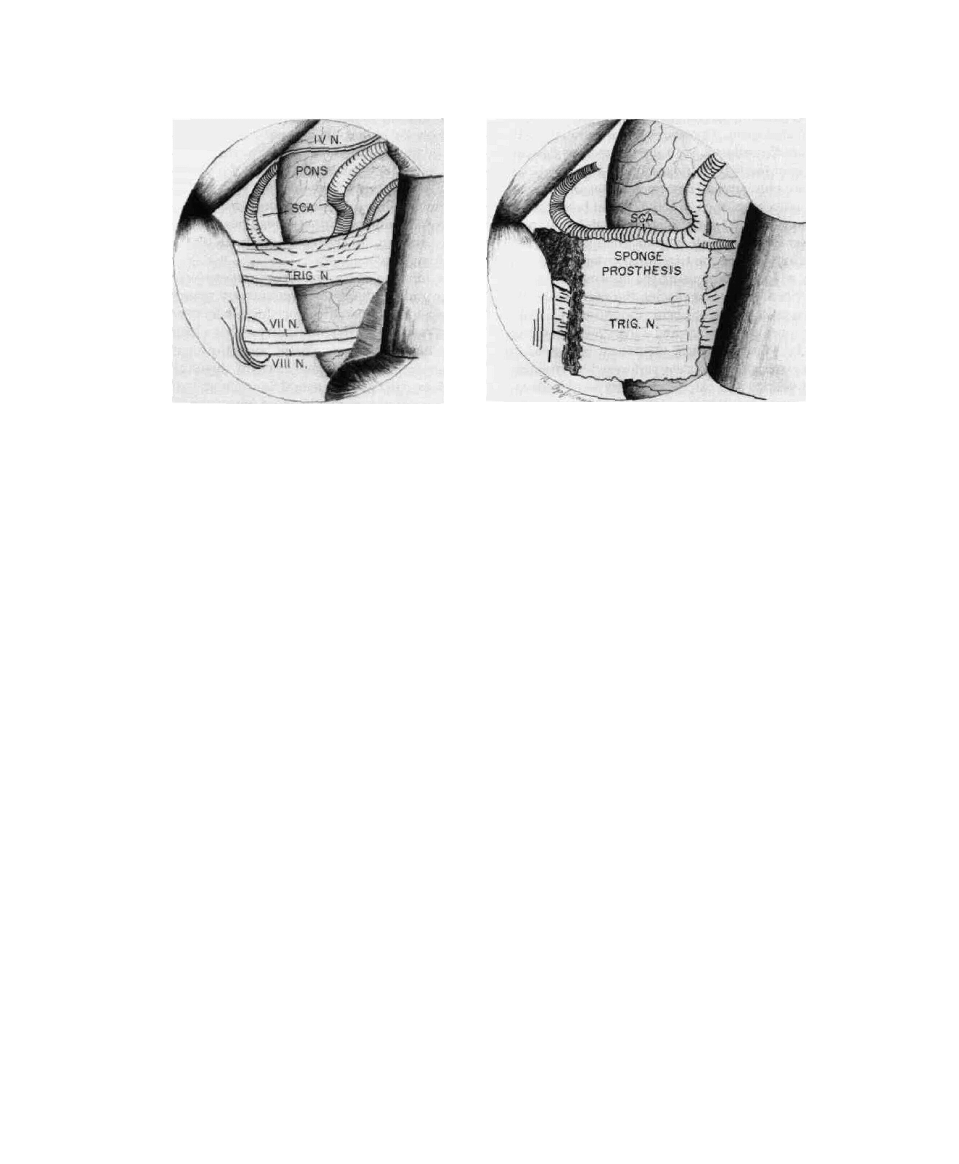
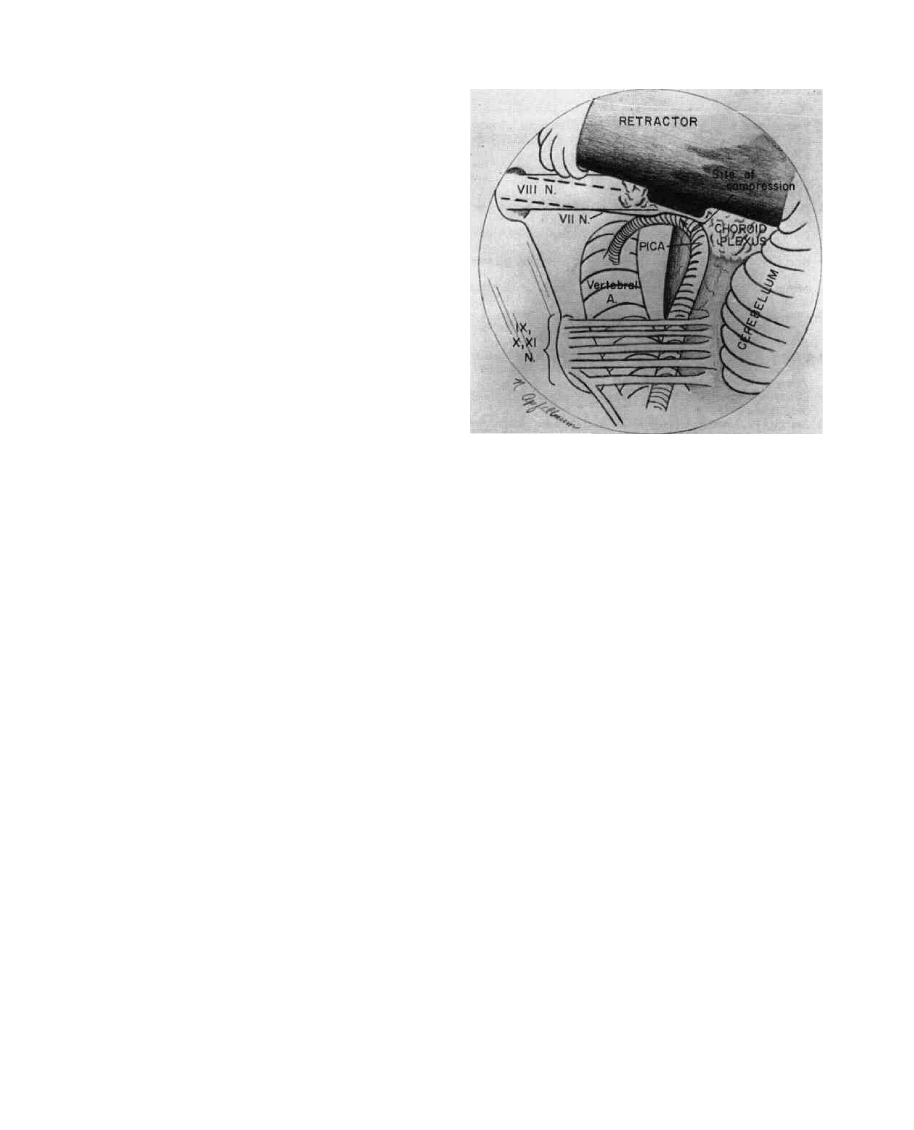
FIG. 6. Surgeon's view through the operating microscope.
Exposure of left facial nerve. When the cerebellum is ele-
vated, the root exit zone of the facial nerve is seen to be
compressed by an elongated loop of the posterior inferior
cerebellar artery (PICA). (From reference 36, with permis-
sion.)
In our personal series of 66 patients, we have found
vessels compressing the nerve in 65 cases: 64 were arte-
rial channels and 1 was a venous channel. A bony exos-
tosis compressed the nerve in the remaining case. No
negative explorations occurred. All patients were ini-
tially relieved of their spasm, although the spasm did
persist in the postoperative period for up to several
months in 10 percent of these patients before finally sub-
siding. Recurrences have appeared in 16 patients. Nine
were transient and resolved completely, four were mini-
mal not requiring further treatment, and two were signifi-
cant. One of these has been relieved by a second opera-
tion. Facial weakness was noted in six patients but was
only minimal in three. All these patients have recovered
from it.
This procedure, of course, involves a formal craniot-
omy under general anesthesia and will always carry with
it a small but real element of risk. In addition to the
generalized risks detailed earlier regarding this operative
technique for trigeminal neuralgia, the procedure as ap-
plied to the facial nerve carries with it the primary risk of
injury to the facial and/or auditory nerve. Thus, hearing
loss has been reported in the literature in approximately
8 percent of patients and facial weakness in 7 percent. In
our own experience, we have encountered hearing loss in
only one patient (2 percent) and, as noted, no permanent
facial weakness.
Wyszukiwarka
Podobne podstrony:
ZX50 cap 11 (carburatore)
neural defect cap 19
Zarz[1] finan przeds 11 analiza wskaz
11 Siłowniki
11 BIOCHEMIA horyzontalny transfer genów
PKM NOWY W T II 11
wyklad 11
R1 11
CALC1 L 11 12 Differenial Equations
Prezentacje, Spostrzeganie ludzi 27 11
zaaw wyk ad5a 11 12
budzet ue 11 12
EP(11)
W 11 Leki działające pobudzająco na ośrodkowy układ
więcej podobnych podstron